

Abstract
Aim
The mental healthcare system in Japan is transitioning from institution‐based to community‐based treatment. To prevent prolonged hospitalization and community integration of psychiatric patients, mental health social workers (MHSWs) are pivotal in coordinating post‐discharge arrangements for psychiatric inpatients. This study aimed to propose a care model to improve clinical outcomes in psychiatric emergency wards in Japan.
Methods
We conducted a mail‐in questionnaire survey targeting medical facilities with psychiatric emergency wards. We collected data of the psychiatric care system, including facility profiles, staffing conditions and caseloads, and the provided psychiatric services and treatment options. Using multiple regression analyses, we explored associations between these data and clinical outcomes, focusing on the average number of days for hospitalization and the integration of patients into a community.
Results
Data were collected from 82 facilities (response rate, 45.8%). The average number of days for hospitalization and community integration were 64.7 and 327.9 days, respectively. The caseloads for MHSWs were significantly associated with longer hospitalization (β = 0.31, p = 0.009) and shorter duration of community living (β = −0.28, p = 0.027).
Conclusion
The clinical performance in psychiatric emergency wards surpassed the Japanese government's targets regarding these outcomes. We found that heavy caseloads on MHSWs were associated with worse clinical outcomes for patients in psychiatric emergency wards. These findings suggest that reducing MHSW caseloads (≤20 cases) may be a potential interventional strategy to prevent prolonged hospitalization and promote successful community integration of patients.
Keywords: community transition, integration, mental health, psychiatric emergency services, psychiatric social workers
In this study on psychiatric care in Japan, the relationship between mental health social worker (MHSW) caseloads and clinical outcomes was investigated to improve patient care in psychiatric emergency wards. Data from 82 facilities revealed that high MHSW caseloads were linked to longer hospital stays and shorter community integration durations. The study suggests that maintaining MHSW caseloads at or below 20 cases could be an effective strategy to prevent prolonged hospitalization and enhance patient integration into the community.

INTRODUCTION
Japan's mental healthcare system has been facing challenges in the process of transitioning from facility‐based treatment to community care. Japan has a significantly higher number of psychiatric beds than the Organisation for Economic Co‐operation and Development (OECD) average, at 266 beds per 100,000 population compared to 66 beds per 100,000 population, respectively. 1 Despite the Ministry of Health, Labour and Welfare implementing the “Vision for Reform of Mental Health and Welfare” in 2004 with the aim of reducing long‐term care beds, 2 the approach has had a limited impact, with only approximately 25,000 beds being reduced between 2004 and 2018. 3 , 4 Furthermore, Japan has been facing a persistent issue of new long‐stay patients (NLS), where newly admitted patients remain in hospital for more than a year. The number of annual NLS cases has not decreased and has remained around 50,000 individuals annually for over a decade. 5
Meanwhile, deinstitutionalizing the mental healthcare system increases outpatient treatment instead of long‐term hospitalization, although it may increase readmission rates. 6 Therefore, it is imperative to focus on the duration of community living rather than solely on readmission rates. Consequently, for evaluating community transition and integration, key indicators of significant treatment outcomes are the reduction in NLS and the increase in the average number of days for community integration within a year of discharge.
The government announced a policy in 2014 under which new psychiatric inpatients will be discharged within a year. 7 This policy is aimed at enhancing psychiatric emergency medical services. These services serve two primary purposes: providing emergent medical interventions during crises with appropriate short‐term hospitalization and offering support to individuals battling mental illness in the community. 8 Specialized psychiatric emergency inpatient treatment is offered in wards that meet higher facility standards, with designated psychiatrists, nurses, and mental health social workers (MHSWs) to ensure comprehensive care.
The policy also emphasizes the establishment of post‐discharge living environment counselors and enhancing collaboration with community service providers of housing, home‐helpers, job assistance, and so forth, during hospitalization to promote the transition from inpatient to community‐based care. In 2017, the “Committee for the Future of Mental Health, Medical Care, and Welfare” under the Ministry of Health, Labour and Welfare clarified that it aims to establish a “comprehensive community care system that addresses mental disabilities” to enable individuals with mental disorders to be accepted as members of the community. 9 Therefore, this system strives to increase the discharge rate significantly within 1 year for newly admitted patients and establish a seamless collaboration with a comprehensive care system in the community that considers post‐discharge community living. Such a system is expected to significantly promote community integration, where individuals live a secure, independent life while enhancing the duration of community living.
