

Abstract
Introduction.
Medicaid managed care organizations (MCO) play a major role in addressing the nation’s epidemic of drug overdose and mortality by administering substance use disorder (SUD) treatment benefits for over 50 million Americans. While it is known that some Medicaid MCO plans delegate responsibility for managing SUD treatment benefits to an outside “carve out” entity, the extent and structure of such carve out arrangements are unknown. This is an important gap in knowledge, given that carve outs have been linked to reductions in rates of SUD treatment receipt in several studies. To address this gap, we examined carve out arrangements used by Medicaid MCO plans to administer SUD treatment benefits in ten states.
Methods.
Data for this study was gleaned using a purposive sampling approach through content analysis of publicly available benefits information (e.g., member handbooks, provider manuals, prescription drug formularies) from 70 comprehensive Medicaid MCO plans in 10 selected states (FL, GA, IL, MD, MI, NH, OH, PA, UT, and WV) active in 2018. Each Medicaid MCO plan’s documents were reviewed and coded to indicate whether a range of SUD treatment services (e.g., inpatient treatment, outpatient treatment, residential treatment) and medications were carved out, and if so, to what type of entity (e.g., behavioral health organization).
Results.
A large majority of Medicaid MCO plans carved out at least some (28.6%) or all (40.0%) SUD treatment services, with nearly all plans carving out some (77.1%) or all (14.3%) medications, mainly due to the carving out of methadone treatment. Medicaid MCO plans most commonly carved out SUD treatment services to behavioral health organizations, while most medications were carved out to state Medicaid fee-for-service plans.
Conclusions.
Carve out arrangements for SUD treatment vary dramatically across states, across plans, and even within plans. Given that some studies have linked carve out arrangements to reductions in treatment access, their widespread use among Medicaid MCO plans is cause for further consideration by policymakers and other key interest groups. Moreover, reliance on such complex arrangements for administering care may create challenges for enrollees who seek to learn about and access plan benefits.
Keywords: Substance use disorder, Medicaid, managed care, treatment, carve outs
1. INTRODUCTION
The United States remains in the midst of an unprecedented epidemic of drug and alcohol-related overdose and mortality. In 2020, over 40 million Americans had a substance use disorder (SUD) and over 100,000 lives were lost to drug-related unintentional poisoning, with another almost 100,000 lives lost due to alcohol-related deaths (Centers for Disease Control and Prevention [CDC], 2022; National Institute on Alcohol Abuse and Alcoholism [NIAAA], 2023; Substance Abuse and Mental Health Services Administration [SAMHSA], 2021). As drug-related overdose and mortality continue to rise, expanding access to SUD treatment is more important than ever. Decades of evidence show that treatment, including psychosocial interventions and medications, can reduce substance use and improve quality of life (U.S. Department of Health & Human Services, 2016). For example, receipt of medications for opioid use disorder such as buprenorphine and methadone are associated with reduced all-cause and drug-related mortality, and research has shown that these medications reduce overdose and acute care use as compared to other treatments such as non-pharmacologic treatments and therapy alone (Lyden & Binswanger, 2019). However, treatment remains difficult to obtain. Only about 10% of Americans with SUD received any treatment for their condition in 2021 (SAMHSA, 2021).
Medicaid represents one of the most important policy levers available to expand access to SUD treatment. First, it is a wide-reaching program that finances health care for over 90 million Americans—roughly 20% of the entire U.S. population (Centers for Medicare & Medicaid Services [CMS], 2023). Second, the prevalence of SUD among this population is high, surpassing that of the uninsured and privately insured, with Medicaid covering 21% of nonelderly adults with SUDs as compared to 16% of those who are commercially insured (Saunders, 2023). Third, Medicaid plays a leading role in paying for SUD treatment in the United States. The Affordable Care Act dramatically expanded eligibility for Medicaid while also requiring state Medicaid programs to ensure that most benefits for SUD are provided at parity with other medical and surgical services, resulting in a major expansion in coverage for SUD treatment. The program is now the largest payer of all SUD treatment in the United States, financing over $12 billion in treatment services annually—more than four times the funding provided by the Substance Abuse Prevention and Treatment Block Grant (Mark et al., 2014).
In order to fully understand Medicaid’s role in financing SUD treatment, it is essential to account for the role of managed care, which has emerged as a dominating force within the program over the past three decades. State Medicaid agencies contract with managed care organizations (MCOs) to manage costs, utilization, and quality through a capitated payment model. As of 2022, 41 states and the District of Columbia operate more than 280 comprehensive managed care plans nationwide (Kaiser Family Foundation, 2022b). Currently, most Medicaid enrollees participate in managed care. In 2020, Medicaid plans across the country assigned roughly 57 million enrollees to MCO plans, accounting for over 70% of all Medicaid enrollees nationally and encompassing the majority of adults covered by the program under age 65 (Kaiser Family Foundation, 2022a).
Although Medicaid MCO plans are federally regulated, federal law nonetheless affords considerable discretion to MCO plans to structure benefit design. Unless states explicitly restrict them from doing so, comprehensive MCO plans are allowed to limit benefits through the use of waivers or state plan amendments (Medicaid and CHIP Payment and Access Commission [MACPAC], n.d.b). Hence, Medicaid MCO plans can and do vary substantially in the benefits that they provide and the way that they manage those benefits. Carve outs, through which a separate organization covers and administers benefits and services, are particularly common within these plans. Primary carve outs are defined as arrangements under which certain benefits are excluded from the primary MCO contract and for which Medicaid maintains the responsibility for their administration—typically by a state’s fee-for-service (FFS) program. Secondary carve outs occur when a MCO plan subcontracts administration of a defined set of benefits to a separate organization or entity (Open Minds, 2016).
Carve out arrangements are particularly common for behavioral health, which typically encompasses both mental health and SUD treatment. Such arrangements have been in existence almost as long as managed care itself. Secondary carve outs to behavioral health organizations (BHOs) began as early as the 1980s, when increasing utilization of hospitalization for treatment of mental health and SUDs led some MCOs to contract with specialty BHOs to administer behavioral health benefits with an eye towards controlling costs and minimizing unnecessary utilization of care (Frank & Garfield, 2007). Much of the proliferation of carve out arrangements has been due to these secondary carve-outs to BHOs. Use of behavioral health carve outs grew substantially over the next several decades. By 2003, roughly three quarters of managed care plans nationally reported contracting out management of their behavioral health benefits, most frequently to a BHO that assumed full financial risk for managing these benefits (Frank & Garfield, 2007). While many states have reported carving in more of their behavioral health services due to federal rules such as the 2016 CMS managed care regulations, many plans have begun to subcontract the management and risk of behavioral health care to BHOs, though the financing stays with the state (Charlesworth et al., 2021). Additionally, some advocates argued that the implementation of carve outs under specialized BHOs could increase quality and effective utilization management, while also avoiding adverse selection by which MCOs could avoid enrolling individuals with serious behavioral health conditions because of excess costs (Horvitz-Lennon et al., 2022).
