

Abstract
White spot lesions (WSLs) refer to localized areas of hypo-mineralization limited to the enamel of the teeth surface, which is noticeable clinically to the naked eye on drying of the teeth. During fixed orthodontic treatment, it is very hard for the patient to maintain excellent oral hygiene as the brackets, bands, wires, elastics, and other appliances and attachments worn intra-orally provide a platform for food retention, plaque formation, and then colonization by acidogenic bacteria like Streptococcus mutans and Lactobacillus. This review aims to elaborate and focus on etiology, pathophysiology, diagnosis, treatment aspect, and future scope for research about the WSLs occurring due to fixed orthodontic treatment.
Keywords: Demineralization, dental plaque, orthodontic appliance, white spot
Introduction
The significant surge for esthetics has enormously increased in recent times. As a result, orthodontic treatment has gained widespread popularity not only among younger individuals but also among adults. However, orthodontic treatment goes beyond merely adjusting the misalignment of teeth; it focuses on enhancing both functional aspects and the overall appearance of a smile, thereby improving facial esthetics. While traditional methods involving wires and brackets were initially employed for tooth alignment, aligners have gained prominence due to patient preferences and demands. Regardless of the method used to reposition teeth, additional attachments on the teeth can lead to increased food retention and plaque formation. This, in turn, creates an environment for acidogenic bacteria, ultimately resulting in the development of unesthetic white spot lesions (WSLs) on the teeth.[1,2]
The initiation of early enamel carious lesions involves the demineralization of enamel rods and the expansion of enamel sheaths. Enamel hypoplasia is an anomaly that may impact a portion of the tooth’s surface, leading to the formation of pits or grooves, resulting in a thin enamel layer or the absence of the enamel. Early-stage caries become apparent under dry conditions but virtually vanish when the enamel is wet. In contrast, hypo-calcification remains visible whether the enamel is wet or dry.
A WSL refers to localized areas of hypo-mineralization limited to the enamel surface of the teeth, clinically visible to the naked eye when the teeth are dry.[1,2] While it may take several weeks to months for WSLs to manifest in patients undergoing fixed orthodontic treatment, research indicates that they can appear as early as 1 week in individuals with inferior oral hygiene and unhealthy dietary habits, particularly those involving high consumption of refined sugars, especially in sticky food forms. Studies have demonstrated that in normal individuals without associated systemic illnesses and with proper oral hygiene practices and dietary restrictions, WSLs typically develop around 3–6 months after the commencement of orthodontic treatment, with origins that can be either carious or non-carious.[3] The objective of this paper is to highlight and focus on the etiology, pathophysiology, diagnosis, treatment aspect, and future scope for research about the WSLs occurring due to fixed orthodontic treatment.
Factors Associated with WSL
During fixed orthodontic treatment, it is very hard for the patient to maintain excellent oral hygiene as the brackets, bands, wires, elastics, and other appliances and attachments worn intra-orally provide a platform for food retention, plaque formation, and then colonization by acidogenic bacteria like Streptococcus mutans and Lactobacillus.[3,4,5,6] Moreover, the process of etching of the enamel done using phosphoric acid before bonding the brackets to the tooth surface using composite resins causes some amount of superficial demineralization.[4]
Other causes of demineralization in patients undergoing orthodontic treatment might include an increased etching time;[4] decreased salivary flow; genetic susceptibility; poor oral hygiene maintenance; systemic factors like diabetes mellitus, hypothyroidism, or any other pre-existing illness; high sticky food consumption which is rich in fermentable carbohydrates; any medication intake which causes xerostomia;[1] vitamin D3 deficiency; and so on [Figure 1].[2]
Figure 1.

Factors leading to the formation of WSLs during fixed orthodontic treatment
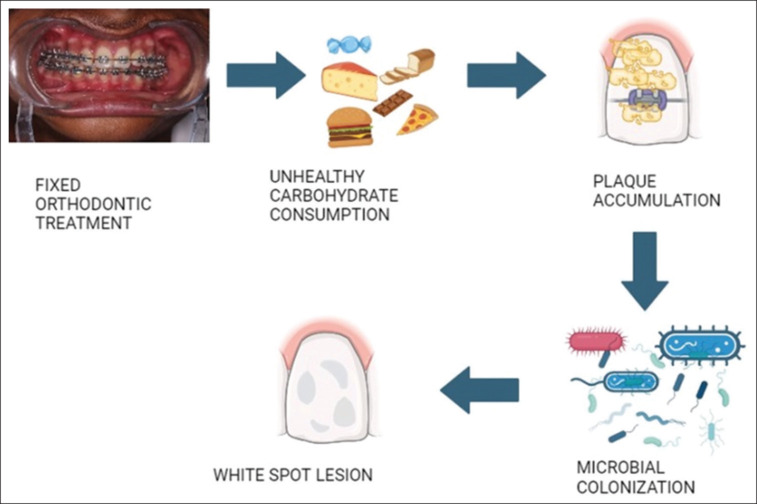
Cycle of Events Leading to WSL
The accumulation of plaque with altered oral microflora composition mainly consisting of acidogenic bacteria will lead to the fermentation of carbohydrates intra-orally and the elaboration of acidic substances.[5,6] This causes the salivary pH to fall below the critical pH. The imbalance resulting because of increased demineralization and decreased remineralization leads to surface dissolution and demineralization of the superficial enamel which causes the micro-porosities, a rough surface, and white opaque appearance of the enamel, which is called the WSL [Figure 2].[3,6,7] During this process, the fluoride content from the surface hydroxyapatite crystals, which makes the enamel resistant to acid dissolution, is lost. If this process proceeds continuously, cavitations of carious lesions result.[8]
Figure 2.
