

Abstract
Background and Objective
Preliminary evidence suggests a possible preventive effect of tumor necrosis factor-α inhibitors (TNFi) on incident dementia. The objective of the analysis was to investigate the association between TNFi and the risk of incident dementia in a population undergoing treatment for rheumatological disorders.
Methods
We followed patients aged ≥ 65 years with dementia and rheumatological conditions in two cohort studies, DANBIO (N = 21,538), a Danish clinical database, and AOK PLUS (N = 7112), a German health insurance database. We defined incident dementia using diagnostic codes and/or medication use and used Cox regression to compare the associations of TNFi with other rheumatological therapies on the risk of dementia. To ensure that the patients were receiving long-term medication, we included patients with rheumatic diseases and systemic therapies.
Results
We observed similar trends towards a lower risk of dementia associated with TNFi versus other anti-inflammatory agents in both cohorts (hazard ratios were 0.92 [95% confidence interval 0.76, 1.10] in DANBIO and 0.89 [95% confidence interval 0.63, 1.24] in AOK PLUS, respectively).
Conclusions
Tumor necrosis factor-α inhibitors may decrease the risk of incident dementia although the association did not reach statistical significance in this analysis. Further research, ideally with randomization, is needed to gauge the potential of repurposing TNFi for dementia prevention and/or treatment.
Supplementary Information
The online version contains supplementary material available at 10.1007/s40266-024-01112-1.
Key Points
| In this study, conducted in a Danish clinical database for rheumatological patients and a large German health insurance database, we observed a trend towards a lower risk of dementia among patients treated with tumor necrosis factor-α inhibitors versus patients treated with other anti-inflammatory drugs. |
| Further clinical trials and cohort studies are needed to clarify the potential of tumor necrosis factor-α inhibitors for the prevention of incident dementia or its progression. |
Background
Dementia and related disorders, including Alzheimer’s disease (AD), are estimated to affect 10% of adult men and 20% of adult women during their lifetimes and represent the fifth most common cause of death globally [1–3]. Given the absence of any proven preventative therapies, novel approaches to reduce the incidence and progression of AD and other dementias are urgently needed.
One intriguing direction for novel dementia therapies relates to the observation that inflammation may play a role in the pathophysiology of neurodegenerative diseases [4–7]. Higher levels of the proinflammatory cytokine tumor necrosis factor (TNF)-α in patients with AD are associated with accelerated cognitive decline [8], and unpublished findings from the pharmaceutical company Pfizer Inc. suggest that the immunosuppressive TNF-α inhibitor (TNFi) etanercept may lower the risk for AD [9]. However, only one small trial with etanercept has been published among patients with AD, and no statistically significant changes in cognition, behavior, or global function were observed [10].
Tumor necrosis factor-α is also known to play an important role in autoimmune disorders, and TNFi treatment is often used as treatment for rheumatological disorders such as rheumatoid arthritis (RA), spondyloarthritis (SA), and psoriatic arthritis (PsA). Studying the effect of systemic treatment with TNFi drugs on the risk of dementia among patients with such autoimmune disorders may represent an avenue to gain important insights into the role of inflammation in the development of dementia with the potential for prevention and treatment. In observational studies relating anti-inflammatory medication use with dementia risk in patients with RA, findings have been mixed with either a lower risk among users or null associations [11–16].
Thus, while TNFi might be a candidate for the treatment of dementia, additional studies are warranted, especially with a larger sample size and a longer duration of follow-up. Therefore, we aimed to investigate the association between the prescription of TNFi drugs and incident dementia in patients with rheumatological disorders aged ≥ 65 years in two national population-based cohort studies: The Danish Rheumatological Database (DANBIO), a clinical database for rheumatological patients for the period 2000–2018, and AOK PLUS, a large German health insurance database for the period 2005–2014.
