

Abstract
OBJECTIVE:
Our objectives with this study were to describe the frequency of selected cooccurring health conditions and individualized education program (IEP) services and post-high school transition planning for adolescents with autism spectrum disorder and identify disparities by sex, intellectual ability, race or ethnicity, and geographic area.
METHODS:
The study sample included 1787 adolescents born in 2004 who were identified as having autism through a health and education record review through age 16 years in 2020. These adolescents were part of a longitudinal population-based surveillance birth cohort from the Autism and Developmental Disabilities Monitoring Network from 2004 to 2020 in 5 US catchment areas.
RESULTS:
Attention deficit hyperactivity disorder (47%) and anxiety (39%) were the most common cooccurring health conditions. Anxiety was less commonly identified for those with intellectual disability than those without. It was also less commonly identified among Black adolescents compared with White or Hispanic adolescents. There was wide variation across Autism and Developmental Disabilities Monitoring Network sites in the provision of school-based IEP services. Students with intellectual disability were less likely to receive school-based mental health services and more likely to have a goal for postsecondary independent living skills compared with those without intellectual disability. A total of 37% of students did not participate in standardized testing.
CONCLUSIONS:
We identified disparities in the identification of cooccurring conditions and school-based IEP services, practices, and transition planning. Working with pediatric health and education providers, families, and adolescents with autism will be important to identify contributing factors and to focus efforts to reduce disparities in the supports and services adolescents with autism have access to and receive.
Autism spectrum disorder (hereafter referred to as autism) is a developmental disability that can cause significant social, communication, and behavioral challenges across the lifespan.1 Cooccurring conditions, such as attention deficit hyperactivity disorder (ADHD) and anxiety, that can impair functioning are common, affecting >70% of people with autism.2,3
Within the school context, some adolescents with autism with impairments may qualify for special education services outlined in an annual Individualized Education Program (IEP).4 Although the process can be started earlier, by the time a student with an IEP reaches the age of 16 years, post-secondary transition-specific goals and actions to meet those goals must be specified as part of the IEP.4
Because impairments that impact educational outcomes may span into adulthood, schools are required to generate education- and employment-specific post-high school (or postsecondary) goals, with recommended but optional planning for post-high school independent living skills.5 Understanding the health status and educational services planned for during this transition period is important to identify disparities and to focus health and education interventions to prepare adolescents with autism and their families for the transition to adulthood.
Beginning in the 2018 Autism and Developmental Disabilities Monitoring (ADDM) Network surveillance year (SY), the US Centers for Disease Control and Prevention expanded surveillance to include 16-year-olds at 5 sites and found variation in identification, cooccurring conditions, and educational supports received by sex, intellectual ability, and race and ethnicity, and ADDM Network site.6,7 Select findings from these reports include that adolescents (1) were more likely to be identified with autism after the age of 8 years if they were Hispanic, had high intelligence quotient (IQ) or adaptive scores, or had certain cooccurring health conditions and (2) were less likely to have transition plan goals for postsecondary education or employment or receive mental health services if they had an intellectual disability. The purpose of this report is to continue to monitor, with a more recent cohort of adolescents with autism, health status and educational services, with a specific focus on the role of intellectual disability and the coronavirus disease 2019 (COVID-19) pandemic.
METHODS
Population and Data Collection
The sample included adolescents born in 2004 whose health and education records were reviewed in 2012 at age 8 for autism surveillance by the ADDM Network (SY 2012) in catchment areas within Arkansas, Georgia, Maryland, Utah, and Wisconsin.8 Selection for review was based on the presence of autism-specific information from special education exceptionalities or health provider billing codes. We reviewed these adolescents’ 2013 to 2020 health and education records during the 2020 ADDM Network SY (SY 2020) at age 16 years at the same 5 sites.9 The SY 2020 data were linked to the SY 2012 data described previously.8
Surveillance Case Definition
A child met the autism case definition if they lived in the SY 2020 study area in 2012 and had either (1) a written statement from a qualified professional diagnosing autism on a comprehensive evaluation, (2) a special education classification of autism in public school, or (3) an autism International Classification of Diseases (ICD) code obtained from administrative or billing information.
Variable Definitions
Data Collected in 2012
Demographic data from 2004 to 2012 included sex, race and ethnicity. Persons of Hispanic ethnicity might be of any race but were categorized as Hispanic. Racial and ethnic data were included because previous reports revealed variation in autism prevalence between groups, likely attributable to differences in community autism identification practices and access to services that are critical to monitor. ADDM Network clinicians reviewed evaluations in abstracted records and documented whether children ever had a written diagnosis of selected common cooccurring conditions (ADHD, anxiety, depression, seizure disorder, or obsessive-compulsive disorder). We collected reports or scores from clinical and education providers from the most recent IQ and adaptive composite tests.