Development of WSLs during fixed orthodontic treatment
After the initial demineralization process, once the pH of saliva returns to neutral pH from acidic pH, the fluoride from the saliva causes remineralization of the superficial hydroxyapatite crystals.[8] For this to happen, at least 3 ppm of fluoride content should be present in the saliva. But if the critical pH is maintained for a prolonged period or the etching time is extended beyond 15 seconds, then the remineralization process will be affected.[4,8]
Two stages of enamel demineralization have been documented. The first stage is limited to superficial loss of inter-prismatic substance in the enamel. The second stage includes sub-surface dissolution with the body of the lesion covered by a richly mineralized layer that is porous. If the demineralization is limited to the first stage, the carious lesion might become an arrested lesion that does not remineralize. The second stage, which is called an active lesion, is more prone to remineralization because of its porous nature, which allows the remineralizing agent to pass to the deeper part of the enamel.[2,9]
Normally, the enamel is translucent with a smooth surface and hard consistency. Initial carious lesions of the enamel are classified as invisible carious lesions (<100 µm deep) or WSLs (<400 µm deep). WSLs consist of a hard enamel surface covering a demineralized cavity that appears white when compared to the surrounding sound enamel. WSLs are resistant to mechanical abrasion or any oral hygiene procedures.[10]
On histologic and microscopic evaluation, the following zones were observed about WSLs:
Intact surface layer (ISL),
Body of the demineralized lesion (white opacity),
Dark zone (base of the demineralized area), and
Translucent zone (advancing front of the lesion).[10]
Usually, WSLs start appearing as early as 4 weeks after the initiation of the fixed orthodontic treatment.[11] Almost 97% of people who underwent fixed orthodontic treatment had developed generalized WSLs post treatment.[5] 23% of patients developed WSLs while undergoing fixed orthodontic treatment. 2.5 times more than mandibular teeth, maxillary teeth seem to be affected.[1] More easily affected teeth were maxillary laterals, maxillary canines, and mandibular canines. Males are shown to be slightly more affected than females.[12]
Various Diagnostic Aids to Detect WSL
Visual diagnosis is done clinically by drying the enamel, which reveals a white, chalky, opaque, and porous enamel surface lesion.[1,13] The International Caries Detection and Assessment System (ICDAS) for measurement of early carious lesions like WSLs, which is also a form of visual examination, is useful mainly in the evaluation of the effectiveness of a newly developed remineralizing agent in the research field and also in epidemiology. The codes start with Code 0: sound tooth surfaces, no evidence of caries after prolonged air drying to extensive distinct cavity with visible dentin: Code 6.[13,14,15]
QLF (quantitative laser fluorescence) depends on the teeth’s auto-fluorescence when the teeth are open to the elements of blue light from an argon-ion laser of 488 nm wavelength.[1] With an intra-oral fluorescence camera and particular software, which includes a video repositioning method, QLF images were recorded. QLF images were analyzed visually for demineralized zones, seen as dark areas enclosed by a bright green fluorescing normal tooth structure. To scrutinize the lesion, a yellow interrupted filter which removes all reflected and backscattered light was placed in front of the eye. It is beneficial clinically for the assessment of surface demineralization of teeth.[16,17,18]
QLF-D, which was digitized, uses the increased intensity of red fluorescence. Demineralized areas are seen as unilluminated surfaces with no fluorescence, which is due to the loss of inorganic substances.[18,19] The potential advantage exists for QLF-D to serve as a valuable method for detecting proximal caries; while dentists must possess the necessary skills to capture accurate images, the photographic process is predominantly automated.[18]
Photographic evaluation using a DSLR camera and 100 mm macro lens also has been used to record the incidence and prevalence of WSLs.[16,20] It excels in image quality and manual settings and offers a vast lens selection, a longer battery life, superior auto-focus, durability, and weather coating. The drawbacks are larger and heavier, potentially more complex for beginners, have slower continuous shooting, are pricier due to premium components, and require additional accessories.[20]
Many dyes like Procion dyes, Calcein dye, fluorescent dye, and Brilliant Blue dye were also used for early caries detection including that of WSL.[21,22,23] The main disadvantage is the lack of specificity, which may stain both infected and healthy dentin at the enamel dentine junction (EDJ), causing false positives.[22]
Optical coherence tomography (OCT) is a non-invasive investigative technique that provides a cross-sectional picture of dental carious lesions at an early stage. The former OCT imaging systems operated on the time-domain principle (TD-OCT), and in the recent swept-source OCT (SS-OCT) system, a fixed mirror is used and the images are recorded faster, which increased its use in clinical and research fields.[14,24] The main constraints of OCT include limited tissue penetration (1–2 mm) due to prolonged light scattering, which hinders its effectiveness in-depth imaging.
DIAGNODent is a mobile system that is mainly dependent on the fluorescence emitted from demineralized surfaces when they are exposed to the laser beam of a wavelength of 655 nm. The reason for increased fluorescence was found to be due to the presence of porphyrins produced by the bacteria present in the carious lesion.[25,26] It is safe, painless, and measurable; this diagnostic method avoids X-rays, ensures comfort, and provides precise measurements for dentists monitoring cavity development. Sometimes, it may give inaccurate readings near sealant margins or near orthodontic bracket sealing.[25]
X-ray micro-tomography (XRMT) is very useful for quantifying the mineral density of WSLs. XRMT along with commercially existing software (VGStudio Max) has allowed for WSLs to be examined in three dimensions.[24] It can non-destructively visualize internal sample features, offering rapid technology with impressive resolution capabilities. The drawbacks encompass substantial initial setup costs, scanning times, infrastructure needs, complex data pipelines, and reconstruction delays.[27]
Scanning electron microscopy (SEM) is used mostly in in vitro and also in vivo in detection of the carious lesions using evaluating surface defects and assessing the permeability of dental hard tissue in conjunction with other methods. It has exceptional ease of use, featuring digital image resolution and a large depth of field for precise characterization. The limitation of SEM is size and cost, a limiting sample size, microorganism observation, and prohibiting wet sample imaging.[28]
A spectrophotometer is used to measure the color change between sound teeth and carious structures using The CIELAB (Commission Internationale de l’Eclairage) color system.[29] It is non-destructive and accurate, providing quickly and inexpensively valuable insights. The main drawback is limited sensitivity and selectivity, lack of portability, and high cost.[29]
Confocal laser scanning microscopy (CLSM)[30] and micro-radiography[31] are the other diagnostic modalities used to assess the mineral density in WSLs. It is expensive and very difficult to use near the chair side in the clinical area.
Treatment Strategy for WSL
Before starting fixed orthodontic treatment
Evaluation of any pre-existing carious or non-carious WSLs.
Taking the proper medical history of any pre-existing systemic illness or medication history that might contribute to WSLs and modifying it if possible.
Education regarding maintenance of proper oral hygiene by explaining the consequence of not doing so.