Study Design and Methods
Study Populations
DANBIO Study
DANBIO has been described elsewhere [17–19]. In brief, DANBIO is a nationwide clinical database on rheumatology founded in 2000 that consists of reporting from patients and healthcare professionals in Denmark. In 2006, it was approved as a clinical quality database by the Danish National Board of Health, mandating registration of all patients with RA, regardless of their treatment, for all public and private hospitals. Thus, patient consent is not required for registration. Patients with rheumatological conditions are recorded in the database when they receive the first diagnosis or at the time when they receive a prescription for medical treatment. Thus, the baseline for each participant is at the time of first registration in DANBIO. Before a consultation, the patients receive a questionnaire regarding their rheumatic disease. Information on the patient’s disease activity, treatment, treatment effect, and adverse events during treatment is registered in the database by the patient and healthcare provider, usually two times a year. If patients discontinue their treatment, the cause is registered in the database, and if the patient changes treatment, it will lead to a new baseline in the register. As rheumatological disorders are chronic non-curable diseases, patients are registered on a lifelong basis.
In the cohort study based on the DANBIO database, individuals were followed from the 1 January, 2000 until the 31 December, 2018. Exclusion criteria included: individuals aged < 65 years, diagnosis of dementia before study entrance, no drug treatment of interest during the study period, or a diagnosis of HIV (International Classification of Diseases, Tenth Revision [ICD-10] codes: B20-B24, Z21, R75) and/or previous organ transplantation (ICD-10 codes: Z94.1-9) because these events are associated with increased levels of TNF-α.
AOK PLUS Study
This cohort study used the AOK PLUS database provided by a large statutory health insurer in Germany that accords with §295, §300, and §301 of the German Social Security Code V. AOK PLUS holds complete information on outpatient healthcare using diagnoses based on the ICD, prescriptions according to the Anatomical Therapeutic Chemical classification, and sociodemographic characteristics of the insured population. The AOK PLUS database has previously been described [20, 21]. At the time of the study, the total number of individuals in AOK PLUS consisted of 650,468 insured individuals aged ≥ 65 years.
In the AOK PLUS study, individuals with rheumatological disorders (RA ICD-10 code M06, SA ICD-10 code M45, and PsA ICD-10 code L40.5) were included and followed from the 1 January, 2005 until the 31 December, 2014. Exclusion criteria were the same as for DANBIO. In addition, for the AOK PLUS study, already deceased insured patients were excluded.
Definition of Drug Exposure
We used commonly prescribed rheumatological drugs based on established treatment guidelines [22]. In both cohorts, the primary exposure of interest was treatment with TNFi (adalimumab, certolizumab, etanercept, golimumab, and infliximab). The exposure had to be present before the dementia diagnosis. Rheumatological treatment with first-line anti-inflammatory drugs was included for comparison, including other biologics not targeting TNF-α, non-steroidal anti-inflammatory drugs, corticosteroids, and disease-modifying antirheumatic drugs. Drugs were classified into the following groups: (1) TNFi, (2) non-TNF-biologics, (3) corticosteroids, (4) low-potency immunosuppressants, (5) intermediate-potency immunosuppressants, and (6) high-potency immunosuppressants. We reduced confounding by only including patients with rheumatic diseases and systemic therapies. We used an intention-to-treat design in which we assumed that patients with a drug prescription started at the time of the first prescription and continued until they were censored from the study or end of study. We refer the reader to Tables 1 and 2 of the Electronic Supplementary Material (ESM) for further information, such as Anatomical Therapeutic Chemical codes, a list of included drugs, and differences between the two databases.
Definition of Dementia
Our primary outcome of interest was the diagnosis of all-cause dementia during the study period. In the DANBIO study, patients with dementia were identified using the following diagnostic codes: International Classification of Disease, Eighth Revision codes 290.10, 293.09-19, 290.11, 290.09, 290.19, 290.18; ICD-10 codes F00.0-00.9, F01.0-01.9, F02.0, F03.9, G30.0-30.9, G31.9, G31.8; and/or at least one prescription of an anti-dementia drug (Anatomical Therapeutic Chemical codes: N06DA02, N06DA03, N06DA04, and N06DX01). In the AOK PLUS study, ICD-10 codes F00.0-00.9, F01.0-01.9, F02.0, F03.9, and G30.0-30.9 documented in outpatient care were used (Tables 1 and 2 of the ESM). The year 2005 was used as the baseline period to separate incident from prevalent dementia. The date of onset of dementia was defined as the date of a patient’s first medical encounter for a diagnosis of dementia in either study.