Data Collected in 2020
A total of 21% of adolescents had an unknown residence and may have moved after 2012, limiting the amount of information available from 2013 to 2020. No significant differences were found by known residence period by sex, race or ethnicity, and intellectual ability (data not shown).
We collected historical and current diagnoses of the selected cooccurring conditions and the most recent examiner reports or scores from IQ and adaptive tests. Adolescents were considered nonverbal or minimally verbal or having suicidal behavior or ideation if any evaluation document included these descriptions.
We collected data from a student’s most recent IEP from ages 15 and 16 years, including primary special education eligibility category, school services (speech, occupational therapy, physical therapy, social skills instruction, special instruction, and mental health), extended school year services, and assessment methods (ie, takes standardized assessments, with or without accommodations, or alternate assessments).10 From the transition plan section of the IEP, we collected additional information, including whether (1) a transition plan was completed, (2) there was an assessment of transition needs, (3) there was a course of study to reach postsecondary goal(s), and (4) post-secondary goals were stated for education, employment, and independent living skills (includes daily living skills and community participation). Lastly, the anticipated high school diploma type was collected (regular or alternate). For students with the most significant cognitive disabilities, an alternate diploma is commonly awarded.11 We also collected the number of IEPs completed by month and year from 2013 to 2019.
Analytic Methods
We dichotomized adolescents’ age of first identification with autism as ≤8 years or 9 to 16 years on the basis of their earliest autism diagnosis, autism eligibility, or autism ICD code. We classified adolescents as having an adaptive impairment on the basis of their most recent adaptive score (≤70). We classified adolescents as having an intellectual disability on the basis of their most recently available IQ score (≤70) or report; adaptive functioning was missing for 44% of adolescents and, thus, was not included in the definition of intellectual disability.12 Among those with intellectual ability documentation, we calculated prevalence ratios to compare the percentage of the autism population with and without intellectual disability by adolescent characteristics.
Among adolescents with ≥1 developmental evaluation from a health source from 2013 to 2020, we estimated the percentage who ever (from birth through age 16) had a diagnosis of selected cooccurring conditions and who (from ages 9 through 16) had nonverbal or minimally verbal or suicidal behavior or ideation documented in their records overall and by sex, race or ethnicity, intellectual ability, and ADDM Network site.
For the aggregate IEP data, we calculated the average number of IEPs completed by month from 2013 to 2019 and the number of IEPs completed by month in 2020, suppressing months with <100 IEPs completed because of high variability in low-volume summer IEP months. The statistical significance of the difference in the number of IEPs between the 2 periods, by month, was calculated by using log-linear regression models. For individuals’ IEP data, we calculated the percentage of students with the selected IEP components among those with ≥1 IEP completed at ages 15 and 16 years. Among the subset of adolescents with ≥1 transition plan, we calculated the percentage of adolescents with selected components in their transition plan. For all individual IEP measures, we calculated percentages overall and by intellectual ability and ADDM Network site. We calculated all 95% confidence intervals around percentages using the Wilson method and used Stata SE/17.0 and R (version 4.2.2) for data management and analyses.
RESULTS
Of 2947 8-year-olds whose records were reviewed in 2012 for autism, by age 16 years, 1787 were ever identified in the community as having autism (Supplemental Fig 3). Most were identified as having autism by age 8 years, whereas 14% were identified during ages 9 to 16 years. Among adolescents with autism, 84% had a clinical diagnosis of autism, 81% had an autism ICD code, and 57% had an autism special education eligibility.
Approximately one-third of adolescents with autism also had an intellectual disability. Those with intellectual disability were more likely to be female, Black, or Asian or Pacific Islander, have an adaptive impairment, and be first identified with autism by age 8 years compared with those without an intellectual disability (Table 1).
TABLE 1.
Comparison of Characteristics of Adolescents with Autism by Intellectual Ability Status (n = 1787): ADDM Network, 5 sites, United States, 2020
| Category | Characteristic | Total | Known Intellectual Ability Statusa | Intellectual Disability | Prevalence Ratio |
|---|---|---|---|---|---|
| (n) | (n) | % (n) | (95% CI) | ||
| Sex | Female | 322 | 238 | 39.5% (94) | 1 |
| Male | 1465 | 1101 | 32.2% (355) | 0.82 (0.68–0.98) | |
| Race/ethnicity | White | 1124 | 823 | 27.5% (226) | 1 |
| Black | 337 | 284 | 50.7% (144) | 1.85 (1.57–2.17) | |
| American Indian or Alaskan Native | 8 | 6 | 0.0% (0) | ||
| Asian or Pacific Islander | 53 | 43 | 44.2% (19) | 1.61 (1.13–2.29) | |
| Other race or multiple races | 70 | 52 | 32.7% (17) | 1.19 (0.79–1.79) | |
| Hispanic regardless of race | 176 | 127 | 32.3% (41) | 1.18 (0.89–1.55) | |
| Adaptive functioning statusb | No adaptive impairment | 416 | 386 | 18.4% (71) | 1 |
| Adaptive impairment | 578 | 531 | 59.1% (314) | 3.21 (2.58–4.01) | |
| Site | Arkansas | 135 | 119 | 37.8% (45) | 1 |
| Georgia | 335 | 295 | 41.0% (121) | 1.09 (0.83–1.42) | |
| Maryland | 335 | 265 | 34.7% (92) | 0.92 (0.69–1.22) | |
| Utah | 571 | 428 | 22.9% (98) | 0.61 (0.45–0.81) | |
| Wisconsin | 411 | 232 | 40.1% (93) | 1.06 (0.81–1.40) | |
| First identification period | 9–16 y | 255 | 198 | 25.8% (51) | 1 |
| ≤8 y | 1532 | 1141 | 34.9% (398) | 1.35 (1.06–1.74) | |
| Total | Total | 1787 | 1339 | 33.5% (449) |
CI, confidence interval.
