

Abstract
The present article revisits the theoretical model of schizophrenia by Hiroshi YASUNAGA (1929–2011). Yasunaga restated ego disturbance in schizophrenia as the “Pattern Reversal” between selfhood and otherness, based on British philosopher Wauchope's concept of “pattern.” This concept is meant as asymmetrical relatedness (A/B) within a pair of concepts, such as life and death, quality and quantity, and self and other, prioritizing the former (A side) over the latter (B side). When applied to the pair of self and other, the pattern is vital for human experiences, and its disruption fundamentally alters every lived experience. Subsequently, Yasunaga extended the theory of pattern and invented his original “Phantom Space Theory,” in which he postulated “Phantom Space,” an experiential space that constitutes system a (A‐side‐led and consciously determined distance) and system a' (B‐side‐dominated and extra‐consciously given distance). He then constructed a kind of neural system model composed of systems a and a', and thereby schematically presented a novel viewpoint on experiences of self and the outside world. The theory further illustrated how the hypothesized imbalance (Phantom Space shrinkage or diminished elasticity of system a') causes symptoms of schizophrenia, such as ego disturbances, auditory hallucinations, and other unspecific symptoms. This article then examines the clinical and theoretical implications of Yasunaga's psychiatric works. Phantom Space Theory is a non‐stigmatizing account of schizophrenia because it does not presuppose personal or existential causes of psychosis. The relationship between Phantom Space Theory and dual‐process theory is also explored.
Keywords: delusion, dual‐process theory, ego disturbance, psychopathology, schizophrenia
The present article revisits the theoretical model of schizophrenia by Hiroshi YASUNAGA (1929–2011). Yasunaga restated ego disturbance in schizophrenia as the “Pattern Reversal” between selfhood and otherness, based on British philosopher Wauchope's concept of “pattern.” Subsequently, Yasunaga extended the theory of pattern and invented his original “Phantom Space Theory.”

INTRODUCTION
Despite great devoted research efforts, schizophrenia remains an enigmatic and often critical psychiatric disorder. Although its causes are still unclear, many researchers agree that certain neurobiological causes are central to its pathogenesis, but also admit that a combination of numerous other neurobiological and psychosocial factors likely contributes to its manifestation. Because a definitive neurobiological cause has not been singled out, even with today's cutting‐edge technologies, symptom description is still important in depicting the features of schizophrenia. However, clinicians find it difficult to understand the experiences that patients have. It is difficult to imagine what it would be like if one's own body and thoughts were manipulated from the outside, or if voices preempted what one was going to think. These symptoms are categorized by Schneider as “ego disturbance” because the patients seem to have lost “the barrier between the individual and [their] environment” (p. 44). 1 Although the current diagnostic criteria for schizophrenia from the Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition, Text Revision 2 and the International Classification of Diseases, 11th Revision 3 have shifted away from emphasizing the importance of Schneider's first‐rank symptoms, which are composed mostly of ego disturbance, these symptoms have considerable specificity in differential diagnosis 4 (see also Jauhar et al. 5 ). Ego disturbance is now subsumed under the broader concept of “self‐disorder” with the scope of self–other relatedness in current psychiatric practice, 6 , 7 and this viewpoint is continuously drawing research interest.
Recently, Sass 8 places studies on patients' experiences into the broader perspective of current psychiatric practice. Sass emphasizes that the “understanding of patients' subjective life is relevant to psychopathology as a scientific enterprise” (p. 165). He asserts that scientific psychiatry necessitates both subjective and objective approaches. He also addresses an ethical issue. Sass acknowledges that some people criticize inquiry into patients' pathology as insulting to the patients, but remarks that specifying the pathology is different from thinking negatively about the patients. Studying patients' experiences without stigmatizing their conditions thus remains a significant challenge.
The present article revisits the original and innovative approach to the psychopathology of schizophrenia by Japanese psychiatrist Hiroshi YASUNAGA (1929–2011). 9 , 10 , 11 , 12 , 13 , 14 , 15 , 16 Yasunaga aimed to understand the barely comprehensible symptoms of schizophrenia: those subsumed under ego disturbance. In analyzing ego disturbance, he applied the concept of “pattern” put forward by British philosopher Oswald S. Wauchope. 17 This concept encompasses the whole of human experiences, including the relationship between selfhood and otherness, which is an important focus in abnormal experiences in schizophrenia. Therefore, Yasunaga applied Wauchope's theory as the basis for understanding ego disturbance and other symptoms.
Yasunaga conducted his theoretical investigation on schizophrenia alongside his clinical work, and his sphere of activity was quite limited within Japan. Yasunaga 15 once gave a keynote lecture at an international conference, but all of his published works were in Japanese. As Choudhary and Choudhary 18 suggest, the academic world in the 20th century was not as globalized as it is at present. It is unfortunate that Yasunaga's achievements have not been recognized internationally. Therefore, this article presents his theory to international readers as a part of the project of introducing classical works on psychopathology in Japan. 19
Before going directly into Yasunaga's theories on schizophrenia, the present article first glimpses Wauchope's philosophy of pattern, followed by Yasunaga's application of pattern theory to psychopathology: the basic “Pattern Reversal” between selfhood and otherness, and the more elaborated “Phantom Space Theory” on self‐disorder in schizophrenia. Finally, some considerations are given to this theory's significance for current clinical practice and research: why Phantom Space Theory is non‐stigmatizing for patients, and how Phantom Space Theory can contribute to present and future research on schizophrenia.
WAUCHOPE'S PHILOSOPHY OF PATTERN
Wauchope was a Cambridge alumnus and independent thinker who evolved his original philosophy founded on the certainty of lively human experiences. At the beginning of his book Deviation into Sense, 17 Wauchope took “subjective non‐rational certitude of self” (p. 9) as the starting point of his argument. His style was very different from the formal approach of logical positivism, while his philosophy might have shared the common spirit of the times with British Ordinary Language Philosophy and G. E. Moore's Common Sense Philosophy. 20 Deviation into Sense was evaluated as “very remarkable” and having “great power of abstract thought, a delightful power of clear and forceful expression” in a book review in the journal Philosophy. 21 In another review, British philosopher Oakeshott 22 labeled the style of the book as “unprofessional,” despite identifying “enough genius” in it. However, Wauchope 17 willfully chose “less professional starting‐points” (p. 9) to examine lived experiences.
