

Abstract
Medical professionals face high stress due to the type of work they do and the prolonged working hours. Frequent burnout results due to the challenging nature of their work. Added to the stress of work, malpractice lawsuits add to their burden. In India, most doctors work in compromised settings with poor infrastructure and manpower but are expected to follow the best practices. In court, they are judged with the Bolam and Bolitho tests being essential considerations. Several tragic incidents have been reported, including depression, anger issues, and even suicide deaths of healthcare professionals (HCPs) after accusations of negligence and subsequent inquiry. Such incidents demonstrate the multitude of challenges an HCP faces in day-to-day practice. It is crucial to find ways to tackle these problems and enhance the capacity of HCP to handle such demanding circumstances. Malpractice litigation can significantly impact the mental health of HCPs. It is common to experience emotional turmoil when faced with a lawsuit. Second victim syndrome (SVS) is a term used to describe a set of symptoms experienced by HCPs who make an error leading to injury to a patient. However, it also happens if he is traumatized by the consequences of violence during healthcare services or a lawsuit or defamation article in newspaper/social media. Following a litigation crisis in their career, many HCPs go through various stages of grief, including shock, denial, anger, bargaining, depression, and acceptance. At times, death by suicide of the HCPs is well known. SVS is known to profoundly affect the personal, family, economic, professional (defensive practice), and social life of HCPs. HCPs should accept the allegations of negligence as an occupational hazard and prepare for the eventual litigation at least once in a lifetime by knowing about the medical laws, HCP's rights, becoming aware of the emotional turmoil of the lawsuit, preparing to cope with the lawsuit, and seeking help from colleagues and indemnity insurance. Frequent training of the HCPs is strongly recommended to know about the changing laws and also to undergo periodic professional competence enhancement to reduce the incidents of errors amounting to medical negligence. Medical and hospital administration should debrief after any incident and conduct internal investigations to identify systemic flaws and prevent future recurrence, resolve issues within their control at their level, and manage media (mainstream and social media) appropriately. If established, a reporting system with online and offline services will ease the internal administrative investigation process and take appropriate, timely actions. During the crisis, HCPs should have adequate and appropriate insurance or indemnity coverage and mental health support systems.
Keywords: Defensive medicine, health care providers, indemnity insurance, malpractice, professional negligence
INTRODUCTION
“Every time a patient dies, A part of me dies too.” – Unknown.
The medical profession is unique and challenging, with high levels of stress and burnout.[1,2] Unexpected or adverse patient outcomes can occur due to various factors, including disease progression, delay in seeking medical help, complications beyond the health care provider (HCP) control, non-adherence to medical advice, unscientific treatments, or medical errors. Several cases of ‘medical errors’ have been reported in the literature, including operating on the wrong side or giving medicine to a patient who is allergic to it, surgical errors during major surgeries, suicide or physical harm resulting from the behaviour of patient with mental illness, failure to monitor medication side effects leading to organ-system damage, and boundary violations in psychotherapy.[3,4] Each of these events can lead to malpractice claims. However, malpractice claims may occur even without a medical error being committed, and examples are extravasation injuries, bile leak from aberrant bile duct despite perfect laparoscopic cholecystectomy, pancreatitis following ERCP and hypoxic injuries of the brain despite proper resuscitation, Steven Johnson Syndrome, and so on.
Per se, “medical errors” are well studied in the literature. But there is a dearth of literature on the consequences of medical errors or medical negligence claims on the HCPs. HCPs can get affected in many ways, such as physical injury from violence against HCPs (personal), legal notices from patients/families, inquisitions, suspension (legal), or even expungement of names from the medical practitioners’ register (occupational). Even with the best HCPs, errors, complications, and adverse unexplained outcomes can occur, and such events might lead to emotional turmoil and other mental health issues in HCPs. However, all medical errors cannot necessarily be attributed to negligence. Therefore, it is important to distinguish ‘medical error’ from ‘medical negligence’ and ‘malpractice’ [Table 1].[5]
Table 1.