Altering the patient’s diet to reduce the intake of sticky fermentable carbohydrates.
Patients should only undergo orthodontic treatment if they exhibit sufficient levels of oral hygiene instruction (OHI) adherence and behavioral commitment to biofilm control techniques.
During the treatment phase
Demonstration of proper brushing techniques, encouraging the use of power toothbrushes and increasing the frequency of brushing to at least twice a day.
Continuous monitoring of oral hygiene status and motivating the patient to use adjunctive oral hygiene aids like flossing, inter-dental brushes or water floss, mouthwash, and remineralizing toothpaste as and when required.
Performing oral prophylaxis regularly.
Use of sealants or varnishes containing remineralizing agents whenever required.
Monitoring of the systemic contributing factors, if any, from time to time.
Treatment completion phase
Encouraging the patient to follow a strict oral hygiene routine.
Also educating him on self-assessment of the development of WSLs and reporting to the dental office if any lesions are developed for appropriate management.
There are a lot of remineralizing agents available that aid in the management of WSLs. The agents are available in various forms for ease of application by the patient itself. After assessing the patient, the appropriate agent is chosen and prescribed by the dental professional. Remineralization agents and the forms available are given in Table 1.
Table 1.
Remineralization agents used in the management of WSL
| Agent used for remineralization | Mechanism of action | Form available for use commercially | ||
|---|---|---|---|---|
| Fluorides | Fluorides replace the hydroxyl group in the hydroxyapatite crystals in the enamel to form fluorapatite, which is more resistant to acid dissolution as their critical pH for solubility is much lower than that of regular HAP in the enamel.[31,32] | Toothpaste,[31] mouth rinse,[33] gels,[8] sealants,[34] varnishes,[35] and fluoride-releasing elastomers[36] | ||
| Casein phosphopeptides- stabilized amorphous calcium phosphate (CPP-ACP) | This is a product derived from the milk case which when applied topically caused the supersaturation of calcium and phosphate ion concentration in the surrounding environment of the tooth, which in turn helps in preventing demineralization by forming a layer that fills the inter-prismatic space and also promotes remineralization[37] | Toothpaste, water-based mousse, sealant, varnish, mouth wash, and lozenges[38,39] | ||
| Resin infiltration | In this method, the pores in the enamel caused due to demineralization, which might be filled with air or water, are penetrated and filled using resin infiltration. The tooth is etched with 15% HCl for 2 mins under rubber dam isolation, and then after rinsing and drying of the enamel, a low-viscosity resin is applied and light-cured.[40,41,42] |
ICON[40,41,42] | ||
| Bioactive glass (BAG)- Novamin and BiominF | BG-45S5 contains calcium, sodium, phosphate, and silicate ions, which cause enamel remineralization by the formation of hydroxycarbonate apatite (HCA) similar to hydroxyapatite present in the enamel. It also has been shown to have bactericidal action against Streptococcus mutants and lactobacillus.[43,44] | Toothpaste,[44] sealants,[45] bonding agents,[46] and surface coating agent.[47] | ||
| Calcium carbonate carrier-SensiStat | It is a mixture of arginine bicarbonate and calcium carbonate. Arginine holds the calcium carbonate to the tooth surface and allows remineralization of the enamel. | Dental cream is like a preclude and include.[48,49] | ||
| Anticay- Toothmin | A calcium sucrose phosphate–calcium orthophosphate blend that reduces demineralization and advances remineralization. | Toothpaste[50] | ||
| Biomimetic hydroxyapatite | It is similar to biological hydroxyapatite present in the tooth structure. It is an artificial form and is available in variable sizes as micro- or nanoparticles. It forms a layer over the demineralized enamel which resembles the biological hap and promotes remineralization. | Toothpaste[51,52,53] | ||
| Xylitol | It is a polyol, which may be used as a low-calorie substitute for sugar. It serves as a substrate for metabolization by S. mutans. It is usually incorporated into chewing gums, which enhances the flow of stimulated saliva which contains a higher concentration of calcium and phosphate ions than unstimulated saliva. Hence, it increases salivary pH, decreases demineralization, and promotes remineralization. | Chewing gum, varnishes, and toothpaste[54,55,56,57,58,59] |
Strategies to Manage WSL
Apart from the various agents available, certain procedures are also available to manage WSLs. A few are listed below:
Micro-abrasion
It was introduced in 1986 by Croll and Cavanaugh. In this procedure, a combination of pumice and 18% hydrochloric acid slurry is applied to the demineralized tooth surface. Surface removal of the hypo-mineralized enamel creates a smooth and lustrous appearance with different optical properties that contribute to improved esthetics. In this procedure, 0.2 mm of a uniform enamel surface is removed. Micro-abrasion exposes the outer, prism-free region which alters the scattering property of light and helps to mask the imperfections. However, the disadvantage is that substantial amounts of the enamel are eroded to create a flawless surface.[59,60]
Bleaching
Bussadori et al. found out the benefits of using a 35% hydrogen peroxide (H2O2) bleaching therapy for masking WSLs.[61] Bleaching is carried out using different concentrations of hydrogen peroxide or carbamide peroxide. The reactive oxygen species liberated during bleaching lead to the lightening of color and creating a uniform hue, thus masking the WSL. However, bleaching is said to further decrease the surface roughness and micro-hardness of the enamel in a few studies. Hence, it is always recommended to use remineralizing agents following bleaching to overcome the side effects.[59,62]
Laser
Argon lasers, CO2, Nd-YAG, and erbium YAG lasers are usually used for the management of demineralization of the enamel. The exact mechanism is still under research. The most probable mechanism hypothesized so far is that laser irradiation causes micro-spaces to appear within the enamel irregularities due to the explosion of entrapped water molecules. These micro-spaces are shown to provide an area for ion absorption and exchange, leading to remineralization.[63]
Plasma treatment
Plasma is a gaseous medium that penetrates easily into irregular surfaces. The plasma is shown to effectively improve the substrate surface hydrophilicity. Cold-plasma treatment is proven to increase remineralization capability and also alter the micro-hardness of the enamel in WSLs.[48]
Potential Areas for Future Research on WSLs Using Natural Extracts
-
Chitosan:
Chitosan is a polymer that is obtained by the deacetylation of chitin, the exoskeleton component of crustaceans. It prevents demineralization and enhances remineralization.[64,65]
-
Galla chinensis:
It is a traditional medicine used in China which is of natural origin. It is shown to stabilize the organic matrix of the enamel and hence protect it from dissolution by acids.[66]
-
Ginger:
Gingerol-10, which is an essential phenol obtained from ginger, is shown to have an anti-bacterial effect against cariogenic microorganisms.[67,68]
-
Natural honey:
Manuka honey has been shown to inhibit Streptococcus mutans. It contains flavonoids and hydrogen peroxide, which contribute to its anticaries activity.[68]
-
Cinnamon extract:
Transcinnamaldehyde, eugenol, and cinnamyl acetate present in cinnamon are shown to exhibit antimicrobial properties against caries-causing microorganisms and hence decrease demineralization.[69]
-
Green tea extract:
Epigallocatechin-3-gallate (EGCG) is shown to be responsible for the anti-carcinogenic properties of green tea.[68,69,70,71]
-
Bitter chocolate:
Theobromine present in bitter chocolate has been shown to enhance enamel remineralization.[68]
Numerous research studies in the scientific literature have explored WSLs resulting from treatment, employing various approaches to address WSL, as illustrated in Table 2.