In Deviation into Sense, 17 Wauchope analyzed the basic structure underlying the ordinary and everyday experiences of human beings. His analysis revealed the polarity that existed between pairs of complementary categories, such as whole versus part, life versus death, self versus other, and quality versus quantity. For each pair, two contrasting concepts are inseparably associated. For example, the whole consists of parts, and the parts necessarily add up to form the whole. However, as Wauchope stressed, such close mutual connection does not mean that these pairs of concepts are symmetrical.
For example, people imagine death as “the negation of life” 17 (p. 28) from the perspective of living creatures having lived experiences. By contrast, it is utterly inconceivable that one might speculate about life from the standpoint of the dead: “life is not deviation from death” (p. 28). Put differently, people understand life without thinking about death, whereas they usually grasp death as the state of “having ceased living” (p. 28). Therefore, life has priority over death in our experiences and system of concepts. Similarly, other pairs of concepts have an asymmetrical structure in which one is conceptually prior to the other. Wauchope referred to the structure consisting of such concept pairs as “pattern.”
Wauchope did not aim to establish metaphysical dualism; rather, he simply discerned patterns of ordinary human experiences. He remarked on the polarity apparent in human experiences, but this polarity is not a dichotomy. For example, Wauchope observed how quality and quantity are mutually dependent. Although quality is conceptually prior to quantity, it is difficult to identify a certain abstract quality that does not have any quantitative aspects. On the other hand, people usually do not think of an abstract quantity devoid of quality. Such an abstract quantity “could not be within experience” 17 (Wauchope, p. 16) in our daily lives, although it may be investigated academically in mathematics. Therefore, quality contains quantitative aspects, and quantity is necessarily associated with quality.
Wauchope considered that pattern was not merely an abstract structure, but rather, endowed with lived experiences with varying degrees of intensity. Wauchope especially focused on such vigor of experiences in analyzing pleasurable or painful events. People, as living creatures, ceaselessly release energy responding to and operating on matters in the world outside them. Wauchope labeled such energy of the subject “A,” and the resistance or pressure from the objects in the outside world “B.” When an event has a very strong impact on a person, that event is painful. In such a case, the person barely survives the event, reacting with “death‐avoiding behaviour” 17 (Wauchope, p. 47). With regard to the relationship between the energy of the person (A) and the impact of the event (B) as illustrated in Figure 1, B is nearly equal to A, or more precisely, A is only slightly stronger than B (the right half of Figure 1). By contrast, if A is evidently stronger than B, that energy surplus makes the person feel comfortable and pleasurable (the left half of Figure 1), and the person behaves livelily. Wauchope called such cases “living behaviour” (p. 46).
Figure 1.

Pleasant and painful events (Wauchope, 17 p. 46).
This analysis of the intensity of experiences demonstrates the relationship between the self and the outside world in terms of pattern, which is vitally important for studies on psychopathology. Therefore, this scheme of lived experiences can serve as a basic framework for the psychopathology of subjective experiences and their relationship to the outside world. The next section reviews how Yasunaga embraced Wauchope's theory of pattern into psychopathology.
“PATTERN REVERSAL” AS EGO DISTURBANCE
Yasunaga strived to grasp the experiences of patients with schizophrenia, all the more so because he was well aware of the impossibility of reliving their symptoms. Based on Wauchope's concept of pattern, Yasunaga 9 observed the relationship between self and other. It is a truism that each person can never stand on a position other than oneself. The theories by Wauchope and Yasunaga did not lead to solipsism, however. They acknowledged that people have experiences of meeting other people, talking to them, and understanding them. Even so, it is exactly from one's own perspective that each person has experiences and representations of other people. By contrast, no one can start from another person's perspective in understanding oneself. Selfhood is absolutely and even axiomatically prior to otherness in the normally conscious experiences of human beings. This asymmetrical pair of concepts comes precisely under Wauchope's pattern. Yasunaga adopted Wauchope's notation of the subjective side as A and the objective side as B, and represented selfhood as A with the intensity of experience a and otherness as B with intensity b. With this notation, the priority of selfhood (A) over otherness (B) is described as a simple formula: a ≥ b.
Then, Yasunaga 9 carried out a series of thought experiments on what it would be like if the pattern A/B relationship between self and other were to be deteriorated and overturned. In other words, what would a person experience if selfhood became subordinate to otherness? Yasunaga represented such a hypothetical state by the formula a < b and called this state of affairs “Pattern Reversal.” He immediately found that this hypothesis could explain ego disturbance and other symptoms of schizophrenia, as shown hereafter.
Yasunaga 9 explained passivity experience, such as delusion of control, from the standpoint of the pattern A/B. Patients with schizophrenia often complain that their movements or thoughts are manipulated by certain outside forces. These experiences are adequately explained by the theory that the B side overwhelms the A side. Healthy people may sometimes be forced to do something unwanted by external enforcement, but they do not lose the sense that they are doing something on their own. Such normal experiences originate from the dominance of the A side. In addition, Pattern Reversal also clarified the difference between the passivity experience of schizophrenia and the imitation or identification of average people. People often incorporate other people's thoughts or habits, and they sometimes identify with, and imitate many features of another person. Nevertheless, they assimilate the norms incorporated from others into their own standards and feel, think, and act by themselves. Even when accessing the B side of others, healthy people never lose their selfhood or spontaneity of the A side. This differs from the passivity experiences of patients with schizophrenia, as stated above.
