

Abstract
BACKGROUND:
Specialist nurses need to have an accurate understanding of colostomy care-related concepts to provide care. Although patients with different types of ostomy have different types of needs, terms such as ostomy care, colostomy care, and ileostomy nursing are interchangeably used. Moreover, there are limited concept analysis studies into the concept of colostomy nursing care (CNC) in ostomy care centers (OCCs). The aim of this study was to analyze and clarify the concept of CNC in outpatient OCCs.
METHODS AND MATERIAL:
This was a concept analysis study. This concept analysis was conducted using Walker and Avant's eight-step method. The online databases were searched until 2022 to retrieve documents on CNC. Finally, 35 articles and four books were included in the analysis, the defining attributes, antecedents, and consequences of the concepts were determined, and model and additional cases as well as empirical referents were presented.
RESULTS:
The defining attributes of CNC in OCCs are the development of professional role, participatory practice and interdisciplinary care, selection of the best clinical procedures, care based on patient education, and patient rehabilitation. The antecedents of the concept are nurse-related antecedents, patient- and family-related antecedents, environmental antecedents, and professional rules and regulations. Its consequences are patients’ and families’ greater care-related knowledge, improvement of nurses’ care quality, patient autonomy, and self-efficacy.
CONCLUSION:
The concept of CNC in OCCs can be defined as “a continuous and coherent care based on knowledge, skill, expertise, experience, and colostomy type which uses interdisciplinary collaboration and the best available evidence in order to select and provide the best services according to patients’ and families’ culture and background, fulfill patients’ physical, mental, sexual, social, and spiritual needs, and timely refer patients to specialists, with the ultimate goal of improving patient autonomy and facilitating their return to normal life.”
Keywords: Colostomy, concept analysis, nursing theories, ostomies
Introduction
A colostomy is one of the most common surgical modalities for the management of the obstructive or malignant problems of the colon. It can be made at the ascending, descending, transverse, or sigmoid colon depending on the underlying problem to allow stool evacuation through an opening to the abdominal wall.[1,2] After the colostomy surgery, patients are discharged from the hospital and receive colostomy nursing care (CNC) from specialist stoma care nurses (SCNs) in home or outpatient settings. SCNs, as members of the professional ostomy care team, are responsible for the management of patients with colostomy in both inpatient and outpatient settings.[3,4,5,6] In outpatient ostomy care centers (OCCs), SCNs should comprehensively assess patients with colostomy, determine care-related goals, and implement appropriate care measures based on the goals.
The results of research on the concept of CNC allow nurses and the ostomy team to provide care based on evidence-based practice and provide basic education for ostomates and their families. Professional nursing care in ostomy centers can reduce workload in hospital wards, reduce the waiting time for receiving care, ensure healthcare providers of treatment effectiveness,[5,7,8,9] improve patients’ access to the necessary educational materials, and help effectively fulfill their different needs.[10] However, noncontinuous care to ostomates can increase the caregiver burden on family members and reduce the quality of life of patients and their family members.[11,12,13]
According to the United Ostomy Associations of America, more than 750000 Americans currently have an ostomy, of which 36% of them have colostomy.[14] Moreover, there are more than 700000 patients with an ostomy in Europe.[15,16] The number of patients with an ostomy is 70000 in Canada.[17] In Asian countries like India, more than 50,000 patients undergo colostomy, and most of them are referred from peripheral centers.[18] The number of patients with an ostomy in Iran is also around 30000, with 70% of them having a colostomy.[19]
Different studies have so far been conducted in CNC. For example, a study showed that the most basic principles of ostomy care were prevention and management of ostomy complications, lifestyle education to patients, and nurses’ adequate knowledge about colostomy care equipment.[1] Another study highlighted that SCNs in OCCs can empower patients for self-care by providing them with strong support and quality education and improving their own knowledge about the appropriate use of ostomy care equipment.[2] A qualitative study reported that nurses’ great experience in providing hospital care to patients with an ostomy, high educational level, and good specialized ostomy care knowledge are antecedent ostomy nursing care.[20] Some studies also showed that the aims of ostomy care in outpatient OCCs are to reduce ostomy-related problems and complications, improve patients’ self-care abilities, and empower patients to return to normal life.[3,21,22]
An essential prerequisite to quality CNC is a clear understanding of the concept of CNC and its attributes, antecedents, and consequences. Given the significant shifts in healthcare provision approaches, such as the wider use of outpatient care services for patients with colostomy, and patients’ greater desire to receive continuous care after hospital discharge, CNC provision in outpatient OCCs is turning into a common colostomy care approach.[23,24,25,26,27] Therefore, careful exploration of the concept of CNC in outpatient OCCs is essential to determine its components, attributes, antecedents, and consequences. Previous studies into ostomy care highlighted two important points. First, SCNs are on the frontline of ostomy care in OCCs and have a key role in care provision to patients with colostomy, but they do not consider themselves responsible for colostomy care due to their limited knowledge about their roles, which roots in ambiguities in the concept of CNC.[28,29,30] Second, expressions such as ostomy care, colostomy care, and ileostomy nursing are interchangeably used, while patients with each type of ostomy have unique needs and all of them need long-term care and specific attention.[31] Nonetheless, to the best of our knowledge, there is no specific concept analysis study on the concept of CNC.[32] Therefore, this study was conducted to reduce this gap. The aim of this study was to analyze and clarify the concept of CNC in OCCs.