However, carve out arrangements have come under increasing scrutiny as the importance of integrating physical and behavioral health services has come to the fore. Carving behavioral health services out of Medicaid MCO plans creates silos in the financing and oversight of these two realms of health care delivery, which can result in barriers to effective service coordination and oversight (Charlesworth et al., 2021). Importantly, the proliferation of managed care has led to struggles with the implementation of the Mental Health Parity and Addiction Equity Act, as well as introduced difficulties with states monitoring the application of utilization management including quantitative (e.g., visit limits) and non-quantitative (e.g., prior authorization) treatment limitations as required by federal parity laws (CMS, 2016; MACPAC, n.d.a). Additionally, recent research has shown that the financial integration of both physical and behavioral health in Medicaid MCOs has been disruptive to providers while not appearing to drive significant clinical benefits for beneficiaries (McConnell et al., 2023). These ongoing issues highlight the challenges associated with separating administration of physical and behavioral health benefits.
While research on the impact of carve outs is limited, the research that does exist suggests that Medicaid MCO plans’ carve out structures may negatively impact access to behavioral health services, particularly in outpatient settings. Studies of MCO plans in Oregon (Charlesworth et al., 2021), Illinois (Xiang et al., 2019), and New York State (Frimpong et al., 2021) have all found evidence that MCO plans are associated with decreases in access to SUD care. Conversely, one study of managed care programs in Maryland and Nebraska found that carving out SUD services to FFS may be associated with increases in utilization. However, these increases were not equal across states and treatment types, resulting in variation both across and within states in terms of carve out structure (Auty et al., 2022). Additionally, recent commentaries have highlighted many of the methodological concerns with studying MCOs and carve out data, (Frank, 2021; Lindner, 2021), further emphasizing the importance of understanding the complex ways in which MCOs and carve outs impact their enrollees.
Despite research indicating that carve out structures influence access to behavioral health services, including SUD treatment, there has been little attention paid to understanding the extent and composition of Medicaid MCO plan carve outs for behavioral health, specifically within and between states. An analysis conducted by the Kaiser Family Foundation found that of the 41 state Medicaid programs that use comprehensive MCO plans in 2021, ten used primary carve outs for behavioral health, in which the administration of services is maintained typically by a state’s Medicaid FFS program. However, the report does not assess secondary carve outs, in which Medicaid MCO plans subcontract behavioral health out to BHOs, and it is unclear what services and medications are carved out in primary and secondary carve out agreements (Guth, 2021). This is a significant gap in the literature given that it is well known that MCO plans may use differential carve out strategies for outpatient and inpatient services, as well as for pharmacy benefits, often specifically for behavioral health (Hinton & Raphael, 2023).
We address this gap in the literature by examining carve out structures for SUD treatment services and medications using data from 70 comprehensive Medicaid MCO plans in 10 states. The goal of this analysis is to understand the complexity of Medicaid MCO plans across the country and to take a preliminary look at the variation both within and between states in terms of carve out structures. To do so, we explore the following questions: First, what proportion of Medicaid MCO plans in this sample use carve outs to administer SUD treatment? Second, what SUD treatment services and medications are most frequently carved out of comprehensive MCO plans? And finally, to which kinds of entities are SUD treatment and medications typically carved out? Answers to these questions are critical for understanding how these benefits are administered within the nation’s Medicaid program, and how the administration of benefits ultimately shapes how consumers navigate and experience treatment benefits.
2. METHODS
2.1. Data Source
The data for this study included publicly available information from 70 comprehensive Medicaid MCO plans in 10 states active in 2018 out of the 40 states including Washington, DC with MCO plans. Comprehensive MCO plans offer comprehensive acute care and may carve out specific services like behavioral health care to other organizations or fee-for-service (Hinton & Raphael, 2023). Selection for states was based on the completeness of coverage and accessible carve out data. More specifically, states were selected if they required any carve out for SUD treatment and that coverage information from the carve out entity could be found and examined. We defined SUD treatment as both SUD services and medications; therefore, we included states that carved out SUD services only, SUD medications only, and carved out both SUD services and medications. Since our study reviewed publicly available benefits, some states we identified with a carve out for SUD treatment had limited to no information publicly released from the carve out organization, making it difficult to access carve out coverage information. As a result, we selected states in which we were able to find complete coverage detail for each MCO plan and for the carve out entity or entities. These selected states included Florida, Georgia, Illinois, Maryland, Michigan, New Hampshire, Ohio, Pennsylvania, Utah, and West Virginia. These plans were identified using the Centers for Medicare and Medicaid Services’ 2018 Medicaid Managed Care Enrollment Report. When multiple Medicaid MCO plans were available for different enrollee groups with a single MCO in a state, we selected the largest-enrollment standard plan that served adult enrollees. We analyzed the following documents on MCO plan websites to identify behavioral health carve outs: member handbooks, provider manuals, and state formularies for all MCO plans for the 2018 contract year. In states in which SUD treatment was carved out to the state’s FFS plan, a behavioral health service organization, or other state entity, we identified the carve out entity’s benefits for SUD treatment by reviewing publicly-available benefits information on carve out organization’s websites and repeating the search process described above. The University of Chicago’s institutional review board approved this study and waived the requirement for informed consent because non–human participant data were used.
The procedure for determining the coverage and carve out structure for each state’s MCO plans included many distinct steps. From the start of the process (finding the state’s list of Medicaid MCO plans) to finish (downloading relevant provider manuals and, if necessary, searching websites for supplemental information), each MCO required a minimum of 12 steps to determine whether critical SUD services and medications were a) covered and b) carved out to a separate entity. This process was repeated for each MCO operating within each state. A more detailed depiction of the stepwise process used to identify these documents is described in Figure 1.