The characteristics of delusions and hallucinations are also explicable from the standpoint of Pattern Reversal. Yasunaga 9 focused on how patients with schizophrenia experience delusions and hallucinations, rather than the contents of these symptoms. Many patients with schizophrenia state that their thoughts and actions are inescapably anticipated or preempted by a certain external force. They also complain that their thoughts are transparent to other people and that their every movement is closely watched. The patients can no longer freely think about an open, undetermined future, and feel as if everything is necessarily predetermined. Even when a concrete delusion has not yet occurred to these patients, they often feel something uncanny and unknown to them is happening outside; this symptom is referred to as a delusional atmosphere. These symptoms all indicate that the B side precedes and overwhelms the A side. Similarly, auditory hallucinations in schizophrenia are perceived by the subjects as coming from the outside and having an enforcing quality; they feel compelled to follow what the “voices” say. Therefore, auditory hallucinations are also a case of the B side overwhelming the A side.
Yasunaga also tried to explain thought disorders with schizophrenia. As an example of thought disorders, he 9 cited Taii's 23 case report: “The Sun is only one. I am an only child. So I am the Sun.” What is strange about this statement? Before Yasunaga, von Domarus 24 and Arieti 25 concentrated on the style of syllogism of patients with schizophrenia that “x is P and y is P. Therefore x is y” (Taii's case was an example of this). This differs from the logically correct inference “x is P and P is Q. Therefore x is Q.” Arieti 25 even claimed that the form of this erroneous syllogism plays a central role in the overall psychopathology of schizophrenia, and named this syllogistic form the “von Domarus Principle.” Contrary to von Domarus and Arieti, Yasunaga 9 did not think that the form of sentences or inferences was the determinant of psychopathology. Yasunaga posed the question of what was different between this type of statement by patients and phrases such as “You are my sunshine,” which is repeatedly used in popular songs and declarations of love. Therefore, it is difficult to identify a pathology in this phrase. Yasunaga remarked that a person stating “You are my sunshine” draws parallels between the overall quality of the loved one and that of the sun: to that person's eyes, the loved one is as dazzling as the sun. By contrast, only the numerical sameness devoid of quality combines the patient themself and the sun in the case cited above. From this case, Yasunaga observed Pattern Reversal such that the total, qualitative aspect becomes subordinate to the partial, quantitative aspect.
The argument that syllogistic failure is characteristic of schizophrenia was later refuted because healthy people also frequently fall into logical fallacies. 26 A recent study reported that the reasoning ability of patients with schizophrenia is not evidently different from that of healthy others. 27 By contrast, Yasunaga's argument can withstand this criticism because his account of Pattern Reversal does not rely on formal sentence structure.
FROM PATTERN REVERSAL TO PHANTOM SPACE THEORY
Yasunaga was not satisfied with Pattern Reversal alone. Although it provided a logically legitimate explanation about what it would be like if otherness preceded selfhood, it did not explain why and how it happens to actual human beings. An analogy with physical stresses illuminates this point. In Wauchope's original theory on pattern, 17 a person whose competence for action (A) is equaled by pressure from the outside (B) is compelled to perform the death‐avoiding behavior. If the physical stresses of the B side actually surpassed the A side, it would result in death. By contrast, even when patients with schizophrenia are mentally disorganized and have passivity experiences, they are conscious of their own experiences and still able to talk about and act on them. Therefore, Yasunaga thought that Pattern Reversal alone was insufficient to explain patients' actual pathology, and that further theoretical elaboration was necessary. In addition, Pattern Reversal does not explain all the symptoms of schizophrenia. For example, Pattern Reversal does not explain negative symptoms, such as anhedonia and avolition, because the supremacy of otherness over selfhood does not take place in these symptoms. From these motives, Yasunaga endeavored to extend his theory further. He recollected his aspiration retrospectively:
… since I am a medical doctor, I am tempted to think in terms of the problems of brain physiology. … We cannot help but think, in terms of explanation, that the basis of the Pattern must have originated eventually from a physiological material system in the brain. Then, what kind of a system would it be? 15
In search for such a system, Yasunaga 10 , 15 obtained a clue about a physiological model of abnormal experiences from the mechanism of the illusions of movement. Let us think about a person suffering paralysis of one of the extraocular muscles due to a neurological problem. Under normal conditions, eye movement to the right causes the countermovement of the retinal image of the outside space to the left. The nervous system anticipates that leftward movement of the retinal image and automatically cancels out the change. Therefore, the person does not experience the movement in the visual field. Supposing that a certain abrupt neurological problem made the right eye unable to turn to the right side anymore: Contrary to the person's intention to turn their eyes to the right, the right eye would not actually move. Obviously, the retinal image of the outside space in the right eye would not move. However, the nervous system of the person would still function to cancel out the anticipated leftward movement of the retinal image. Thus, a discrepancy would arise between the unchanging retinal image and its expected movement, and that person would feel as if the outside space was turning to the right. Paralysis in an extraocular muscle alters the way people experience the space around them. Yasunaga added another original thought experiment: What would happen if one of the legs suddenly shrank while walking, unknown to the person? Then that person would illusorily feel as if the ground had made a downward movement. By analogy, Yasunaga speculated that some neurophysiological mechanisms similar to that of the illusions of movement play a role in the formation of schizophrenia symptoms. Of course, Yasunaga was not insisting that hallucinations in schizophrenia were illusions. Nevertheless, he envisioned a spatial metaphor for usual and unusual mental experiences that could be juxtaposed with changes in the spatial experiences in regard to the illusions of movement. From this pursuit, Yasunaga developed his original “Phantom Space Theory.”
PHANTOM SPACE THEORY
The central idea of Yasunaga's Phantom Space Theory 10 is that the intensity of experiences is closely related to psychological distances: weak, unremarkable experiences are perceived as distant from the subject having the experiences, whereas vivid and intense experiences are proximal. Accordingly, the distance can be metrically represented as a kind of reciprocal function of the intensity of experiences. Yasunaga applied this concept of distances to Wauchope's observation of the relationship between the subjective side A and the objective side B. Taking both sides into account, the metrics of experiential distance have at least two variables. Then, the relationship between the A side and the B side, as shown in Figure 2(a), is changeable as far as the condition of the normal experiences a ≥ b is satisfied (the dotted area in Figure 2(a)). Thus, Yasunaga extended Wauchope's linear (one‐dimensional) model and proposed a geometrical representation of psychological experiences. Yasunaga coined the term “Phantom Space” to refer to this experiential space.