Intellectual ability based on most recently available IQ score (≤70) or examiner’s report.
Adaptive functioning based on most recently available adaptive score (≤70) or examiner’s report.
Cooccurring Conditions
ADHD (47%) and anxiety (39%) were the most frequently diagnosed cooccurring conditions by age 16 years (Supplemental Table 3). Those with intellectual disability were more likely to have a seizure diagnosis or be nonverbal than those without intellectual disability (Fig 1). In contrast, those without intellectual disability were more likely to have a diagnosis of ADHD, anxiety, depression, or have documented suicidal behavior or ideation. Males were more likely to have ADHD and less likely to have seizures than females (Supplemental Table 3). Anxiety and depression were more commonly diagnosed among white and Hispanic adolescents than among Black adolescents. White adolescents were less likely to be nonverbal compared with Black or Asian Pacific Islander adolescents. We found wide variation across sites in diagnoses of all cooccurring conditions, except for obsessive-compulsive disorder.
FIGURE 1.
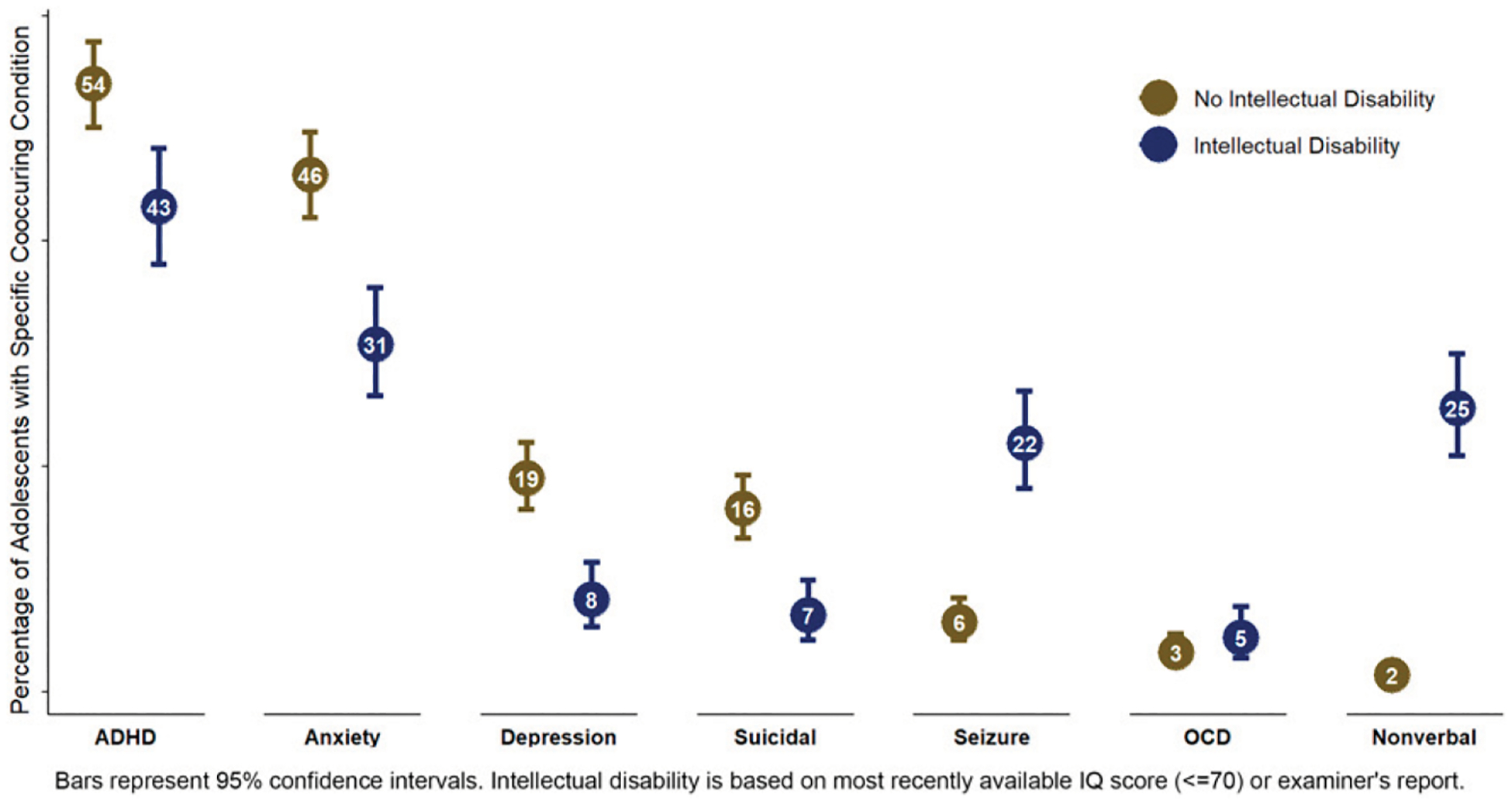
Percentage of adolescents with autism with an ever occurrence of selected cooccurring health conditions from 2004 to 2020, by intellectual ability status (n = 1340).
