

Abstract
BACKGROUND:
Gestational diabetes mellitus (GDM) is a glucose intolerance that shows its first onset during pregnancy. In India, GDM affects as many as 5 million women annually. The interprofessional collaborative educational intervention is crucial for GDM management. This study illustrates the collaborative effort in developing and validating an interprofessional health education module designed for healthcare professionals during consultation sessions with GDM patients.
MATERIALS AND METHODS:
The investigation involved three stages: 1) needs assessment for module contents and objectives, 2) health education module development by an interprofessional team, and 3) module validation. We received ethics approval from the institution's ethics committee.
RESULTS:
The interprofessional team developed and validated the evidence-based English-printed module. The module had 27 units and covered six topics: an introduction to GDM and its management, dietary recommendations for GDM, exercise, yoga recommendations for GDM, weight control, and postpartum care.
CONCLUSION:
The interprofessional team developed the educational module, wherein there is an integration of the domains of exercise and yoga along with medicines and nutrition therapy. The module was developed based on local requirements and evidence-based practices. Healthcare professionals can use the interprofessional health education module when advising diabetic pregnant patients.
Keywords: Exercise, gestational diabetes mellitus, interprofessional, module, nutrition, yoga
Introduction
Gestational diabetes mellitus (GDM) is a glucose intolerance that shows its first onset during pregnancy.[1] The prevalence of GDM shows an upward trend in low-income and middle-income countries. The age-standardized prevalence of GDM in India is 28%, compared with 14% in high-income countries.[2] GDM affects as many as 5 million women in India annually.[3] GDM poses short-term and long-term health consequences for the mother and child. The importance of accepting and dealing with the disease is now an acceptable phenomenon among healthcare professionals. Despite several guidelines by various organizations, most women with GDM in low- and middle-income countries are undiagnosed or inadequately managed.[4]
Reports have disclosed that scarcity of knowledge about GDM, limited availability of resources, failure to approach follow-up care, and low motivation and compliance of the patients due to a lack of social support acted as substantial barriers to detecting and managing GDM.[5,6] Even though India has evidence-based GDM management and detection guidelines, there is a need for better implementation. A national audit showed that only one-third of the practicing physicians were adhering to the federal guidelines for screening, of which two-thirds were unable to recollect the protocol.[7] In Bangalore, India, a study demonstrated that only 50% of the doctors had sound knowledge about GDM management.[8] Educational interventions targeted to improve knowledge of clinical guidelines are effective in improving the practice of health providers and clinical outcomes, including diabetes.[9,10]
Pregnancy is a considerable time in the life of any woman. GDM women are self-motivated to manage the condition as it may affect the life of a fetus. Limited programs are designed for GDM, even in high-income countries.[11] Even highly effective programs fail to succeed in low- and middle-income countries if they are logistically challenging and may require resources.[4]
The interventions should consider various circumstantial and structural factors, which might disturb the use of any interventions.[4] These factors include the growing concern of family toward pregnant women, wherein every family member has an opinion that might confuse the patient and complicate the entire treatment process. Some patients even hesitate to seek answers, representing poor communication with healthcare professionals, leading to misconceptions.[12,13] Although exercise benefits pregnant women, adherence to diet, training, and medications is a significant challenge to care for GDM patients, given one's cultural practices. The necessity to educate many patients about blood glucose control and treatment compliance diverts attention from the benefits of treatment. The knowledge gap of dietary concerns and treatment protocols leads to malnutrition in mothers and children due to inadequate glucose control.[13]
The interprofessional collaborative educational intervention, including physicians, nutritionists, exercise consultants, and yoga therapists, is crucial for GDM management. This approach improves patient obedience and fosters better pregnancy outcomes.[14,15,16,17]
The study illustrates the collaborative effort to develop and validate an interprofessional health education module designed for healthcare professionals during consultation sessions with gestational diabetic patients.
Materials and Methods
Study design and setting
The mixed-methods study involving both qualitative and quantitative methods was conducted at Sri Devaraj Urs Academy of Higher Education and Research, Kolar, Karnataka, India.
There were three stages of the investigation. 1) needs evaluation for the module contents and objectives, 2) health education module development by interprofessional team, and 3) professional validation of the developed module. The institution's ethics committee granted its approval (https://drive.google.com/file/d/14hvkjIvNJaxp82zW9FRzu8z7A5KYQ6G9/view?usp=share_link). All individuals provided written informed consent for the study.
