

Abstract
Background
Interruptions in the pharmacy setting by nurses are common. While the source of nurse-generated interruptions may be variable, the appropriateness of these interruptions remains unknown.
Objective
To evaluate the impact and appropriateness of nursing interruptions on pharmacist workflow resulting from telephone calls, alphanumeric pagers, and in-person interactions.
Methods
An electronic data collection tool was created to record nursing-based interruptions of pharmacists through telephone calls, pages, and in-person interactions. The data were collected during all pharmacist shifts (day, evening, and night) over 14 days in 2 separate, 7-day data collection periods in December 2011 and January 2012. The data collection form comprised 7 questions that addressed the purpose of this study, including the shift; unit location; type, nature, and appropriateness of the interruption; estimated time spent; and whether the interruption was duplicated.
Results
A total of 3,531 interruptions were documented during the 14 days of data collection; an average of 252 data points per day were recorded by the pharmacists. About 55% of the interruptions were initiated through alphanumeric pagers, 33% from phone calls, and 12% from face-to-face interactions. Sixty-three percent of the total interruptions were annotated as appropriate interruptions, while 37% of were annotated as inappropriate interruptions. The total time spent addressing the interruptions deemed inappropriate was 75 hours during the study period.
Conclusion
Distinct opportunities exist for process improvement changes, as well as educational and behavioral changes, that would greatly benefit nursing and pharmacy staff.
Keywords: interruption, nurse, pharmacy, workflow
Interruptions in the pharmacy setting are common and multifactorial.1,2 While pharmacist interactions with other health care providers regarding patient care (ie, physicians and nurses) are important to optimize patient care and delivery of therapy, little is known about the impact of these interactions on the pharmacist workflow. Prior reports from physicians and nurses demonstrated that interruptions have a negative impact on the workflow of health care workers.3–13 Other investigators suggest that interruptions increase the risk of medication errors.14,15 The link between interruptions and medication errors is beyond the scope of this study.
Pharmacists play a key role in patient care and are in a vital position to provide specific information about medication-related inquiries that are “interruptions” from other health care providers. At our institution, a hospital-wide survey identified job-related stress as a major factor leading to employee dissatisfaction in the pharmacy department. A subsequent survey of pharmacists identified excessive interruptions through telephone calls, alphanumeric pagers, and face-to-face interactions as the most common contributors to job stress. As a result, the pharmacy department leadership considered this to be an area to target for future performance process improvement.
Although the sources of interruptions are varied, we only considered nurse-generated interruptions for the purpose of this study because (1) nurses are the largest group among health care providers; (2) nursing-related staff account for the majority of all interruptions (based on an earlier survey); and (3) it is easiest to characterize types of interruptions from a single group of health care providers.
Few reports have quantified the amount of phone interruptions in the pharmacy practice setting,16–18 but none of these have included other (non-telephone) types of interruptions, such as face-to-face interactions and alphanumeric pagers. In addition, it has not been reported whether the data collectors deemed these interruptions appropriate or inappropriate. We therefore sought to evaluate the root causes of the nurse-generated interruptions, to quantify their frequency, and to determine the appropriateness so that we could identify opportunities for future change. To our knowledge, this is first pharmacy practice–related study to evaluate and characterize nurse-generated interruptions in an inpatient setting.
Methods
This observational study was conducted at a 793-bed tertiary academic medical center over two 7-day periods (total, 14 days). Pharmacists in all shifts (day, evening, night) were required to participate in the research. The distribution of pharmacists differed between shifts. On weekdays, during the day shift, there were 20 pharmacists distributed over the floors to provide pharmacy services. However, there were only 8 pharmacists during the evening shift and 3 pharmacists during the night shift who were responsible for providing pharmacy services; they were physically present in the main pharmacy. On the weekends, there were 8 pharmacists during the day shift, 5 during the evening shift, and 3 during the night shift. The number of technicians also varied among the shifts.
Interruptions were recorded electronically via an online, Web-based survey tool. The data collection form included 7 questions for each documented interruption and required the following data to be recorded: shift (day, evening, night), nurse service location, type of interruption (page, phone call, in-person “face-to-face encounter”), nature of the interruption (see the box titled, “Categories of the Nature of Nursing Interruptions”), estimated time spent per interruption, whether the interruption was appropriate or inappropriate, and whether the interruption was a duplicated request. The data collection form was trialed by a sample group of pharmacists; this confirmed that the form was efficient and easy to use. Broadcast e-mails and educational presentations were provided to all pharmacists over 2 weeks prior to the study initiation to explain the study criteria. All pharmacists submitted at least one test interruption to verify that they know how to access and use the data collection form prior to the start of the actual data collection.