Table 2.
Studies on WSLs in the scientific literature
| Authors and year | Nature of study | Methodology | Conclusion | |||
|---|---|---|---|---|---|---|
| Sonesson et al. in 2023[72] | Systematic review | Evaluation of the effect of continuous application of fluoride varnish during fixed orthodontic treatment in the prevention of WSLs. | WSL adjacent to brackets was shown to be prevented on professional application of fluoride varnish regularly during fixed orthodontic treatment.[72] | |||
| Höchli et al. in 2017[73] | Systematic review and meta-analysis | The therapeutic and adverse effects of casein phosphopeptide stabilized amorphous calcium phosphate creams, external tooth bleaching, low- or high-concentration fluoride films, gels, mouth rinses or varnishes, resin infiltration, miswak chewing sticks, bioactive glass toothpaste, or to no adjunct treatment (i.e., conventional oral hygiene) in the management of WSL were evaluated. | The regular use of fluoride varnish followed by the use of fluoride film was shown to be effective in the management of WSL compared to other agents.[73] | |||
| Aref et al. in 2022[74] | In vitro study | Evaluation of the effectiveness of casein phosphopeptide amorphous calcium phosphate (CPP-ACP) coupled with universal adhesive resin in the treatment of WSLs. | Treatment of WSL using CPP-ACP and consequently coated with universal adhesive resin is shown to be promising in the management of WSL efficiently through increasing surface microhardness and restoring esthetics while yielding a smoother surface.[74] | |||
| Horan et al. in 2023[75] | Randomized clinical trial | To evaluate the development of WSLs during fixed orthodontic therapy and compare between the conventional three-step bonding system, a self-etching primer bonding system, and a one-step adhesive bonding system. | WSL was significantly greater in the group in which the one-step adhesive system was used compared with the groups that used self-etch primer and the conventional bonding system.[75] | |||
| Gu et al. in 2019[76] | A split-mouth, randomized clinical trial | To compare the effectiveness of resin infiltration and microabrasion in the treatment of WSL for 12 months | Resin infiltration showed superior results in the management of WSL compared to microabrasion at 12 months[76] | |||
| Mahmoudzadeh et al. in 2019[77] | Randomized clinical trial | Assessment of the effectiveness of carbon dioxide (CO2) laser in the prevention of WSLs. | The CO2 laser irradiation seemed to be effective in the prevention of the incidence of WSLs.[77] | |||
| Sardana et al. in 2019[78] | Systematic review | To appraise the current literature systematically for evaluating the effectiveness of self-applied topical fluorides in the management of WSLs. | This study did not confirm the effectiveness of self-applied fluorides in the management of WSLs developed during fixed orthodontic treatment.[78] | |||
| Hu et al. in 2020[79] | Systematic review and meta-analysis | Comparing the effectiveness of remineralizing agents [sodium fluoride (NaF), acidulated phosphate fluoride (APF) foam, dichlorosilane (Dfs) varnish, and high-concentration fluoride toothpaste (HFT)] in management of WSLs. | APF foam showed the highest remineralization efficiency, followed by Dfs varnish and HFT.[79] | |||
| Albhaisi et al. in 2020[80] | Randomized clinical trial | To compare WSL development between clear aligner (CA) therapy and orthodontic fixed appliance (FA) | The CA group showed large but shallow WSL development, but the FA group developed more new severe lesions that were smaller in area. More plaque accumulation was found in the FA group compared with the CA group.[80] | |||
| Adel et al. in 2020 | An in vitro study | Comparison of the effect of the use of laser, casein phosphopeptide–amorphous calcium phosphate (CPP–ACP), and their combination on the management of WSL using polarized light microscopy to check lesion depth. | The combined use of laser and CPP–ACP showed the best result in the management of WSL development. The use of CPP–ACP or laser alone also resulted in a good reduction in WSL but was less than their combined use, with no significant difference between them.[81] |
Conclusion
Though a lot of remineralizing agents are available in the market and a great deal of research has also been in progress regarding the prevention of WSLs, nothing has been shown to 100% eradicate the problem. Hence, an ideal product that has the property to prevent demineralization and also promote remineralization, instead of having either one property alone, might be a good solution to eradicate WSLs, which should also be accompanied by good patient compliance in maintaining oral hygiene.
Highlights
The surge in orthodontic treatments for esthetic enhancement has led to widespread popularity, especially with the preference for aligners over traditional methods.
However, this rise in treatment demand has brought attention to the development of white spot lesions (WSLs), visible signs of enamel hypo-mineralization. These lesions can manifest as early as 1 week into treatment, posing esthetic concerns.
Factors contributing to WSLs include prolonged acidity, genetic susceptibility, and systemic illnesses.
Diagnosis involves various aids such as quantitative laser fluorescence and imaging techniques.
Management strategies encompass multifaceted approaches, including oral hygiene education, prophylaxis, and exploration of natural extracts for potential preventive measures.
Ongoing research aims to discover a comprehensive solution for the prevention and effective management of WSLs.