Phase I: Needs assessment for module contents and objectives
Study participants
This study included physicians (n = 2), obstetrics and gynecology (OBG) consultants (n = 2), nutritionists (n = 2), physiotherapists (n = 2), and yoga consultants (n = 2) with more than 10 years of experience in their concerned field at our University.
Study design and data collection
Extensive literature review and semi-structured interviews were conducted by all the participants to determine the potential contents of interest in module development. The literature search began using search engines such as EBSCO Host and Google to find relevant guidelines, articles, and educational materials on GDM and exercise, nutrition, and yoga prescriptions for GDM. The information was extracted and summarized.
An interprofessional team from our institution that included physicians (n = 2), OBG consultants (n = 2), nutritionists (n = 2), physiotherapists (n = 2), and yoga consultants (n = 2) participated in semi-structured interviews.
Data analysis
Trained interviewers conducted the discussions in the private rooms of the participants of the study. The responses to the interview sessions were written down and summarized.
Phase II: Health education module development by an interprofessional team
Study participants
Five experts, a physician, OBG consultant, nutritionist, physiotherapist, and yoga therapist, are involved in the research activity.
Study design and data collection
Based on the interview outcomes and literature review the module development involved an iterative design and appraisal activity by five experts, comprising a physician, OBG consultant, nutritionist, physiotherapist, and yoga therapist. An English module was drafted based on the interview outcomes and review of existing literature. It consisted of 27 units under six topics of an overview of GDM and treatment, nutritional recommendations for GDM, exercise prescription for GDM, yoga prescription for GDM, weight management, and postnatal care.
Based on the phase I recommendation, printed material was the mode of delivery chosen, which can later be converted into audiovisual aids. The module used simple terms and language, colorful pictures, and culturally appropriate examples.
Phase III: Module validation
Study participants
The interprofessional team includes physicians, OBG consultants, nutritionist, physiotherapist, and yoga therapist from different private universities in our state.
Study design and data collection
The quantitative design used a content validation form. The validation form we used was adapted from an instrument proposed by Castro and colleagues.[18]
We asked a panel of interdisciplinary teams from different private universities in our state with more than a decade of experience working in their chosen fields to assess the module's contents. The team consisted of a physician (n = 2), OBG consultant (n = 2), nutritionist (n = 2), physiotherapist (n = 2), and yoga therapist (n = 2). Five experts were chosen based on the prior study's recommendations.[19] We specifically chose the diverse panel to provide concepts from each area of expertise.[20]
Content validation was an independent evaluation process using a content validation form—a modified validation form from a tool suggested by Castro and associates[18]—module on seven aspects: two aspects, scientific accuracy, and content linked to content validity. Five criteria on literary presentation, images, sufficiently explicit and understandable material, readability and printing characteristics, and quality information are related to face validity.
Data analysis
For content validation, a content validity index (CVI) was used.[21] The experts studied each unit and rated the sections on a scale ranging from 1 (strongly disagree) to 5 (strongly agree). We used the CVI to test the validity of the module content. The CVI was determined by dividing the total number of experts by those who agreed or strongly agreed (4 or 5). The CVI conveys the acceptance rate of each item's relevance, which ranges from 0 to 1.[22] An accepted item should have a CVI of 0.80 or higher.[23] According to the analysis, each item was considered appropriate if the CVI was more than 0.79, in need of revision if it was between 0.70 and 0.79, and omitted if it was less than 0.70.[24] Items considered validated for face validation had at least 75% positive answers.[25] Additionally, we sent an open-ended inquiry regarding any suggestions for enhancing the module to the experts.
The validation activity during the coronavirus disease 2019 (COVID-19) pandemic was performed via email and phone communications. An email containing a brief overview of the produced module and guidelines on how the validation process should be performed was given to the participants. The module and a validation form were included in the email.
Ethical consideration
All ethical standards were strictly adhered to by the researchers, including informed consent, confidentiality, plagiarism, double publication, and data manipulation. The ethical clearance no. is SDUMC/KLR/IEC/362/2020-21 provided by the institutional ethics committee of Sri Devaraj Urs Medical College, Kolar, Karnataka.