Individualized Education Programs
Of students with autism receiving special education services at ages 15 and 16 years (n = 482), 69% were served under an autism special education eligibility. Special instruction (65%) and speech (54%) were the most common school services noted on IEPs (Supplemental Table 4). Sites varied greatly in the percentage of students receiving specific services; for example, school-based mental health services were only documented at 2 sites (Maryland and Utah). Those with intellectual disability were more likely to have an extended school year and receive school-based services for speech, occupational therapy, and physical therapy but less likely to receive school-based services for mental health (Fig 2). Few (16%) students with autism with IEPs participated in standardized testing without accommodations, and 37% did not participate in standardized testing (ie, they took an alternate assessment; Supplemental Table 4). A total of 66% of students with autism and intellectual disability took an alternate assessment compared with 13% of students with autism and without intellectual disability (Fig 2).
FIGURE 2.
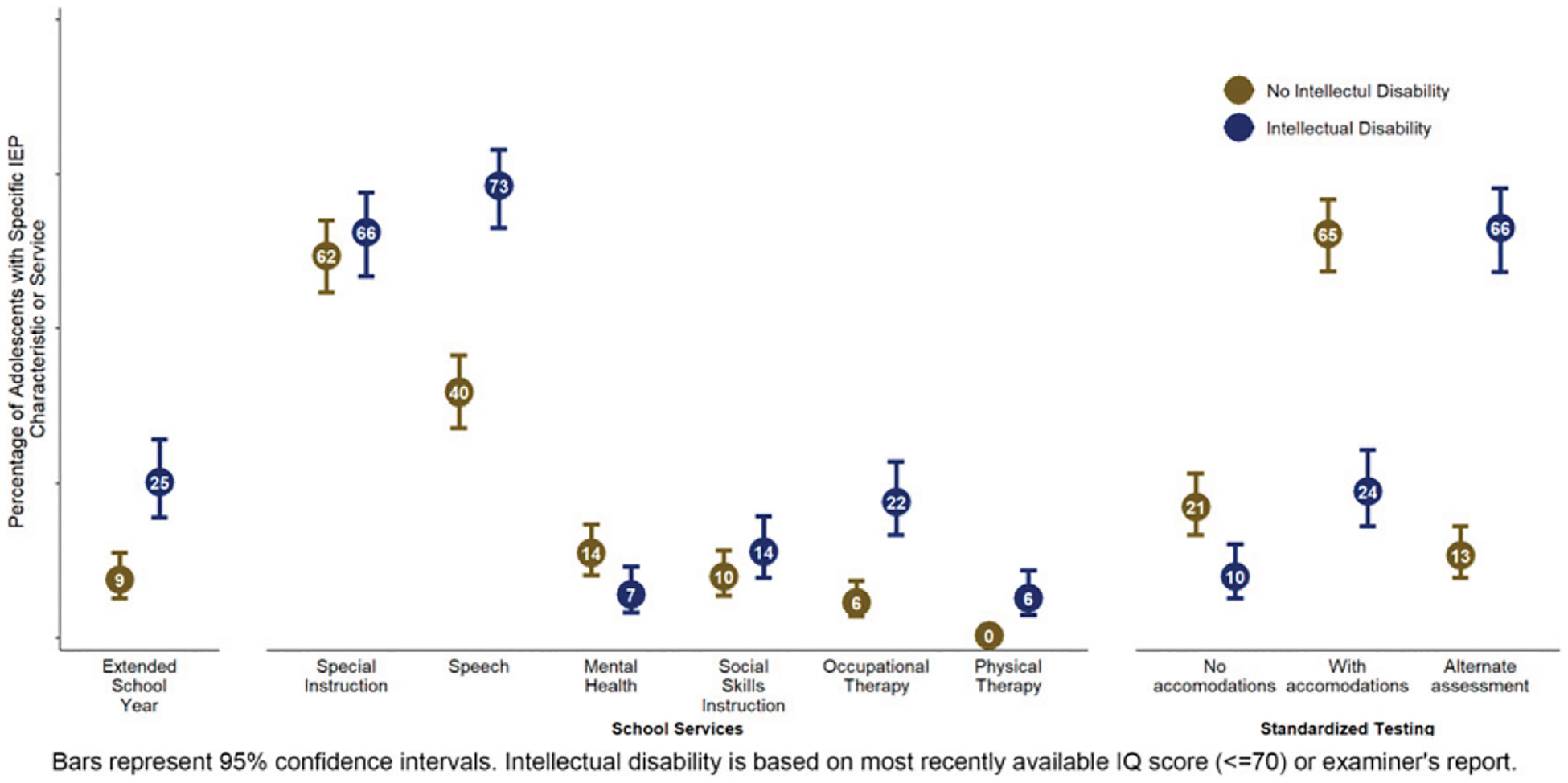
Percentage of adolescents with autism with specific IEP components and services, by intellectual ability status (n = 482).