Statistical Methods
Cox proportional hazard regression, with a 95% confidence interval (CI), was used to investigate the association of treatment with TNFi in patients with rheumatoid diseases with incident dementia, compared with the other five anti-inflammatory drug groups combined (non-TNF-biologics, corticosteroids, and three classes of immunosuppressants). Individuals contributed time until dementia diagnosis, loss to follow-up, death, or end of study. The analysis was adjusted for age, sex, diabetes mellitus (ICD-10 codes E10, E11, E14), stroke (ICD-10 codes I60-I64), hypertension (ICD-10 code I10), and coronary disease and peripheral atrial occlusive disease (ICD-10 codes I70-I73). The proportional hazards assumption was examined in all analyses and appeared valid.
In additional sensitivity analyses, we also compared the individual association with the risk of dementia among users of other anti-inflammatory treatments (non-TNF-biologics, corticosteroids, three classes of immunosuppressants) in comparison to non-users of those treatments. Additionally, for all six treatment groups (TNFi, non-TNF-biologics, corticosteroids, three classes of immunosuppressants), the associations with the risk of dementia were individually examined, when compared with a ‘mixed control group’. The ‘mixed control group’ refers to the entire Danish population or AOK PLUS population after consideration of all other exclusion criteria in addition to the prescription of drugs of interest (DANBIO: n = 1,959,374; AOK PLUS: n = 172,791). This comparison was intended to address whether a healthy user bias for all medications might exist.
For all analyses, p < 0.05 was considered statistically significant. All statistical analyses were performed using R version 4.1.3 [23].
Results
Characteristics of the Study Populations
In the DANBIO cohort study, 21,538 individuals met our eligibility criteria and had an age range from 65 to 95 years (mean: 69.9 years). In the AOK PLUS cohort study, 7112 individuals were included, with a similar age range as in DANBIO (65–100 years, mean 76.5 years). See Figs. 1 and 2 of the ESM for a study flow diagram of the two cohorts and Table 1 for baseline characteristics of the study population. The prevalence rates of diabetes and hypertension in AOK PLUS were higher than in DANBIO. The use of anti-inflammatory treatment also differed between the two studies, with a higher percentage of prescriptions of corticosteroids (95.8%) in AOK PLUS and TNFi (24.5%) and high-potency immunosuppressants (87.0%) in DANBIO.
Table 1.
Baseline characteristics of the analytical cohorts
| DANBIO | AOK PLUS | |
|---|---|---|
| N | 21,538 | 7112 |
| Person-years | 120,300 | 55,799 |
| Sex, female | 14,169 (65.8%) | 4903 (68.9%) |
| Age, years | 69.9 (5.9) | 76.5 (6.4) |
| Prevalent cardiovascular comorbidities | ||
| Diabetes mellitus | 1627 (7.6 %) | 2684 (37.7%) |
| Stroke | 1001 (4.6%) | 191 (2.7%) |
| Hypertension | 4825 (22.4%) | 5208 (73.2%) |
| Peripheral arterial occlusive disease | 1112 (5.2%) | 939 (13.2%) |
| Drug treatment | ||
| TNFi | 5284 (24.5%) | 197 (2.8%) |
| Non-TNF biologics | 1792 (8.3%) | 67 (0.9%) |
| Corticosteroids | 6457 (30.0%) | 6815 (95.8%) |
| Low-potency immunosuppressants | 7677 (35.6%) | 659 (9.3%) |
| Intermediate-potency immunosuppressants | 1755 (8.1%) | 636 (8.9%) |
| High-potency immunosuppressants | 18,732 (87.0%) | 2042 (28.7%) |
| Incident dementia | 766 (3.6%) | 1840 (25.9%) |
| Follow-up until dementia, yearsa | 4.9 (2.6–7.9) | 4.6 (2.4–6.6) |
TNF tumor necrosis factor, TNFi tumor necrosis factor-α inhibitors
aValues expressed as median (quartile 1 to quartile 3). All other values expressed as mean (standard deviation) or N (%)
Association of Treatment with TNFi with Incident Dementia
A total of 766 (3.6%) DANBIO individuals and 1840 (25.9%) AOK PLUS individuals were diagnosed with dementia during the follow-up (DANBIO: median time to diagnosis 4.9 years, interquartile range 2.6–7.9 years; AOK PLUS: median time to diagnosis 4.6 years, interquartile range 2.4–6.6 years). A tendency towards a lower risk of incident dementia was observed among patients prescribed TNFi, compared with patients prescribed other anti-inflammatory drugs (all five treatment groups) in the DANBIO study (hazard ratio [HR] = 0.92; 95% CI 0.76, 1.10) and the AOK PLUS study (HR = 0.89; 95% CI 0.63, 1.24]) (Table 2). When pooling the results of these two studies, the effect was 0.91 [95% CI 0.77, 1.07] (Fig. 1).