A previous study has highlighted the importance of seamless care transitions for social and long‐term psychiatric patients, emphasizing the need for personnel and programs to facilitate these transitions. 10 Post‐discharge living environment counselors, established under the revision of the Mental Health and Welfare Act in April 2014, are central in coordinating post‐discharge arrangements for long‐term and socially dependent psychiatric patients. 11 MHSWs primarily hold the post‐discharge living environment counselor position, but there are no regulations regarding the specific number of patients they should be responsible for. It can be hypothesized that reducing the workload of MHSWs would promote post‐discharge support, leading to better outcomes, such as reducing the number of days spent living in the community. However, limited research has explored the relationship between caseload and services provided by various professions, including MHSWs, and treatment outcomes.
This study involved a nationwide survey involving medical facilities in Japan with psychiatric emergency units to collect information regarding facility characteristics, staffing (including MHSWs), resources, and post‐discharge support services to identify factors contributing to better treatment outcomes for community transition and stabilization. In the future, we propose an optimal care model that prioritizes allocating specialized professionals and providing services by analyzing the present findings. Ultimately, this model seeks to prevent prolonged hospitalization and promote successful community integration.
METHODS
Study design and ethics
This study employed a cross‐sectional design and utilized a questionnaire survey administered through mail to gather data. The anonymous questionnaire survey was conducted from November 11, 2021, to January 15, 2022. It did not collect respondents’ personal information, except for their occupation, as it was anonymous. Therefore, individual respondents cannot be identified. Returning the questionnaire was considered an agreement for participation, and participants were exempted from providing written informed consent. The facilities that participated were informed of the research details and the voluntary nature of participation. Consent to participate in the research was confirmed for all participants who completed the questionnaire and returned it. The study received ethical approval from the Ethical Review Committee of the Graduate School of Medicine, Chiba University, on September 15, 2021 (Approval No. 419).
Participants
The study included all 179 medical facilities nationwide with psychiatric emergency wards affiliated with the Japanese Association for Emergency Psychiatry. The respondents were identified as administrative staff and MHSWs affiliated with their respective facilities.
Questionnaire
We prepared several questionnaires that included basic information about the wards and their clinical practices. Questionnaire (1) asked about the number of wards and beds, rate of new admissions, rate of transition to home care within 3 months, number of personnel by occupation, and presence of affiliated facilities (see Supporting Information: Supplementary Table S1). Questionnaires (2) and (3) asked psychiatric emergency and chronic care wards, respectively, about their treatment programs, participating occupations, and other clinical practices with a focus on items reimbursed under the medical insurance system. Questionnaire (1) was answered by administrative staff, and Questionnaires (2) and (3) by MHSWs. Questionnaire (3) targeted chronic psychiatric wards, but the content has not been discussed in the main text, and no data have been presented. We also asked for the completion of a sheet that calculated the average number of days living in the community for 50 patients admitted to the emergency ward. The formula for calculating the average number of days living in the community was the total duration of stay in the community within a year of discharge divided by the total number of discharged patients within that year.
Outcomes
To assess the indicators of community transition and integration, we identified the following survey results as primary outcomes: average number of days living in the community and average number of hospital admission days. Additionally, we established secondary outcomes, including the rate of new admissions, rate of transition to home care within 3 months, and readmission rates within 30 days, 90 days, and 1 year.
Variables
The list of results obtained from the questionnaire survey used for the analysis in this study can be found in Supplementary Table S2. We utilized these data as independent variables for statistical analysis, encompassing the number and placement of professional staff and caseload, conference and risk evaluation, the type and presence of affiliated facilities, availability of treatment options (such as clozapine and modified electroconvulsive therapy), and the presence or absence of support and services after discharge, as well as collaboration with community assistance providers.
Data analysis
To examine the relationship between the outcome variables listed in Table 1 and the independent variables in Supplementary Table S2, a comprehensive correlation analysis was performed using Spearman's method. Candidate variables were identified based on a significance level of p < 0.2 and subsequently included in multiple regression analyses for each outcome variable. 12 We performed multivariate analysis using the extracted candidate variables to control for confounding factors. Three models were constructed: a crude Model 1 with all candidate variables, Model 2 using a stepwise method, and Model 3, which included the total number of hospital beds as a covariate, as presented in Supplementary Table S3. The independent variables used for Model 3, representing the final analysis results, are listed in Tables 1 and 2, and the results of Model 3 are summarized in Table 3. In conducting multiple regression analyses, statistical significance was determined by a threshold of two‐tailed p‐values of 0.05, with 95% confidence intervals considered appropriate. Furthermore, multicollinearity was evaluated by ensuring that all variance inflation factor values were below 10. All statistical analyses were conducted utilizing SPSS Version 28.0.