Study design and setting
This concept analysis was conducted using Walker and Avant's method. Walker and Avant modified Wilson's thirteen-step method of concept analysis into an eight-step approach that is easier to understand and use for novice researchers and enables them to systematically assess independent concepts.[33] The main goal of this method is to distinguish between the determining and irrelevant attributes of a concept.[34] This method can be used to clarify a concept through its simplification.[35] The eight steps of this method are the selection of a concept, determination of the aims or purposes of analysis, identification of all uses of the concept, determination of its defining attributes, construction of a model case, construction of borderline, related, and contrary cases, identification of antecedents and consequences, and definition of empirical referents.[36] During data analysis, excerpts from the data that were relevant to the concept of CNC in OCCs were identified and coded, and thereby, the defining attributes, antecedents, and consequences of the concepts were determined and model, borderline, related, and contrary cases and empirical referents were presented. Defining attributes are the characteristics of a concept, which frequently appear and differentiate it from similar concepts.[36]
Data collection tool and technique
Initially, a literature search was performed in the Cumulated Index to Nursing and Allied Health Literature (CINAHL), MEDLINE (MED), Web of Science, Google Scholar, ProQuest, PubMed, Scopus, Embase, and Ovid online databases to retrieve documents on CNC, and the Oxford dictionary was searched until 2022 for the definitions of the concept. Examples of search keywords for database search were ostomy nursing care, colostomy nursing, and ileostomy nursing.
Study participants and sampling
Given the diversity of documents on ostomy care, we only included documents on CNC in the study. After the omission of repetitive and irrelevant records, 346 articles and five books were assessed, and finally, 35 articles and four books were included in the final analysis [Figure 1].
Figure 1.
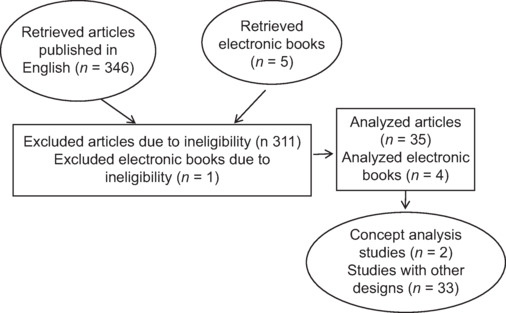
Flow diagram of the study
Ethical consideration
This concept analysis was exempt from the Institutional Review Board approval; the research did not involve human subjects.
Concept selection
In concept analysis, a concept should be selected with care and previous interest.[36,37] CNC is an important concept because quality CNC provision in OCCs can be associated with positive outcomes for patients and healthcare systems, reduce patients’ unessential attendance at care centers, shorten their waiting time to receive care services, ensure physicians and other healthcare providers of treatment appropriateness, and decrease colostomy care costs. However, CNC in specialized OCCs has different dimensions and understanding these dimensions is rather difficult. Moreover, previous studies into CNC mostly focused on short-term and routine CNC provision in hospital settings, paid little attention, if any, to CNC provision in OCCs,[38] and did not provide a clear and precise definition of the CNC concept.[5,39,40,41] Therefore, the concept of CNC in OCCs was selected for further clarification and analysis in the present study.