Simplified definitions of medical error, negligence, and malpractice
| Legal terms | Descriptions |
|---|---|
| Medical error | A medical event of erroneous outcome |
| Medical negligence | A healthcare professional fails to meet the standard of care expected of someone in their position, resulting in harm to the patient |
| Medical malpractice | Medical malpractice is a subset of medical negligence and refers to the professional negligence or misconduct by a healthcare provider and involves gross negligence or misconduct that results in severe harm to the patient |
In India, one can file compensation suits for the damage caused by medical negligence in several courts, medical commissions, human rights commissions, and consumer forums. An aggrieved party can now file a police complaint against a physician for criminal negligence. The Supreme Court of India ruled that the Medical Services should be treated as “services” within the ambit of Section 2(1) (o) of the Consumer Protection Act, 1986. A complaint can be filed under the Consumer Protection Act, 1986 (a) in the District Forum if the value of services and compensation claimed is less than 20 lakh rupees, (b) before the State Commission if the value of the goods or services and the compensation claimed does not exceed more than 1 crore rupees, or (c) in the National Commission if the value of the goods or services and the compensation exceeds more than 1 crore rupees. However, Medical Services which are free of charge are not considered under the purview of this section.[6] The party can also claim for monetary compensations under Section 30 of the newly developed National Medical Commission (NMC) Act 2019. This Section 30 has raised serious concern among medical professionals because now NMC can also award compensation similar to Consumer Court. It was earlier argued that State Medical Councils under erstwhile MCI did not have powers to award monetary compensation to the aggrieved party. Hence, medical services must be covered under Consumer Protection Act, 1986. It is a ‘double jeopardy’ situation, where HCP will undergo the stress, expense, and potential injustice of facing repeated prosecution or punishment for the alleged offense.[7,8] Medical negligence, litigation, and their consequences on HCP are poorly addressed in the scientific literature, especially the psychological and mental health consequences. The objective of the review is to highlight the magnitude of the problem and consequences of litigation and to provide recommendations on how to handle medical negligence suits.
METHOD
Articles were searched using Medline through PubMed, Scopus, and Web of Science. The following search terms were used in various combinations: “Negligence”, “Malpractice”, “Litigation”, and “Consequences”. The initial “All field” search using “Negligence AND Litigation AND Consequences” revealed 952 articles [Figure 1]. We focused on recent publications and emphasized this review based on documents from India. We could not include any search results from the legal database. Based on the review, we have constructed this paper under the following headings: assessment of the magnitude of the problem, consequences of medical negligence litigation, and evidence-based recommendations for various stakeholders.
Figure 1.
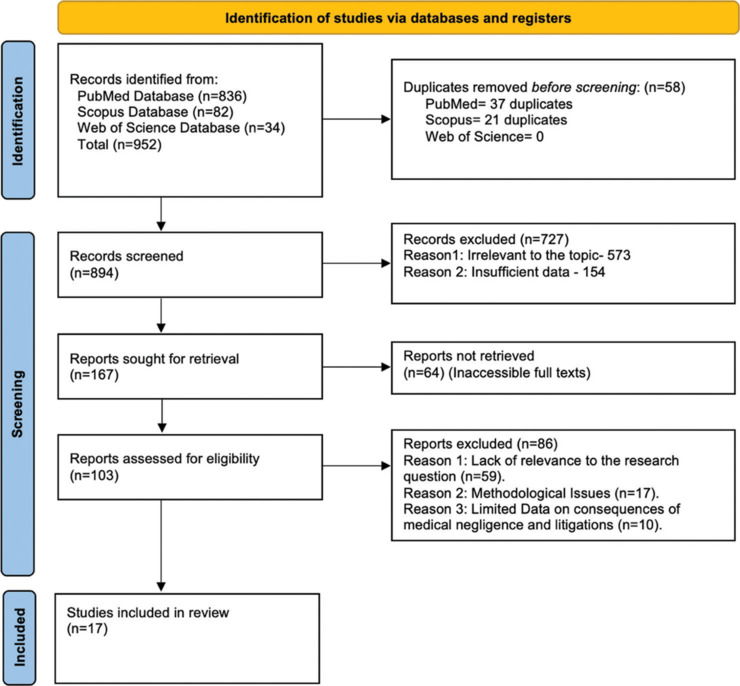
PRISMA flow chart for study selection process
MAGNITUDE OF THE PROBLEM OF MEDICAL NEGLIGENCE IN INDIA
Rising litigations on HCPs
There are no systematic data on lawsuits filed against HCPs for medical negligence in India over the years. In one of the first compilations of cases of medical negligence decided by Indian Courts, a total of 113 cases were found till 1995. Only NCDRC, in one year, 2015–2016, decided on 66 medical negligence cases. All State Consumer Dispute redressal commissions do not upload their data on the NCDRC website. District forum cases of medical negligence can only be guessed. In Punjab and Haryana till from 2009 to 2014, 74 cases were filed in police stations against doctors for criminal negligence. It is to be understood that for every case decided by courts, 20 cases are pending, and this number is constantly rising. Since the formation of the National Medical Commission under the NMC Act 2019, changes have been made in the power of the respective state medical councils. A report publicly available from the NMC website has enlisted the details of all the doctors who were found guilty of medical negligence or misconduct from January 2011 to January 2013. Out of 75 (N = 75) cases, most cases (N = 13) received strong warnings to be more cautious, followed by suspension during the trial period and expungement of names from the medical register for various duration ranging from 15 days to 5 years. Most cases were reported from Delhi (N = 12) and Haryana (N = 12) states. However, these data are only for 2 years and far from a comprehensive list of all civil and criminal medical negligence cases against doctors.[9]
Understandably, a medical negligence suit is an emotionally devastating experience for the HCP. These cases demonstrate the importance of informed consent, communicating effectively with patients and their families, following best clinical practices and guidelines, and handling pressure situations.