Table 1.
Dependent variable profiles.
| Number of responses | Mean (SD) | Median [range] | |
|---|---|---|---|
| Average number of hospital admission days | 67 | 64.7 days (11.91) | 66.8 days [31–87] |
| Average number of days of living in the community | 67 | 327.9 days (21.79) | 331.6 days [243–361] |
| New admission rate to emergency wards | 78 | 87.6% (11.86) | 92.0% [37–100] |
| Rate of moving to emergency wards within 3 months | 77 | 77.7% (8.975) | 77.0% [56–100] |
| 30‐day readmission rate | 67 | 7.7% (0.051) | 8.0% [0–20.4] |
| 90‐day readmission rate | 67 | 14.3% (0.079) | 14.0% [2.0–40.0] |
| 1‐year readmission rate | 67 | 36.1% (0.144) | 34.0% [8.0–100] |
Abbreviation: SD, standard deviation.
Table 2.
List of independent variables used in the final regression model (Model 3).
| Variable on staffing | Number of responses | Mean (SD) | Median [range] |
|---|---|---|---|
| Total number of psychiatric beds per facility | 82 | 268.90 (146.34) | 256.0 [42–806] |
| Number of psychiatric emergency beds per | |||
| Full‐time psychiatrist | 63 | 5.02 (2.08) | 4.8 [1.6–10] |
| Full‐time non‐designated psychiatrist | 60 | 18.44 (14.14) | 13.0 [2.22–60] |
| Physician in all departments (including part‐time) | 63 | 3.23 (1.64) | 2.9 [0.54–8.57] |
| MHSWs | 63 | 19.02 (6.39) | 20.0 [4.55–30] |
| Number of psychiatric emergency patients assigned per | |||
| MHSW average | 81 | 16.38 (6.49) | 15.0 [0–30] |
| Number of occupations per facility | |||
| Full‐time non‐designated psychiatrist | 66 | 5.56 (4.42) | 4.5 [0–21] |
| MHSW | 66 | 12.77 (6.32) | 12.0 [3–29] |
| Variable on service | Number of responses | Yes | % |
|---|---|---|---|
| Availability of annexed facilities | |||
| Day care for patients with severe dementia | 81 | 18 | 22.2% |
| Home‐visit nursing care station | 81 | 42 | 51.9% |
| Availability of services used for post‐discharge support | |||
| Home‐visit nursing care station of own corporation | 82 | 72 | 87.8% |
| Outpatient occupational therapy | 82 | 33 | 40.2% |
| Availability of services routinely performed in collaboration with community assistance providers | |||
| Joint hospital and community workshops or case conferences | 82 | 27 | 32.9% |
| Tours of community resources | 82 | 26 | 31.7% |
Abbreviations: MHSW, mental health social worker; SD, standard deviation.
Table 3.
Summary of multiple regression model.
| Variable | B | 95% CI | SE | β | p | ||
|---|---|---|---|---|---|---|---|
| Average number of hospital admission days (n = 66) | Number of psychiatric emergency patients assigned per MHSW (average) | 0.58 | 0.15 | 1.02 | 0.22 | 0.31 | 0.009 |
| Outpatient occupational therapy | −8.73 | −14.18 | −3.29 | 2.72 | −0.36 | 0.002 | |
| Average number of days living in the community (n = 66) | Number of psychiatric emergency patients assigned per MHSW (average) | −0.94 | −1.78 | −0.11 | 0.42 | −0.28 | 0.027 |
| New admission rate to emergency wards (n = 60) | Number of MHSWs | 0.53 | 0.06 | 1.00 | 0.24 | 0.32 | 0.029 |
| Number of psychiatric emergency beds per full‐time non‐designated psychiatrist | 0.23 | 0.04 | 0.42 | 0.10 | 0.31 | 0.018 | |
| 30‐day readmission rate (n = 67) | Tours of community resources | 0.03 | 0.01 | 0.06 | 0.01 | 0.29 | 0.021 |
| 90‐day readmission rate (n = 67) | Tours of community resources | 0.05 | 0.01 | 0.09 | 0.02 | 0.32 | 0.009 |
| 1‐year readmission rate (n = 67) | Home‐visit nursing care station of own corporation | 0.13 | 0.01 | 0.25 | 0.06 | 0.26 | 0.037 |
Note: The final multiple regression model (Model 3) was constructed by adjusting for the total number of beds in each facility and using the forced entry method to include candidate variables.