FIGURE 1:
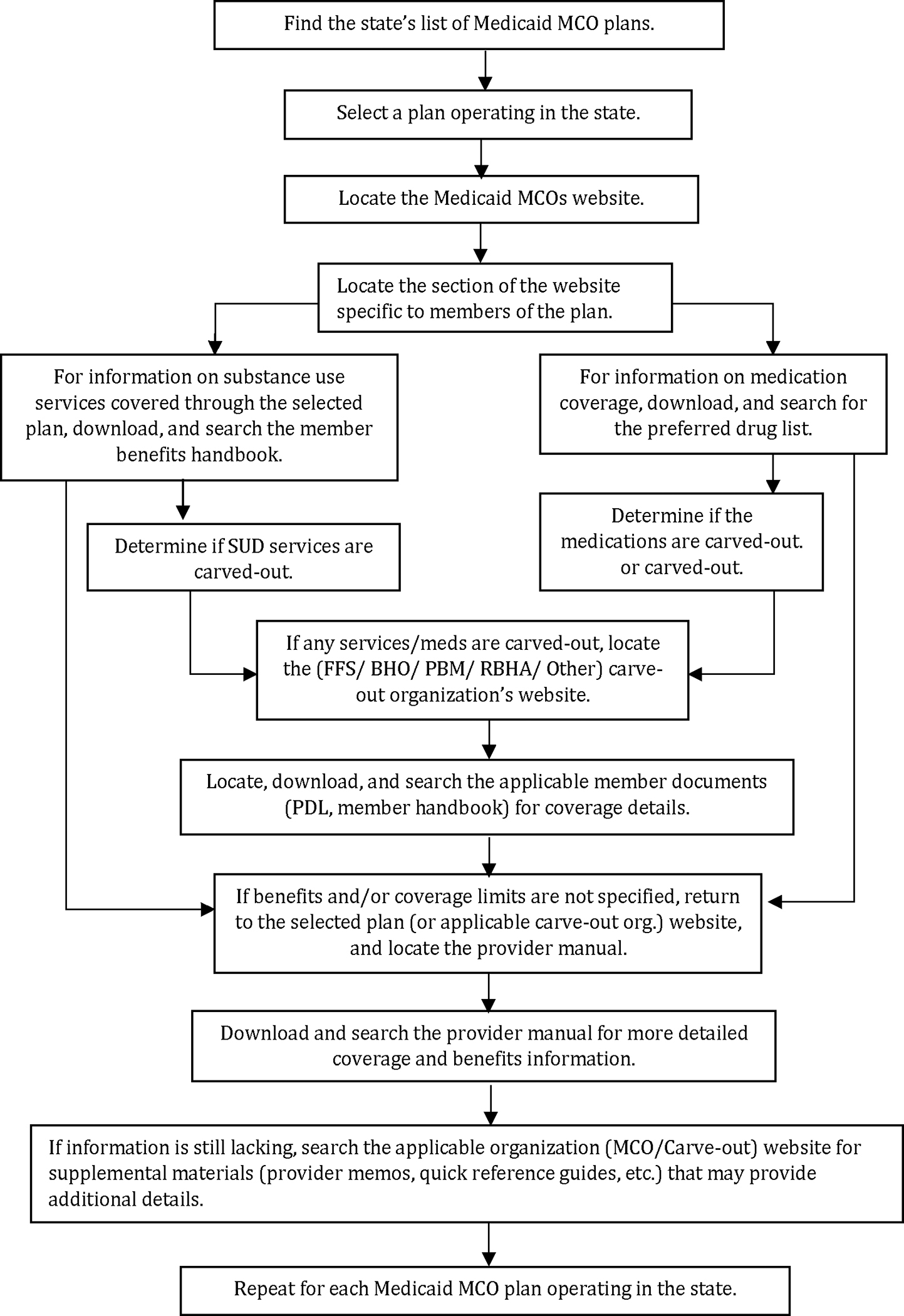
Stepwise Procedure for Identifying Medicaid Managed Care Plan Carve Out Structure
2.2. Study Measures
While carve outs have been a central feature of Medicaid MCOs since its inception, there have been many ways to define carve outs and these definitions have varied across sources and over time. Across research and practice, there is little consensus on how carve outs are defined and implemented, including carve outs to the state FFS Medicaid program. For the purposes of this analysis, we define any service carved out of the MCO plan, whether to the state FFS program or other entity (such as a BHO), as a carve out. We selected this approach due to the language used in the MCO plans (i.e., plans stating “carved out to state Medicaid plan”) and prior policy analysis suggesting that this is acceptable (MACPAC, n.d.b). We created dichotomous measures for carve-outs indicating that any service or medication specifically provided by the MCO itself was considered carved in and any service or medication provided through another entity was considered carved out. Additionally, we defined SUD treatment broadly as both SUD services and medications.
First, we determined which MCO plans utilized carve outs to cover any services or medications. More specifically, we examined if services and medications related to SUD treatment were described as carved-out to FFS, a BHO or other state entities from the MCO plan documents or MCO specific websites. The SUD services analyzed for carve outs included outpatient treatment, intensive outpatient treatment, residential treatment, and SUD assessment services. For medications, we examined both medications for opioid use disorder (i.e., methadone, buprenorphine, injectable naltrexone, and naloxone– an opioid overdose reversal medication) and alcohol use disorder (i.e., oral naltrexone, disulfiram and acamprosate). For the purpose of our study, methadone was included as a medication rather than a treatment service.
Next, we searched each MCO plan document for behavioral health coverage information. In each document obtained for review, we conducted searches using combinations of the terms “behavioral health,” “mental illness/health,” “drug,” “substance,” “chemical,” “alcohol, “use disorder,” “abuse,” “dependence,” and “addiction.” Data was coded to indicate whether each MCO plan reported coverage for each of the following services: assessments, outpatient treatment, intensive outpatient treatment, residential treatment, and inpatient hospitalizations. For services, coverage was indicated as being provided, not provided, or not specified. “Not specified” was coded in cases in which none of the MCO plan records indicate whether a given service was covered or not. We also coded whether each MCO plan’s formulary included FDA-approved medications for opioid use disorder and medications for alcohol use disorder: methadone, naloxone, injectable naltrexone, oral naltrexone, buprenorphine, disulfiram, and acamprosate. Since methadone is not always listed on plan formularies for opioid use disorders, we included methadone as a search term in the general plan documents as well. For medications, we coded any listed on the formulary as being covered and any not listed as not being covered. In plans that we identified a carve out for some or all services, a carve out for some or all medications, or a carve out for medications and services, we repeated our search process by additionally analyzing each carve out document for additional behavioral health coverage information.