Abbreviations
WSL: White spot lesion
QLF: Quantitative laser fluorescence
QLF-D: Quantitative laser fluorescence-Digital
ICDAS: International Caries Detection and Assessment System
DSLR: Digital single-lens reflex
OCT: Optical coherence tomography
TD-OCT: Time-domain principle
SS-OCT: Swept-source OCT
XRMT: X-ray micro-tomography
SEM: Scanning electron microscopy
CIELAB: Commission Internationale de l’Eclairage
CLSM: Confocal laser scanning microscopy
CPP-ACP: Casein phosphopeptides-stabilized amorphous calcium phosphate
ICON
BAG: Bioactive glass
HCA: Hydroxycarbonate apatite
HFT: High-concentration fluoride toothpaste
APF: Acidulated phosphate fluoride
Dfs: Dichlorosilane
CA: Clear aligner
FA: Fixed appliance.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
References
- 1.Heymann GC, Grauer D. A contemporary review of white spot lesions in orthodontics. J Esthet Restor Dent. 2013;25:85–95. doi: 10.1111/jerd.12013. [DOI] [PubMed] [Google Scholar]
- 2.Karad A, Dhole P, Juvvadi SR, Joshi S, Gupta A. White spot lesions in orthodontic patients: An expert opinion. J Int Oral Health. 2019;11:172–80. [Google Scholar]
- 3.Toti Ç, Meto A, Kaçani G, Droboniku E, Hysi D, Tepedino M, et al. White spots prevalence and tooth brush habits during orthodontic treatment. Healthcare (Basel) 2022;10:320. doi: 10.3390/healthcare10020320. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Abufarwa M, Voorhees RD, Varanasi VG, Campbell PM, Buschang PH. White spot lesions: Does etching matter? J Investig Clin Dent. 2018;9:e12285. doi: 10.1111/jicd.12285. [DOI] [PubMed] [Google Scholar]
- 5.Miller MJ, Bernstein S, Colaiacovo SL, Nicolay O, Cisneros GJ. Demineralized white spot lesions: An unmet challenge for orthodontists. Semin Orthod. 2016;22:193–204. [Google Scholar]
- 6.Shimpo Y, Nomura Y, Sekiya T, Arai C, Okada A, Sogabe K, et al. Effects of the dental caries preventive procedure on the white spot lesions during orthodontic treatment—An open-label randomized controlled trial. J Clin Med. 2022;11:854. doi: 10.3390/jcm11030854. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Bishara SE, Ostby AW, Laffoon J, Warren JJ. Enamel cracks and ceramic bracket failure during debonding in vitro. Angle Orthod. 2008;78:1078–83. doi: 10.2319/112007-540.1. [DOI] [PubMed] [Google Scholar]
- 8.Øgaard B. White spot lesions during orthodontic treatment: Mechanisms and fluoride preventive aspects. Semin Orthod. 2008;14:183–93. [Google Scholar]
- 9.Guzmán-Armstrong S, Chalmers J, Warren JJ. White spot lesions: Prevention and treatment. Am J Orthod Dentofacial Orthop. 2010;138:690–6. doi: 10.1016/j.ajodo.2010.07.007. [DOI] [PubMed] [Google Scholar]
- 10.Roberts WE, Mangum JE, Schneider PM. Pathophysiology of demineralization, part II: Enamel white spots, cavitated caries, and bone infection. Curr Osteoporos Rep. 2022;20:106–19. doi: 10.1007/s11914-022-00723-0. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.He T, Li X, Dong Y, Zhang N, Zhong Y, Yin W, et al. Comparative assessment of fluoride varnish and fluoride film for remineralization of post orthodontic white spot lesions in adolescents and adults over 6 months: A single-center, randomized controlled clinical trial. Am J Orthod Dentofacial Orthop. 2016;149:810–9. doi: 10.1016/j.ajodo.2015.12.010. [DOI] [PubMed] [Google Scholar]
- 12.Julien KC, Buschang PH, Campbell PM. Prevalence of white spot lesion formation during orthodontic treatment. Angle Orthod. 2013;83:641–7. doi: 10.2319/071712-584.1. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Manton DJ. Diagnosis of the early carious lesion. Aust Dent J. 2013;58:35–9. doi: 10.1111/adj.12048. [DOI] [PubMed] [Google Scholar]
- 14.Kitasako Y, Sadr A, Shimada Y, Ikeda M, Sumi Y, Tagami J. Remineralization capacity of carious and non-carious white spot lesions: Clinical evaluation using ICDAS and SS-OCT. Clin Oral Investig. 2019;23:863–72. doi: 10.1007/s00784-018-2503-1. [DOI] [PubMed] [Google Scholar]
- 15.Ismaïl AI, Sohn W, Tellez M, Amaya A, Sen A, Hasson H, et al. The International caries detection and assessment system (ICDAS): An integrated system for measuring dental caries. Community Dent Oral Epidemiol. 2007;35:170–8. doi: 10.1111/j.1600-0528.2007.00347.x. [DOI] [PubMed] [Google Scholar]
- 16.Beerens MW, Boekitwetan F, Van Der Veen MH, Ten Cate JM. White spot lesions after orthodontic treatment assessed by clinical photographs and by quantitative light-induced fluorescence imaging; A retrospective study. Acta Odontol Scand. 2015;73:441–6. doi: 10.3109/00016357.2014.980846. [DOI] [PubMed] [Google Scholar]
- 17.De Jong ED, Sundström F, Westerling H, Tranaeus S, Ten Bosch JJ, Angmar-Månsson B. A new method for in vivo quantification of changes in initial enamel caries with laser fluorescence. Caries Res. 1995;29:2–7. doi: 10.1159/000262032. [DOI] [PubMed] [Google Scholar]
- 18.Fathima F, Mathew BT. Quantitative light-induced fluorescence (QLF) in orthodontics–A review. Eur J Mol Clin Med. 2021;8:303–12. [Google Scholar]
- 19.Kim BR, Kang SM, de Josselin de Jong E, Kwon HK, Kim BI. In vitro red fluorescence as an indicator of caries lesion activity. Oper Dent. 2019;44:405–13. doi: 10.2341/17-369-L. [DOI] [PubMed] [Google Scholar]