Abbreviations: β, standardized regression coefficient; B, regression coefficient; CI, confidence interval; MHSW, mental health social worker; SE, standard error.
Missing values were handled using pairwise deletion. Any data points with missing values were excluded from the analysis, and no imputation or other methods were employed to fill in the missing values.
RESULTS
Characteristics of the surveyed facilities
A questionnaire survey was conducted involving 179 facilities with psychiatric emergency wards nationwide. We received responses from 81 facilities for the facility overview questionnaire (response rate: 45.3%). For the psychiatric emergency and acute care unit questionnaire, we received responses from 82 facilities (response rate: 45.8%). Regarding the calculation sheet for the average number of days living in the community, we received responses from 68 facilities (response rate: 38.0%).
The characteristics of the surveyed facilities are as follows. Among the 81 facilities that responded, installation entities were distributed as follows: medical corporations accounted for 43% (35 facilities), other corporations 30% (25 facilities), public institutions 21% (17 facilities), government agencies 4% (three facilities), and national institutions 1% (one facility). Regarding the psychiatric care infrastructure, 428 psychiatric wards were identified across the surveyed facilities, providing a combined total of 22,040 psychiatric beds. On average, each facility had 5.2 psychiatric wards, with a standard deviation of 2.7. The number of wards ranged from a minimum of one to a maximum of 14. Similarly, the average number of psychiatric beds per facility was 268.8, with a standard deviation of 146.5. These findings provide an overview of the diversity and capacity of the surveyed facilities in terms of psychiatric care provision.
Key demographic data of the survey results
The results of the clinical outcomes (dependent variables) were as follows: the average number of hospital admission days was 64.7 days, the average number of days living in the community was 327.9 days, the rate of new admissions was 87.6%, the rate of transitioning to home within 3 months was 77.7%, the 30‐day readmission rate was 8%, the 90‐day readmission rate was 14%, and the 1‐year readmission rate was 36% (Table 1). The results for the independent variables, including staffing, services, and treatment options, are presented in Supplementary Table S2.
Correlation between the caseload of MHSWs and clinical outcomes
There was a significant correlation between the caseload of MHSWs and the average number of hospital admission days in psychiatric emergency wards (Figure 1). The correlation equation was y = 0.6436x + 54.115, with an R 2 value of 0.1166, a correlation coefficient (ρ) of 0.3432, and a p‐value of 0.005. Furthermore, a significant correlation was found between the caseload of MHSWs and the average number of days living in the community. The correlation equation was y = −1.0768x + 345.31, with an R 2 value of 0.1003, a correlation coefficient (ρ) of −0.388, and a p‐value of 0.001 (Figure 2). These results remained significant, demonstrating a robust relationship even after adjusting for the potential confounding variable of the total number of beds, which could act as a confounding factor in the subsequent regression analysis. However, although some other variables showed significant univariate associations, the significance disappeared after adjustment.
Figure 1.

Scatterplot of the caseload of mental health social workers (MHSWs) in psychiatric emergency wards and average number of hospital admission days. R 2, coefficient of determination; ρ, Spearman's correlation coefficient.
Figure 2.
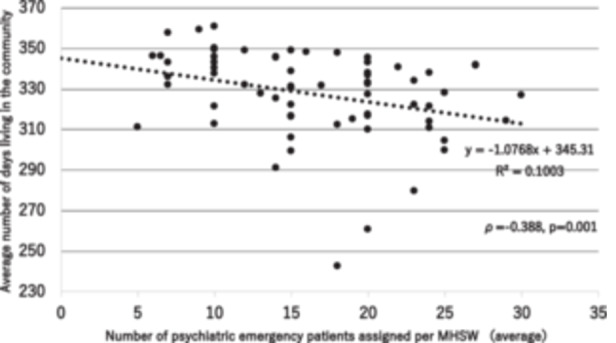
Scatterplot of the caseload of mental health social workers (MHSWs) in psychiatric emergency wards and average number of days of living in the community. R 2, coefficient of determination; ρ, Spearman's correlation coefficient.