For the purpose of this study, we defined an interruption as (1) a signal that distracts the pharmacist from the main task on which he or she is working, 16 or (2) a break in a task being performed that results in a different task being completed first. 19 Only interruption events related to patient care that were generated by nurses through page, phone, or face-to-face encounter were considered for this study. There was no hospital policy regarding the use of communication devices (ie, page or phone).
Categories of the Nature of Nursing Interruptions
-
•
Automated Dispensing Cabinet (ADC) equipment (eg, broken, door stuck)
-
•
ADC refill/restock request
-
•
Change package request (eg, change tablet to oral liquid)
-
•
Computerized physician order entry or electronic medication administration record (eMAR) related question
-
•
Drug information
-
•
Extra dose request
-
•
Inquiry about the location of medication (refrigerator vs patient-specific bin vs ADC)
-
•
Medication scheduling/timing in eMAR
-
•
Nonurgent or urgent order approval request
-
•
“Please send” request in eMAR for medications that are newly prescribed
-
•
Pneumatic tube delivery medication request
During the study period, pharmacists were asked to keep the data collection form open on their desktop or laptop computer during their entire shift so that it would be available on their task bar for quick and easy data submission. The data collection form is on a continuous loop; once the pharmacist submits the event, it will auto refresh and quickly allow the pharmacist to enter another interruption. All information related to any nurse-generated interruption, whether it was from a page, a phone call, or in-person, had to be recorded by the pharmacist right after the event. For all interruptions, the recording pharmacist evaluated the nature of interruption for appropriateness considering the following factors: nature, timing, frequency, and whether the request could have been addressed through online resources or electronic applications available on the pharmacy Web page or within the clinical information systems. The principal investigator reviewed all the submitted interruptions to verify the accuracy of the documentation of the appropriateness. During all study periods, daily data summaries were posted on a bulletin board in central pharmacy so pharmacists could see the project progress and results. Additionally, ongoing informational meetings regarding the progress of this study were conducted to keep all pharmacists informed about its status.
Results
During the observation time of 14 days, a total of 3,531 interruptions were documented with an average of 252 data points per day. Overall, 1,944 (55%) of interruptions were initiated through alphanumeric pagers, 1,173 (33%) were attributed to phone calls, and 414 (12%) involved face-to-face interactions. The total incidence of interruptions was highest during the day shift (41.7% [day] vs 30.7% [evening] vs 27.6% [night]). However, when the number of interruptions per shift was normalized to the number of pharmacists covering the respective shifts, the overnight shift had the greatest number of interruptions per pharmacist per shift (16.9 [day] vs 27.1 [evening] vs 43.2 [night]).
Of the 3,531 interruptions documented, 2,215 (63%) were annotated by the recording pharmacists as appropriate, and 1,316 (37%) were annotated as inappropriate. Of the inappropriate interruptions, 748/1,316 (56.8%) occurred through alphanumeric pages, 484/1,316 (36.8%) through phone calls, and 84/1,316 (6.4%) through face-to-face interactions. The frequency of the inappropriate interruptions according to their nature is shown in Figure 1.
Figure 1.
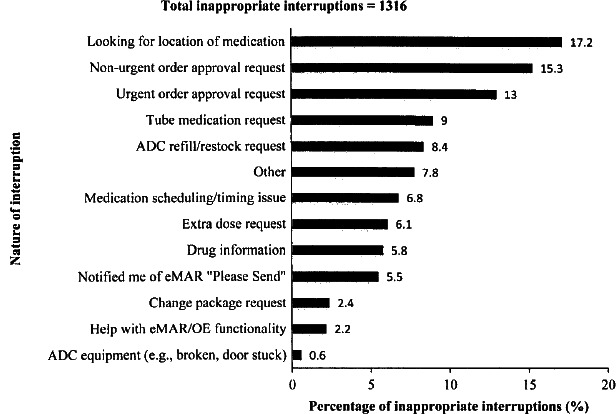
Breakdown of the nature of the interruptions that were annotated as inappropriate. The “Other” category includes inquiries about the pharmacist beeper (available online), inquiries about nonpharmacy products, looking for floor stock items, pages with no message, a page with insufficient information, dispensing medication to a family member, and automated dispensing cabinet (ADC)–related issues (eg, discrepancies, transferring patients, adding patients). eMAR = electronic medication administration record; OE = order entry.