2.3. Analysis
We calculated descriptive statistics for all study variables related to coverage and carve out structure to better understand the relationship between carve outs, services, and medications for SUD in Medicaid MCO plans. Specifically, we assessed if all SUD treatment services were carved in, carved out, or if only some (at least one) were carved out in a plan. Similarly, we assessed if none, any, or all SUD medications were carved out. These three groups are mutually exclusive, with plans being designated either fully carved out, partially carved out, or fully carved in for both services and medications. Second, we calculated the percentages of plans that clearly specified the coverage of SUD services and medications; by doing this, we were able to assess how clear these coverage documents were in specifying if a service or medication was or was not covered in the plan. Finally, we determined the carve out structure of each service and medication (i.e., to which organization the services and medications were carved out) to assess variation both within and across services and medications in terms of carve outs to BHOs, FFS, and other entities.
3. RESULTS
3.1. Overall Carve Out Structure
Overall, the vast majority of Medicaid MCO plans employed at least some form of carve out arrangement for SUD services and medications. In total, 40.0% (n=28) of plans carved out all SUD services and 14.3% (n=10) of plans carved out all SUD medications, with an additional 28.6% (n=20) of plans carving out some SUD services and 77.1% (n=54) carving out some SUD medications. Therefore, a total of 61.5% (n=48) of plans had some form of carve out in place for services while 91.4% (n=64) had some form of carve out arrangement for SUD medications (Figure 2). Very few plans (n=4, 5.7%) did not utilize any carve out arrangements, including three plans in Georgia and one in Ohio.
FIGURE 2:
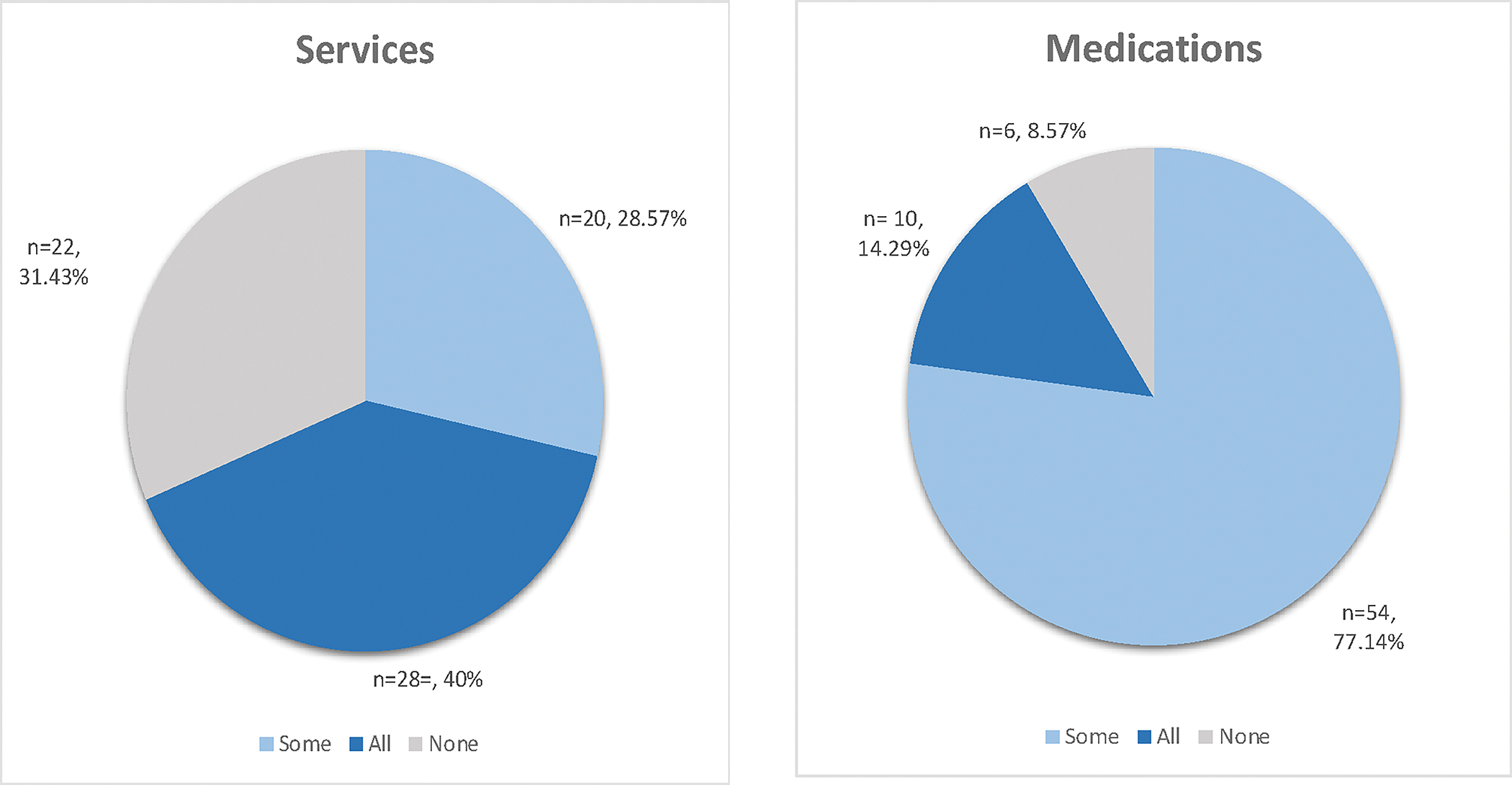
Substance Use Disorder Treatment Carve Out Structure in Medicaid Managed Care Plans
Of note, not all plans covered all services and medications. For services, inpatient hospitalization was most frequently covered (n=68), followed by IOP (n=60), outpatient (n=59), assessment (n=56), and residential (n=54). Outpatient hospitalization (n=51) was the least frequently covered. For medications, buprenorphine was covered by all (n=70) plans, followed closely by naloxone (n=68), and oral naltrexone (n=65). Methadone, injectable naltrexone, and disulfiram were all covered by the same number of plans (n=62) and acamprosate was the least covered of all medications (n=55).
Table 2 provides full details on carve out structure for SUD treatment. There was wide variation both between and within states in terms of the frequency of carve outs for SUD treatment. For example, in Maryland, 100.0% of MCO plans carved out all SUD treatment. In contrast, plans in Ohio carved-in all services and medications except for methadone. Additionally, the frequency of carve outs for different types of services and medications varied widely. The most frequently carved out service was residential services (72.2% of plans that covered residential services carved it out) while the least frequently carved out service was assessment (53.8% of plans that covered assessment services carved it out). The variation for medication carve outs was even more stark, with 95.2% of plans that covered methadone carving it out, while only 20.6% of plans that covered naloxone covered this medication (Table 2). Importantly, not all plans included carve outs for both services and medications. While the majority of plans (67.1%, n = 47) carved out both services and medications, 22.9% (n=16) only included carve outs for medications (mainly for methadone), and only one plan (1.4%) carved out only services. An additional 8.6% of plans (n=6) did not have any services or medications carved out.