Table 2.
Association of tumor necrosis factor inhibitor-α prescriptions with incident dementia
| DANBIO | AOK PLUS | |
|---|---|---|
| N (cases) | 21,538 (766) | 7112 (1840) |
| HR (95% CI) | 0.92 (0.76, 1.10) | 0.89 (0.63, 1.24) |
Model adjusted for age, sex, prevalent diabetes mellitus, prevalent stroke, prevalent hypertension, and prevalent peripheral arterial occlusive disease
CI confidence interval, HR hazard ratio
Fig. 1.
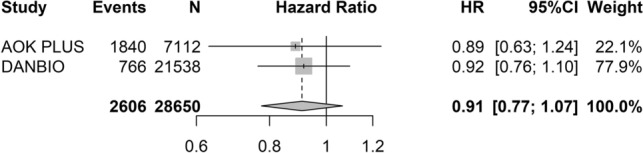
Meta-analysis of the association of tumor necrosis factor-α inhibitor treatment with incident dementia for two cohort studies. CI confidence interval, HR hazard ratio
Sensitivity Analyses
We evaluated the associations of five other systemic rheumatological anti-inflammatory drug treatments (non-TNF biologics, corticosteroids, low-potency immunosuppressants, intermediate-potency immunosuppressants, and high-potency immunosuppressants) with incident dementia, compared to patients not treated with the particular treatment group. Only the treatment group with low-potency immunosuppressants in DANBIO had a statistically significant lower HR of incident dementia (0.84; 95% CI 0.72, 0.99). None of the other associations examined in DANBIO and AOK PLUS reached statistical significance (Table 3 of the ESM). When the analysis of each treatment group was compared against the ‘mixed control group’, the risk of dementia was significantly lower for all treatment groups (compared with individuals regardless of whether they were receiving drug treatment), suggesting the presence of a healthy user bias for analyses that do not restrict to current medication users (Table 4 of the ESM).
Discussion
In the present study, we undertook two different observational cohort studies based on nationwide population-based databases in Denmark and Germany, to analyze the association between the prescription of TNFi and incident dementia in older adults with rheumatological disorders. We observed a trend towards a lower risk of dementia among patients treated with TNFi drugs versus patients treated with other anti-inflammatory drugs; however, the association did not reach statistical significance.
As sensitivity analyses, we tested five other treatment groups (non-TNF biologics, corticosteroids, low-potency immunosuppressants, intermediate-potency immunosuppressants, and high-potency immunosuppressants), which are commonly used in rheumatological systemic treatment and have anti-inflammatory properties through other mechanisms than targeting TNF-α. Only the group with low-potency immunosuppressants in DANBIO showed a statistically significant association (HR = 0.84; 95% CI 0.72, 0.99). None of the other analyses reached statistical significance, which is similar to other epidemiological studies and clinical trials, although it is an area with conflicting results [24–27].
Of note, we performed further sensitivity analyses, where patients treated with one of the six treatment groups (including TNFi) were compared with a ‘mixed control group’ that consisted of individuals aged ≥ 65 years taking any other prescription drug or no drugs. All analyses reached a significant association with a decreased risk of dementia. Thus, we were able to reproduce the results of the study by Chou et al. [11]. This small nested case-control study was based on health claims data from 2000 to 2007 and showed that only etanercept was associated with a lower risk of AD in patients with RA compared with other therapies for RA with a ‘mixed control group’. One possible argument for the increased risk of dementia for patients without prescriptions of the analyzed drugs may be the healthy user effect. This analysis shows the importance of a suitable control group for the interpretation of study results.
Relatively few epidemiological studies have so far investigated treatment with TNFi and incident dementia [10–16]. The available data suggest that TNFi may be promising candidates for the treatment of dementia, but there are methodological limitations to the prior studies in terms of the observation period and study design [11–14].