Results
Phase I: Needs assessment for module contents and objectives
From the literature review and search, the plan was to consider four topics with 22 units for the health education module for health professionals for use during consultation sessions with GDM patients [Table 1].
Table 1.
Proposed topics and contents for the health education module
| Topics | Contents |
|---|---|
| Introduction to GDM and its management | 1. What is gestational diabetes mellitus (GDM)? 2. Why diabetes starts during pregnancy? 3. How is GDM screened and diagnosed during pregnancy ? 4. Whom should I approach if I have GDM? 5. Will GDM affect my fetus? 6. Will GDM affect my delivery? 7. Will I have diabetes in the future? 8. What should I do if I have GDM? 9. The general treatment plan for GDM 10. Blood sugar monitoring and hypoglycemia |
| Nutritional recommendations for GDM | 1. Dietary tips for healthy eating during pregnancy 2. The meal plan composition 3. GDM sample meal plan 4. Carbohydrates, low glycemic index, and glycemic load foods 5. Regularity of meal timings 6. Diet control in insulin therapy 7. Diet chart |
| Exercise recommendation | 1. Benefits of exercise 2. Precaution to be taken 3. Exercise prescription (frequency and type mode) 4. Contraindications |
| Yoga recommendations | 1. Benefits of yoga 2. Types of yoga 3. Ratio and timing |
During interview sessions, tabular presentations with proposed topics and contents were given to ten interprofessional panelists, with a mean age of 41 ± 5 years. The interprofessional panelists included were physicians (n = 2), OBG consultants (n = 2), nutritionist (n = 2), physiotherapist (n = 2), and yoga consultants (n = 2) from our university. Most were female (60%), with a mean working experience of 10 years.
The objectives of the module derived included educating patients about GDM, associated complications, and treatment strategies in GDM, creating awareness of the significance of diet, exercise, and yoga in managing GDM and education on illusions and health facts.
Most of the panelists agreed that emphasis on the significance of optimal blood glucose maintenance is required to manage GDM. Proper dietary intake, physical activity, yoga practice, and agreement with medications and treatment plans will ensure optimum blood glucose maintenance. Regarding dietary management, most panelists highlighted the necessity for including meal portions in the diet plan. The exercise recommendations should ponder the cultural context. The panelist recommended a proposal to include common misconceptions regarding GDM and its management in the new module. Supplementing the suggested topics, the panelist also emphasized the need to include two more units on weight management and postnatal care. Culturally relevant information was also suggested by participants, as these lifestyle changes are mainly related to culture. The panelist recommended including typical locally available food as part of the cultural component.
The panelists also highlighted that a newly developed module should have fewer texts, the correct font sizes, and simpler layperson terms to cater to readers’ literacy levels within a distinct educational background. Some of the recommendations that stemmed during an interview are represented in Table 2.
Table 2.
Summary of recommendations
| Suggestions and recommendations from an expert panel |
| Emphasis on the importance of optimal blood glucose maintenance through weight management, exercise, yoga, and following a diet plan |
| Treatment plans and their monitoring |
| Exercise recommendations and emphasis on the cultural context |
| Nutrition should include local foods and culturally acceptable |
| Alleviate misconceptions about GDM |
| Contraindications for exercise |
| New modules developed should have few texts, font sizes should be appropriate, and simple layman terms to cater to readers' literacy level within a diverse educational background |
Phase 2: Development of health education module by an interprofessional team
The developed module has 27 units under six topics. The module comprises 40 pages, including a front cover and an introduction section describing the unit's objective. Table 3 summarizes the newly developed interprofessional educational module for managing GDM.
Table 3.
Summary of the newly developed module
| Topics | Contents |
|---|---|
| Introduction to GDM and its management | 1. What is GDM? 2. Why diabetes starts during pregnancy? 3. Whom should I approach if I have GDM? 4. Will GDM affect my fetus? 5. Will GDM affect my delivery? 6. Will I have DM in the future? 7. What should I do if I have GDM? 8. General treatment plan for GDM 9. Blood sugar monitoring and hypoglycemia in GDM 10. Warning signs of GDM |
| Nutritional recommendations for GDM | 1. Dietary tips for healthy eating during pregnancy 2. The meal plan composition 3. GDM sample meal plan 4. Carbohydrates, low glycemic index, and glycemic load foods 5. Regularity of meal timings 6. Diet chart 7. Inclusion of locally available food in the recommended list |
| Exercise recommendation | 1. Benefits of exercise 2. Precaution to be taken 3. Exercise prescription (frequency, type, and mode) 4. Contraindications 5. Adjuvants |
| Yoga recommendations | 1. Benefits of yoga 2. Types of yoga 3. Ratio and timing |
| Weight management | 1. The target for weight maintenance |
| Postnatal care | 1. Postnatal care and follow-up |
Phase 3: Module validation
Ten interprofessional experts from different universities validated the module with a mean age of 43 ± 7 years and a mean experience of 13 ± 6 years.