Multiple regression analysis
The significant independent variables identified in the multiple regression analysis are summarized in Table 2. The final multiple regression model (Model 3), adjusted for the total number of beds, is presented in Table 3. For the average number of hospital admission days, a regression model was constructed with the average number of psychiatric emergency patients assigned per MHSW and outpatient occupational therapy as independent variables. The regression coefficients were β = 0.31 (p = 0.009) and β = −0.36 (p = 0.002), respectively. Regarding the average number of days of living in the community, a regression model was constructed with the average number of psychiatric emergency patients assigned per MHSW, resulting in β = −0.28 (p = 0.027). Concerning the new admission rate to emergency wards, a regression model was constructed with the number of MHSW and number of psychiatric emergency beds per full‐time non‐designated psychiatrist, resulting in β = 0.32 (p = 0.029) and β = 0.31 (p = 0.018), respectively. No significant independent variables were found for the rate of moving to emergency wards within 3 months. A regression model for the 30‐day readmission rate was constructed with tours of community resources as an independent variable, yielding β = 0.29 (p = 0.021). Similarly, the same independent variable, tours of community resources, was associated with the 30‐day readmission rate, resulting in β = 0.32 (p = 0.009). As for the 1‐year readmission rate, a regression model was constructed with home visits nursing care station of own corporation, resulting in β = 0.26 (p = 0.037).
DISCUSSION
The findings indicated that the average number of hospital admission days was 64.7 days, and the average number of days of living in the community was 327.9 days. The statistical analysis revealed significant correlations between these clinical outcomes and the caseload of MHSWs and several healthcare services.
In this survey, the average number of days of living in the community was 327.9 days, which was relatively long. In a previous survey conducted in 2018, the national average for days living in the community was 310 days, and the target value set by the government was 316 days or more, representing the level of the top 10% of prefectures. 13 It should be noted that the response rate for the survey was low, and there may be a bias in the selective participation of facilities with high activity levels and favorable outcomes.
The main outcomes for the average number of days living in the community and the average length of hospital stay were that the lower caseload of MHSWs resulted in favorable outcomes. An earlier study reported a minimum threshold of 16.3 patients per MHSW, 14 and our survey revealed a relatively low average caseload of 16.4 patients per MHSW. The correlation analysis yielded a linear function, indicating that assuming an average caseload of 20 patients per MHSW, the average number of days living in the community would be 323.8 days, and the average length of hospital stay would be 67.0 days, which could be considered reasonable levels.
The results of the multiple regression analysis suggest the following implications. The average length of hospital stay decreases when “the psychiatric emergency unit has a lower average caseload of MHSWs” and “outpatient occupational therapy is available.” Additionally, the average number of days living in the community increases when “the psychiatric emergency unit has a lower average caseload of MHSWs.” These findings are important as they indicate that a lower caseload for MHSWs leads to favorable treatment outcomes. These results have also been demonstrated in the previous simple regression analyses, and they maintain their robustness even when conducting multiple regression analyses with the inclusion of other variables or the adjustment for the confounding factor of total number of psychiatric beds. The relationship between MHSW caseload and both the average length of hospital stay and average number of days living in the community is consistently highlighted in this multiple regression analysis, underscoring the robustness of these associations. Although specific regulations regarding the caseload of MHSWs are currently lacking, future efforts are expected to focus on increasing the number of MHSWs or reducing their caseloads to facilitate smooth post‐discharge support and community living.
There are several possible reasons why outpatient occupational therapy is associated with a decrease in the average length of hospital stay. Compared to daycare programs that primarily focus on creating a supportive environment, outpatient occupational therapy tends to involve an increasing proportion of patients with relatively high‐level activities of daily living abilities. Moreover, outpatient occupational therapists likely possess strong assessment skills related to social functioning and other factors. They also provide individualized care tailored to each patient's specific needs. These factors may contribute to effective follow‐up care after discharge.
Regarding readmission rates, the following findings were observed. The presence of “community resource tours” is associated with increased 30‐ and 90‐day readmission rates. In contrast, “visiting nursing services provided by the organization” is associated with increased 1‐year readmission rates. As mentioned earlier, it is known that enhancing welfare services after discharge leads to higher readmission rates. 10 There is a possibility that collaboration with community resources and the availability of visiting nursing services lower the threshold for hospitalization. Therefore, it can be inferred that there is a tendency for a reduction in the average length of hospital stay when the organization provides visiting nursing services, suggesting their contribution to early detection and admission during exacerbations.