Malpractice litigation and rising suicides among doctors
“I have done nothing wrong and not killed anyone… Perhaps my death might prove my innocence” – Dr Archana Sharma wrote in her suicide note, 2022.
A prominent gynecologist in India tragically took her life by hanging herself after being falsely accused of the death of a young woman during a routine procedure. In her suicide note, she pleaded for innocent doctors to be protected from baseless accusations and harassment, emphasizing the need to support and safeguard doctors.[10]
“Dead people can't be put on trial, so the obvious solution is for me not to be alive” – Dr Michael McPhillips wrote in his suicide note in 2022.
A highly regarded psychiatrist from West London also committed suicide after receiving communication from the General Medical Council (GMC) that led to his state of mind. The GMC's procedures have been criticized for making doctors under investigation feel guilty until proven innocent, resulting in several suicides. The organization has since reformed its approach to be more supportive and compassionate toward doctors under investigation, providing free and confidential emotional support from fellow doctors. However, the tragic death of Dr McPhilips highlights a crucial point that even psychiatrists are not protected from the adverse mental health consequences of malpractice litigations.[11]
These are the two among many recent cases of suicide among HCPs due to the psychological burden and tremendous social pressure arising from litigations due to alleged medical negligence. There are no systematic data on this important mental health issue of the HCPs themselves. But such incidents kept occurring across the globe. Evidence-based systematic reforms are the need of the hour to avoid such unfortunate incidents in the future.
Rising violence on doctors
Doctors facing medical negligence suits must also deal with the growing concern of violence against them worldwide. According to the World Health Organization (WHO) data, between 8% and 38% of health workers suffer physical violence at some point in their careers. Publicly available data have shown 220 reported violence cases against HCPs since 2016. This number contributes to 3.4% of global cases, 5 times higher than the global average. Countries like Nepal, the United Kingdom, and China have 4, 57, and 850 times lesser incidents rates, respectively.[12] Many reports say that patients’ relatives and surrounding mobs often perpetrate violence. Factors contributing to violence include negative media portrayal, perception of financial or political gain by perpetrators, perceived negligence on duties by doctors, long waiting times for patients, inadequate grievance redressal systems, and perceived inadequate legal remedy.[13] COVID-19 has highlighted the severity of the scenario with a sharp rise in violence against HCPs in India.[14] In a recent event, a 25-year-old house surgeon at a taluk hospital in Kollam, Kerala, was stabbed to death by an accused patient when police brought him to treat his injured legs and hands. The Indian Medical Association said the authorities had been repeatedly warned of growing attacks on doctors and health professionals, but their specific demands remain unheard.
Clearly, HCPs are facing the brunt of the heat linked to the violence from angry mobs or poorly guarded convicted patients, especially under unproven medical negligence. The lack of systematic data on this sensitive issue has made it difficult for the governing authorities to act appropriately. This paper will discuss the psycho-social impact of medicolegal cases, inquiries, court proceedings, and violence on HCPs and various recommendations to manage such scenarios.
IMPACT AND OUTCOME OF MEDICOLEGAL CASES ON HEALTH CARE PROVIDERS
Emotional and psychological impact
4.1.1. Stress: Litigations can cause significant emotional distress, leading to increased stress and anxiety among doctors. The prolonged process of litigation can contribute to feelings of burnout, impacting job satisfaction and overall well-being.