Aims or purposes of analysis
Concept analysis clarifies ambiguous and complex concepts, differentiates a concept from similar ones, and provides a basis for concept development.[36] The CNC concept is a concept that is interchangeably used with concepts such as ostomy care, colostomy care, and ileostomy nursing. Moreover, there is no differentiation between short-term inpatient CNC and long-term outpatient CNC, while the latter has different dimensions and its clarification can improve nurses’ understanding of it and facilitate its further development.
Results
Uses of the concept
Walker and Avant argue that the uses of a concept refer to all aspects of its application in all fields of study beyond nursing and medicine because understanding a concept in a given field of study may cause biases in its understanding in other fields. Therefore, a preliminary step in determining the uses of a concept is to depict a general illustration of it.[36]
As there was no clear and precise definition of CNC in the literature, we assessed the definitions of colostomy, ostomy nursing care, and community-based ostomy care.
The term ostomy derives from the Greek term “stoma,” which means mouth or opening. Ostomy is a surgically made opening to deviate stool, urine, cerebrospinal fluid, or tracheal airflow from their normal routes.[2] Taber's Medical Dictionary defines colostomy as “the opening of a portion of the colon through the abdominal wall to its skin surface” and notes that colostomy can be made into the ascending, descending, transverse, or sigmoid colon.[42] According to the World Council of Enterostomal Therapy, an ostomy care nurse is a registered nurse with a history of participation in an educational program recognized by the council or nurses’ national professional society and defines ostomy nursing care as the prevention and management of ostomy complications and maximization of patients’ physiological and psychosocial adaptation by ostomy care nurses.[29] In medicine, ostomy care refers to ostomy management by a nurse since the time of surgical ostomy creation to maintain skin and mental health and improve knowledge about ostomy management.[43] In the nursing literature, ostomy care is defined as specialist SCNs’ support for patients with an ostomy through patient education and empowerment.[2] Ostomy nursing is also considered specialized and independent care provision to patients with an ostomy to facilitate their living with their new conditions.[20,44]
Ostomy care after hospital discharge is considered as a type of community-based nursing[1,45,46] and is defined as dietary modification and protective measures to prevent or manage ostomy complications such as trauma to the stoma, problems related to ostomy bag changing, and injury to the ostomy tissues.[47] Another definition considers community-based ostomy care as nurses’ physical, mental, spiritual, and social support for patients with an ostomy to improve their adaptation to their new life conditions. These definitions consider home and clinical settings as the sites of CNC[1,45] and trained nurses or ostomy therapists as ostomy care providers.[43]
Defining attributes of the concept
The determination of defining attributes is the core of concept analysis. In concept analysis, the most relevant defining attributes are determined to provide a deeper insight into the intended concept. This step helps differentiate the intended concept from similar or relevant concepts.[36,48] According to the ostomy care standards of the International Ostomy Association, the defining attributes of CNC in OCCs are the development of a professional role, participatory practice and interdisciplinary care, selection of the best clinical procedures, care based on patient education, and patient rehabilitation.[2,49,50,51]
Development of professional role: Nurses should promote their specialized skills, perform research studies that are appropriate for their clinical settings, implement their care measures based on clinical policies and rules, participate in clinical decision-making, adhere to the ethical principles of ostomy care, participate in financial supporting programs for patients, and have adequate knowledge about the theories and research studies on ostomy care.[39,49]
Participatory practice and interdisciplinary care: This attribute pertains to nurses' skills for communication with patients and other healthcare team members. Communication of team members with each other is one of the most important requirements of the ostomy rehabilitation process. Nurses ‘communication with other members of team helps to be aware of patients’ progress. It holds that nurses should establish and maintain good therapeutic relationship with patients based on their culture and beliefs, respect their privacy, establish professional communications with other healthcare team members to fulfill patients' needs, timely refer patients to other healthcare specialists, and act as a trainer and counselor for novice healthcare providers.[39,42,49,52,53]
Selection of the best clinical procedures: This refers to nurses’ practice based on scientific resources and highlights that nurses should continuously assess patients based on scientific methods, assess stressors and patients’ and families’ coping mechanisms, assess patients’ and families’ sources of support, collect patient data from different sources, timely refer patients to specialists, and appropriately collect documents related to long-term patient care.[1,49,52,54]
Care based on patient education and rehabilitation: Nurses should assess the necessary resources to create a learning environment, select the best educational method for each patient or family, provide lifestyle-related education based on colostomy type, consider patients’ and families’ religious beliefs during the process of education, and collaborate with healthcare authorities in developing public education programs.[5,49,52]
Patient rehabilitation: The rehabilitation of patients with colostomy largely depends on maintaining care continuity and procuring colostomy care equipment. Nurses need to regularly assess patients and their needs through regular home visits during the first three months after hospital discharge and then through telephone contacts or during patient attendance at OCCs. Moreover, they need to provide continuous psychological support to patients respecting their sexual and body image concerns, perform specialized assessment of colostomy conditions and colostomy care equipment, and provide multidimensional support to patients [Table 1].[1,52,55,56,57]
Table 1.