Figure 2.

(a) Phantom Space (Yasunaga 10 p. 263), and (b) Phantom Space shrinkage (Modified from Yasunaga 10 p. 213 Figure 5‐4 and p. 271 Figure 7‐5).
Yasunaga 10 , 11 , 12 also reinforced Wauchope's idea that the polarity of pattern is not a dichotomy. Even though selfhood is prior to otherness, each person does not stand alone without otherness. Each person has the reflection of the outside world in oneself. On the other hand, people sometimes observe their own mental states, and some aspects of the self or ego are treated like objects. Therefore, Yasunaga postulated several levels of polarity between selfhood and otherness within each person's experience of self and the world.
First of all, Yasunaga 10 postulated that the human nervous system has two component systems. One system automatically and extra‐consciously processes the input from the world and brings it to consciousness. The extra‐conscious neural functions considered here are different from the concept of the unconscious in psychoanalysis. This system has the role of reflecting the outside world into the person, although it differs from the outside world itself. Yasunaga labeled this system a' to distinguish it from the outside world, to which the character b had formerly been assigned. The other system consciously and explicitly deals with formal and schematic representations. This system was given the same symbol a as selfhood in Pattern Reversal theory because it has the function of the conscious self. Additionally, Yasunaga surmised that there were yet unknown neurophysiological systems that perform the role of each system. The two vertical lines in Figure 2(b) indicate the intensity levels of systems a and a'.
Normally, the human nervous system as a whole functions in unity and there is no split within it. 10 Systems a and a' work adaptively in coordination so that the person can have experiences with various qualities and degrees of intensity. For example, the difference between perception and representation is explained by the relationship between systems a and a'. 10 , 11 , 12 In perception, system a' processes the input from the outside world. Then, system a also operates and locates the percept into the object schema, while system a is not regulating the percept. In this case, systems a and a' are in equilibrium and operating with the same intensity. Therefore, the relationship between systems in the case of perception is described as a = a'. By contrast, when someone brings a representation of something into consciousness, system a is functioning predominantly over system a'. People produce representations voluntarily, and those are not controlled from the outside world. In this case, system a is operating more intensely than is system a', and this is formulated as a > a'. In Figure 2(b), the point P on the slanted line is an example of perception, whereas the point R above that line indicates representation. Similarly, the diagonal ABmax–O in Figure 2(a) corresponds to perception, and the dotted area to representation.
However, sometimes, a certain neurophysiological dysfunction might deprive system a' of the ability to adjust to various inputs with varying degrees of intensity. Yasunaga used the metaphor of diminished “elasticity” and resultant “shrinkage” to represent such a loss of adaptability. 10 , 11 , 12 Then, systems a and a' begin to work in different and uncoordinated ways, just like how the estimation by the nervous system and the actual eye movement diverge in the case of the illusion of movement. In Figure 2(b), the gap between the solid and broken lines figuratively represents the discordance between the systems generated by Phantom Space shrinkage or diminished elasticity against side B intensity (system a' dysfunction). The afflicted person does not sense that the property of system a' has changed; however, the discordance is resultantly brought to consciousness and the person feels that something extraordinary happens within themself and the world.
With the aim of interpreting this theory into actual experiences in schizophrenia, Yasunaga introduced another theoretical distance concept, “the experiential line,” on the basis of the psychological distance in an ordinary meaning, starting from the near end of subjectivity and reaching far‐located external objects. A rough sketch of this line is presented in Figure 3(a). At the subject end of the experiential line is the “ego‐pole,” which is the innermost sense of subjectivity, labeled “e,” and the “ego‐schema,” which is composed of images and thoughts pertaining to the subject, such as self‐image and identity, and labeled “E.” Strictly put, the “ego‐pole” is situated at the nearest end, while the ego‐schema is situated slightly downstream because the “ego‐pole” is the origin point of the subjective sense of activity. At the other end, the theoretically conceived “object pole,” labeled “f,” is placed at the farthest end, and the object schema, which is a set of forms and contents derived from the experiences of objects and labeled “F,” is located around a slightly closer and upstream point from this end. Under normal conditions, “e” operates together with “E,” and “F” with “f,” and each pair is usually perceived together in lived experiences. The experiential line can basically be projected to a horizontal line, representing a kind of psychological distance, as shown in Figure 2(b), where E and F indicate the directions of the subject and object ends, respectively.
Figure 3.
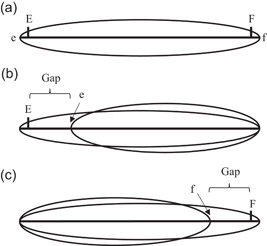
(a) The experiential line (Yasunaga 16 p. 138). (b) E‐e disarrayed condition (Modified from Yasunaga 12 p. 202 Figure 5‐5). (c) f‐F disarrayed condition (Modified from Yasunaga 12 p. 193 Figure 5‐2).
Yasunaga construed that the imbalance between systems a and a' disrupts the alignment of eEFf in the experiential line. 11 That disarray causes experiences in which the subject is overwhelmed by unknown, external forces. From this standpoint, Pattern Reversal as indicated in the formula a < b does not actually occur, not even in schizophrenia, and can be recaptured as a particular type of experiential disruption.
The next section explores how each symptom of schizophrenia can be explained by disorder in the Phantom Space.