4.1.2. Grief: Dr Elizabeth Kubler-Ross introduced the model for the psychological reaction to imminent death in her book.[15] This model was subsequently applied to the experience of loss in many contexts, including grief and other significant life changes. HCPs can undergo similar stages of emotional turmoil once they face medico-legal suits [Table 2].
Table 2.
Stages of emotional reactions in HCPs after negligence litigation
| Emotional response to Litigation | Description |
|---|---|
| Shock | • The normal response to litigation when an HCP is confronted • Manifested as feeling numb, dazed or confused • This may persist for hours to days |
| Denial | • HCP may use denial as a defence mechanism to cope with the stress of being sued • If the medical error was unintentional, they might refuse to accept their mistake and believe they did everything to prevent it • Denial can prevent them from taking responsibility and addressing patient concerns, making the legal process more difficult |
| Anger | • Medical negligence suits can evoke anger in HCPs, especially if they believe they provided the best care • This emotion may be directed toward the patient, their family members, HCPs' own family, or oneself • Anger can also serve as a defense mechanism to cope with guilt, shame, and inadequacy that come with being sued |
| Bargain | • HCPs may feel guilty or responsible for the adverse outcome associated with a medical negligence suit • Bargaining may involve trying to negotiate with the patient or their family to resolve the suit or find a way to make amends • It is essential to recognize that bargaining is not always a productive or appropriate response to a medical negligence suit • Bargaining may also be seen as an admission of fault, which can have legal and professional consequences |
| Depression | • It is characterized by low mood, loss of interest, fatigability, decreased concentration, loss of appetite, and low self-esteem • Sometimes, the depression can become severe enough to lead to suicidal thoughts or attempts • The legal process can be lengthy and stressful, and the negative impact on their professional reputation and emotional well-being can be significant • The fear of losing their licence or being sued again can lead to persistent anxiety and depression |
| Acceptance | • Acceptance in the context of medical negligence suits for HCPs can involve acknowledging that a mistake was made and taking responsibility for it • It can also involve accepting the legal consequences of the situation, such as accepting a settlement or a ruling against them • Acceptance can be difficult, but the desired stage to reach • By accepting the situation and taking steps to learn from it, HCPs can move forward and strive to improve their practice to prevent similar mistakes in the future • Acceptance can also involve seeking support and coping strategies to manage any ongoing emotional or mental health issues resulting from the experience |
4.1.3. Second Victim Syndrome: Albert Wu (2000) coined the term second victim syndrome (SVS), a condition unique to healthcare personnel. SVS is a set of symptoms experienced by doctors who make an error and are traumatized by the consequences. Symptoms include psychological, cognitive, and physical reactions such as shame, guilt, anxiety, grief, depression, compassion, dissatisfaction, burnout, and secondary traumatic stress.[16] Later, Scott and colleagues described six stages of SVS [Table 3]. These stages may have some thematic overlap with the stages of grief by Kuber-Ross. If SVS continues untreated, it may progress to develop fully formed post-traumatic stress disorder.[17]
Table 3.
Stages of SVS adapted with permission from the University of Missouri Health System (for You Team)
| Staging | Stage characteristics | Common questions in mind |
|---|---|---|
| Stage 1: Chaos and Accident Response | Error realized/event recognized Tell someone→get help May not be able to continue care of patient Distracted Experience a wave of emotions |
How did that happen? Why did that happen? |
| Stage 2: Intrusive Reflections | Re-evaluate scenario Self-isolate Haunted re-enactments of event Feelings of internal inadequacy |
Why did I miss? Could this have been prevented? |
| Stage 3: Restoring Personal Integrity | Acceptance among work/social structure Fear is prevalent |
What will others think? Will I ever be trusted again? How much trouble am I in? How come I can't concentrate? |
|
| ||
| (Stages 1–3 may occur individually or simultaneously) | ||
|
| ||
| Stage 4: Enduring the Inquisition | Realization of level of seriousness Reiterate case scenario Respond to multiple “why's” about the event Interact with many different ‘event’ responders Understanding event disclosure to patient/family Litigation concerns emerge |
How do I document? What happens next? Who can I talk to? Will I lose my job/license? How much trouble am I in? |
| Stage 5: Obtaining Emotional First Aid | Seek personal/professional help Getting/receiving help/support |
Why did I respond in this manner? What is wrong with me? Do I need help? Where can I turn help? |
| Stage 6: Moving On | Dropping out Transfer to a different unit or facility Consider quitting Feelings of inadequacy |
Is this the profession I should be in? Can I handle this kind of work? |
| Surviving Coping, but still have intrusive thoughts Persistent sadness, trying to learn from event |
How could I have prevented this from happening? Why do I still feel so badly/guilty? |
|
| Thriving Maintain life/work balance Gain insight/perspective Does not base practice/work on one event Advocates for patient safety initiatives |
What can I do to improve our patient safety? What can I learn from this? |
|
Professional and social reputation
Litigations and adverse outcomes can harm a doctor's professional reputation within the medical community and among patients. Malpractice litigations can erode patient trust and strain doctor–patient relationships. Losing a professional reputation also affects social stature, often leading to ostracization, hostile confrontation, and familial isolation.