The TNF pathway appears to be specifically implicated in AD. Gene prioritization in the new loci identified 31 genes that were suggestive of new genetically associated processes, including the TNF-α pathway through the linear ubiquitin chain assembly complex [28]. Regarding the specific question of TNFi and central nervous system penetration, we can imagine at least two different pathophysiological scenarios. First, AD has been specifically associated with the breakdown of the blood–brain barrier early in its course (see [29] for further on this topic), which promotes the entry of a broad array of moieties, including AD-specific drugs. Of note, drugs such as etanercept have nearly identical molecular weights to AD-targeting agents such as aducanumab. Second, it is possible that TNFi act strictly in the periphery, but this results in systemic changes that secondarily affect dementia, perhaps by affecting other small-molecule members of the inflammatory cascade.
One strength of our study is the cohort design in two population-based databases. Even though we had up to 20 and 9 years of follow-up in DANBIO and AOK PLUS, respectively, the median follow-up for both cohorts approximated 5 years. However, as dementia possibly has a long prodromal phase with neuroinflammatory and inflammatory pathology many years before diagnosis [30], it seems likely that the maximal benefit from the anti-inflammatory properties of TNFi might require a longer follow-up and earlier treatment. Zheng et al. also had a long follow-up of 14 years (median) among patients with RA and found no difference in the effect over time [15]. Yet, more studies are warranted with longer follow-ups.
Drug combinations are commonly used in rheumatological treatment and a limitation in our study is that it is difficult to disentangle the complexity of anti-inflammatory drug treatment. As a result, the patients in our study were often treated with multiple drugs of interest at different timepoints through the follow-up. According to current RA treatment guidelines, a combination of traditional disease-modifying antirheumatic drugs (high-potency, intermediate-potency, and low-potency immunosuppressants) or TNFi/methotrexate (high-potency immunosuppressants) combinations are suggested for patients with moderate or high disease severity [22]. We tested multiple anti-inflammatory drug classes, which could partially be an indication of different degrees of the severity of rheumatological disease. Confounding by indication is common in observational studies and it is difficult to separate whether patients receiving TNFi treatment are different from patients taking other anti-inflammatory treatments, both in disease severity and underlying pathophysiology of the rheumatological disease, especially given that these are highly heterogeneous and complex diseases.
An additional bias that could be part of our study is the healthy user effect. This bias may derive from both patient and clinician factors, both of which are possible in our analyses. For example, medication adherence has been associated with better health in several studies [31, 32] . Similarly, clinicians may elect only to prescribe medications that require long-term adherence and monitoring to patients perceived to have a favorable long-term prognosis outside of their autoimmune conditions, leading to a lower observed risk of future dementia. Our results using medication non-users tend to validate this concern.
Furthermore, a limitation in both cohort studies was that the definition of drug use was based on prescriptions, and it was not possible for us to assess compliance with the prescribed drugs.
However, we were fortunately able to create a reasonably homogenous dataset that reduced confounding by only including patients with rheumatic diseases and systemic therapies. As a result, within this patient cohort, even a single prescription code, for example, is likely to be classified correctly in nearly every instance.
In an intention-to-treat framework, we assumed that patients with a drug prescription started at the time of the first prescription and continued until they were censored from the study or end of study. In addition, we did not investigate details on drug usage duration, dosage, and, as mentioned before, drug combinations. Patients normally do not get biologics as first-line therapy for rheumatic diseases. A new-user design could therefore only include patients with second-line therapies, which would exclude a large proportion of the patient group with systemic medications. Because of different starting dates of the TNFi therapy before dementia, no cumulative dose of TNFi was counted in the analyses.
Moreover, our primary outcome of interest was all-cause dementia because AD frequently coexists with other dementia types such as vascular dementia. Detailed information on dementia subtypes is not available in disease registers. Our dementia definition was solely based on the first documented ICD code, which probably leads to an underdiagnosis and a misdiagnosis in both DANBIO and AOK PLUS, especially for the early stages of the disease. However, previous evidence [33] using a single billing claim for dementia found sensitivity and specificity values of 85–89%, suggesting a high degree of validity.