PSYCHOTIC SYMPTOMS FROM THE STANDPOINT OF PHANTOM SPACE THEORY
Passivity experiences
Passivity experiences are at the core of ego disturbance in schizophrenia. Phantom Space Theory explains passivity experience by the disarray between the ego‐pole (e) and the ego‐schema (E). 11 , 12 , 15 Normally, the ego‐pole (e) is prior to the ego‐schema (E) in the experiential line (Figure 3(a)). Ego‐schema (E) functions properly only under endorsement by the ego‐pole (e). If the ego‐schema (E) were to take priority over the ego‐pole (e), a paradoxical state of affairs would ensue. Yasunaga explained this situation as follows:
Here it is as if the e stumbles forward and leaves the ego‐schema behind. Even though e is actually working through E, the position of E is located behind e, which is a very paradoxical situation. E is originally the person's self but, by being located behind e, it does not feel like his self any longer. The lived experience is that something like the other's ego is operating on [the patients with schizophrenia] and no resistance is possible against it. 15 (italics added)
That dislocation between E and e is illustrated in Figure 3(b). The ego‐schema (E) would be alienated from the sense of oneself (e) in this condition: therefore, the patients would no longer sense that they are the agent of themselves, and would feel that they are controlled by invisible, external forces.
This model fits excellently to passivity experiences, but how is such a state possible? Phantom Space Theory posits that the Phantom Space shrinkage or the diminished elasticity of system a' and the resultant discordance between systems a and a' could bring about the divide between the ego‐schema (E) and the subjective pole (e). 10 , 11 While the discordance between systems a and a' is represented in Figure 2(b) as the gap between the solid and broken slanted lines, the gap could theoretically be set on the opposite side of the triangle, which corresponds to the subjective side. 11 Ego‐schema is mainly held consciously by system a, whereas the ego‐pole (e) needs more strong sustenance by system a' that is primarily compromised by Phantom Space shrinkage or diminished elasticity of system a'. Therefore, the gap generated on the subjective side causes a positional inversion between e and E. Rephrased into terms of the experiential line, the ego‐pole (e) could be located farther than ego‐schema (E), as indicated in Figure 3(b). In that situation, the person afflicted loses their basic sense of self, is deprived of the feeling that they have their own intentions, will, or spontaneity, and further feels dominated or controlled by external forces.
Delusions and hallucinations
Delusions and hallucinations are also typical symptoms of schizophrenia. Particularly, auditory hallucinations are frequent among patients with schizophrenia. With regard to delusions, patients with schizophrenia typically attribute idiosyncratic meanings to percepts of mundane things and events: this type of primary delusion is called delusional perception. 1 , 28 The contents of delusions and hallucinations are ultimately what the patients think and feel, because these contents do not belong to the outside world. The problem is why these contents are experienced in forms different from ordinary thoughts.
Yasunaga 11 , 14 , 15 maintained that the “quasi‐perceptualization of imagination” plays a central role in the formation of delusions and hallucinations. As described in the previous sections, normal imagination and representations are characterized by the state that system a operates more intensely than does system a' (R in Figure 2(b)), whereas in normal perception, both systems work with equal intensity (P). Similar to the case of passivity experiences, Phantom Space shrinkage generates a gap between the solid and broken lines in Figure 2(b). In this case, however, the gap appears on the object end. Then, the surplus of system a over system a' in the formula a > a' is diminished to narrow the gap. As a result, the representation (R) loses the energy and freedom expressed as a surplus of a over a'. In this situation, the representation would be experienced like perception (P) with the formula a = a'.
Patients experience delusions with absolute certainty, although they usually cannot tell why the contents of the delusions seem certain to them. Especially in delusional perception, an idiosyncratic meaning is experienced as being attached to perception. These basic features of delusional experiences are pertinently explained by the quasi‐perceptualization of imagination. Quasi‐perceptualization takes the feeling of spontaneity away from the contents of thoughts. In addition, such a quasi‐perceptualized object schema might be coupled with a proper perceptual experience to form a delusional percept. In the experience of delusional perception, it is considered that imagination or thoughts of little relevance associated with the percept undergo change into delusional thoughts through quasi‐perceptualization. Thus, the contents are experienced as compelling and coming from the outside. Then, the patients endorse the contents as indubitable.
With regard to auditory hallucinations in schizophrenia, Yasunaga assumed that the quasi‐perceptualization of imagination and the mechanism of passivity experiences could both be at work. 10 , 11 , 15 The mechanism of passivity experiences takes the feeling of agency away from the ego‐schema (E). Passivity experiences deprive feelings of spontaneity from the patient's own imagining and thinking functions. Quasi‐perceptualization impacts the thought contents: imagination and thoughts lose selfhood and are experienced as coming from the outside, as already explained regarding the case of delusion. Therefore, both verbal representations and the agent generating those representations lose selfhood and are perceived as being alienated. 10
Depersonalization and dissociation‐like symptoms
Patients with schizophrenia sometimes show depersonalization symptoms early in the course of illness, even though depersonalization is considered separately from passivity experiences and other hallucinatory symptoms, and is usually seen as a dissociative symptom in the current symptomatology. 28 Yasunaga 13 , 15 observed that depersonalization often precedes or coexists with psychotic symptoms, although he acknowledged that it also emerges in other mental disorders. Yasunaga provided an explanation of depersonalization by Phantom Space Theory (the symptom discussed here is derealization, or allopsychic depersonalization). He contended that this is explained by the split between the object schema (F) and the object pole (f) (Figure 3(c)). If the object schema (F) were psychologically more distant than “f,” the person would perceive the object schema (F) as weaker and more detached than anticipated; that experience would correspond to depersonalization. Yasunaga attributed the cause of the split between “f” and “F” to the gap produced by system a' dysfunction and the resultant Phantom Space shrinkage indicated in Figure 2(b).
Dissociative symptoms in psychosis are attracting fresh attention. 29 Yasunaga 11 , 12 , 13 , 15 also analyzed dissociation‐like symptoms in schizophrenia. He proposed the term “quasi‐possession” to denote possession‐like phenomena in which patients behave as if they have been taken over by a particular other person. Yasunaga argued that the symptom is, similar to passivity experience, derived from a gap in the Phantom Space located around the subject end in the experiential line. A schema that is activated for understanding that person has overwhelming veracity through Phantom Space shrinkage, as seen in the case of quasi‐perceptualization, and resultantly behaves as if it were a part of the patient's own ego‐schema (E), on which the ego‐pole (e) of the patient got stuck or fitted. An important characteristic of this phenomenon is that it is accompanied by some passivity experience. Thus, Yasunaga stressed that “quasi‐possession” in schizophrenia is different from the genuine dissociative symptoms of nonpsychotic patients (this point was pursued further by Shibayama 30 ).