The content of the health education module obtained a CVI of 0.9 for content, and scientific accuracy obtained a score of 0.9, indicating an acceptable level of understanding between the experts for content validity [Table 4]. As the overall CVI was 0.9, the module was validated for its content.
Table 4.
Results of content validity by experts
| Items | Agree and strongly agree | Disagree and neutral | CVI | Interpretation |
|---|---|---|---|---|
| Content | ||||
| The objectives of the module are evident | 09 | 01 | 0.9 | Accepted |
| The recommendation given regarding behavior change is satisfactory | 09 | 01 | 0.9 | Accepted |
| Important points rereviewed well | 09 | 01 | 0.9 | Accepted |
| Pointless information is eliminated | 09 | 01 | 0.9 | Accepted |
| The language used is neutral and self-explanatory | 09 | 01 | 0.9 | Accepted |
| Promotes and encourages treatment adherence by emphasizing the risk and benefits of a recommendation | 09 | 01 | 0.9 | Accepted |
| Scientific accuracy | ||||
| The contents of the module are in agreement with the current trends | 09 | 01 | 0.9 | Accepted |
| Necessary recommendations are correctly managed | 09 | 01 | 0.9 | Accepted |
The expert recommendations for improvement of the module were evaluated, and vital corrections were made wherever feasible. Table 5 depicts the expert suggestions given and the action taken.
Table 5.
Expert recommendations for improvement of the module
| Recommendations by experts | Rectification |
|---|---|
| A paragraph on regular follow-up with the pediatrician as babies of GDM mothers are prone to childhood obesity | Was added in follow-up after delivery |
| Use locally grown foods with nutritional value in food recommendation | Ragi and millets are included in the recommendation with the nutritional value |
| Recommended dietary allowance for pregnant women can be highlighted and the extra allowances needed can be justified | Highlighting performed with extra allowances justified |
| Benefits of yoga in mindfulness to be included | Rectified by adding a paragraph on the benefits of yoga |
Face validity is obtained using the expert opinion on the level of agreement for five aspects of the instrument: providing good quality information, good literary presentation, adequacy of the illustrations, legibility, specificity of contents, and accuracy. Figure 1 demonstrates agreement ranging from 80% to 90% among the expert group. The minimum agreement level was 75%. The agreement shows that the module has adequate face validity.
Figure 1.
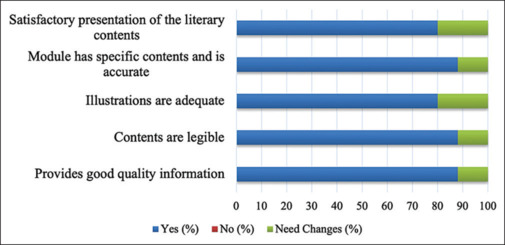
Level of agreement among experts for aspects of face validity
Discussion
The current study effectively developed an interprofessional health education module for managing GDM, which consultants can use during interactions with gestational diabetics. Considering the prevalence and complications of GDM, this module will serve as an essential step in health education and management of GDM. It was developed based on the interprofessional team's suggestions and recommendations.
Pregnancy is one of the noteworthy times in any woman's life, and it is also a stressful condition. The situation becomes even more fragile if the woman is diagnosed with GDM. Poorly controlled GDM is often associated with reduced quality of life.[26,27,28]
GDM patients require detailed information and education on the gestational diabetes pathophysiology, available treatment, and the condition's management. Self-monitoring blood sugar levels, maintaining adequate weight gain, planning meal intake, exercising, and avoiding possible complications of GDM are required.[29] The critical strategy of providing education during pregnancy is to gain sufficient knowledge and acquire skills for self-management of GDM. The module developed contains adequate information on managing GDM using a multi-professional approach. This module expects to fill this section's knowledge and practice gap among healthcare professionals.