Attributes, antecedents, and consequences of colostomy nursing care in ostomy care centers
| Results | Titles | Details |
|---|---|---|
| Antecedents | Nurse-related antecedents | 6 Cs of nursing, nursing degree Specialized knowledge and skills, experience in care for patients with an ostomy, participate in conducting research studies |
| Patient- and family-related antecedents | Courage, adequate knowledge about colostomy care after hospital discharge | |
| Environmental antecedents | Easy access to colostomy care equipment and centers, communication with peers, financial support of patients by the healthcare system, supportive work environment for nurses, adequate nursing staff | |
| Professional rules and regulations | Written rules and regulations, adequate knowledge about patients' rights, recognition of patients' cultures, traditions, and beliefs Adherence to the ethical principles of care Respect for patient privacy Availability of nursing theories Implementation of regular educational programs |
|
| Attributes of the concept | Development of professional role | Promote their specialized skills Perform research studies Implement their care measures based on clinical policies and rules Participate in clinical decision-making The ethical principles of ostomy care Participate in financial supporting programs Adequate knowledge about the theories and research studies |
| Participatory practice and interdisciplinary care | Therapeutic relationship with patients based on their culture Respect patient privacy professional Communications with team members Timely refer patients to healthcare specialists Act as a trainer and counselor for novice nurses |
|
| Selection of the best clinical procedures | Assess patients based on scientific methods Assess stressors and patients' and families' coping mechanisms Assess patients' and families' sources of support Collect patient data from different sources Timely refer patients to specialists Collect the documents related to long-term care |
|
| Care based on patient education | Assess the necessary resources Select the best educational method for each patient or family Provide lifestyle-related education based on Colostomy type Consider patients' and families' religious beliefs during education Collaborate with healthcare authorities in developing public education |
|
| Patient rehabilitation | Regularly assess patients and their needs through regular home visits, telephone contacts, or during patient attendance at OCCs. Psychological support to patients respecting their sexual and body image concerns Specialized assessment of colostomy conditions and colostomy care equipment Multidimensional support to patients |
|
| Consequences (return to a creative lifestyle, patient autonomy, and patient self-efficacy) | Provision of quality patient education | Improves patients' understanding of their diseases Behavior modification independent care-related decisions Improves patients' technical skills |
| Reduce physical complications | Prevent rehospitalization Reduce hospitalization-related costs |
|
| Reduce social consequences | Patients' lower stress over engagement in social activities Greater productivity at work Better organization of daily activities Effective adaptation to social life |
|
| Reduce psychological consequences | Sense of support Lower stress Easier recovery Higher quality of life Improvement of the mental and financial status of the family |
|
| Nursing-related consequences | Patients' and families' trust in SCNs Patient satisfaction with CNC services Reduced workload of nurses |
Construction of a model case
The model case is an example of using the intended concept that shows all of its defining attributes. In other words, it is “a pure case of the concept, a paradigmatic example, or a pure exemplar.”[36,58]
Mr. A. is seventy years old, has descending colostomy for eight months due to colorectal cancer, and lives with his wife. When he refers to the OCC, Mrs. D., an ostomy care nurse, notices stoma prolapse during examination. During medical history taking, she finds that the patient has inappropriate dietary regimen and physical activity, suffers from chronic constipation most of the time, carries heavy things during daily shopping, and performs intense exercises during physical exercise that put strain on the ostomy. Moreover, his wife cannot help him change the colostomy bag and he individually changes it while he has inadequate skills for colostomy bag changing due to old age and hence, cuts the ostomy hole larger than the stoma, leading to skin lesions around the stoma. Accordingly, Mrs. D. holds a session with Mr. A. and his wife and child to provide them with education about appropriate dietary regimen and physical activity, colostomy care, and colostomy bag changing, uses modern dressing for the lesions, plans for patient's regular attendance at the ostomy care center, and emphasizes that dressing and colostomy bag should be changed exclusively by an SCN until the healing of the skin lesions. Moreover, she provides them with education about the best colostomy bag type and the appropriate colostomy bag hole size, recommends ostomy-specific belts to prevent further complications, and informs them where they can access such belts. In the next visits, she notices the healing of the lesions and the persistence of the prolapse. Therefore, she contacts the surgeon and refers Mr. A. to the surgeon. Mr. A. and his wife are concerned with the need for another surgery and their children's awareness of his problems. Thus, Mrs. D. listens to their concerns, attempts to support them through providing them with counseling services, and ensures them of the confidentiality of their data.