TABLE 2:
Percent of Managed Care Plans Carving Out SUD Treatment Services and Medications by State
| Type | FL (n=15) | GA (n=4) | IL (n=7) | MD (n=9) | MI (n=11) | NH (n=2) | OH (n=5) | PA (n=9) | WV (n=4) | UT (n=4) | Tot. (n=70) |
|---|---|---|---|---|---|---|---|---|---|---|---|
| Services | % | % | % | % | % | % | % | % | % | % | % |
| Assessment | 54 | 25 | 20 | 100 | 100 | 100 | 0 | 0 | 0 | 100 | 54 |
| Outpatient | 69 | 25 | 14 | 100 | 100 | 100 | 0 | 100 | 25 | 100 | 69 |
| Outpatient Hosp. | 67 | 33 | 14 | 100 | 100 | 100 | 0 | 0 | 0 | 100 | 67 |
| Intensive Outpt. | 70 | 25 | 14 | 100 | 100 | 100 | 0 | 100 | 33 | 0 | 68 |
| Inpatient Hospital | 25 | 25 | 14 | 100 | 100 | 100 | 0 | 100 | 25 | 100 | 66 |
| Residential | 60 | 33 | 14 | 100 | 100 | 100 | 0 | 100 | 100 | 0 | 72 |
| Medications | % | % | % | % | % | % | % | % | % | % | % |
| Methadone | 100 | 0 | 83 | 100 | 100 | 100 | 80 | 100 | 0 | 100 | 95 |
| Inj. naltrexone | 7 | 0 | 0 | 100 | 100 | 0 | 0 | 0 | 100 | 100 | 47 |
| Buprenorphine | 7 | 0 | 0 | 100 | 100 | 0 | 0 | 0 | 100 | 100 | 41 |
| Oral Naltrexone | 7 | 0 | 0 | 100 | 100 | 0 | 0 | 0 | 0 | 75 | 37 |
| Disulfiram | 7 | 0 | 0 | 100 | 100 | 0 | 0 | 0 | 0 | 0 | 34 |
| Acamprosate | 7 | 0 | 0 | 100 | 100 | 0 | 0 | 0 | 0 | 0 | 38 |
| Naloxone | 7 | 0 | 0 | 100 | 0 | 0 | 0 | 0 | 100 | 0 | 21 |
Number of plans that covered each service and medication: Assessment (n = 56), Outpatient (n=59), Outpatient Hospitalization (n=51), Intensive Outpatient (n=60), Inpatient Hospital (n=68), Residential (n=54), Methadone (n=62), Injectable Naltrexone (n=62), Buprenorphine (n=70), Oral Naltrexone (n=65), Disulfiram (n=62), Acamprosate (n=55), and Naloxone (n=68)
3.2. Carve Out Arrangements
There was a marked difference in the structure of the receiving entities for carve outs of the selected SUD services and medications. When services were carved out, the receiving entity was most frequently a BHO such as Beacon or Cenpatico. SUD services most frequently carved out to BHOs were residential care (38.9%), intensive outpatient services (37.7%), and outpatient care (36.8%). Carve outs to an FFS Medicaid plan were most common for inpatient hospitalization services (25.4%), but far less common for assessment (7.1%), outpatient (5.9%), and outpatient hospitalization (7.7%). No Medicaid MCO plans carved out intensive outpatient or residential services to FFS (Figure 3).
FIGURE 3:

Receiving Entities of Managed Care Plan Benefit Carve Outs by Service and Medication Type
In addition to carve outs to either a Medicaid FFS plan or BHO, we found that some MCOs carved out to a combination-type FFS and BHO arrangement. For example, Maryland has a BHO serve as the administrative manager for the state public behavioral health system, so some services are carved out through both a BHO and FFS system. Plans most frequently used this combination-type carve out structure for hospitalizations, with 17.3% of plans carving out outpatient hospitalization and 15.3% of plans carving out inpatient hospitalization in this way. In addition, 10.7% of both assessment and residential services, 8.8% of outpatient services, and 9.8% of intensive outpatient services used a combination of BHO and FFS carve outs.
Finally, some of the MCO’s carved-out to “other” entities. For example, Michigan carved-out services to Prepaid Inpatient Health Plans (PIHPs). In all, an additional 21.4% of assessment, 17.6% of outpatient, 23.1% of outpatient hospitalization, 19.7% of inpatient hospitalization, and 22.2% of residential services were carved out to entities other than a BHO, state Medicaid FFS plan, or a combination of the two. Finally, among services that remained carved in to the MCO plan, assessment (37.5%) was the most frequent. Residential treatment was the service least likely to be carved in to MCO plans (27.8%).
With the exception of methadone, carve out structures for medications for opioid and alcohol use disorder were very different from that of services. Only 9.7% of plans that covered medications carved medications out to BHOs. A majority of Medicaid MCO plans carved in medications, ranging from 53.2% for injectable naltrexone to 75.4% for naloxone. When these medications were carved out, MCO plans most often used carve outs to state Medicaid FFS plans, ranging from 22.8% for naloxone to 45.2% for injectable naltrexone. Combination strategies including elements of BHO and FFS involvement were rarely used for medication carve outs. Only methadone was carved out in this manner, with 14.5% of plans carving out methadone to a combination of BHO and FFS, and 8.1% carving out to an “other” entity such as a PIHP.
4. DISCUSSION
This is the first study to our knowledge to examine the variation of Medicaid MCO carve out structure, both within and across states. The goal of this analysis was to gain a greater understanding on the scope of complexity of the carve out structures used by Medicaid MCO plans by using data provided by plans that are made available to Medicaid MCO beneficiaries. By analyzing the types of treatment that MCO plans are carving out, along with the distinction between medication and service carve outs and the types of entities to which they are being carved out, such as BHOs, FFS, and other third-party organizations, we aimed to further understand the wide range of arrangements of Medicaid MCO plans into which a beneficiary could be entered.
The findings of this study illustrate the complexity of Medicaid MCO carve out arrangements for administering SUD treatment benefits. Notably, there was substantial variation in the number and type of both SUD treatment services and medications that are carved out from MCO plans, and in the entities to which services and medications were carved out, both within and between states. MCO plans in some states in our sample, such as Maryland and Michigan, consistently carved out all services. Other states carved in all services (e.g., Ohio), or all medications (e.g., Georgia). Some states, such as Florida, had little consistency across plans with regard to what was carved out.