In addition, we did not have sufficient numbers of cases of diseases other than RA to compare the effects across rheumatological disorders. In AOK PLUS, 90% of patients belong to the RA group, 8% to the SA, and 4% to the PsA. About 0.9% had RA and SA and 0.6% had RA and PsA. Similarly, in DANBIO, the distribution of diagnoses was as follows: 92% RA, 4% SA, and 4% PsA. About 0.6% had RA and SA and 0.8% had RA and PsA. Finally, we were not able to control for all known risk factors, such as apolipoprotein ε4 status, smoking, alcohol consumption, and other lifestyle factors, because this information was lacking in both databases.
Conclusions
Our results of the two cohort studies indicate important evidence for an association between TNFi and a lower dementia risk among patients with rheumatological diseases; however, the association did not reach statistical significance. Ultimately, additional cohort studies in other populations and clinical trials with an extended follow-up are needed to understand the potential of TNFi as a new drug treatment for dementia.
Supplementary Information
Below is the link to the electronic supplementary material.
Acknowledgements
The authors thank the health insurance company AOK PLUS for providing the data. The authors also thank Victoria Stephan and Thomas Birkner (Center for Evidence-Based Healthcare) for their support in data preparation and a linguistic review of the manuscript.
Declarations
Funding
Open Access funding enabled and organized by Projekt DEAL. Kenneth J. Mukamal received a grant that covered research on dementia (NIH K24AG065525). Kristine F. Moseholm, Emilie R. Hegelund, Minh Chau S. Nguyen, Laust H. Mortensen, and Majken K. Jensen are supported by grants from the Novo Nordic Foundation Challenge Programme: Harnessing the Power of Big Data to Address the Societal Challenge of Aging (NNF17OC0027812). Saskia Berger, Falko Tesch, and Jochen Schmitt have no funding to declare.
Conflict of Interest
Unrelated to this study, Jochen Schmitt received institutional grants for investigator-initiated research from Sanofi-Aventis, Pfizer, Novartis, and ALK-Abelló and acted as a consultant for Sanofi-Aventis and Novartis. Unrelated to this study, Majken K. Jensen received institutional grants for investigator-initiated research from Novo Nordisk and acted as a consultant for Pfizer on an unrelated study. Saskia Berger, Falko Tesch, Kenneth J. Mukamal, Kristine F. Moseholm, Emilie R. Hegelund, Minh Chau S. Nguyen, and Laust H. Mortensen have no outside or financial interests to declare.
Consent to Participate
Not applicable.
Consent for Publication
Not applicable.
Data Availability
The raw data from AOK PLUS used in this study cannot be made available in the article, the supplemental files, or in a public repository because of German data protection laws (Bundesdatenschutzgesetz). The data used to estimate the model are stored on a secure drive at Center for Evidence-Based Healthcare and can be viewed upon reasonable request from the corresponding author. The data from DANBIO used in this study can be viewed only after application to the Danish Health Data Authority.
Code Availability
Not applicable.
Author Contributions
SB, KFM, FT, KJM, JS, and MKJ conceptualized and designed the study. SB, KFM, ERH, FT, LHM and MCSN conducted the statistical analyses and discussed and interpreted the results. SB and KFM drafted the manuscript. All authors critically reviewed the paper for intellectual content and approved the manuscript for publication. JS and MKJ and KJM are the guarantors of this work and, as such, had full access to all the data in the study and take responsibility for the integrity of the data and the accuracy of the data analysis.
Footnotes
Saskia Berger, Kristine F. Moseholm, Jochen Schmitt and Kenneth J. Mukamal contributed equally to this work.