There needs to be more than oral knowledge and skills in communication for an educational process. The printed educational materials, such as booklets, counseling, and communication shared by the consultant, effectively translate into patient education.[30] Hence, healthcare professionals can use the educational material developed through this study during counseling sessions with patients. Educational modules improve patient compliance with medical advice, motivate patients, enhance their quality of life, and lower healthcare expenses in our society.
The booklets used for health education must comply with basic requirements regarding content, the flow of information, layout, and illustrations.[31] Using simple language with appropriate charts, figures, and illustrations is vital while developing printed educational material.[32] The content in educational materials should have authentic information (evidence-based) and be reliable.[31,33] The module developed by this study has undergone validation for all the aspects mentioned. This booklet will give additional help as it contains comprehensive information on the self-management of GDM.
A similar study was conducted, which developed an educational manual for healthy pregnancy designed for women with GDM.[34] The feedback study on this showed high satisfaction among the patients. Even in this technological era, printed information can improve literacy on GDM and provide motivation and change in attitude toward the management of GDM, which will contribute to a decrease in morbidity and mortality associated with GDM for the mother and the fetus.
The use of technology and the transformation of information in the module into Web-based educational programs and applications will help disseminate remotely without physical contact between the patient and healthcare provider. Many studies have demonstrated the beneficial effect of such applications in GDM management.[35,36] However, these types of Web-based interventions might be challenging to understand by women with low computer literacy. Printed modules developed through this study will help overcome this barrier and provide cost-effective solutions in resource-poor settings for better management of GDM.
Many reviews have mentioned that the interprofessional collaborative approach is the guiding force for managing GDM, as patient adherence to treatment and proper educational interventions will favor better pregnancy outcomes.[37] An interprofessional team developed this educational module based on local requirements and evidence-based practices.
Limitations and recommendation
The primary limitation of the research is that it took place during the COVID-19 epidemic. Due to a patient shortfall, the module's acceptance among the intended audience of gestational diabetes is still to be determined. To accommodate larger people with varied literacy backgrounds, the English version of the educational material must be translated into a local language. For wider use, the module needs to be transformed into a Web-based application.
Conclusions
An interprofessional team developed this validated education module by integrating exercise, yoga, medicines, and nutrition therapy domains. The module was designed based on local requirements and evidence-based practices. This validated interprofessional health education module for managing GDM can be used by healthcare professionals during consultations with GDM patients.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
Acknowledgement
The work has been conducted and accomplished as a part completion of my fellowship at MAHE-FAIMER International Institute for Leadership in Interprofessional Education, Manipal Academy of Higher Education and Research, Manipal, Karnataka, India.
The author would like to thank the Director, Dr. Ciraj AM, and all the faculty at MAHE-FAIMER Institute, Manipal, Karnataka, India, for their guidance and constant support during the conduct of this study.
References
- 1.Metzger BE, Coustan DR. Summary and recommendations of the Fourth international workshop conference on gestational diabetes. The organising committee. Diabetes Care. 1998;21(Suppl 2):B161–7. [PubMed] [Google Scholar]
- 2.Guariguata L, Linnenkamp U, Beagley J, Whiting DR, Cho NH. Global estimates of the prevalence of hyperglycemia in pregnancy. Diabetes Res Clin Pract. 2014;103:176–85. doi: 10.1016/j.diabres.2013.11.003. [DOI] [PubMed] [Google Scholar]