Financial impact
HCPs may experience higher malpractice insurance premiums following malpractice litigation, potentially affecting their financial stability. Defending against malpractice litigations can result in substantial legal expenses, even if the HCP is found not liable. Financial loss can also occur if suspended for long or legal registration is canceled due to the inability to resume practice.
Time and productivity
HCPs involved in malpractice litigations must dedicate significant time to legal proceedings, removing them from patient care and other professional responsibilities. Litigations can disrupt HCPs’ workflow, potentially impacting their productivity and quality of life. Overt involvement with the litigation process may also lead to a lack of quality time with family and friends.
Practice changes
4.5.1. Defensive medicine: Doctors may adopt defensive medicine practices, such as ordering unnecessary tests or procedures, to minimize the risk of future litigation. Some doctors may choose to change specialities or areas of practice following malpractice litigation, especially if they feel particularly vulnerable to future claims.[18]
4.5.2. Work environment: Litigations involving an HCP can create a ripple effect, causing stress and anxiety among colleagues and impacting the overall work environment. The serving HCP may be asked to take an administrative break, get suspended, or lose a job, especially when working in a corporate set-up.
Patient care
Litigation can distract doctors, potentially affecting their ability to provide optimal patient care. Doctors facing malpractice litigations may reduce their patient load or leave certain practice areas, reducing patient care access. In worse scenarios, a serving doctor may make more mistakes under extreme psychological pressure from the fraternity, family, and society.
Professional development and advancement
Malpractice litigations can impede a doctor's career advancement, potentially limiting promotion opportunities or leadership roles. Doctors involved in litigations may need to allocate additional time and resources to fulfil legal requirements or educational programs related to risk management and medical ethics. Most doctors end up practicing defensive medicine and start avoiding high-risk procedures. Since courts decide cases in leisurely decades, doctors with many years of experience stop doing high-risk procedures. This is a loss of crucial human resources for society.
To sum up, HCPs can experience troubles from multiple dimensions and in various severities [Figure 2]. When left unresolved, these problems may lead to anxiety, depression, chronic insomnia, substance use, and not uncommonly suicidal ideas and self-harm attempts. Immediate attention should be drawn to address this rarely highlighted issue.[2]
Figure 2.
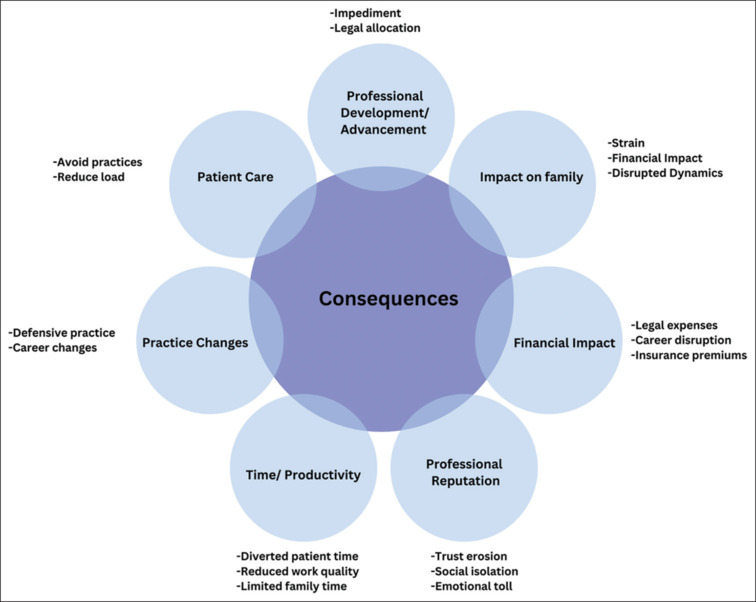
Consequences of medical negligence litigation on HCPs
RECOMMENDATIONS ON HOW TO HANDLE MEDICAL NEGLIGENCE SUITS
Recommendations for practitioners
(a) Occupational hazard: Proactive steps to becoming aware, accepting, identifying, and mitigating occupational hazards by implementing preventive steps and learning to deal with such situations effectively; (b) Continuing medical education and professional development: Continuing medical education (CME) is essential for healthcare providers to stay up-to-date on the latest medical advances, procedures, medical laws, and best practices; (c) Emotional impact of the medical lawsuits: HCPs should know the emotional impact of the medical lawsuit and seek help from mental health professionals. They should avoid poor coping skills such as alcohol use, drug abuse, and defensive practice; (d) Addressing physician burnout and stress: Physician burnout and stress can contribute to medical errors and negligence lawsuits. HCP burnout and stress should be managed by promoting work–life balance and supporting positive mental health. (e) Addressing suicide: Stress due to medical negligence litigation and family disputes may lead to suicidal ideas and attempts. Medical professionals should take immediate help for suicidal ideation to avoid further adverse consequences. (f) Medico-legal expert opinion: HCPs should actively seek help from medical experts and legal experts to address the issue at hand. Proper legal advice at proper stage will prevent long-term harassment in courts. (g) Encouraging a culture of safety: Safety culture includes promoting open communication among staff, encouraging staff to report incidents and near-misses, and regularly assessing/improving patient safety processes. (h) Effective patient–doctor communication skills: Open communication between the doctor and patient builds confidence, improves compliance, and reduces mistakes and mishaps, thereby