Overall, the majority (94%) of students had a transition plan associated with their most recent IEP (Table 2). The presence of a transition plan varied by site, with 74% in Wisconsin compared with 100% in Maryland and Utah. An assessment of transition needs, a course of study to reach postsecondary goals, and postsecondary goals for education and employment were present in >90% of IEPs. However, completion of a goal for postsecondary independent living skills was lower overall (47%) and varied by site (17% in Maryland compared with 96% in Arkansas) and intellectual ability (36% for those without intellectual disability compared with 62% for those with intellectual disability). It was anticipated that three-quarters of students with autism would receive a regular high school diploma.
TABLE 2.
Percentage of Adolescents With Autism With IEP Transition Plans and Specific Components (n = 482): ADDM Network, 5 sites, United States, 2020
| Category | Characteristic | Percentage With a Transition Plan of Those With an IEP | Required Transition Age (y) | Assessment of Transition Needs, % (95% CI) | Course of Study to Reach Postsecondary Goals, % (95% CI) | Postsecondary Education Goal, % (95% CI) | Post-Secondary Employment Goal, % (95% CI) | Postsecondary Independent Living Skills Goal, % (95% CI) | Anticipated to Receive Regular High School Diploma,a % (95% CI) |
|---|---|---|---|---|---|---|---|---|---|
| Intellectual abilityb | No intellectual disability | 96% (251/262) | 94% (90%–96%) | 93% (89%–95%) | 99% (97%–100%) | 99% (97%–100%) | 36% (30%–42%) | 94% (90%–96%) | |
| Intellectual disability | 93% (172/186) | 92% (87%–95%) | 91% (85%–94%) | 99% (97%–100%) | 99% (96%–100%) | 62% (55%–69%) | 51% (43%–59%) | ||
| Site | Arkansas | 78% (54/69) | 16 | 98% (90%–100%) | 89% (78%–95%) | 96% (87%–99%) | 96% (87%–99%) | 96% (87%–99%) | — |
| Georgia | 95% (124/130) | 16 | 81% (74%–87%) | 91% (85%–95%) | 100% (97%–100%) | 99% (96%–100%) | 69% (61%–77%) | 96% (91 %–98%) | |
| Maryland | 100% (151/151) | 14 | 95% (91 %–98%) | 89% (83%–93%) | 100% (98%–100%) | 100% (98%–100%) | 17% (12%–24%) | 61% (53%–68%) | |
| Utah | 100% (101/101) | 14 | 100% (96%–100%) | 98% (93%–99%) | 99% (95%–100%) | 99% (95%–100%) | 35% (26%–44%) | 70% (60%–79%) | |
| Wisconsin | 74% (23/31) | 14 | 91% (73%–98%) | 83% (63%–93%) | 100% (86%–100%) | 100% (86%–100%) | 52% (33%–71%) | — | |
| Overall | Total | 94% (453/482) | 93% (90%–95%) | 91% (88%–94%) | 99% (98%–100%) | 99% (98%–100%) | 47% (42%–51 %) | 75% (71%–79%) |
CI, confidence interval.
Anticipated high school diploma data excludes Wisconsin and Arkansas because of missing data from their sites’ IEPs.
Intellectual ability based on most recently available IQ score (≤70) or examiner’s report.
Based on aggregate IEP count data, there was a decline in the number of IEPs completed during the months of March, April, and December of 2020, an early pandemic period when many schools were operating virtually, compared with those same months during the comparison period (2013–2019; Supplemental Fig 4).