Negative symptoms
The negative symptoms of schizophrenia, such as “diminished emotional expression” and “diminished speech output” 2 , 3 were not adequately explained by Pattern Reversal. Yasunaga 10 , 11 applied Phantom Space Theory to account for symptoms in the chronic phase of schizophrenia, including negative symptoms. Yasunaga thought that declines in the energy and adaptability of system a' (in Yasunaga's words, Phantom Space shrinkage or diminished elasticity) also played a significant role in the formation of negative symptoms. The change in system a' causes discrepancy between systems a and a' to varying degrees. However, if the structure of experiences eEFf mentioned above is preserved, positive symptoms, such as hallucinations or passivity experiences, do not occur. For example, when only a minimally discrepant and relatively intact portion of the systems was used to cope with the newly emerged inner environment, the patient would not have passivity experiences or quasi‐perceptualization. This unimpaired portion is of course narrower than the original system as a whole, which means that the experiences of the patient are also limited within a narrower range of emotion, thinking, and resultant actions. Therefore, Phantom Space shrinkage also explains negative symptoms, such as anhedonia, avolition, and diminished speech output.
IMPLICATIONS OF PHANTOM SPACE THEORY
The rigor of Yasunaga's theoretical inquiry does not mean that he was an unpractical theorist detached from reality. Yasunaga spent most of his career at the Department of Neuropsychiatry of the University of Tokyo Branch Hospital (1962–1989), and served as the Head of the Department for almost two decades (1971–1989). 31 Under his leadership, the Department carried out significant clinical and psychopathological works, distancing itself from the political divide among groups of psychiatrists at that time. Even after retiring from his academic career, he continued working at a psychiatric institute for another two decades. His long and profound clinical experiences were the sources of Phantom Space Theory and other psychopathological studies. Though he also learned phenomenology, psychoanalysis, and structuralism, 11 , 12 , 13 , 16 his view did not hinge on these major schools of thought. Yasunaga was quite an independent and innovative thinker, just like Wauchope.
Non‐stigmatizing theory on psychotic symptoms
Phantom Space Theory explains most symptoms of schizophrenia from the assumption of a breakdown in a neural system leading to disequilibrium between two yet unspecified neurophysiological systems within the patient. Yasunaga did not add any further assumptions about the patient's personality or deep existential problems. He was aware of the risk that apparently humanistic and anthropological accounts of disease could often personalize the problems. Phantom Space Theory promotes the view that “schizophrenia is neither a personality defect nor a mysterious disease.” 15
When explaining psychotic symptoms to patients and their families, Yasunaga 12 , 14 , 16 often used analogies with orthopedic disturbances, such as sprain, dislocation, and fracture. These analogies fit precisely with Phantom Space Theory because it presumes a partial breakdown and resultant functional alteration within the nervous system of the patient. In addition, orthopedic problems are easier for lay people to imagine and visualize compared with invisible psychiatric disorders. Therefore, sprain and fracture analogies are more suitable for instructing patients on how to maintain a healthy daily life overall without activating the damaged part too early, and on how to wait for recovery without hurrying. This is a way of conveying insights from Phantom Space Theory to the patients and their families without insulting them.
Clinical sense of psychological distance
Yasunaga 16 revealed his subtle sense of psychological distance between patients and the psychiatrist in his writings other than those on Phantom Space Theory. He remarked that frank and open communication between patients and clinicians is important, but he also noted that this frank and open attitude is different from simply having a relationship such as that of close friends. An overly close psychological distance tends to make clinicians neglect patients' problems, so it is not beneficial to patients either. Tangibly, Yasunaga addressed subtle differences between acceptance and permission, between empathy and pity, and so on. In these arguments, Yasunaga did not schematize interpersonal distances because he did not think that a doctrinaire approach could solve interpersonal issues. Nevertheless, his keen sense of psychological distance was noticeable in his remarks cited above.
IS PHANTOM SPACE THEORY A KIND OF DUAL‐PROCESS THEORY?
How is Phantom Space Theory linked with current inquiries into psychotic symptoms? Recently, the points at issue are the levels of self‐disorder and the neural correlates of psychotic symptoms. Because the current concept of self‐disorder encompasses a broad scope, various levels of selfhood have drawn the attention of researchers. 6 , 32 , 33 While self‐disorder at the basic, pre‐reflective level is attracting major research interest, 7 other researchers are concentrating on the meta‐cognition of patients with psychotic symptoms. 34 Corresponding to the conceptual heterogeneity, various neural mechanisms have been hypothesized as the causes of each psychotic symptom. 7 , 35 Concerning these research issues, Phantom Space Theory assumes that most psychotic symptoms are caused by an unknown physiological change in extra‐consciously functioning system a' and the resultant discrepancy between system a' and the rather conscious system a. 10 , 11 , 12 Yasunaga did not delve into specifying neurobiological abnormalities, which represents concurrently the weakness and potentiality of Phantom Space Theory. Indeterminate neural correlates are not a fatal flaw because the neurobiological causes of self‐disorder have yet to be determined. Rather, Phantom Space Theory can be combined with any other novel neurobiological theory to explain the psychopathological states of schizophrenia.