- 3.International Diabetes Federation . Brussels: IDF; 2011. Policy Briefing: Diabetes in Pregnancy: Protecting Maternal Health. Available from: http://www.idf.org/diabetes . [Google Scholar]
- 4.Oakley LL, Namara A, Sahu B, Nadal IP, Ana Y, Coombe H, et al. Educational films for improving screening and self-management of gestational diabetes in India and Uganda (GUIDES): Study protocol for a cluster-randomised controlled trial. Trials. 2021;22:501. doi: 10.1186/s13063-021-05435-x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Nielsen KK, de Courten M, Kapur A. Health system and societal barriers for gestational diabetes mellitus (GDM) services - lessons from World Diabetes Foundation supported GDM projects. BMC Int Health Hum Rights. 2012;12:33. doi: 10.1186/1472-698X-12-33. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Utz B, De Brouwere V. “Why screen if we cannot follow-up and manage?” Challenges for gestational diabetes screening and management in low and lower-middle income countries: Results of a cross-sectional survey. BMC Pregnancy Childbirth. 2016;16:341. doi: 10.1186/s12884-016-1143-1. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Mahalakshmi MM, Bhavadharini B, Maheswari K, Anjana RM, Jebarani S, Ninov L, et al. Current practices in the diagnosis and management of gestational diabetes mellitus in India (WINGS-5) Indian J Endocrinol Metab. 2016;20:364–8. doi: 10.4103/2230-8210.180001. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Babu GR, Tejaswi B, Kalavathi M, Vatsala GM, Murthy GVS, Kinra S, et al. Assessment of screening practices for gestational hyperglycemia in public health facilities: A descriptive study in Bangalore, India. J Public Health Res. 2015;4:448. doi: 10.4081/jphr.2015.448. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Benjamin EM, Schneider MS, Hinchey KT. Implementing practice guidelines for diabetes care using problem-based learning. A prospective controlled trial using firm systems. Diabetes Care. 1999;22:1672–8. doi: 10.2337/diacare.22.10.1672. [DOI] [PubMed] [Google Scholar]
- 10.Jeffery RA, To MJ, Hayduk-Costa G, Cameron A, Taylor C, Van Zoost C, et al. Interventions to improve adherence to cardiovascular disease guidelines: A systematic review. BMC Fam Pract. 2015;16:147. doi: 10.1186/s12875-015-0341-7. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Carolan-Olah MC. Educational and intervention programmes for gestational diabetes mellitus (GDM) management: An integrative review. Collegian. 2016;23:103–14. doi: 10.1016/j.colegn.2015.01.001. [DOI] [PubMed] [Google Scholar]
- 12.Ghaffari F, Salsali M, Rahnavard Z, Parvizy S. Compliance with treatment regimen in women with gestational diabetes: Living with fear. Iran J Nurs Midwifery Res. 2014;19(Suppl 1):S103–11. [PMC free article] [PubMed] [Google Scholar]
- 13.Carolan M, Gill GK, Steele C. Women's experiences of factors that facilitate or inhibit gestational diabetes self-management. BMC Pregnancy Childbirth. 2012;12:99. doi: 10.1186/1471-2393-12-99. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Mohan V, Usha S, Uma R. Screening for gestational diabetes in India: Where do we stand? J Postgrad Med. 2015;61:151–4. doi: 10.4103/0022-3859.159302. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Balaji V, Balaji M, Anjalakshi C, Cynthia A, Arthi T, Seshiah V. Diagnosis of gestational diabetes mellitus in Asian-Indian women. Indian J Endocrinol Metab. 2011:187–90. doi: 10.4103/2230-8210.83403. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Pimouguet C, Le Goff M, Thiébaut R, Dartigues JF, Helmer C. Effectiveness of disease- management programs for improving diabetes care: A meta-analysis. Can Med Assoc J. 2011;183:E115–27. doi: 10.1503/cmaj.091786. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Li R, Zhang P, Barker LE, Chowdhury FM, Zhang X. Cost-effectiveness of interventions to prevent and control diabetes mellitus: A systematic review. Diabetes Care. 2010;33:1872–94. doi: 10.2337/dc10-0843. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Castro MS, Pilger D, Fuchs FD, Ferreira MB. Development and validity of a method for the evaluation of printed education material. Pharm Pract (Granada) 2007;5:89–94. doi: 10.4321/s1886-36552007000200007. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Zamanzadeh V, Ghahramanian A, Rassouli M, Abbaszadeh A, Alavi-Majd H, Nikanfar A. Design and implementation content validity study: Development of an instrument for measuring patient-centered communication. J Caring Sci. 2015;4:165–78. doi: 10.15171/jcs.2015.017. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Parmenter K, Wardle J. Evaluation and design of nutrition knowledge measures. J Nutr Educ. 2000;32:269–77. [Google Scholar]