In this case, the nurse was able to establish timely nursing diagnoses and prevent the progress of the complications due to her adequate ostomy-related knowledge and experience. She also continuously assessed the patient and made an appropriate decision to refer the patient to the surgeon. Moreover, she did not limit patient care to physical care and provided multidimensional (physical, mental, and financial) care to the patient. She provided evidence-based care through modern dressing. Her contact with the surgeon also indicates that she had good interprofessional communication. She also provided patient and family education, attracted family support for the patient, and considered ethical principles in her practice.
Examining additional cases
Construction of a borderline case
The borderline case is a case that shows most but not all defining attributes of the intended concept. It may include most or even all attributes but differ from the model case in the intensity or the duration of the attributes.[36,58]
In the OCC, an ostomy care nurse provides education about wound care and bag changing to a patient with second degree stoma skin wound, uses modern dressing for wound management, reduces patient's concerns about wound healing through talking to him and providing counseling services, ensures him of the confidentiality of his data, and refers him to the surgeon. However, she does not provide any information about when to refer to the center and delegates care to the patient without any virtual or in-person follow-up contact.
In this model, the nurse provided evidence-based colostomy care, patient education, and psychological and financial support, considered ethical principles in colostomy care, and referred the patient to the appropriate specialist, but did not follow the patient, did not determine the time for next visits, and was unaware of the process of wound healing.
Construction of a related case
A related case does not have the defining attributes of the intended concept but is similar to the concept and this similarity causes confusion or errors in the definition of the concept.[36,59]
The husband of Mrs. M. sadly refers to the OCC. The nurse asks him about the reason for his sadness and he explains that colostomy bags are very expensive and their insurance organization does not cover this expense. Therefore, he attends the center to receive bags and asks the nurse to give him several bags. After listening to his words, the nurse provides him with education about how to buy bags, talks to the manager of the center, and provides him with several colostomy bags.
In this case, the nurse provided financial support and several colostomy bags to the patient and his husband. Although financial support is related to the concept of CNC, this model does not have all defining attributes of the concept. However, the provision of colostomy bag is not among the responsibilities of SCNs.
Construction of a contrary case
A contrary case is a clear example of what the concept is not.[36,59]
Mrs. J. is 55 years old and has transverse colostomy. She refers to the OCC for the first time with her husband and daughter. The ostomy care nurse asks her to refer to the examination room, remove her colostomy bag, and lie down on the examination bed. During examination, room door is open and another patient who is in the waiting saloon sees the examination process and gets out of the center. On the other hand, Mrs. J. feels ashamed and the nurse says that this process is normal and asks her not to get worried. Moreover, when Mrs. J. asks the nurse to provide her with education about colostomy bag changing, the nurse says that she should rapidly change the bag due to her heavy workload and the bad smell of the colostomy.
In this case, the nurse did not protect patient privacy, openly exposed the patient, reminded the patient of the bad smell of the colostomy, and, thereby, damaged patient's self-confidence. Moreover, she ignored patient education, which is one of the main components of colostomy care, ignored patient request, and just provided routine care.
Identifying antecedents and consequences
Antecedents
Antecedents are events or incidents that should be available before the occurrence of the intended concept.[36] Colostomy care in specialized OCCs is provided to patients and families by specialist nurses. Therefore, its antecedents are nurse-related antecedents, patient- and family-related antecedents, environmental antecedents, and professional rules and regulations.