Particularly, the parallel between Phantom Space Theory and dual‐process theory is worth examining because dual‐process theory also posits that the human nervous system consists of automatic system(s) (often called system 1, or in more recent years, type 1 36 ) and reflective system(s) (system 2 or type 2). According to dual‐process theory, system 1 first gives a fast and rough estimate of the perceived situation. Thereafter, system 2 makes a slow but more precise, multifactorial analysis and adjusts the first estimate. Coordination between two systems is considered vital to an efficient and appropriate judgment. Diverse views on the detailed functions and exact neural correlates of each system have been expressed. 36 , 37 While some researchers criticize dual‐process theory for embracing overly broad, umbrella concepts, 38 the proponents of the theory continue conducting further examinations of specific neurocognitive functions. 36 , 39 Therefore, studies on psychotic symptoms from the viewpoint of dual‐process theory are also in progress. 35 , 40
Phantom Space Theory and dual‐process theory share the common postulate that coordination between the extra‐conscious and conscious systems plays a vital role in the normal functioning of the nervous system. Each theory has a specific time scale and a particular focus of attention. Dual‐process theory focuses on how the two systems bring about each judgment in a moment in combination. In contrast, Phantom Space Theory does not seem to cover transient dissonance within the nervous system or its resolution in normal judgment. Instead, Phantom Space Theory deals with the persistent discordance or irreconcilability in the neural systems of patients that lead to perplexity and inexactness. Rephrased into dual‐process terms, it is similar to the state that systems 1 and 2 do not converge, and each system continues to make different estimates. This suggests that Phantom Space Theory does not attribute the cause of psychotic symptoms to the dysfunction of conscious reasoning. Therefore, integrating the insights from Phantom Space Theory and current neurocognitive theories might provide a clue for studying how neural systems operate in developing psychotic symptoms.
CONCLUSIONS
The present article has reviewed Yasunaga's studies on the psychopathology of schizophrenia. His endeavor in this area of investigation owed a great deal to British philosopher Wauchope. Yasunaga applied Wauchope's concept of pattern to the analysis of the relationship between selfhood and otherness. According to Wauchope's theory on pattern, it is self‐evident that selfhood surpasses otherness. Ego disturbance and other symptoms of schizophrenia were explained as a state in which otherness overwhelms selfhood. This was the first version of Yasunaga's theory on schizophrenia, namely, Pattern Reversal. He further pursued how and why selfhood gives way in actual patients. From this pursuit, he extended Wauchope's theory and developed his original Phantom Space Theory. Yasunaga postulated the existence of conscious and extra‐conscious systems and contended that the imbalance between the two, represented by Phantom Space shrinkage, would have some as yet unspecified neurophysiological basis. Yasunaga demonstrated how this single hypothesis explains most of the symptoms of schizophrenia, from the core symptoms, such as passivity experiences and hallucinations, to rather unspecific ones, such as depersonalization, dissociation‐like symptoms, and negative symptoms. Because the aim of the present article was to revisit the basic principles of Yasunaga's theory, it has not delved into the extended area of investigations based on Phantom Space Theory, such as those on disturbed consciousness or the relationship between language and psychopathology. The last part of this article explored the clinical and theoretical implications of Yasunaga's psychiatric works. Because Phantom Space Theory does not hypothesize personal or existential problems, it leads to a non‐stigmatizing view on psychotic symptoms and patients with schizophrenia. As a suggestion for further studies on schizophrenia, the similarities and differences between Phantom Space Theory and current dual‐process theory were also examined.
The authors of the present article have attempted to explain Yasunaga's theory as plainly as possible. Nevertheless, his theory further addressed stubborn questions on the psychopathology of schizophrenia, sometimes requiring toilsome effort on the part of readers. As Utsumi, one of the disciples of Yasunaga, stated, “Hiroshi YASUNAGA needs to be [re]discovered by us” 31 (p. 175).
FUNDING INFORMATION
This research received no specific grant from any funding agency in the public, commercial, or not‐for‐profit sectors.
AUTHOR CONTRIBUTIONS
T.K. wrote the first manuscript and revised it. N.H. collected the primary sources and revised the manuscript.
CONFLICT OF INTEREST STATEMENT
The authors declare no conflict of interest.
ETHICS APPROVAL STATEMENT
The ethics approval statement is not applicable.
PATIENT CONSENT STATEMENT
The patient consent statement is not applicable.
CLINICAL TRIAL REGISTRATION
The clinical trial registration is not applicable.
ACKNOWLEDGMENTS
We express our gratitude to Takeshi UTSUMI for promoting our synergy.
Kumazaki T, Hayashi N. Self‐disorder explained: Yasunaga's “Phantom Space Theory” on schizophrenia. Psychiatry Clin Neurosci Rep. 2023;2:e90. 10.1002/pcn5.90
DATA AVAILABILITY STATEMENT
Not applicable as this is a review article.
REFERENCES
- 1. Schneider K. Primary and secondary symptoms in schizophrenia [Marshall H Trans.]. In: Hirsch SR, Shepherd M, editors. Themes and variations in European psychiatry: an anthology. Charlottesville, VA: University Press of Virginia; 1957. p. 40–4. [Google Scholar]
- 2. American Psychiatric Association . Diagnostic and statistical manual of mental disorders. 5th ed, text rev. Washington, DC: American Psychiatric Association; 2022. [Google Scholar]
- 3. World Health Organization . ICD‐11 for mortality and morbidity statistics, 2019. Available from: https://icd.who.int/browse11/l-m/en#/http%3a%2f%2fid.who.int%2ficd%2fentity%2f1683919430
- 4. Soares‐Weiser K, Maayan N, Bergman H, Davenport C, Kirkham AJ, Grabowski S, et al. First rank symptoms for schizophrenia. Cochrane Database Syst Rev. 2015;1:CD010653. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5. Jauhar S, Johnstone M, McKenna PJ. Schizophrenia. Lancet. 2022;399:473–86. [DOI] [PubMed] [Google Scholar]
- 6. Fuchs T. From self‐disorders to ego disorders. Psychopathology. 2015;48(5):324–31. [DOI] [PubMed] [Google Scholar]
- 7. Sass L, Borda JP, Madeira L, Pienkos E, Nelson B. Varieties of self disorder: a bio‐pheno‐social model of schizophrenia. Schizophr Bull. 2018;44(4):720–7. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8. Sass L. Subjectivity, psychosis and the science of psychiatry. World Psychiatry. 2022;21(2):165–6. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9. Yasunaga H. The essential character of schizophrenic experiences. Psychiatria et neurologia Japonica. 1960;62(3):437–66. (in Japanese) [Google Scholar]
- 10. Yasunaga H. [Phantom Space Theory]. Collected papers, 1. Tokyo: Kongo Shuppan;1977/1992. (in Japanese). [Google Scholar]
- 11. Yasunaga H. [Geometry of the mind]. Tokyo: Iwanami Shoten; 1987. (in Japanese). [Google Scholar]
- 12. Yasunaga H. [Development of Phantom Space Theory]. Collected papers, 2: Tokyo: Kongo Shuppan; 1992. (in Japanese). [Google Scholar]
- 13. Yasunaga H. [Methodology and clinical concepts]. Collected papers, 3, Tokyo: Kongo Shuppan; 1992. (in Japanese). [Google Scholar]
- 14. Yasunaga H. [Symptomatology and psychotherapy]. Collected papers, 4, Tokyo: Kongo Shuppan; 1992. (in Japanese). [Google Scholar]
- 15. Yasunaga H. O.S. Wauchope's possible contribution to the next generation: pattern, Pattern Reversal and Phantom Space Theory. 20th International Human Science Research Conference, 2001 Aug 21; Tokyo, Japan; [Yoshida A, Halling S Trans.] 2001.