Our study findings also suggest that comprehensive MCO plans are less likely to manage SUD treatment services than medications. Excluding methadone—which is typically billed as a treatment service—MCO plans were more likely to carve-in SUD medications and more likely to carve out SUD services. Importantly, utilization management techniques such as prior authorization are widespread both for medications managed under MCOs (Abraham et al., 2022) as well as those billed directly to state Medicaid FFS programs (Shoulders et al., 2023). Furthermore, carve out arrangements for SUD services consisted of a broader array of carve out entities than seen with medication carve outs. This is likely due to the greater complexity involved in managing SUD service benefits, particularly those services that are more intensive such as residential and inpatient care. The far higher costs that are involved in delivering more intensive treatment services place a greater financial risk on MCO plans than medications typically do.
Our findings—which document widespread, yet highly varied use of carve out arrangements—raise important concerns regarding equitable access to care. Existing research is mixed on whether Medicaid managed care plans alone improve access to care (Franco Montoya et al., 2020). While research from 2007 revealed that carve outs are generally associated with maintaining or improving access to care (Frank & Garfield, 2007), more recent research after the passing of the Affordable Care Act has shown that the use of carve outs is associated with reduced access to SUD treatment. Charlesworth and colleagues (2021) found that enrollees in an Oregon-based Medicaid MCO plan that carved out behavioral health benefits were less likely to receive behavioral health services than enrollees in a similar plan that carved in behavioral health. In Illinois, Xiang and colleagues (2019) found that eliminating an existing carve out for behavioral health benefits resulted in significant increases in health care utilization. A similar evaluation to integrate administration of physical and behavioral health benefits in New York also found that when carve outs were eliminated, outpatient behavioral health utilization increased, while avoidable hospitalizations decreased (Frimpong et al., 2021).
Given that carve out arrangements can vary substantially, and that most enrollees are auto assigned into an MCO plan, enrollees randomly placed into plans subject to carve out arrangements may experience more difficulties in accessing treatment than enrollees placed into plans that do not use carve outs. Research has shown that switching from carve out plans to carve-in models was associated with increased access to care among those who used to be enrolled in carve out models (Ettner et al., 2019), which indicates that there could be important policy barriers to care for enrollees placed into more carve out-heavy MCOs. One study also documented differences in enrollment in carve-in versus carve-out arrangements by race and ethnicity, finding that carving in behavioral health services to the managed care plan is associated with improved access for Black beneficiaries (Charlesworth et al., 2021). These findings raise important questions regarding equitable access to treatment across enrollees in Medicaid MCO plans.
Additionally, there have been many important developments related to carve out structures within the past years. Namely there has been a push by states to integrate behavioral health care into Medicaid managed care contracts, along with movement for carving in pharmacy benefits and long-term services and supports (Hinton & Raphael, 2023). Much of this momentum to move toward a carve-in structure is due to the mixed evidence on carve outs for enrollees with behavioral health conditions, along with the administrative burden on states associated with entering into multiple contracts with MCOs (Horvitz-Lennon et al., 2022). Although many states have moved toward carving in and integrating behavioral health services, they still allow subcontracting at the MCO level. Through these secondary carve out arrangements, the state contracts with MCOs for comprehensive behavioral and primary health care, but the behavioral health services are contracted out by the MCO to another entity, such as a BHO, resulting in a de facto carve out arrangement at the plan, rather than state, level (McConnell et al., 2021). Thus, while only 11 states have primary carve out arrangements through which some or all outpatient or inpatient SUD services were carved out of MCOs at the state level (Gifford et al., 2019), significant variation still exists in terms of secondary carve out arrangements at the plan level, as evidenced by our results.
Given that carve out arrangements are so widespread in the management of SUD treatment by Medicaid MCOs, future research should examine the factors that influence Medicaid MCO plans’ decisions to carve out some versus all services and medications. Little is known regarding why Medicaid MCO plans set up the carve out arrangements they do, and what plans perceive as the benefits of doing so. Further research is also needed to understand the consequences of these kinds of arrangements. Recent studies on this topic have focused solely on access to outpatient SUD treatment, and little is known about the effects of carve outs on receipt of SUD treatment medications and more intensive services. Related to this, it is important to discern whether specific carve out entities, such as carving out to the state FFS or to BHOs, provide better access to care and improved outcomes, and if so, why.
Finally, it is important to note the implications that these findings have for Medicaid researchers. Only five states (Alaska, Connecticut, Maine, Vermont, and Wyoming) have 100% of Medicaid beneficiaries receiving services through FFS (Kaiser Family Foundation, 2023). Thus, inclusion of the managed care population when attempting to assess Medicaid coverage and outcomes is critical. However, the findings of our study illuminate the complexity involved in doing so, as accurate measurement necessitates the inclusion of the sub-contractual arrangements deployed by these organizations to manage and deliver services and medications via carve outs. Importantly, Transformed Medicaid Statistical Information System (T-MSIS) Analytic Files (TAF) include both FFS and MCO data. Collecting data on plan characteristics as we have done in this analysis allows researchers to merge data with claims for future research to begin to understand the impact of carve out arrangements on enrollee utilization and outcomes. Failure to take this into account will likely result in an incomplete picture of Medicaid coverage, poor measurement, and inaccurate findings.
4.1. Limitations
There are several limitations to our study. First, due to the time constraints involved in extracting these data through an extremely time-intensive process, we selected 10 states in this analysis rather than all states that had at least one comprehensive MCO plan in 2018. As a result, it is possible that the selected states in this study oversample those that always carve out SUD treatment and this study will not necessarily be generalizable to other states and MCO plans. However, this was a preliminary attempt at examining these plan variations to provide evidence for a study into the full national scope, rather than a study aimed at generalizability to all states and MCO plans. Secondly, our study is limited to only 2018 coverage; however, this is the first study to our knowledge that looks at coverage documents to identify the coverage and carve out arrangement of Medicaid MCO plans and one of the main goals of this study was to gather more information on the scope of variability both within and between states’ MCO plans. Although the data are from 2018 and may therefore not represent the current state of each MCO plan analyzed, it is important to note that these results characterize the variation in structure at large, which is likely pertinent to this day. Third, this study relies on documents that are released to the public; therefore, it is possible that some of the coverage that we identified as not specified during our analysis are actually specified elsewhere in plan documents that were not publicly available.