- 20.Erbe C, Hartmann L, Schmidtmann I, Ohlendorf D, Wehrbein H. A novel method quantifying caries following orthodontic treatment. Sci Rep. 2021;11:1–5. doi: 10.1038/s41598-021-00561-7. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Rawls HR, Owen WD. Demonstration of dye-uptake as a potential aid in early diagnosis of incipient caries. Caries Res. 1978;12:69–75. doi: 10.1159/000260317. [DOI] [PubMed] [Google Scholar]
- 22.O’Brien WJ, Vazquez L, Johnston WM. The detection of incipient caries with tracer dyes. J Dent Res. 1989;68:157–8. doi: 10.1177/00220345890680021101. [DOI] [PubMed] [Google Scholar]
- 23.Benson PE, Parkin N, Millett DT, Dyer FE, Vine S, Shah A. Fluorides for the prevention of white spots on teeth during fixed brace treatment. Cochrane Database Syst Rev. 2004;(3):CD003809. doi: 10.1002/14651858.CD003809.pub2. [DOI] [PubMed] [Google Scholar]
- 24.Ibusuki T, Kitasako Y, Sadr A, Shimada Y, Sumi Y, Tagami J. Observation of white spot lesions using swept-source optical coherence tomography (SS-OCT): In vitro and in vivo study. Dent Mater J. 2015;34:545–52. doi: 10.4012/dmj.2015-058. [DOI] [PubMed] [Google Scholar]
- 25.Lussi A, Hibst R, Paulus R. DIAGNOdent: An optical method for caries detection. J Dent Res. 2004;83(1_Suppl):C80–3. doi: 10.1177/154405910408301s16. [DOI] [PubMed] [Google Scholar]
- 26.Tagtekin DA, Ozyoney G, Baseren M, Ando M, Hayran O, Alpar R, et al. Caries detection with DIAGNOdent and ultrasound. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2008;106:729–35. doi: 10.1016/j.tripleo.2008.05.010. [DOI] [PubMed] [Google Scholar]
- 27.Huang TT, Jones AS, He LH, Darendeliler MA, Swain MV. Characterization of enamel white spot lesions using X-ray micro-tomography. J Dent. 2007;35:737–43. doi: 10.1016/j.jdent.2007.06.001. [DOI] [PubMed] [Google Scholar]
- 28.Pai D, Bhat S, Taranath A, Sargod S, Pai V. Use of laser fluorescence and scanning electron microscope to evaluate remineralization of incipient enamel lesions remineralized by topical application of casein phospho peptide amorphous calcium phosphate (CPP-aCP) containing cream. J Clin Pediatr Dent. 2008;32:201–6. doi: 10.17796/jcpd.32.3.d083470201h58m13. [DOI] [PubMed] [Google Scholar]
- 29.Kim HE, Kim BI. An in vitro comparison of quantitative light-induced fluorescence-digital and spectrophotometer on monitoring artificial white spot lesions. Photodiagnosis Photodyn Ther. 2015;12:378–84. doi: 10.1016/j.pdpdt.2015.06.006. [DOI] [PubMed] [Google Scholar]
- 30.Wang L, de Almendra Freitas MC, Prakki A, Mosquim V, González AH, Rios D, et al. Experimental self-etching resin infiltrants on the treatment of simulated carious white spot lesions. J Mech Behav Biomed Mater. 2021;113:104146. doi: 10.1016/j.jmbbm.2020.104146. [DOI] [PubMed] [Google Scholar]
- 31.Shen P, McKeever A, Walker GD, Yuan Y, Reynolds C, Fernando JR, et al. Remineralization and fluoride uptake of white spot lesions under dental varnishes. Aust Dent J. 2020;65:278–85. doi: 10.1111/adj.12787. [DOI] [PubMed] [Google Scholar]
- 32.Sardana D, Zhang J, Ekambaram M, Yang Y, McGrath CP, Yiu CK. Effectiveness of professional fluorides against enamel white spot lesions during fixed orthodontic treatment: A systematic review and meta-analysis. J Dent. 2019;82:1–10. doi: 10.1016/j.jdent.2018.12.006. [DOI] [PubMed] [Google Scholar]
- 33.Oliveira GM, Ritter AV, Heymann HO, Swift E, Jr, Donovan T, Brock G, et al. Remineralization effect of CPP-ACP and fluoride for white spot lesions in vitro. J Dent. 2014;42:1592–602. doi: 10.1016/j.jdent.2014.09.004. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 34.Bock NC, Seibold L, Heumann C, Gnandt E, Röder M, Ruf S. Changes in white spot lesions following post-orthodontic weekly application of 1.25 percent fluoride gel over 6 months—A randomized placebo-controlled clinical trial. Part II: Clinical data evaluation. Eur J Orthod. 2017;39:144–52. doi: 10.1093/ejo/cjw061. [DOI] [PubMed] [Google Scholar]
- 35.Knösel M, Ellenberger D, Göldner Y, Sandoval P, Wiechmann D. In-vivo durability of a fluoride-releasing sealant (OpalSeal) for protection against white-spot lesion formation in orthodontic patients. Head Face Med. 2015;11:1–8. doi: 10.1186/s13005-015-0069-6. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 36.Vivaldi-Rodrigues G, Demito CF, Bowman SJ, Ramos AL. The effectiveness of a fluoride varnish in preventing the development of white spot lesions. World J Orthod. 2006;7:138–44. [PubMed] [Google Scholar]
- 37.Miura KK, Ito IY, Enoki C, Elias AM, Matsumoto MA. Anticariogenic effect of fluoride-releasing elastomers in orthodontic patients. Braz Oral Res. 2007;21:228–33. doi: 10.1590/s1806-83242007000300007. [DOI] [PubMed] [Google Scholar]
- 38.Indrapriyadharshini K, Kumar PM, Sharma K, Iyer K. Remineralizing potential of CPP-ACP in white spot lesions–A systematic review. Indian J Dent Res. 2018;29:487–96. doi: 10.4103/ijdr.IJDR_364_17. [DOI] [PubMed] [Google Scholar]
- 39.Gupta R, Prakash V. CPP-ACP complex as a new adjunctive agent for remineralization: A review. Oral Health Prev Dent. 2011;9:151–65. [PubMed] [Google Scholar]