- 16. Yasunaga H. [Psychiatrist's way of thinking: from clinical experiences]. Tokyo: Kongo Shuppan; 2002. (in Japanese). [Google Scholar]
- 17. Wauchope OS. Deviation into sense: the nature of explanation. London: Faber & Faber; 1948. [Google Scholar]
- 18. Choudhary AR, Choudhary R. An analysis of modalities of academic globalization and acceptance criteria for future models. Iss Inform Syst. 2011;12(1):473–82. [Google Scholar]
- 19. Kobayashi T. The significance of mixed states in mania and depression: from the psychopathological viewpoint of Tadao Miyamoto. Psychiatr Clin Neurosci Rep. 2022;1:e53. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20. Moore GE. A defense of common sense. In: Baldwin T, editor. G. E. Moore: Selected writings. London: Routledge; 1925/1993. p. 106–33. [Google Scholar]
- 21. Dingle H. Deviation into sense: the nature of explanation. By O.S. Wauchope. Philosophy. 1950;25(93):188–9. [Google Scholar]
- 22. Oakeshott M. Review of O.S. Wauchope, deviation into sense. Times Literary Supplement 1949, Jan 15.
- 23. Taii S. [Psychotic language]. In: Endo Y, editor. [Psychology of language]. Tokyo:Nakayama Shoten;1958. p. 225–52 (in Japanese). [Google Scholar]
- 24. von Domarus E. The specific laws of logic in schizophrenia. In: Kasanin JS, editor. Language and thought in schizophrenia: collected papers. Berkeley, CA: University of California Press; 1944. p. 104–14. [Google Scholar]
- 25. Arieti S. Interpretation of schizophrenia. London: Crosby Lockwood Staples; 1955. [Google Scholar]
- 26. Williams EB. Deductive reasoning in schizophrenia. J Abnorm Social Psychol. 1964;69:47–61. [DOI] [PubMed] [Google Scholar]
- 27. Revsbech R, Mortensen EL, Owen G, Nordgaard J, Jansson L, Sæbye D, et al. Exploring rationality in schizophrenia. BJPsych Open. 2015;1:98–103. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28. Oyebode F. Sims' symptoms in the mind: textbook of descriptive psychopathology. 6th ed. Edinburgh: Elsevier; 2018. [Google Scholar]
- 29. Longden E, Branitsky A, Moskowitz A, Berry K, Bucci S, Varese F. The relationship between dissociation and symptoms of psychosis: a meta‐analysis. Schizophr Bull. 2020;46(5):1104–13. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 30. Shibayama M. Differential diagnosis between dissociative disorders and schizophrenia. Seishin shinkeigaku zasshi = Psychiatria et neurologia Japonica. 2011;113(9):906–11 (in Japanese). [PubMed] [Google Scholar]
- 31. Utsumi T. In memory of YASUNAGA Hiroshi sensei. Jpn J Psychopathol. 2011;32(2):173–80 (in Japanese). [Google Scholar]
- 32. Hamm JA, Buck B, Lysaker PH. Self‐experience in schizophrenia: metacognition as a construct to advance understanding. Philos Psychiatr Psychol. 2015;22(3):217–20. [Google Scholar]
- 33. Stanghellini G. Some suggestions to integrate the self‐disorder hypothesis of schizophrenia. Philos Psychiatr Psychol. 2015;22(3):213–5. [Google Scholar]
- 34. Mishara AL, Lysaker PH, Schwartz MA. Self‐disturbances in schizophrenia: history, phenomenology, and relevant findings from research on metacognition. Schizophr Bull. 2014;40(1):5–12. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 35. Speechley WJ, Woodward TS, Ngan ET. Failure of conflict to modulate central executive network activity associated with delusions in schizophrenia. Front Psychiatry. 2013;4:113. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 36. Evans JStBT, Stanovich KE. Dual‐process theories of higher cognition: advancing the debate. Perspect Psychol Sci. 2013;8(3):223–41. [DOI] [PubMed] [Google Scholar]
- 37. Apperly IA, Butterfill SA. Do humans have two systems to track beliefs and belief‐like states? Psychol Rev. 2009;116(4):953–70. [DOI] [PubMed] [Google Scholar]
- 38. Melnikoff DE, Bargh JA. The mythical number two. Trends Cogn Sci. 2018;22(4):280–93. [DOI] [PubMed] [Google Scholar]
- 39. Pennycook G, Neys WD, Evans JStBT, Stanovich KE, Thompson VA. The mythical dual‐process typology. Trends Cogn Sci. 2018;22(8):667–8. [DOI] [PubMed] [Google Scholar]
- 40. Bronstein MV, Pennycook G, Joormann J, Corlett PR, Cannon TD. Dual‐process theory, conflict processing, and delusional belief. Clin Psychol Rev. 2019;72:101748. [DOI] [PMC free article] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Data Availability Statement
Not applicable as this is a review article.