References
- 1.Chêne G, Beiser A, Au R, et al. Gender and incidence of dementia in the Framingham Heart Study from mid-adult life. Alzheimers Dement. 2015;11(3):310–320. doi: 10.1016/j.jalz.2013.10.005. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.2021 Alzheimer's disease facts and figures. Alzheimers Dement. 2021;17(3):327–406. [DOI] [PubMed]
- 3.GBD Global, regional, and national incidence, prevalence, and years lived with disability for 354 diseases and injuries for 195 countries and territories, 1990-2017: a systematic analysis for the Global Burden of Disease Study 2017. Lancet. 2017;392(10159):1789–1858. doi: 10.1016/S0140-6736(18)32279-7. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Perry VH, Cunningham C, Holmes C. Systemic infections and inflammation affect chronic neurodegeneration. Nat Rev Immunol. 2007;7(2):161–167. doi: 10.1038/nri2015. [DOI] [PubMed] [Google Scholar]
- 5.Sipilä PN, Heikkilä N, Lindbohm JV, et al. Hospital-treated infectious diseases and the risk of dementia: a large, multicohort, observational study with a replication cohort. Lancet Infect Dis. 2021;21(11):1557–1567. doi: 10.1016/S1473-3099(21)00144-4. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Oberlin LE, Erickson KI, Mackey R, et al. Peripheral inflammatory biomarkers predict the deposition and progression of amyloid-β in cognitively unimpaired older adults. Brain Behav Immun. 2021;95:178–189. doi: 10.1016/j.bbi.2021.03.015. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Darweesh SKL, Wolters FJ, Ikram MA, et al. Inflammatory markers and the risk of dementia and Alzheimer's disease: a meta-analysis. Alzheimers Dement. 2018;14(11):1450–1459. doi: 10.1016/j.jalz.2018.02.014. [DOI] [PubMed] [Google Scholar]
- 8.Holmes C, Cunningham C, Zotova E, et al. Systemic inflammation and disease progression in Alzheimer disease. Neurology. 2009;73(10):768–774. doi: 10.1212/WNL.0b013e3181b6bb95. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Rowland C. Pfizer had clues its blockbuster drug could prevent Alzheimer’ disease. Why didn’t it tell the world? 2019. https://www.bostonglobe.com/business/2019/06/05/pfizer-had-clues-its-blockbuster-drug-could-prevent-alzheimer-why-didn-tell-world/TXEbu0hP69VSSsHnuL5uOP/story.html [Accessed Jun 2019].
- 10.Butchart J, Brook L, Hopkins V, et al. Etanercept in Alzheimer disease: a randomized, placebo-controlled, double-blind, phase 2 trial. Neurology. 2015;84(21):2161–2168. doi: 10.1212/WNL.0000000000001617. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Chou RC, Kane M, Ghimire S, et al. Treatment for rheumatoid arthritis and risk of Alzheimer's disease: a nested case-control analysis. CNS Drugs. 2016;11:1111–1120. doi: 10.1007/s40263-016-0374-z. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.McGuinness B, Holmes C, Mirakhur A, et al. The influence of TNF inhibitors on dementia incidence in patients with rheumatoid arthritis; an analysis from the BSRBR-RA. Int J Geriatr Psychiatry. 2018;33(3):556–558. doi: 10.1002/gps.4793. [DOI] [PubMed] [Google Scholar]
- 13.Zhou M, Xu R, Kaelber DC, et al. Tumor necrosis factor (TNF) blocking agents are associated with lower risk for Alzheimer's disease in patients with rheumatoid arthritis and psoriasis. PLoS One. 2020;15(3):e0229819. doi: 10.1371/journal.pone.0229819. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Kern DM, Lovestone S, Cepeda MS. Treatment with TNF-alpha inhibitors versus methotrexate and the association with dementia and Alzheimer's disease. Alzheimers Dement (N Y). 2021;7(1):e12163. doi: 10.1002/trc2.12163. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Zheng C, Fillmore NR, Ramos-Cejudo J, et al. Potential long-term effect of tumor necrosis factor inhibitors on dementia risk: a propensity score matched retrospective cohort study in US veterans. Alzheimers Dement. 2022;18(6):1248–1259. doi: 10.1002/alz.12465. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Desai RJ, Varma VR, Gerhard T, et al. Comparative risk of Alzheimer disease and related dementia among medicare beneficiaries with rheumatoid arthritis treated with targeted disease-modifying antirheumatic agents. JAMA Netw Open. 2022;5(4):e226567. doi: 10.1001/jamanetworkopen.2022.6567. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Hetland ML. DANBIO: powerful research database and electronic patient record. Rheumatology (Oxford) 2011;50(1):69–77. doi: 10.1093/rheumatology/keq309. [DOI] [PubMed] [Google Scholar]