DISCUSSION
Although diagnoses of cooccurring conditions, especially ADHD and anxiety, were more common among adolescents with autism compared with previous findings in the general population,13,14 the percentages with these conditions were lower than those reported for ADDM SY2018.6 This may be attributable, in part, to the negative impact of the COVID-19 pandemic on access to mental health diagnosis and care in 2020, understanding conditions may have been diagnosed at any age; other studies have highlighted the increased mental health burden and reduced access to services for adolescents during the pandemic.15–18 The differences may also be due to the changing composition of adolescents in the population due to an increase in the number of children identified with autism over time. Compared with adolescents in the general population, the high frequency of cooccurring conditions suggests that the medical needs of many adolescents with autism may be complex and continue as they transition into adulthood.19 It will be important to ensure that mental health services are available during adolescence and to continue to monitor cooccurring mental health conditions among adolescents with autism in future SYs.
Disparities in the presence of cooccurring conditions were identified by intellectual ability, race or ethnicity, sex, and site. The higher percentage of white and Hispanic adolescents with cooccurring anxiety and depression compared with Black adolescents with autism may indicate disparities in the identification and treatment of mental health concerns for Black adolescents. Adolescents from racial minority groups are more likely to be affected by mental health disorders but less likely to be identified or to receive mental health services compared with white adolescents.20,21 A lack of access to services may also contribute to the higher percentage of Black compared with white adolescents who were nonverbal. Compared with those without intellectual disability, those with intellectual disability were more likely to be nonverbal and experience seizures and less likely to have documented anxiety or suicidal ideation or behavior. The lower percentage of adolescents with cooccurring anxiety and suicidal ideation or behavior may be related to challenges in the screening and diagnosis of these conditions among those with intellectual disability, particularly among those who are nonverbal.22,23 The differences in cooccurring conditions reinforce our understanding of the heterogeneity of autism in access to treatment and service needs and the need for individualized support during the transition to adulthood.
Despite the high prevalence of cooccurring mental health conditions among adolescents with autism relative to the general population, only 2 sites reported any student with autism and an IEP receiving school-based mental health services. Schools have faced mental health provider shortages for years.24 Moreover, although those with intellectual disability had higher utilization of most school services, they were less likely to receive mental health services compared with those without intellectual disability, which is consistent with previous findings.25 Those without intellectual disability may be more readily able to describe their experiences related to mental health to be identified for school services compared with those with intellectual disability.26 For all students, externalizing behaviors, such as hyperactivity, may be more apparent for capturing attention and services, compared with internalized mental health issues.27 Although students’ conditions may be managed in a health care setting, mental health services provided by schools may also serve to increase access.26,28
Beyond school-based mental health services, we observed wide variation across sites in the percentage of students with autism and an IEP receiving specific services. These differences in service provision may be due to differences at the district or state levels in policy, programs, or resources available or the characteristics of adolescents with autism being served.29 Schools may consider tracking service use over time, if not already monitoring, to ensure that services provided to students are appropriately matched to their needs.
The substantial drops we observed in the number of IEPs completed during the first 2 months (March and April 2020) of the COVID-19 pandemic and in December 2020 compared with previous years are likely, in part, attributable to disruptions in schools due to COVID-associated closures.30 More recent data after 2020 are needed to understand the extent of disruptions in 2020 and more recently due to the long-term impacts of pandemic measures.
A total of 37% of students with autism and an IEP in our sample took an alternative assessment. Alternative assessments are aligned to alternative standards and are for students with the most significant cognitive disabilities. Participation in alternative assessments is limited to no more than 1% of students per grade per state.31 A total of 13% of those with autism who did not have documented intellectual disability took alternative assessments, potentially indicating that they were inappropriately administered. It could also indicate an underdiagnosis of or lack of documentation of intellectual disability, which may make it more difficult for these adolescents to qualify for supplemental security income benefits as adults.32 Participating in standardized testing can be one marker indicating that a student is on track to receive a regular high school diploma.10,11
Similar to the ADDM SY 2018,7 we found high overall inclusion of transition plans in IEPs, and the completion of transition assessments and postsecondary goals, with the exception of the independent living skills goal, which is required only if the student’s IEP team determines it to be appropriate. The wide variation in the completion of an independent living skill goal by site and intellectual ability status may indicate state- or district-level factors influencing whether this element is prioritized for completion. Despite this goal being optional and acknowledging the possibility that this goal may still be completed before high school exit, it may be beneficial for students qualifying for an IEP to consider and plan for independent living skills after high school exit. Both educators and health care providers play an important role in supporting adolescents in transition planning to adulthood in health care, education, employment, and independence.33
Although this study is based on a large, population-based sample, the findings are not representative of all adolescents with autism. The sample was based on adolescents with indications of autism by age 8 years, and we would have missed follow-up information on adolescents who moved from the study area or stopped using education or health services after age 8 years. Increases in telemedicine availability and primary care providers diagnosing health conditions may have led to the under-capture of cooccurring health conditions. Expanding the range of providers captured in autism surveillance may be warranted in future SYs. Students who were aged 15 years at the most recently collected IEP may not have been required to have a transition plan in their IEP. We could not report on services received by students with autism without an IEP or services such as mental health received outside of a school setting. Moreover, although we reported on the presence of documented goals and services, we could not capture whether they were implemented or their quality. Lastly, our surveillance definition of intellectual disability differs from the clinical definition of intellectual disability, which includes a measure of adaptive functioning. The high missingness of adaptive functioning tests highlights a potential opportunity for improvement in conducting this assessment in clinical practice.