5. CONCLUSION
The use of carve outs to manage and deliver behavioral health services has been linked to reduced treatment access. Despite this, our findings indicate that carve outs are extremely common within Medicaid managed care. This is concerning given that over 70% of all Medicaid enrollees receive services and medications through a Medicaid managed care plan. While efforts to carve in behavioral health services have increased in recent years in response to growing recognition of the issues that stem from segregating SUD treatment administration, our findings shed light on the significant amount of work that remains to be done to reintegrate behavioral health into mainstream medical care. In light of the epidemic of addiction currently faced by the United States, efforts to increase treatment access by reducing the use of carve outs to serve this high need and high-risk population is of critical importance.
TABLE 1:
Medicaid Managed Care Plans Included in the Study (n=70)
| STATE | MANAGED CARE PLAN | STATE | MANAGED CARE PLAN |
|---|---|---|---|
| Florida | AHF/Positive Healthcare | Michigan | Aetna Better Health of Michigan |
| Amerigroup Florida, Inc. | Blue Cross Complete of Michigan | ||
| Better Health | HAP Midwest Health Plan, Inc. | ||
| Aetna Better Health of Florida | Harbor Health Plan | ||
| Freedom Health, Inc. | McLaren Health Plan | ||
| Humana Medical Plan | Meridian Health Plan of Michigan | ||
| Magellan Complete Care, LLC | Molina Healthcare of Michigan | ||
| Molina Healthcare of Florida | Priority Health Choice, Inc. | ||
| Prestige Health Choice | Total Health Care | ||
| Simply DBA Clear Health Alliance | UnitedHealthcare Community Plan | ||
| Simply Healthcare Plans, Inc. | Upper Peninsula Health Plan | ||
| South Florida Community Care | New Hampshire | New Hampshire Healthy Families | |
| Staywell Health Plan of Florida | Well Sense Health Plan | ||
| Sunshine State Health Plan, Inc. | Ohio | Buckeye Community Health Plan | |
| UnitedHealthcare of Florida | CareSource | ||
| Georgia | Amerigroup Community Care | Molina HealthCare | |
| CareSource | Paramount Advantage | ||
| Peach State Health Plan | UnitedHealthcare Community Plan | ||
| WellCare | Pennsylvania | Aetna Better Health | |
| Illinois | Blue Cross Community Plan | AmeriHealth Caritas Pennsylvania | |
| County Care | AmeriHealth Northeast | ||
| Harmony Health Plan | Gateway Health | ||
| IllniCare Health | Geisinger Health Plan | ||
| Meridian Health Plan | Health Partners Plans | ||
| Molina Healthcare | Keystone First | ||
| Next Level | UnitedHealthcare Community Plan | ||
| Maryland | Aetna Better Health | UPMC Health Plan | |
| Amerigroup Community Care | Utah | HealthChoice Utah | |
| Jai Medical Systems | Healthy U | ||
| Kaiser Permanente | Molina Healthcare | ||
| Maryland Physicians Care | SelectHealth Community Care | ||
| MedStar Family Choice | West Virginia | Aetna Better Health of WV | |
| Priority Partners | Health Plan of Upper Ohio Valley | ||
| UnitedHealthcare Community Plan | Unicare | ||
| Univ. of Maryland Health Partners | West Virginia Family Health |
Highlights:
There is wide variation in carve outs from Medicaid MCO plans for SUD treatment
Comprehensive MCO plans are less likely to manage SUD services than medications
SUD services were carved out to a wide array of third-party entities
Funding Source:
This work was supported by the National Institute on Alcoholism and Alcohol Abuse (R01AA029097) and the National Institute on Drug Abuse (R01DA052425)
Footnotes
Declarations of interest: none
Publisher's Disclaimer: This is a PDF file of an unedited manuscript that has been accepted for publication. As a service to our customers we are providing this early version of the manuscript. The manuscript will undergo copyediting, typesetting, and review of the resulting proof before it is published in its final form. Please note that during the production process errors may be discovered which could affect the content, and all legal disclaimers that apply to the journal pertain.
REFERENCES
- Abraham AJ, Andrews CM, Harris SJ, Westlake MM, & Grogan CM (2022). Coverage and prior authorization policies for medications for opioid use disorder in Medicaid managed care. JAMA Health Forum, 3(11), e224001. 10.1001/jamahealthforum.2022.4001 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Auty SG, Cole MB, & Wallace J (2022). Association between Medicaid managed care coverage of substance use services and treatment utilization. JAMA Health Forum, 3(8), e222812. 10.1001/jamahealthforum.2022.2812 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Centers for Disease Control and Prevention. (2022, May 11). U.S. Overdose Deaths in 2021 Increased Hald as Much as in 2020—But Are Still p 15%. National Center for Health Statistics. https://www.cdc.gov/nchs/pressroom/nchs_press_releases/2022/202205.htm [Google Scholar]
- Charlesworth CJ, Zhu JM, Horvitz-Lennon M, & McConnell KJ (2021). Use of behavioral health care in Medicaid managed care carve-out versus carve-in arrangements. Health Services Research, 56(5), 805–816. 10.1111/1475-6773.13703 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Centers for Medicare and Medicaid Services (CMS) (2016, June 1). Warning Signs—Plan or Policy Non-Quantitative Treatment Limitations (NQTLs) that Require Additional Analysis to Determine Mental Health Parity Compliance. https://www.cms.gov/cciio/resources/regulations-and-guidance/downloads/mhapeachecklistwarningsigns.pdf
- CMS. (2023). September 2023 Medicaid & CHIP Enrollment Data Highlights. https://www.medicaid.gov/medicaid/program-information/medicaid-and-chip-enrollment-data/report-highlights/index.html
- Ettner SL, Xu H, & Azocar F (2019). What happens when employers switch from a “carve-out” to a “carve-in” model of managed behavioral health? The Journal of Mental Health Policy and Economics, 22(3), 85–94. [PubMed] [Google Scholar]
- Franco Montoya D, Chehal PK, & Adams EK (2020). Medicaid managed care’s effects on costs, access, and quality: An update. Annual Review of Public Health, 41(1), 537–549. 10.1146/annurev-publhealth-040119-094345 [DOI] [PubMed] [Google Scholar]