- 40.Imani MM, Safaei M, Afnaniesfandabad A, Moradpoor H, Sadeghi M, Golshah A, et al. Efficacy of CPP-ACP and CPP-ACPF for prevention and remineralization of white spot lesions in orthodontic patients: A systematic review of randomized controlled clinical trials. Acta Inform Med. 2019;27:199–204. doi: 10.5455/aim.2019.27.199-204. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 41.Paris S, Schwendicke F, Keltsch J, Dörfer C, Meyer-Lueckel H. Masking of white spot lesions by resin infiltration in vitro. J Dent. 2013;41:e28–34. doi: 10.1016/j.jdent.2013.04.003. [DOI] [PubMed] [Google Scholar]
- 42.Senestraro SV, Crowe JJ, Wang M, Vo A, Huang G, Ferracane J, et al. Minimally invasive resin infiltration of arrested white-spot lesions: A randomized clinical trial. J Am Dent Assoc. 2013;144:997–1005. doi: 10.14219/jada.archive.2013.0225. [DOI] [PubMed] [Google Scholar]
- 43.Knösel M, Eckstein A, Helms HJ. Long-term follow-up of camouflage effects following resin infiltration of post orthodontic white-spot lesions in vivo. Angle Orthod. 2019;89:33–9. doi: 10.2319/052118-383.1. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 44.Milly H, Festy F, Watson TF, Thompson I, Banerjee A. Enamel white spot lesions can remineralize using bio-active glass and polyacrylic acid-modified bio-active glass powders. J Dent. 2014;42:158–66. doi: 10.1016/j.jdent.2013.11.012. [DOI] [PubMed] [Google Scholar]
- 45.Salah R, Afifi RR, Kehela HA, Aly NM, Rashwan M, Hill RG. Efficacy of novel bioactive glass in the treatment of enamel white spot lesions: A randomized controlled trial. J Evid Based Dent Pract. 2022;22:101725. doi: 10.1016/j.jebdp.2022.101725. [DOI] [PubMed] [Google Scholar]
- 46.Abbassy MA, Bakry AS, Almoabady EH, Almusally SM, Hassan AH. Characterization of a novel enamel sealer for bioactive remineralization of white spot lesions. J Dent. 2021;109:103663. doi: 10.1016/j.jdent.2021.103663. [DOI] [PubMed] [Google Scholar]
- 47.Manfred L, Covell DA, Crowe JJ, Tufekci E, Mitchell JC. A novel biomimetic orthodontic bonding agent helps prevent white spot lesions adjacent to brackets. Angle Orthod. 2013;83:97–103. doi: 10.2319/110811-689.1. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 48.El-Wassefy NA. The effect of plasma treatment and bioglass paste on enamel white spot lesions. Saudi J Dent Res. 2017;8:58–66. [Google Scholar]
- 49.Andrian S, Stoleriu S, Tărăboanţă I, Gamen AC, Dimbu E, Negraia D. Remineralization of incipient enamel lesions using non-fluoride agents. A review. Int J Med Dent. 2018;22:41. [Google Scholar]
- 50.Hegde S, Roma M, Shetty D. Non-fluoridated remineralization agents in dentistry. J Pharm Sci Res. 2016;8:884–7. [Google Scholar]
- 51.Raghu TN, Ananthakrishna S. Remineralization potential of calcium sucrose phosphate on demineralized enamel: Results of an in vitro study. J Int Oral Health. 2016;8:704–8. [Google Scholar]
- 52.Colombo M, Beltrami R, Rattalino D, Mirando M, Chiesa M, Poggio C. Protective effects of a zinc-hydroxyapatite toothpaste on enamel erosion: SEM study. Ann Stomatol (Roma) 2017 Jan 10;7(3):38–45. doi: 10.11138/ads/2016.7.3.038. doi: 10.11138/ads/2016.7.3.038. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 53.Badr S, Ragab H. The effectiveness of a nano-hydroxyapatite paste and a tri-calcium phosphate fluoride varnish in white spot lesions remineralization (randomized clinical trial) Egypt Dent J. 2018;64:2757–65. [Google Scholar]
- 54.Singh A, Shetty B, Mahesh CM, Reddy VP, Chandrashekar BS, Mahendra S. Evaluation of efficiency of two nanohydroxyapatite remineralizing agents with hydroxyapatite and a conventional dentifrice: A comparative In vitro study. J Indian Orthod Soc. 2017;51:92–102. [Google Scholar]
- 55.Miake Y, Saeki Y, Takahashi M, Yanagisawa T. Remineralization effects of xylitol on demineralized enamel. J Electron Microsc (Tokyo) 2003;52:471–6. doi: 10.1093/jmicro/52.5.471. [DOI] [PubMed] [Google Scholar]
- 56.Steinberg LM, Odusola F, Mandel ID. Remineralizing potential, antiplaque, and antigingivitis effects of xylitol and sorbitol sweetened chewing gum. Clin Prev Dent. 1992;14:31–4. [PubMed] [Google Scholar]
- 57.Cardoso CA, Cassiano LP, Costa EN, Souza-E-Silva CM, Magalhães AC, Grizzo LT, et al. Effect of xylitol varnishes on remineralization of artificial enamel caries lesions in situ. J Dent. 2016;50:74–8. doi: 10.1016/j.jdent.2016.03.011. [DOI] [PubMed] [Google Scholar]
- 58.Sano H, Nakashima S, Songpaisan Y, Phantumvanit P. Effect of xylitol and fluoride-containing toothpaste on the remineralization of human enamel in vitro. J Oral Sci. 2007;49:67–73. doi: 10.2334/josnusd.49.67. [DOI] [PubMed] [Google Scholar]
- 59.Donly KJ, Sasa IS. Potential remineralization of post orthodontic demineralized enamel and the use of enamel microabrasion and bleaching for esthetics. Semin Orthod. 2008;14:220–5. [Google Scholar]
- 60.Son JH, Hur B, Kim HC, Park JK. Management of white spots: Resin infiltration technique and micro abrasion. J Korean Acad Conserv Dent. 2011;36:66–71. [Google Scholar]
- 61.Bussadori SK, do Rego MA, da Silva PE, Pinto MM, Pinto AC. Esthetic alternative for fluorosis blemishes with the usage of a dual bleaching system based on hydrogen peroxide at 35% J Clin Pediatr Dent. 2004;28:143–6. doi: 10.17796/jcpd.28.2.g45173lp7661g078. [DOI] [PubMed] [Google Scholar]
- 62.Kim Y, Son HH, Yi K, Ahn JS, Chang J. Bleaching effects on color, chemical, and mechanical properties of white spot lesions. Oper Dent. 2016;41:318–26. doi: 10.2341/15-015-L. [DOI] [PubMed] [Google Scholar]