reducing malpractice suits. Training in breaking bad news can decrease. (i) Training in communicating bad news: Lack of sufficient training in breaking bad news is a handicap to most physicians and health care workers. Periodic training is essential. (j) Indemnity insurance: A professional indemnity offers financial protection to medical practitioners in case of legal disputes and compensation claims made by patients. Professional Indemnity Insurance covers the economic damage resulting from unintentional errors and omissions made by the insured doctor, qualified and non-qualified employees, and staff. Some insurance companies also cover the cost of legal defense in court within their indemnity insurance. The policy does not cover criminal actions. Doctors must ensure that they have appropriate and adequate insurance or indemnity arrangements to cover all aspects of their medical practice. Besides personal and professional indemnity insurance, doctors must also take error and omission policies for the clinical establishment.
Recommendations for institutions
Doctors are divided by specialities/super-specialities and not united by MBBS degree. This needs to stop and focus on developing family physician culture in society. Professional societies, associations, bodies, and corporate institutes have a significant role in managing medical negligence litigations’ consequences. The institutions should adopt the following steps: (a) Security: Adequate security measures to prevent violence against HCPs and also have rapid response systems to deploy medical professionals in the neighborhood in case of any violence against HCPs; (b) Design and infrastructural changes, like furniture being fixed to floor, wide counters so an aggressor cannot reach across, safe rooms, CCTV cameras, proper lighting, and escape doors; (c) SOPs, institutes need to have regular training drills of Standard Operating Procedure in case of anticipated or actual violence. Follow the “broken window” hypothesis (Wilson and Kelling 1982) to prevent encouraging more serious crimes. (d) Coping with lawsuits: There is an urgent need to train HCPs in coping with occupational hazards; (e) Case conferences: Medico-legal case conference presented by the doctor/team who have been involved in the conflict with patient and debriefing of such cases at the association level; (f) Media Management: Institutions need to have media management cells to deal with both online and offline media regarding such cases to give the medical perspective of the case to the public at large; (g) Medico-legal cells: All professional bodies need to have medico-legal cells to counsel and support systems to reduce undue stress experienced by doctors involved in lawsuits and related matters. Collaborating with legal experts and professional organisations can help healthcare providers stay supported, guided during the tough times, up-to-date on legal issues and best practices; (h) Mental Health Support: Access to psychological first-aid, counseling and treatment provisions for depression, substance use, and other serious mental health conditions for HCPs is need of the hour; (i) Indemnity Insurance: All institutions and professional bodies should have a mandatory provision for indemnity insurance for all the practising HCPs in the institute whether they are residents, trainees or consultants; (j) Risk Management: A robust risk management program that includes processes for identifying potential risks, reporting incidents, and conducting investigations. Institutional debriefing of medical error events will help everyone be on the same page and reduce confusion and the risk of blaming each other. A thorough debriefing of all the staff involved will also help avoid erroneous statements during court hearings. (k) Dispute resolution: Traditional litigation can be time-consuming, expensive, and emotionally draining for patients and HCPs. If alternative Methods of Dispute Resolution within the legal framework implemented may ease the emotional turmoil of the litigation, they should be adopted. Further internal reporting and surveillance systems can resolve many cases before reaching the legal justice system. A multi-modal, easy-to-access, and quickly responding grievance resolution service will be able to mitigate many cases before escalation. (l) CME topics: Should incorporate topics related to medical negligence suits into the CME and staff training programs.[19]
Recommendations for governments and governing bodies