- 21.Grant JS, Davis LL. Selection and use of content experts for instrument development. Res Nurs Health. 1997;20:269–74. doi: 10.1002/(sici)1098-240x(199706)20:3<269::aid-nur9>3.0.co;2-g. [DOI] [PubMed] [Google Scholar]
- 22.Lynn MR. Determination and quantification of content validity. Nurs Res. 1986;35:382–5. [PubMed] [Google Scholar]
- 23.Davis LL. Instrument review: Getting the most from a panel of experts. Appl Nurs Res. 1992;5:194–7. [Google Scholar]
- 24.Abdollahpour E, Nejat S, Nourozian M, Majdzadeh R. The process of content validity in instrument development. Iran Epidemiol. 2010;6:66–74. [Google Scholar]
- 25.Teles LM, Oliveira AS, Campos FC, Lima TM, da Costa CC, de Souza Gomes LF, et al. Construcao e validacao de manual educativo para acompanhantes durante o trabalho de parto e parto. Rev Esc Enferm Usp. 2014;48:977–84. doi: 10.1590/S0080-623420140000700003. [DOI] [PubMed] [Google Scholar]
- 26.Rosenstein MG, Cheng YW, Snowden JM, Nicholson JM, Doss AE, Caughey AB. The risk of stillbirth and infant death stratified by gestational age in women with gestational diabetes. Am J Obstet Gynecol. 2012;206:1–309. doi: 10.1016/j.ajog.2012.01.014. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27.Devlieger R, Casteels K, Van Assche FA. Reduced adaptation of the pancreatic B cells during pregnancy is the major causal factor for gestational diabetes: Current knowledge and metabolic effects on the offspring. Acta Obstet Gynecol Scand. 2008;87:1266–70. doi: 10.1080/00016340802443863. [DOI] [PubMed] [Google Scholar]
- 28.Murphy MS, Fell DB, Sprague AE, Corsi DJ, Dougan S, Dunn SI, et al. Data resource profile: Better outcomes registry & network (BORN) Ontario. Int J Epidemiol. 2021;50:1416–7h. doi: 10.1093/ije/dyab033. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29.Goldschmidt VJ, Colletta B. The challenges of providing diabetes education in resource-limited settings to women with diabetes in pregnancy: Perspectives of an educator. Diabetes Spectr 2. 0161;29:101–4. doi: 10.2337/diaspect.29.2.101. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 30.Wizowski L, Harper T, Hutchings T. 4th. Hamilton Health Sciences; 2008. Writing Health Information for Patients and Families: A Guide to Creating Patient Education Materials that are Easy to Read, Understand and Use. [Google Scholar]
- 31.Hoffmann T, Worrall L. Designing effective written health education materials: Considerations for health professionals. Disabil Rehabil. 2004;7:1166–73. doi: 10.1080/09638280410001724816. [DOI] [PubMed] [Google Scholar]
- 32.Lebanova H, Getov I. Adapted methodology for development and evaluation of patients’ educational materials for pharmacovigilance. Academia. 2013;3:35–7. [Google Scholar]
- 33.Oliveira SC, Lopes MV, Fernandes AF. Development and validation of an educational booklet for healthy eating during pregnancy. Rev Lat Am Enfermagem. 2014;22:611–20. doi: 10.1590/0104-1169.3313.2459. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 34.Staynova RA, Gueorguiev SR, Petkova-Gueorguieva ES, Vasileva EV, Stoimenova AH, Yanatchkova VE, et al. Written health education materials for women with gestational diabetes mellitus-evaluation of usefulness and patients’ satisfaction. Folia Med. 2019;31:127–33. doi: 10.2478/folmed-2018-0041. [DOI] [PubMed] [Google Scholar]
- 35.Xie W, Dai P, Qin Y, Wu M, Yang B, Yu X. Effectiveness of telemedicine for pregnant women with gestational diabetes mellitus: An updated meta- analysis of 32 randomized controlled trials with trial sequential analysis. BMC Pregnancy Childbirth. 2020;20:198. doi: 10.1186/s12884-020-02892-1. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 36.Sayakhot P, Carolan-Olah M, Steele C. Use of a web-based educational intervention to improve knowledge of healthy diet and lifestyle in women with gestational diabetes mellitus compared to standard clinic-based education. BMC Pregnancy Childbirth. 2016;16:208. doi: 10.1186/s12884-016-0996-7. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 37.Morampudi S, Balasubramanian G, Gowda A, Zomorodi B, Patil AS. The challenges and recommendations for gestational diabetes mellitus care in India: A review. Front Endocrinol (Lausanne) 2017;24:56. doi: 10.3389/fendo.2017.00056. [DOI] [PMC free article] [PubMed] [Google Scholar]