Expanded US autism surveillance of the adolescent period in 2020 provided an opportunity to monitor the presence of, and disparities associated with, cooccurring health conditions and special educational services. Clinicians, educators, other service providers, and policymakers can use these data to inform service development for adolescents with autism and focus interventions to reduce disparities in educational programming and the identification and treatment of cooccurring conditions before the transition to adulthood.
Supplementary Material
WHAT’S KNOWN ON THIS SUBJECT:
Among adolescents with autism, there are few recent population-based data on cooccurring health conditions, education services, and planning for postschool life.
WHAT THIS STUDY ADDS:
In this study, we found racial and ethnic disparities in anxiety and a wide variation in school-based services and transition planning by geographic area and intellectual ability, identifying potential areas of focus to improve quality and reduce disparities.
FUNDING:
This surveillance activity was supported by funding from the Centers for Disease Control and Prevention (CDC). The CDC led the study design, data collection, data analysis, data interpretation, and writing of the report.
ABBREVIATIONS
- ADDM
Autism and Developmental Disabilities Monitoring
- ADHD
attention-deficit/hyperactivity disorder
- COVID-19
coronavirus disease 2019
- ICD
International Classification of Diseases
- IEP
Individualized Education Program
- IQ
intelligence quotient
- SY
surveillance year
Footnotes
The findings and conclusions in this report are those of the authors and do not necessarily represent the official position of the Centers for Disease Control and Prevention.
CONFLICT OF INTEREST DISCLOSURES: The authors have indicated they have no conflicts of interest relevant to this article to disclose.
REFERENCES
- 1.Centers for Disease Control and Prevention. Autism spectrum disorder (ASD). Available at: https://www.cdc.gov/ncbddd/autism/index.html. Accessed May 16, 2023
- 2.Lai M-C, Lombardo MV, Baron-Cohen S. Autism. The Lancet. 2014;383(9920):896–910 [DOI] [PubMed] [Google Scholar]
- 3.Ameis SH, Szatmari P. Common psychiatric comorbidities and their assessment. In: Anagnostou E, Brian J, eds. Clinician’s Manual on Autism Spectrum Disorder. Springer International Publishing; 2015:19–32 [Google Scholar]
- 4.U.S. Department of Education. Sec. 300.320 Definition of individualized education program. Available at: https://sites.ed.gov/idea/regs/b/d/300.320. Accessed May 16, 2023
- 5.U.S. Department of Education. Post-secondary transition guide. Available at: https://sites.ed.gov/idea/files/postsecondary-transition-guide-may-2017.pdf. Accessed June 10, 2023
- 6.Hughes MM, Shaw KA, Patrick ME, et al. Adolescents with autism spectrum disorder: diagnostic patterns, co-occurring conditions, and transition planning. J Adolesc Health. 2023;73(2): 271–278 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Hughes MM, Kirby AV, Davis J, et al. Individualized education programs and transition planning for adolescents with autism. Pediatrics. 2023;152(1):e2022060199. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Christensen DL, Braun KVN, Baio J, et al. Prevalence and characteristics of autism spectrum disorder among children aged 8 years - Autism And Developmental Disabilities Monitoring Network, 11 sites, United States, 2012. MMWR Surveill Summ. 2018;65(13):1–23 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Maenner MJ, Warren Z, Williams AR, et al. Prevalence and characteristics of autism spectrum disorder among children aged 8 years - Autism and Developmental Disabilities Monitoring Network, 11 sites, United States, 2020. MMWR Surveill Summ. 2023;72(2):1–14 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.U.S. Department of Education. Sec. 300.160 Participation in assessments. Available at: https://sites.ed.gov/idea/regs/b/b/300.160. Accessed May 16, 2023
- 11.Georgia Department of Education. State-defined alternate diploma: frequently asked questions for families. Available at: https://www.gadoe.org/Curriculum-Instruction-and-Assessment/Special-Education-Services/Documents/Sp%20Ed%20homepg/ESSA%20Alternate%20Diploma%20FAQ%20for%20Families.pdf. Accessed May 17, 2023
- 12.Obi O, Van Naarden Braun K, Baio J, et al. Effect of incorporating adaptive functioning scores on the prevalence of intellectual disability. Am J Intellect Dev Disabil. 2011;116(5):360–370 [DOI] [PubMed] [Google Scholar]