Central and state governments must be critical in mitigating the rising litigation and violence against HCPs. Several systematic changes are needed to be incorporated into the existing functioning of the health, justice, and social systems. (a) Health Education: Incorporation of topics related to medical negligence and litigations into the medical curriculum nationwide, beginning with medical school and continuing through residency training; (b) Health services: There should be a well-established online and offline “grievance redressal system” with responsible bodies or boards involved in free, fair, and quick internal investigation and countermeasures; (c) On-service safety: Provision of safety measures for the HCPs including adequate guarding of the hospital and zero tolerance for any violence in any healthcare establishment; (d) Compulsory indemnity insurance: There should be provisions for compulsory indemnity insurance for all HCPs by the government, the medical bodies, or other agencies; (e) Judicial reforms: Clear rules and regulations on various civil, criminal, and consumer protection litigations lodged against HCPs. Compensation and quantum of punishment should also be documented for quick, equitable, and fair judicial action. The same information can be used to educate the HCPs. Simultaneous prosecution in multiple courts, commissions, and fora on the same issue between same parties must be forbidden; (f) Compensation capping: The central and state governments should have legislation with compensation capping for various identified medical negligence scenarios.[16] The absurdly huge quantum of compensation awards is doing a disservice in providing healthcare to the masses; (g) No-fault liability: A provision for immediate compensation of the aggrieved parties must be considered. May adopt a system similar to that of some Scandinavian countries, which separates a doctor's accountability from compensation by utilizing a contractual Patient Compensation Insurance or Indemnity insurance; (h) Helpline for HCPs: A national helpline for HCPs for psychological and other supports will be beneficial; (i) Legal actions: Those who are found guilty of violence against HCPs and destroy the hospital properties should be charged with appropriate laws [e.g., Epidemic Diseases (Amendment) Ordinance, 2020; Healthcare Service Personnel and Clinical Establishments (Prohibition of Violence and property damage) Bill, 2019; and Indian Penal Code, 1860] without undue delay especially to showcase the law-and-order structure of the country; (j) Medical Tribunal: Authors recommend having a dedicated “Medical Tribunal” to deal with all types of medical lawsuit so that HCPs are not harassed under different laws, different statutes, commissions, forums, and courts for single lawsuit. The objective of this tribunal shall be bringing all medical lawsuits under one umbrella, experts under one roof, reviewing compensation, the severity of punishments, and other complex scenarios.
Limitation
This review has some limitations. Despite all efforts, this review was not exhaustive inclusion of all articles related to medical negligence due to various reasons. We could not retrieve any article from legal databases. Many states and regulatory bodies do not have accessible data on medical negligence. Some information was obtained from news media articles (e.g., information related to the suicide of doctors following medical negligence lawsuit). The descriptive synthesis of the review was followed by recommendations, which had opinions from experts in the subject matter.
CONCLUSION
In conclusion, medical negligence litigation can have far-reaching consequences for HCPs, professionally and personally. Such litigations’ emotional and psychological impact can lead to stress, burnout, and even tragically suicides among doctors. Furthermore, violence against doctors is a growing concern worldwide.
Several recommendations are made to mitigate the impact of medical negligence litigation among HCPs, such as promoting mental health awareness, providing access to mental health resources, coping with lawsuits, becoming aware of medical laws, fostering a supportive workplace culture, and encouraging work–life balance. Institutions, governments, and other stakeholders also have to take up their responsibilities.
Overall, a comprehensive and evidence-based approach is needed to address the psycho-social impact of medical negligence litigation on healthcare providers and to create a safer and more supportive environment for doctors to provide the best possible patient care. By considering these recommendations, we can work toward a healthcare system that prioritizes the well-being of patients and healthcare providers. Otherwise, the time is close when defensive medicine will be a norm, with several significant impacts on the healthcare system, patients, and HCPs.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
Acknowledgement
University of Missouri Health System (forYou Team) for kindly allowing us to use the “Second Victim Syndrome Trajectory”.