Furthermore, a multidisciplinary approach known as intensive case management, involving a team capable of providing comprehensive outreach services for individuals with severe mental illnesses, has been widely adopted in North America and Europe; it has contributed to the prevention of rehospitalization. 15 However, the adoption of such a multidisciplinary approach is limited in Japan, potentially contributing to the high readmission rates. Consequently, personnel in various community settings, including visiting nurses and welfare service staff, might exhibit a preference for referring individuals with severe mental illness or acute psychiatric symptoms to hospitals rather than providing support within the community. This systematic shortfall could be a contributing factor to the observed correlation between elevated readmission rates and the limited dissemination of welfare services in the community.
Potential limitations
As a limitation of this study, it should be noted that the survey's low response rate introduces a selection bias, as only hospitals with favorable outcomes may have participated. Additionally, the survey targeted facilities with psychiatric emergency units, excluding those with only chronic units or other types of facilities. Moreover, due to the study's cross‐sectional design, causal relationships cannot be established definitively.
Conclusions
Based on a nationwide survey of medical facilities in Japan with psychiatric emergency wards, the study found that the average number of hospital admission days was 64.7 days, and the average number of days for living in the community was 327.9 days. These results indicated favorable clinical outcomes compared to the government's target values. Furthermore, we found that heavy caseloads on MHSWs were associated with worse clinical outcomes for patients in psychiatric emergency wards. These findings suggest that the reduction of caseloads on MHSWs (≤20 cases) may serve as a potential intervention to prevent prolonged hospitalization and patient transition to a community in Japan.
AUTHOR CONTRIBUTIONS
Conception and design of the study: Kosuke Suzuki, Tomihisa Niitsu, Hiroshi Kimura, Yuta Yanagisawa, Marina Ono, Hideki Komatsu, Kensuke Yoshimura, Hiroyuki Watanabe, Masaomi Iyo. Acquisition and analysis of data: Kosuke Suzuki, Tomihisa Niitsu, Hiroshi Kimura, Yuta Yanagisawa, Marina Ono, Hideki Komatsu, Kensuke Yoshimura, Hiroyuki Watanabe, Masaomi Iyo. Drafting the manuscript or figures: Kosuke Suzuki, Tomihisa Niitsu, and Masaomi Iyo. All authors contributed to and approved the final manuscript.
CONFLICT OF INTEREST STATEMENT
Masaomi Iyo is an Editorial Board member of Psychiatry and Clinical Neurosciences Reports and a co‐author of this article. To minimize bias, they were excluded from all editorial decision‐making related to the acceptance of this article for publication. The remaining authors declare no conflict of interest.
ETHICS APPROVAL STATEMENT
The study received ethical approval from the Ethical Review Committee of the Graduate School of Medicine, Chiba University, on September 15, 2021 (Approval No. 419).
PATIENT CONSENT STATEMENT
By responding to the questionnaire and submitting the forms, the participating facilities are considered to have consented to collaborate in this study.
CLINICAL TRIAL REGISTRATION
N/A.
Supporting information
Supporting Information.
ACKNOWLEDGMENTS
The authors extend their gratitude to the medical facilities that participated in this study. They also wish to express their appreciation to Editage (www.editage.com) for their valuable assistance with English‐language editing. This study received support through a grant from the Japanese Ministry of Health, Labour, and Welfare under the Disability Policy Comprehensive Research Project (Grant No. 21GC1011).
Suzuki K, Niitsu T, Kimura H, Yanagisawa Y, Ono M, Komatsu H, et al. Association between mental health social worker staffing in psychiatric emergency wards and readmission outcomes: a nationwide survey in Japan. Psychiatry Clin Neurosci Rep. 2024;3:e189. 10.1002/pcn5.189
DATA AVAILABILITY STATEMENT
The data that support the findings of this study are available from the corresponding author upon reasonable request.