This study found that 4,487 minutes over the 14 days of data collection were spent addressing interruptions that were deemed inappropriate (3.4 minutes for each interruption). This equates to approximately 5.3 hours per day of pharmacist time devoted to interruptions that could be avoided; when annualized, this adds up to 0.92 of a full-time employee.
Discussion
The health care environment is interruptive by nature. Our study demonstrates the large number of interruptions that pharmacists encounter during their regular shifts. Although part of the pharmacist workflow involves being interrupted by other health care providers to assist with patient-related medical service activities, it is clear that some of these interruptions are unnecessary.
The majority of the inappropriate interruptions were related to either missing medications (~40%) or orders that needed approval (~28%). We investigated the documented reasons as to why pharmacists deemed these interruptions inappropriate in order to identify possible areas for process improvement or increased collaboration. Documented reasons included unnecessary inquiries for medications that had already been approved and/or delivered, not taking advantage of the multiple communication functionalities in the clinical information systems (ie, electronic medication administration record, computerized physician order entry), and duplicate inquiries about an issue that was in the process of being dealt with or had already been addressed.
Given that 68% of the documented interruptions were for missing medications and/or medications needing approval, our study highlighted the importance of expanding the role of pharmacy technicians in the process of medication dispensing and distribution. This would allow pharmacists to become more involved and active participants in the multidisciplinary team in terms of patient management discussions and recommendations.
This study identified some actions that may help to reduce unnecessary interruptions, including nursing education regarding different or preferential ways to communicate with the pharmacy staff via the telephone/paging directory system to improve work-flows, the different functionalities available in clinical information systems that can be used for various nursing inquiries; and the accessible clinical information resources (eg, guidelines, electronic medication references). Pharmacy also needs to work on different ways to communicate their actions with other health care professionals in order to avoid unnecessary inquiries. One example of this would be the development of a system that allows nurses to check the current status of new orders, urgent orders, location of the medication to be delivered, and the estimated wait time for each process.
Pharmacists' roles have been expanding in our institution. The data from this study are currently being utilized to create solutions for decreasing unnecessary interruptions resulting from process or behavioral issues that would greatly benefit both nursing and pharmacy staff. The pharmacy department is conducting several projects that will assist in minimizing the amount of pharmacist time that is wasted on unnecessary interruptions and facilitating better compliance with nursing needs. These projects include the implementation of a phone call tree in the central pharmacy to better direct the calls, formulation of a quality improvement process for restocking automated dispensing cabinets and delivering medications to inpatient care units, and reallocation of pharmacist resources to better align the staffing of day, evening, and night shifts with workload requirements. These changes may lead to a significant decrease in inappropriate interruptions of pharmacy staff and possibly alter the frequency of certain types of appropriate interruptions to help improve pharmacist workflow, efficiency, and job satisfaction.
Our survey has some limitations. This study was limited to a single academic center, thus the workload per pharmacist may be not applicable to other institutions that have a larger staff of pharmacists and technicians. We did not investigate the correlation between the interruptions and the risk of medication errors. This is due to the lack of validated measures to estimate the correlation and the lack of an advanced surveillance system to track a medication error to a pharmacist interruption. However, one study in the ambulatory care setting showed that the rate of dispensing errors was higher when pharmacists were interrupted.' Further research is warranted to investigate this relationship. This study examined only nurse-generated interruptions and did not include interruptions generated by other health care providers. We focused on identifying specific types of workflow interruptions that were generated by the nurses to allow us to tailor an action plan to present to the nursing department and formulate a targeted intervention. Thus, results from this study may not be extrapolated to interruptions from other health care providers.
Despite these limitations, our study was the first to investigate the number, type, duration, and appropriateness of interruptions in an inpatient institutional pharmacy practice. Further studies are needed to investigate the impact of pharmacist interruptions on medication errors.
Conclusion
Several sources of unnecessary interruptions of pharmacists were identified that should be considered when quality improvement programs are being formulated.