Nurse-related antecedents: These antecedents include adherence to the 6 Cs of nursing, namely continuous care provision, compassion, courage, communication, commitment, and competence.[1,60] Moreover, SCNs need to have bachelor's or master's nursing degree, have specialized knowledge and skills respecting colostomy care,[1,20,44,49,56,61,62] use the nursing process,[63] have great experience in care provision to patients with an ostomy, and participate in conducting research studies.[20,49]
Patient- and family-related antecedents: These antecedents include family support for patients, patients’ personal characteristics such as courage,[57,64] and adequate knowledge about colostomy care after hospital discharge [Table 1].[65,66,67]
Environmental antecedents: Examples of these antecedents are easy access to colostomy care equipment and centers, communication with peers,[67,68] financial support of patients by the healthcare system,[69] supportive work environment for nurses, and adequate nursing staff.[70,71]
Professional rules and regulations: These antecedents include written rules and regulations,[52,72] adequate knowledge about patients’ rights, recognition of patients’ cultures, traditions, and beliefs, adherence to the ethical principles of care, respect for patient privacy,[49,73,74] availability of nursing theories for colostomy care,[64] and implementation of regular educational programs.[14,75]
Consequences
Consequences are events that happen after the occurrence of the intended concept.[36] The most important consequences of the concept of CNC include return to a creative lifestyle, patient autonomy, and patient self-efficacy.[3,21,22] Provision of quality patient education about colostomy care improves patients’ understanding of their diseases, facilitates their behavior modification, and enables them to make independent care-related decisions. It also improves patients’ technical skills for skin and wound care, incontinence management, colostomy bag changing, and dressing changing. CNC can also reduce physical complications of colostomy, prevent rehospitalization, and reduce hospitalization-related costs.[3,21,22,45,63] The social consequences of CNC include patients’ lower stress and concern over engagement in social activities, greater productivity at work, better organization of daily activities, and more effective adaptation to social life.[20,63,67,76,77] CNC also has psychological consequences for patients, including sense of support, lower stress, easier recovery, higher quality of life, and improvement of the mental and financial status of the family.[8,57,67] Nursing-related consequences of CNC also include patients’ and families’ trust in SCNs, their satisfaction with CNC services, and reduced workload of nurses [Table 1].[78,79]
Empirical referents
Empirical referents help measure the intended concept or determine its existence in the real world.[36] They are a series of actual phenomena whose existence indicates the occurrence of the intended concept. They are not simple instruments for measurement; rather, they are instruments that can be used to determine or measure the defining attributes of the concept. Therefore, empirical referents are directly related to the defining attributes of a concept rather than the whole concept.[36] Instruments for the measurement of the defining attributes of the CNC concept are the long-term/lifetime specialist SCN support, the short-term follow-up care by a specialist SCN (up to three months), and patient/family/carer satisfaction audit.[56]
Discussion
This study analyzed the concept of CNC in OCCs, determined its defining attributes, antecedents, and consequences, and defined its empirical referents. The results of this study consider education-based care as the main attribute of CNC in specialized care centers. In this regard in various studies, the British Nursing Association and the International Ostomy Association state that after hospital discharge, most patients with an ostomy experience nonacceptance of ostomy due to their limited knowledge about their diseases and ostomy care, and hence, education and counseling about living with an ostomy should immediately be provided to them and their families. Otherwise, they may experience different familial and social problems.[49,52] For this reason, the main goal of the nurse is the patient's self-efficacy through education.
The results of this study showed that the rehabilitation of patients with colostomy is intertwined with the other attributes of CNC. In this regard, the International Ostomy Association states in various studies that maintaining care continuity and developing a schedule for care provision are among the principal attributes of nursing care in specialized care centers. To maintain care continuity, nurses should get ensured that after their first attendance at OCCs, patients will have easy access to nursing support and counseling services and nurses will monitor their conditions online.[49,56] This common feature in all studies can be due to the patients’ need for long-term care to achieve independence in life activities.
According to the results of this study, the nurse's specialized knowledge is a prerequisite for proper care of colostomy patients and correct use of ostomy equipment, However, the nurse specialized knowledge as the antecedents for care is different from the development of knowledge, which is the care attributes. In this regard, a study highlighted that using appropriate equipment based on the type of colostomy and secretions is an inseparable component of colostomy care, and hence, nurses should have adequate knowledge about colostomy care equipment and how to use it implicitly to appropriately use it for their patients and thereby win the patient's trust and protect the stoma and its surrounding skin against potential injuries.[47] For comprehensive and optimal care, they need to update their information during care, which is proposed as care attributes.
