

Abstract
We, herein, report a surgical technique for laparoscopy-assisted jejunostomy tube placement in an infant using a loop needle device to fix the jejunum and abdominal wall. A 3-year-old boy with Down’s syndrome underwent nutritional management by gastrostomy due to oral feeding difficulty after radical surgery for congenital duodenal stenosis and following bile duct stenosis. However, intractable gastrostomy site leakage emerged; hence, laparoscopy-assisted gastrostomy takedown and simultaneous laparoscopy-assisted jejunostomy tube placement were planned. After laparoscopy-assisted gastrostomy closure was performed, the jejunum was extracted through the umbilical trocar wound. A jejunostomy tube kit was inserted at the left side of the umbilicus. After tube insertion into the jejunum, the jejunostomy tube was wrapped with four interrupted sutures using the Witzel technique. Suture threads were extracted by percutaneous insertion of a loop needle device, and then, the jejunum was fixed to the abdominal wall. The post-operative course was uneventful. Percutaneous insertion of a loop needle device is useful for fixing a jejunostomy tube to the abdominal wall using the Witzel technique. Our technique is safe, secure and expected to reduce the risk of dislodgement of tube and peritonitis associated with jejunostomy tube placement.
Keywords: Jejunostomy tube placement, laparoscopy-assisted procedure, loop needle device
INTRODUCTION
Gastrostomy is performed for paediatric patients with oral feeding difficulty, such as oesophageal atresia patients with post-operative anastomotic stricture and neurologically impaired patients. However, patients with gastroesophageal reflux disease (GERD) or delayed gastric emptying are at risk of developing aspiration pneumonia due to injection into the stomach. Similarly, there are other situations in which it is necessary to refrain from injecting nutrients into the stomach after surgery, such as in cases of oesophageal reconstruction and oesophageal placement. In addition, gastrostomy sometimes causes severe skin issues. For such patients, an enteral feeding tube is temporarily inserted to prevent symptomatic worsening. However, patients with recurrence of severe GERD require permanent jejunostomy placement.
Feeding jejunostomy is a useful approach for achieving long-term post-pyloric nutrition in such patients.[1,2,3] In recent years, minimally invasive methods for jejunostomy placement have been introduced owing to the use of laparoscopes and the evolution of surgical devices.[4,5]
We, herein, report a case of safe and secure laparoscopy-assisted jejunostomy tube placement using a percutaneous loop needle device for an infant.
PATIENT AND SURGICAL TECHNIQUE
A 3-year-old boy with Down’s syndrome had a history of congenital duodenal stenosis and underwent laparoscopic duodenoduodenostomy at 6 months old. As bile duct dilatation became clinically evident, he also underwent laparoscopic extrahepatic bile duct resection and Roux-Y hepaticojejunostomy. Since he had oral feeding difficulty, he underwent laparoscopy-assisted gastrostomy at 1 year old. However, it became difficult to feed him through the gastrostomy starting 8 months after the operation due to intractable gastrostomy site leakage and dermatitis around the gastrostomy [Figure 1]. Because enteral nutrition could not be established and nutritional disorders were observed, gastrostomy closure and laparoscopic-assisted jejunostomy tube placement were planned at 3 years old.
Figure 1.