REFERENCES
- 1.Rotenstein LS, Brown R, Sinsky C, Linzer M. The association of work overload with burnout and intent to leave the job across the healthcare workforce during COVID-19. J Gen Intern Med. 2023;38:1920–7. doi: 10.1007/s11606-023-08153-z. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Kesarwani V, Husaain ZG, George J. Prevalence and factors associated with burnout among healthcare professionals in India: A systematic review and meta-analysis. Indian J Psychol Med. 2020;42:108–15. doi: 10.4103/IJPSYM.IJPSYM_387_19. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Mela M, Luther G, Gutheil TG. Forty-five years of civil litigation against Canadian psychiatrists: An empirical pilot study. Can J Psychiatry. 2016;61:112–8. doi: 10.1177/0706743715625943. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Procyshyn RM, Barr AM, Brickell T, Honer WG. Medication errors in psychiatry: A comprehensive review. CNS Drugs. 2010;24:595–609. doi: 10.2165/11533710-000000000-00000. [DOI] [PubMed] [Google Scholar]
- 5.Price K. Towards a history of medical negligence. Lancet. 2010;375:192–3. doi: 10.1016/S0140-6736(10)60081-5. [DOI] [PubMed] [Google Scholar]
- 6.Joga Rao SV. Medical negligence liability under the consumer protection act: A review of judicial perspective. Indian J Urol. 2009;25:361–71. doi: 10.4103/0970-1591.56205. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Bal BS. An introduction to medical malpractice in the United States. Clin Orthop Relat Res. 2009;467:339–47. doi: 10.1007/s11999-008-0636-2. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.The Lancet Medical negligence: There are no winners. Lancet. 2018;391:2079. doi: 10.1016/S0140-6736(18)31119-X. [DOI] [PubMed] [Google Scholar]
- 9.NMC document: List of Doctors found guilty of Medical Negligence/Misconduct and Punished by Medical Council of India, New Delhi during Jan 2011 to 31.01.2013. Available from: https://www.nmc.org.in/wp-content/uploads/2018/01/Doctors_Guilty.pdf . [Last accessed on 2024 Mar 13] [Google Scholar]
- 10.Rajasthan: All accused in Dr Archana Sharma suicide case get bail. The Times of India. 2022 published online May 19. Available from: https://timesofindia.indiatimes.com/city/jaipur/all-accused-in-doc-suicide-case-get-bail/articleshow/91651064.cms . [Last accessed on 2023 Aug 03] [Google Scholar]
- 11.Dyer C. Psychiatrist died by suicide four days after learning of GMC investigation. BMJ. 2022;378:o2328. doi: 10.1136/bmj.o2328. [DOI] [PubMed] [Google Scholar]
- 12.Nair A, Zadey S. Ending violence against healthcare workers in India: A bill for a billion. Lancet Reg Health Southeast Asia. 2022;6:100064. doi: 10.1016/j.lansea.2022.100064. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Ghosh K. Violence against doctors: A wake-up call. Indian J Med Res. 2018;148:130–3. doi: 10.4103/ijmr.IJMR_1299_17. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Das N, Mishra P. Protecting healthcare workers from COVID-19 and the assaulting society: Indian perspective. Pharm Biomed Res. 2020;6:5–8. [Google Scholar]
- 15.Kübler-Ross E. London: Routledge; 1973. On Death and Dying. [Google Scholar]
- 16.Wu AW. Medical error: The second victim. The doctor who makes the mistake needs help too. BMJ. 2000;320:726–7. doi: 10.1136/bmj.320.7237.726. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Scott SD, Hirschinger LE, Cox KR, McCoig M, Brandt J, Hall LW. The natural history of recovery for the healthcare provider ‘second victim’ after adverse patient events. Qual Saf Health Care. 2009;18:325–30. doi: 10.1136/qshc.2009.032870. [DOI] [PubMed] [Google Scholar]
- 18.Chandra MS, Math SB. Progress in medicine: Compensation and medical negligence in India: Does the system need a quick fix or an overhaul? Ann Indian Acad Neurol. 2016;19:S21–7. doi: 10.4103/0972-2327.192887. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Dhadphale MR. Psychiatrist facing litigation. Indian J Psychiatry. 2019;61:405–8. doi: 10.4103/psychiatry.IndianJPsychiatry_316_17. [DOI] [PMC free article] [PubMed] [Google Scholar]