The results of the study showed that the colostomy care attributes in ostomy centers are interconnected and cannot be considered separately from each other. In this regard, a study reported that given the high risk of colostomy complications, referral of patients with colostomy to other specialists is among the main attributes of CNC, and hence, SCNs should have effective communication and collaboration with other members of the ostomy care team (including social worker, occupational therapist, physiotherapist, and clinical psychologist) and facilitate their interprofessional communication.[56] A review study also showed that CNC is a multidimensional and comprehensive care and nurses who provide care to patients with colostomy are expected to value mental, sexual, social, and spiritual patient support as much as physical support and provide their services based on patients’ needs to facilitate their adaptation.[80] Nurses can develop their professional role in CNC through evidence-based practice and clinical governance policies.[49] Moreover, the observance of all defining attributes of the CNC concept depends on close adherence to ethical principles. Therefore, colostomy care nurses need to modify their professional roles based on ethical principles and the standards of ostomy associations.[49]
Respecting the antecedents of the concept of CNC, two studies reported clinical knowledge, skills, and experience as significant antecedents of CNC in OCCs, highlighted that these antecedents can improve patient safety and satisfaction, and, hence, recommended the implementation of specialized educational courses, particularly for novice nurses.[20,61] Family support, as another significant antecedent of CNC, can also improve patients’ self-care behaviors and autonomy and lead to positive outcomes for families, nurses, and healthcare systems.[81,82] These imply that the absence of the antecedents of CNC can be associated with challenges in quality CNC provision and negatively affect its outcomes.
Limitations and recommendation
We had limited access to some online databases and, hence, might have missed some potentially eligible studies. Given the challenges of CNC provision in inpatient settings, concept analysis through the hybrid model is recommended to provide clearer understanding of the CNC concept. The proposed definition in this article is used to guide research that aims to understand the meanings and experiences related to the phenomenon of CNC in ostomy centers.
Conclusion
Based on the findings of this study, the concept of CNC in OCCs can be defined as “a continuous and coherent care based on knowledge, skill, expertise, experience, and colostomy type which uses interdisciplinary collaboration and the best available evidence in order to select and provide the best services according to patients’ and families’ culture and background, fulfill patients’ physical, mental, sexual, social, and spiritual needs, and timely refer patients to specialists, with the ultimate goal of improving patient autonomy and facilitating their return to normal life.”
Financial support and sponsorship
Nil.
Conflicts of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as potential conflicts of interest.
Acknowledgement
This article was derived from the PhD dissertation in nursing. The authors are very thankful to all the participants for their valuable contribution.
References
- 1.Palmer SJ. Overview of stoma care for community nurses. Br J Community Nurs. 2020;25:340–4. doi: 10.12968/bjcn.2020.25.7.340. [DOI] [PubMed] [Google Scholar]
- 2.Bradshaw E, Collins B. Managing a colostomy or ileostomy in community nursing practice. Br J Community Nurs. 2008;13:514–8. doi: 10.12968/bjcn.2008.13.11.31523. [DOI] [PubMed] [Google Scholar]
- 3.Santos RdP, Fava SMCL, Dázio EMR. Self-care of elderly people with ostomy by colorectal cancer. J Coloproctol (Rio J Impr) 2019;39:265–73. [Google Scholar]
- 4.Kirkland-Kyhn H, Martin S, Zaratkiewicz S, Whitmore M, Young HM. Ostomy care at home. Am J Nurs. 2018;118:63–8. doi: 10.1097/01.NAJ.0000532079.49501.ce. [DOI] [PubMed] [Google Scholar]
- 5.Appleby SL. Role of the wound ostomy continence nurse in the home care setting: A patient case study. Home Healthc Now. 2011;29:169–77. doi: 10.1097/NHH.0b013e3181fe438b. [DOI] [PubMed] [Google Scholar]