References
- 1.Flynn E.A., Barker K.N., Gibson T. et al. Impact of interruptions and distractions on dispensing errors in an ambulatory care pharmacy. Am J Health Syst Pharm. 1999; 56(13): 1319–1325. [DOI] [PubMed] [Google Scholar]
- 2.Peterson G.M., Wu M.S., Bergin J.K. Pharmacist's attitudes towards dispensing errors: Their causes and prevention. J Clin Pharm Ther. 1999; 24(1): 57–71. [DOI] [PubMed] [Google Scholar]
- 3.Liu D., Grundgeiger T., Sanderson PM et al. Interruptions and blood transfusion checks: Lessons from the simulated operating room, Anesth Analg. 2009; 108(1): 219–222. [DOI] [PubMed] [Google Scholar]
- 4.Grundgeiger T., Snaderson P. Interruptions in healthcare; theoretical views. Int J Med Inform. 2009; 78: 293–307. [DOI] [PubMed] [Google Scholar]
- 5.Prakash V., Koczmara C., Savage P. et al. Mitigating errors caused by interruptions during medication verification and administration: Interventions in a simulated ambulatory chemotherapy setting. BMJ Qual Saf. 2014; 11: 884–892. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Spooner A.J., Corley A., Chaboyer W. et al. Measurement of the frequency and source of interruptions occurring during bedside nursing handover in the intensive care unit: An observational study. Aust Crit Care. 2015; 28(1): 19–23. [DOI] [PubMed] [Google Scholar]
- 7.Berg L.M., Källberg A.S., Göransson K.E. et al. Interruptions in emergency department work: An observational and interview study. BMJ Qual Saf. 2013; 22(8): 656–663. [DOI] [PubMed] [Google Scholar]
- 8.Weigl M., Müller A., Vincent C. et al. The association of workflow interruptions and hospital doctors' workload: A prospective observational study. BMJ Qual Saf. 2012; 21(5): 399–407. [DOI] [PubMed] [Google Scholar]
- 9.Wiegmann D.A., ElBardissi A.W., Dearani J.A. et al. Disruptions in surgical flow and their relationship to surgical errors: An exploratory investigation. Surgery. 2007; 142: 658–665. [DOI] [PubMed] [Google Scholar]
- 10.Kosits L.M., Jones K. Interruptions experienced by registered nurses working in the emergency department. J Emerg Nurs. 2011; 37(1): 3–8. [DOI] [PubMed] [Google Scholar]
- 11.Jeanmonod R., Boyd M., Loewenthal M. et al. The nature of emergency department interruptions and their impact on patient satisfaction. Emerg Med J. 2010; 27(5): 376–379. [DOI] [PubMed] [Google Scholar]
- 12.Trbovich P., Prakash V., Stewart J. et al. Interruptions during the delivery of high-risk medications. J Nurs Adm. 2010; 40(5): 211–218. [DOI] [PubMed] [Google Scholar]
- 13.Coiera E.W., Jayasuriya R.A., Hardy J. et al. Communication loads on clinical staff in the emergency department. Med J Aust. 2002; 176(9): 415–418. [DOI] [PubMed] [Google Scholar]
- 14.Westbrook J.I., Woods A., Rob M.I. et al. Association of interruptions with an increased risk and severity of medication administration errors. Arch Intern Med. 2010; 170(8): 683–690. [DOI] [PubMed] [Google Scholar]
- 15.O'Shea E. Factors contributing to medication errors: A literature review. J Clin Nurs. 1999; 8: 496–504. [DOI] [PubMed] [Google Scholar]
- 16.Brixey J.J., Walji M., Zhang J.J. et al. Proposing a taxonomy and model of interruption. In: Proceedings of the 6th International Workshop on Enterprise Networking and Computing in Healthcare Industry. HEALTHCOM. 2004: 184–188.
- 17.Burford M.E., Yeck A.E., Tucker J.A. Stressors in the pharmacy: An observational of interruptions in pharmacy. In: Proceedings of the Human Factors and Ergonomics Society Annual Meeting. 2011; 55: 1970–1974. [Google Scholar]
- 18.Silver J. Interruptions in the pharmacy: Classification, root-cause, and frequency. ISMP Web site, www.ismp.org/docs/SilverJ_SHS2010.pdf. Accessed June 1, 2012.
- 19.Chisholm C.D., Dornfeld A.M., Nelson D.R. et al. Work interrupted: A comparison of workplace interruptions in emergency departments and primary care offices. Ann Emerg Med. 2001; 38(2): 146–151. [DOI] [PubMed] [Google Scholar]