- 13.Ghandour RM, Sherman LJ, Vladutiu CJ, et al. Prevalence and treatment of depression, anxiety, and conduct problems in US children. J Pediatr. 2019;206:256–267.e3 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Danielson ML, Bitsko RH, Ghandour RM, et al. Prevalence of parent-reported ADHD diagnosis and associated treatment among U.S. children and adolescents, 2016. J Clin Child Adolesc Psychol. 2018;47(2):199–212 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Jones SE, Ethier KA, Hertz M, et al. Mental health, suicidality, and connectedness among high school students during the COVID-19 pandemic - Adolescent Behaviors and Experiences Survey, United States, January-June 2021. MMWR Suppl. 2022;71(3):16–21 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Baweja R, Brown SL, Edwards EM, Murray MJ. COVID-19 pandemic and impact on patients with autism spectrum disorder. J Autism Dev Disord. 2022;52(1):473–482 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.World Health Organization. The Impact of COVID-19 on Mental, Neuro-logical and Substance Use Services. World Health Organization; 2020 [Google Scholar]
- 18.Straub L, Bateman BT, Vine S, Huybrechts KF. Prevalence of mental health diagnoses in commercially insured children and adolescents in the US before and during the COVID-19 pandemic. JAMA Netw Open. 2023;6(5):e2314415. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Kirsch AC, Huebner ARS, Mehta SQ, et al. Association of comorbid mood and anxiety disorders with autism spectrum disorder. JAMA Pediatr. 2019;174(1):63–70 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Lu W, Todhunter-Reid A, Mitsdarffer ML, et al. Barriers and facilitators for mental health service use among racial/ethnic minority adolescents: a systematic review of literature. Front Public Health. 2021;9:641605. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Bailey RK, Mokonogho J, Kumar A. Racial and ethnic differences in depression: current perspectives. Neuropsychiatr Dis Treat. 2019;15:603–609 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Ludi E, Ballard ED, Greenbaum R, et al. Suicide risk in youth with intellectual disabilities: the challenges of screening. J Dev Behav Pediatr. 2012;33(5):431–440 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.Marlow NM, Xie Z, Tanner R, et al. Association between disability and suicide-related outcomes among U.S. adults. Am J Prev Med. 2021;61(6):852–862 [DOI] [PubMed] [Google Scholar]
- 24.Panchal N, Cox C, Rudowitz R; KFF. The landscape of school-based mental health services. Available at: https://www.kff.org/other/issue-brief/the-landscape-of-school-based-mental-health-services/#:~:text=Going%20into%20the%202022%2D2023,fill%20these%20mental%20health%20positions. Accessed June 10, 2023
- 25.Hughes MM, Shaw KA, DiRienzo M, et al. The prevalence and characteristics of children with profound autism, 15 sites, United States, 2000–2016. Public Health Rep. 2023;138(6):971–980 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26.Eaton C, Tarver J, Shirazi A, et al. A systematic review of the behaviours associated with depression in people with severe-profound intellectual disability. J Intellect Disabil Res. 2021;65(3):211–229 [DOI] [PubMed] [Google Scholar]
- 27.Bradshaw CP, Buckley JA, Ialongo NS. School-based service utilization among urban children with early onset educational and mental health problems: The squeaky wheel phenomenon. Sch Psychol Q. 2008;23:169–186 [Google Scholar]
- 28.So M, McCord RF, Kaminski JW. Policy levers to promote access to and utilization of children’s mental health services: a systematic review. Adm Policy Ment Health. 2019;46(3):334–351 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29.The Individuals with Disabilities Education Act: A Comparison of State Eligibility Criteria. 2020;1–46 [Google Scholar]
- 30.Jackson D, Bowdon J. Spotlight on students with disabilities. Available at: https://www.air.org/sites/default/files/COVID-Survey-Spotlight-on-Students-with-Disabilities-FINAL-Oct-2020.pdf. Accessed June 10, 2023 [Google Scholar]
- 31.Additional Information Regarding the Requirements to Request a Waiver from the One Percent Cap on the Percentage of Students Who May Be Assessed with an Alternate Assessment Aligned with Alternate Academic Achievement Standards (AA-AAAS) (United States Department of Education Office of Elementary and Secondary Education) (2018). https://sites.ed.gov/idea/idea-files/policy-memo-to-states-regarding-the-cap-on-the-percentage-of-students-who-may-be-assessed-with-an-alternate-assessment-auǵ-27-2018/
- 32.Power D; Organization for Autism Research. Applying for social security disability benefits with autism. Available at: https://researchautism.org/blog/applying-for-social-security-disability-benefits-with-autism/. Accessed May 16, 2023
- 33.White PH, Cooley WC; Transitions Clinical Report Authoring Group; American Academy of Pediatrics; American Academy of Family Physicians; American College of Physicians. Supporting the health care transition from adolescence to adulthood in the medical home. Pediatrics. 2018;142(5):e20182587. [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.