REFERENCES
- 1. Allison S, Bastiampillai T, Licinio J, Fuller DA, Bidargaddi N, Sharfstein SS. When should governments increase the supply of psychiatric beds? Mol Psychiatry. 2018;23:796–800. [DOI] [PubMed] [Google Scholar]
- 2. Japan Ministry of Health, Labour and Welfare . Vision for reform of mental health and welfare. 2004. [cited 2023 Sep 25]. Available from: https://www.mhlw.go.jp/topics/2004/09/dl/tp0902-1a.pdf
- 3. Japan Ministry of Health, Labour and Welfare . Medical facility survey. 2018. [cited 2023 Sep 25] Available from: https://www.mhlw.go.jp/toukei/saikin/hw/iryosd/18/dl/09gaikyo30.pdf
- 4. Tachimori H, Takeshima T, Kono T, Akazawa M, Zhao X. Statistical aspects of psychiatric inpatient care in Japan: based on a comprehensive nationwide survey of psychiatric hospitals conducted from 1996 to 2012. Psychiatry Clin Neurosci. 2015;69:512–522. [DOI] [PubMed] [Google Scholar]
- 5. Ministry of Health, Labour and Welfare . Policy for discharging long‐stay psychiatric patients to community. 2014. [cited 2023 Sep 25]. Available from: http://www.mhlw.go.jp/file/05-Shingikai-12201000-Shakaiengokyokushougaihokenfukushibu-Kikakuka/0000051138.pdf
- 6. Jeppesen RM, Christensen T, Vestergaard CH. Changes in the utilization of psychiatric hospital facilities in Denmark by patients diagnosed with schizophrenia from 1970 through 2012: The advent of ‘revolving door’ patients. Acta Psychiatr Scand. 2016;133:419–425. [DOI] [PubMed] [Google Scholar]
- 7. Ministry of Health, Labour and Welfare . National guideline for high quality and appropriate mental health care. 2014. [cited 2023 Sep 25]. Available from: http://www.mhlw.go.jp/seisakunitsuite/bunya/hukushi_kaigo/shougaishahukushi/kaisei_seisin/dl/kokuji_anbun_h26_01.pdf
- 8. Sugiyama N, Fujita K, editors. Guidelines for psychiatric emergency service. Tokyo: The Japanese Association for Emergency Psychiatry; 2022 (in Japanese).
- 9. Ministry of Health, Labour and Welfare . Building a comprehensive community care system for mental disorders. 2023. [cited 2023 Sep 25]. Available from: https://www.mhlw.go.jp/stf/seisakunitsuite/bunya/chiikihoukatsu.html
- 10. Ministry of Health, Labour and Welfare . Comprehensive study on understanding and optimizing the quality of psychiatric care. 2010. [cited 2023 Sep 25] Available from: https://mhlw-grants.niph.go.jp/project/16971
- 11. Ministry of Health, Labour and Welfare . Details regarding the implementation of the Act amending certain provisions of the Mental Health and Welfare for Persons with Mental Health Disabilities Law. 2014. [cited 2023 Sep 25]. Available from: https://www.mhlw.go.jp/seisakunitsuite/bunya/hukushi_kaigo/shougaishahukushi/kaisei_seisin/dl/shikou_gaiyo.pdf
- 12. Steyerberg EW. Clinical prediction models: a practical approach to development, validation, and updating. New York: Springer Cham; 2009. [Google Scholar]
- 13. Imamura T. Policy research for promoting establishment of medical service delivery system according to local realities. Grant‐in‐Aid for Scientific Research on Health and Labor Sciences for the Fiscal Year 2018 (Research Project for Promoting Development of Community Medical Infrastructure). 2019 [cited 2023 Sep 25]. Available from: https://mhlw-grants.niph.go.jp/project/28031
- 14. Japan Psychiatric Hospitals Association . Report on the national survey on the actual situation of medical protection hospitalization following the revision of the Mental Health and Welfare Act: Fiscal Year 2014 Health and Labour Sciences Research Grant Project for Comprehensive Promotion of Welfare for Persons with Disabilities. 2015 [cited 2023 Sep 25]. Available from: https://www.mhlw.go.jp/file/06-Seisakujouhou-12200000-Shakaiengokyokushougaihokenfukushibu/0000099530.pdf
- 15. Burns T, Catty J, Dash M, Roberts C, Lockwood A, Marshall M. Use of intensive case management to reduce time in hospital in people with severe mental illness: systematic review and meta‐regression. BMJ. 2007;335(7615):336. [DOI] [PMC free article] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
Supporting Information.
Data Availability Statement
The data that support the findings of this study are available from the corresponding author upon reasonable request.