- 18.Ibfelt EH, Jensen DV, Hetland ML. The Danish nationwide clinical register for patients with rheumatoid arthritis: DANBIO. Clin Epidemiol. 2016;8:737–742. doi: 10.2147/CLEP.S99490. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Ibfelt EH, Sørensen J, Jensen DV, et al. Validity and completeness of rheumatoid arthritis diagnoses in the nationwide DANBIO clinical register and the Danish National Patient Registry. Clin Epidemiol. 2017;9:627–632. doi: 10.2147/CLEP.S141438. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Fuhrmann S, Tesch F, Romanos M, et al. ADHD in school-age children is related to infant exposure to systemic H1-antihistamines. Allergy. 2020;75(11):2956–2957. doi: 10.1111/all.14411. [DOI] [PubMed] [Google Scholar]
- 21.Schmitt J, Wüstenberg E, Küster D, et al. The moderating role of allergy immunotherapy in asthma progression: results of a population-based cohort study. Allergy. 2020;75(3):596–602. doi: 10.1111/all.14020. [DOI] [PubMed] [Google Scholar]
- 22.Singh JA, Saag KG, Bridges SL, Jr, et al. 2015 American College of Rheumatology guideline for the treatment of rheumatoid arthritis. Arthritis Rheumatol. 2016;68(1):1–26. doi: 10.1002/art.39480. [DOI] [PubMed] [Google Scholar]
- 23.RC Team . A language and environment for statistical computing. Vienna: R Foundation for Statistical Computing; 2021. [Google Scholar]
- 24.Chou MH, Wang JY, Lin CL, et al. DMARD use is associated with a higher risk of dementia in patients with rheumatoid arthritis: a propensity score-matched case-control study. Toxicol Appl Pharmacol. 2017;334:217–222. doi: 10.1016/j.taap.2017.09.014. [DOI] [PubMed] [Google Scholar]
- 25.Jaturapatporn D, Isaac MG, McCleery J, et al. Aspirin, steroidal and non-steroidal anti-inflammatory drugs for the treatment of Alzheimer's disease. Cochrane Database Syst Rev. 2012;2:CD006378. doi: 10.1002/14651858.CD006378.pub2. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26.Judge A, Garriga C, Arden NK, et al. Protective effect of antirheumatic drugs on dementia in rheumatoid arthritis patients. Alzheimers Dement (N Y) 2017;3(4):612–621. doi: 10.1016/j.trci.2017.10.002. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27.McGeer PL, Schulzer M, McGeer EG. Arthritis and anti-inflammatory agents as possible protective factors for Alzheimer's disease: a review of 17 epidemiologic studies. Neurology. 1996;47(2):425–432. doi: 10.1212/WNL.47.2.425. [DOI] [PubMed] [Google Scholar]
- 28.Bellenguez C, Küçükali F, Jansen IE, et al. New insights into the genetic etiology of Alzheimer’s disease and related dementias. Nat Genet. 2022;54:412–436. doi: 10.1038/s41588-022-01024-z. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29.Alkhalifa AE, Al-Ghraiybah NF, Odum J, et al. Blood-brain barrier breakdown in Alzheimer's disease: mechanisms and targeted strategies. Int J Mol Sci. 2023;24(22):16288. doi: 10.3390/ijms242216288. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 30.Livingston G, Huntley J, Sommerlad A, et al. Dementia prevention, intervention, and care: 2020 report of the Lancet Commission. Lancet. 2020;396(10248):413–446. doi: 10.1016/S0140-6736(20)30367-6. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 31.Brookhart MA, Patrick AR, Dormuth C, et al. Adherence to lipid-lowering therapy and the use of preventive health services: an investigation of the healthy user effect. Am J Epidemiol. 2007;166(3):348–354. doi: 10.1093/aje/kwm070. [DOI] [PubMed] [Google Scholar]
- 32.Shrank WH, Patrick AR, Brookhart MA. Healthy user and related biases in observational studies of preventive interventions: a primer for physicians. J Gen Intern Med. 2011;26(5):546–550. doi: 10.1007/s11606-010-1609-1. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 33.Taylor DH, Jr, Østbye T, Langa KM, et al. The accuracy of Medicare claims as an epidemiological tool: the case of dementia revisited. J Alzheimers Dis. 2009;17(4):807–815. doi: 10.3233/JAD-2009-1099. [DOI] [PMC free article] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
Data Availability Statement
The raw data from AOK PLUS used in this study cannot be made available in the article, the supplemental files, or in a public repository because of German data protection laws (Bundesdatenschutzgesetz). The data used to estimate the model are stored on a secure drive at Center for Evidence-Based Healthcare and can be viewed upon reasonable request from the corresponding author. The data from DANBIO used in this study can be viewed only after application to the Danish Health Data Authority.