Pre-operative appearance of gastrostomy. Dermatitis around the gastrostomy due to intractable gastrostomy leakage
Under general anaesthesia, a longitudinal skin incision was made at the umbilicus. The combination of E-Z ACCESS and a LAP-PROTECTOR (Hakko Co. Ltd., Tokyo, Japan) was applied, and a 5-mm trocar was introduced for a 5-mm 30° scope [Figure 2a]. Pneumoperitoneum was achieved with 8 mm Hg CO2 insufflation. Another 5-mm E-Z trocar (Hakko Co. Ltd.) and 3-mm reusable trocar were also introduced. A vessel sealing system (LigaSure™ Maryland; Medtronic, Minneapolis, MN, USA) was used to dissect and remove the gastrostomy from the abdominal wall, and closure of the gastrostomy was performed in two layers with 4-0 PDS interrupted sutures through the umbilical wound under direct vision. A jejunostomy kit (NCJ kit; PhyCon, Oklahoma, OK, USA) was introduced into the abdominal cavity at the left side of the umbilicus. The jejunostomy kit and jejunum were extracted through a wrap protector attached to the umbilical wound, and the kit was introduced into the lumen of the jejunum 40 cm anal side from the ligament of Treitz and also the anal side of Roux-Y jejunojejunostomy. The tip of the jejunostomy tube was placed into the jejunum. The jejunostomy tube was covered with four interrupted sutures of the seromuscular layer using 4-0 PDS and tunnelled according to the Witzel technique. After reducing the jejunum into the abdominal cavity, pneumoperitoneum was established again [Figure 2b]. A loop needle device (LAPA-HER-CLOSURE; Hakko Co. Ltd.) was percutaneously inserted into the abdominal cavity to grasp the suture threads used in the Witzel technique under laparoscopic inspection [Figure 2c]. The jejunum and abdominal wall were fixed by pulling out the loop needle device [Figure 2d and e] and ligating the grasped thread to make a subcutaneous knot [Figure 3 and Video 1]. A schematic image of the intraoperative findings is presented because the patient received multiple surgeries [Figure 4]. Post-operatively, the skin findings of the site of previous gastrostomy and umbilicus improved without complications like infection, and enteral nutrition was well established.
Figure 2.

Intraoperative findings. (a) The port layout, (b) The thread used to cover the jejunostomy catheter with seromuscular suture was left long, (c) The thread was gripped with a loop needle device. (d) The jejunum was fixed to the abdominal wall by pulling the thread. (e) Jejunum and abdominal wall fixation was completed (long pointed line: the catheter used in the Witzel technique, short pointed line: the catheter in the jejunum)
Figure 3.

Post-operative appearance of the abdominal wall. The surgical wound of the loop needle device (arrowhead)
Figure 4.
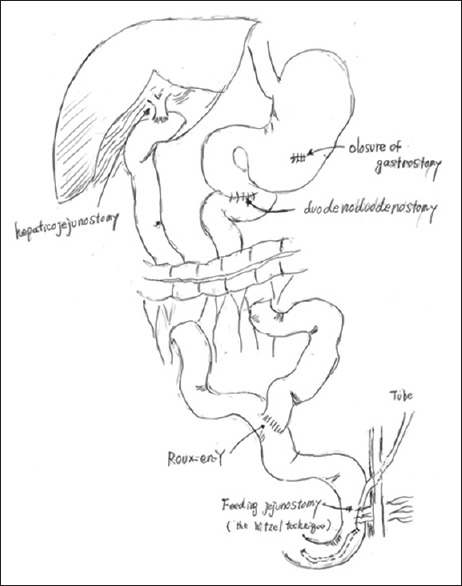
The schematic image of intraoperative findings. The patients with a history of laparoscopic duodenoduodenostomy, laparoscopic extrahepatic bile duct resection, Roux-Y hepaticojejunostomy and laparoscopy-assisted gastrostomy underwent laparoscopy-assisted jejunostomy tube placement
DISCUSSION
Since 1990, advances in laparoscopic surgical techniques have permitted the insertion of feeding jejunostomies. Belsha et al. introduced the percutaneous laparoscopic-endoscopic jejunostomy technique,[4] describing its provision of valuable visualisation of the bowel loops intraabdominally, thereby eliminating the risk of puncturing through overlapping loops of the small bowel or colon.[4] Esposito et al. introduced the laparoscopy-assisted jejunostomy tube, in which the jejunum and abdominal wall are fixed with two ‘U-stitches’.