- Frank RG (2021). Behavioral health carve-outs: Do they impede access or prioritize the neediest? Health Services Research, 56(5), 802–804. 10.1111/1475-6773.13704 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Frank RG, & Garfield RL (2007). Managed behavioral health care carve-outs: Past performance and future prospects. Annual Review of Public Health, 28, 303–320. 10.1146/annurev.publhealth.28.021406.144029 [DOI] [PubMed] [Google Scholar]
- Frimpong EY, Ferdousi W, Rowan GA, & Radigan M (2021). Impact of the 1115 behavioral health Medicaid waiver on adult Medicaid beneficiaries in New York State. Health Services Research, 56(4), 677–690. 10.1111/1475-6773.13657 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Gifford K, Ellis E, Lashbrook A, Nardone M, Hinton E, Rudowitz R, Diaz M, & Tian M (2019, October 18). A view from the states: Key Medicaid policy changes: Results from a 50-state Medicaid budget survey for state fiscal years 2019 and 2020. Kaiser Family Foundation. https://www.kff.org/report-section/a-view-from-the-states-key-medicaid-policy-changes-delivery-systems/ [Google Scholar]
- Guth M (2021, December 9). State policies expanding access to behavioral health care in Medicaid. Kaiser Family Foundation. https://www.kff.org/medicaid/issue-brief/state-policies-expanding-access-to-behavioral-health-care-in-medicaid/ [Google Scholar]
- Hinton E, & Raphael J (2023, March 1). 10 things to know about Medicaid managed care. Kaiser Family Foundation. https://www.kff.org/medicaid/issue-brief/10-things-to-know-about-medicaid-managed-care/ [Google Scholar]
- Horvitz-Lennon M, Levin JS, Breslau J, Kushner J, Eberhart NK, & Bhandarkar M (2022). Carve-in models for specialty behavioral health services in Medicaid: Lessons for the state of California. RAND Corporation. https://www.rand.org/pubs/research_reports/RRA1517-1.html [Google Scholar]
- Kaiser Family Foundation. (2022a, August 4). Total Medicaid MCO enrollment. State Health Facts. https://www.kff.org/other/state-indicator/total-medicaid-mco-enrollment/ [Google Scholar]
- Kaiser Family Foundation. (2022b, August 4). Total Medicaid MCOs. State Health Facts. https://www.kff.org/medicaid/state-indicator/total-medicaid-mcos/ [Google Scholar]
- Kaiser Family Foundation. (2023). Share of Medicaid population covered under different delivery systems. https://www.kff.org/medicaid/state-indicator/share-of-medicaid-population-covered-under-different-delivery-systems/?currentTimeframe=0&sortModel=%7B%22colId%22:%22Location%22,%22sort%22:%22asc%22%7D
- Lindner S (2021). Comment on Frimpong et al.: Impact of the 1115 behavioral health Medicaid waiver on adult Medicaid beneficiaries in New York State (SSRN Scholarly Paper 3862895). 10.2139/ssrn.3862895 [DOI] [PMC free article] [PubMed]
- Lyden J, & Binswanger IA (2019). The United States opioid epidemic. Seminars in Perinatology, 43(3), 123–131. 10.1053/j.semperi.2019.01.001 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Mark TL, Levit KR, Yee T, & Chow CM (2014). Spending on mental and substance use disorders projected to grow more slowly than all health spending through 2020. Health Affairs (Project Hope), 33(8), 1407–1415. 10.1377/hlthaff.2014.0163 [DOI] [PubMed] [Google Scholar]
- McConnell KJ, Edelstein S, Hall J, Levy A, Danna M, Cohen DJ, Lindner S, Unützer J, & Zhu JM (2023). The effects of behavioral health integration in Medicaid managed care on access to mental health and primary care services-Evidence from early adopters. Health Services Research, 58(3), 622–633. 10.1111/1475-6773.14132 [DOI] [PMC free article] [PubMed] [Google Scholar]
- McConnell KJ, Hall J, Linder S, Unützer J, Zier S, Zhu J, & Cohen D (2021). Financial integration of behavioral health in Medicaid managed care organizations: A new taxonomy [Issue Brief]. https://www.ohsu.edu/sites/default/files/2021-05/McConnell%20et%20al.%20Financial%20Integration%20of%20Behavioral%20Health%20in%20Medicaid.pdf
- Medicaid and CHIP Payment and Access Commission [MACPAC]. (n.d.a). Key federal program accountability requirements in Medicaid managed care.. Retrieved May 3, 2022, from https://www.macpac.gov/subtopic/key-federal-program-accountability-requirements-in-medicaid-managed-care/
- MACPAC. (n.d.b). Types of managed care arrangements.. Retrieved May 3, 2022, from https://www.macpac.gov/subtopic/types-of-managed-care-arrangements/
- National Institute on Alcohol Abuse and Alcoholism. (2023, April 12). Alcohol-related deaths, which increased during the first year of the COVID-19 pandemic, continued to rise in 2021. https://www.niaaa.nih.gov/news-events/research-update/alcohol-related-deaths-which-increased-during-first-year-covid-19-pandemic-continued-rise-2021
- Open Minds. (2016). Which state Medicaid plans carve-out behavioral health benefits? [Market Intelligence Report]. Open Minds. https://openminds.com/store/state-medicaid-plans-carve-addiction-treatment-services-open-minds-market-intelligence-report/ [Google Scholar]
- Saunders H (2023, February 17). A look at substance use disorders (SUD) among Medicaid enrollees. Kaiser Family Foundation. https://www.kff.org/mental-health/issue-brief/a-look-at-substance-use-disorders-sud-among-medicaid-enrollees/ [Google Scholar]
- Shoulders A, Andrews CM, Westlake MA, Abraham AJ, & Grogan CM (2023). Changes in Medicaid fee-for-service benefit design for substance use disorder treatment during the opioid crisis, 2014 to 2021. JAMA Health Forum, 4(8), e232502. 10.1001/jamahealthforum.2023.2502 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Substance Abuse and Mental Health Services Administration. (2021). Key substance use and mental health indicators in the United States: Results from the 2020 National Survey on Drug Use and Health (HHS Publication No. PEP21–07-01–003; NSDUH Series H-56). Center for Behavioral Health Statistics and Quality, Substance Abuse and Mental Health Services Administration. https://www.samhsa.gov/data [Google Scholar]
- US Department of Health & Human Services. (2016). Facing addiction in America: The Surgeon General’s report on alcohol, drugs, and health. Office of the Surgeon General. https://addiction.surgeongeneral.gov/ [PubMed] [Google Scholar]
- Xiang X, Owen R, Langi FLFG, Yamaki K, Mitchell D, Heller T, Karmarkar A, French D, & Jordan N (2019). Impacts of an integrated Medicaid managed care program for adults with behavioral health conditions: The experience of Illinois. Administration and Policy in Mental Health, 46(1), 44–53. 10.1007/s10488-018-0892-8 [DOI] [PMC free article] [PubMed] [Google Scholar]