- 63.Poosti M, Ahrari F, Moosavi H, Najjaran H. The effect of fractional CO2 laser irradiation on remineralization of enamel white spot lesions. Lasers Med Sci. 2014;29:1349–55. doi: 10.1007/s10103-013-1290-9. [DOI] [PubMed] [Google Scholar]
- 64.Zhang J, Lynch RJ, Watson TF, Banerjee A. Chitosan-bioglass complexes promote subsurface remineralization of incipient human carious enamel lesions. J Dent. 2019;84:67–75. doi: 10.1016/j.jdent.2019.03.006. [DOI] [PubMed] [Google Scholar]
- 65.Zhang J, Lynch RJ, Watson TF, Banerjee A. Remineralization of enamel white spot lesions pre-treated with chitosan in the presence of salivary pellicle. J Dent. 2018;72:21–8. doi: 10.1016/j.jdent.2018.02.004. [DOI] [PubMed] [Google Scholar]
- 66.Huang S, Gao S, Cheng L, Yu H. Combined effects of nano-hydroxyapatite and Galla chinensis on remineralization of initial enamel lesion in vitro. J Dent. 2010;38:811–9. doi: 10.1016/j.jdent.2010.06.013. [DOI] [PubMed] [Google Scholar]
- 67.Hassan S, Hafez A, Elbaz MA. Remineralization potential of ginger and rosemary herbals versus sodium fluoride in treatment of white spot lesions: A randomized clinical trial. Egypt Dent J. 2021;67:1677–84. [Google Scholar]
- 68.Çelik ZC, Özbay Yavlal G, Yanıkoğlu F, Kargül B, Tağtekin D, Stookey GK, et al. Do ginger extract, natural honey and bitter chocolate remineralize enamel surface as fluoride toothpaste? An in-vitro study. Niger J Clin Pract. 2021;24:1283–8. doi: 10.4103/njcp.njcp_683_20. [DOI] [PubMed] [Google Scholar]
- 69.Maha J. Al Anni M. Sc. Effect of water extracts of cinnamon on the microhardnessof initial carious lesion of permanent teeth, compared tostannous fluoride (An in vitro study) J Bagh Coll Dentistry. 2011;23(1):120–124. [Google Scholar]
- 70.Farouk H, Mosallam R, Aidaros NH. Effect of green tea, black tea and moringa oleifera on remineralization of artificially demineralized enamel and dentin: An in-vitro microhardness analysis. Adv Dent J. 2021;3:24–34. [Google Scholar]
- 71.Ferrazzano GF, Roberto L, Amato I, Cantile T, Sangianantoni G, Ingenito A. Antimicrobial properties of green tea extract against cariogenic microflora: An in vivo study. J Med Food. 2011;14:907–11. doi: 10.1089/jmf.2010.0196. [DOI] [PubMed] [Google Scholar]
- 72.Sonesson M, Twetman S. Prevention of white spot lesions with fluoride varnish during orthodontic treatment with fixed appliances: A systematic review. Eur J Orthod. 2023;45:485–90. doi: 10.1093/ejo/cjad013. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 73.Höchli D, Hersberger-Zurfluh M, Papageorgiou SN, Eliades T. Interventions for orthodontically induced white spot lesions: A systematic review and meta-analysis. Eur J Orthod. 2017;39:122–33. doi: 10.1093/ejo/cjw065. [DOI] [PubMed] [Google Scholar]
- 74.Aref NS, Alrasheed MK. Casein phosphopeptide amorphous calcium phosphate and universal adhesive resin as a complementary approach for management of white spot lesions: An in-vitro study. Prog Orthod. 2022;23:10. doi: 10.1186/s40510-022-00404-9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 75.Horan OG, Al-Khateeb SN. Comparison of three orthodontic bonding systems in white spot lesion development: A randomized clinical trial. Angle Orthod. 2023;93:531–7. doi: 10.2319/111422-781.1. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 76.Gu X, Yang L, Yang D, Gao Y, Duan X, Zhu X, et al. Esthetic improvements of post orthodontic white-spot lesions treated with resin infiltration and microabrasion: A split-mouth, randomized clinical trial. Angle Orthod. 2019;89:372–7. doi: 10.2319/041218-274.1. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 77.Mahmoudzadeh M, Alijani S, Soufi LR, Farhadian M, Namdar F, Karami S. Effect of CO2 laser on the prevention of white spot lesions during fixed orthodontic treatment: A randomized clinical trial. Turk J Orthod. 2019;32:165–71. doi: 10.5152/TurkJOrthod.2019.18052. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 78.Sardana D, Manchanda S, Ekambaram M, Yang Y, McGrath CP, Yiu CK. Effectiveness of self-applied topical fluorides against enamel white spot lesions from multi-bracketed fixed orthodontic treatment: A systematic review. European Journal of Orthodontics. 2019;41:661–8. doi: 10.1093/ejo/cjz015. [DOI] [PubMed] [Google Scholar]
- 79.Hu H, Feng C, Jiang Z, Wang L, Shrestha S, Yan J, et al. Effectiveness of remineralizing agents in the prevention and reversal of orthodontically induced white spot lesions: A systematic review and network meta-analysis. Clin Oral Investig. 2020;24:4153–67. doi: 10.1007/s00784-020-03610-z. [DOI] [PubMed] [Google Scholar]
- 80.Albhaisi Z, Al-Khateeb SN, Alhaija ES. Enamel demineralization during clear aligner orthodontic treatment compared with fixed appliance therapy, evaluated with quantitative light-induced fluorescence: A randomized clinical trial. Am J Orthod Dentofacial Orthop. 2020;157:594–601. doi: 10.1016/j.ajodo.2020.01.004. [DOI] [PubMed] [Google Scholar]
- 81.Adel SM, Marzouk ES, El-Harouni N. Combined effect of Er, Cr: YSGG laser and casein phosphopeptide amorphous calcium phosphate on the prevention of enamel demineralization: An in-vitro study. Angle Orthod. 2020;90:369–75. doi: 10.2319/032819-238. [DOI] [PMC free article] [PubMed] [Google Scholar]