[5] Lotti et al. reported a novel technique for establishing a laparoscopic jejunostomy tube using a single barbed suture to secure the bowel and tunnelling the jejunostomy catheter according to the Witzel technique.[6] In our case, tunnelling of the jejunostomy catheter was performed by extracting the jejunum from the umbilicus port site. We also used the thread to wrap in the seromuscular layer to fix the jejunum and the abdominal wall for similar purposes. If this thread is too long, it will be difficult to manipulate it in the abdominal cavity; hence, it should be the minimum length that can be ligated after being pulled out of the abdominal cavity. Complications of tube jejunostomy include skin troubles due to the backflow of intestinal juice from the opening and intestinal torsion around the fixation of the tube jejunostomy.[2,7] However, using the Witzel technique, it is possible to prevent backflow from the skin opening,[5] and the risk of intestinal torsion can be reduced by fixing the abdominal wall and the intestinal tract extensively.[8] It should be noted that, like other intra-abdominal procedures, it is contraindicated for intestinal obstruction[7] and is not recommended for patients with severe intra-abdominal adhesions. Our surgical technique combined with the Witzel procedure under direct vision with secure fixation using a loop needle device under laparoscopy inspection is safe and reliable for jejunostomy tube placement.
Ethics statement
Informed consent was obtained from the family of the patient for the publication of this case report.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
Video available on: https://journals.lww.com/JMAS
Acknowledgements
We thank Mr. Brian Quinn for his comments and help with the manuscript.
REFERENCES
- 1.D’Cruz JR, Cascella M. StatPearls. Treasure Island (FL): StatPearls Publishing Copyright©. StatPearls Publishing LLC; 2022. Feeding jejunostomy tube. [PubMed] [Google Scholar]
- 2.Egnell C, Eksborg S, Grahnquist L. Jejunostomy enteral feeding in children: Outcome and safety. JPEN J Parenter Enteral Nutr. 2014;38:631–6. doi: 10.1177/0148607113489832. [DOI] [PubMed] [Google Scholar]
- 3.Raval MV, Phillips JD. Optimal enteral feeding in children with gastric dysfunction: Surgical jejunostomy versus image-guided gastrojejunal tube placement. J Pediatr Surg. 2006;41:1679–82. doi: 10.1016/j.jpedsurg.2006.05.050. [DOI] [PubMed] [Google Scholar]
- 4.Belsha D, Thomson M, Dass DR, Lindley R, Marven S. Assessment of the safety and efficacy of percutaneous laparoscopic endoscopic jejunostomy (PLEJ) J Pediatr Surg. 2016;51:513–8. doi: 10.1016/j.jpedsurg.2015.11.023. [DOI] [PubMed] [Google Scholar]
- 5.Esposito C, Alicchio F, Escolino M, Ascione G, Settimi A. Laparoscopy-assisted jejunostomy in neurological patients with chronic malnutrition and GERD. Technical considerations and analysis of the results. Pediatr Med Chir. 2013;35:125–9. doi: 10.4081/pmc.2013.45. [DOI] [PubMed] [Google Scholar]
- 6.Lotti M, Capponi MG, Ferrari D, Carrara G, Campanati L, Lucianetti A. Laparoscopic Witzel jejunostomy. J Minim Access Surg. 2021;17:127–30. doi: 10.4103/jmas.JMAS_248_19. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Tapia J, Murguia R, Garcia G, de los Monteros PE, Oñate E. Jejunostomy: Techniques, indications, and complications. World J Surg. 1999;23:596–602. doi: 10.1007/pl00012353. [DOI] [PubMed] [Google Scholar]
- 8.Pagan A, Bianchi A, Martínez JA, Jiménez M, Gonzalez FJ. Laparoscopic surgical transmesocolic jejunostomy: A new surgical approach. Turk J Surg. 2018;34:155–7. doi: 10.5152/turkjsurg.2017.3211. [DOI] [PMC free article] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.