- 6.Subcommittee, W.C.P.W. Ankle brachial index: Quick reference guide for clinicians. Journal of wound, ostomy, and continence nursing: official publication of The Wound. Ostomy and Continence Nurses Society. 2012;39(2 Suppl):S21–S29. doi: 10.1097/WON.0b013e3182478dde. [DOI] [PubMed] [Google Scholar]
- 7.Sierko E, Werpachowska MT, Sokół M, Wojtukiewicz MZ. Quality of nursing care of colorectal cancer patients undergoing first line palliative chemotherapy—A questionnaire study in a single institution in Poland. Adv Palliative Med. 2011;10:65–72. [Google Scholar]
- 8.Ferreira-Umpiérrez A, Fort-Fort Z. Experiences of family members of patients with colostomies and expectations about professional intervention. Rev Lat Am Enfermagem. 2014;22:241–7. doi: 10.1590/0104-1169.3247.2408. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.LeSeure P, Chongkham-Ang S. The experience of caregivers living with cancer patients: A systematic review and meta-synthesis. J Pers Med. 2015;5:406–39. doi: 10.3390/jpm5040406. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Richbourg L, Thorpe JM, Rapp CG. Difficulties experienced by the ostomate after hospital discharge. J Wound Ostomy Continence Nurs. 2007;34:70–9. doi: 10.1097/00152192-200701000-00011. [DOI] [PubMed] [Google Scholar]
- 11.Erlingsson CL, Magnusson L, Hanson E. Family caregivers’ health in connection with providing care. Qual Health Res. 2012;22:640–55. doi: 10.1177/1049732311431247. [DOI] [PubMed] [Google Scholar]
- 12.Sujianto U, Billy R, Margawati A. Family's experience: Nursing care for colorectal cancer patients with colostomy. Nurse Media J Nurs. 2020;10:96–106. [Google Scholar]
- 13.Mosher CE, Adams RN, Helft PR, O’Neil BH, Shahda S, Rattray NA, et al. Family caregiving challenges in advanced colorectal cancer: Patient and caregiver perspectives. Support Care Cancer. 2016;24:2017–24. doi: 10.1007/s00520-015-2995-z. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Abd El-latief Shahat Ali H, Ali JS, Taha SH. Effect of educational program on nurses performance about colostomy care. Minia Scientific Nurs J. 2020;8:103–10. [Google Scholar]
- 15.Hubbard G, Beeken RJ, Taylor C, Watson AJM, Munro J, Goodman W. A physical activity intervention to improve the quality of life of patients with a stoma: A feasibility study protocol. Pilot Feasibility Stud. 2019;5:1–8. doi: 10.1186/s40814-019-0461-2. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Goodman W, Downing A, Allsop M, Munro J, Taylor C, Hubbard G, et al. Quality of life profiles and their association with clinical and demographic characteristics and physical activity in people with a stoma: A latent profile analysis. Qual Life Res. 2022;31:2435–44. doi: 10.1007/s11136-022-03102-5. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Ostomy Canada Society. 2020 Available from: https://www.ostomycanada.ca . [Google Scholar]
- 18.Davis D, Ramamoorthy L, Pottakkat B. Impact of stoma on lifestyle and health-related quality of life in patients living with stoma: A cross-sectional study. J Educ Health Promot. 2020;9:328. doi: 10.4103/jehp.jehp_256_20. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Parchami M, Ahmadi Z. Effect of telephone counselling (telenursing) on the quality of life of the patients with colostomy. J Client Centered Nurs Care. 2016;2:123–30. [Google Scholar]
- 20.Alenezi A, Kimpton A, McGarth I, Livesay K. Confidence, skills and barriers to ostomy patient care by nursing staff in Saudi Arabia. Nurs Forum. 2022;57:403–11. doi: 10.1111/nuf.12701. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Bagheri M, Sharifan P, Behboudi Far A, Pouresmall Z, Kavousi F. Nurses’ knowledge about fecal intestinal Ostomies's care: A cross-sectional study. Jundishapur J Chronic Dis Care. 2017;6:e43345. [Google Scholar]
- 22.Colwell JC, Goldberg MT, Carmel JE. Missouri: Elsevier Health Sciences; 2012. Fecal & Urinary Diversions-E-Book: Management Principles. [Google Scholar]
- 23.Martins LM, Sonobe HM, Vieira Fde S, De Oliveira MS, Lenza Nde F, Da Silva Teles AA. Rehabilitation of individuals with intestinal ostomy. Br J Nurs. 2015;24:S4. doi: 10.12968/bjon.2015.24.Sup22.S4. S6, S8. [DOI] [PubMed] [Google Scholar]
- 24.Kadam A, Shinde MB. Effectiveness of structured education on caregiver's knowledge and attitude regarding colostomy care. Int J Sci Res. 2014;3:586–93. [Google Scholar]
- 25.Hashemi M, Taleghani F, Kohan S, Yousefi A. Iranian caregivers, silent mediums in caring for relatives suffering from cancer. Iran J Nurs Midwifery Res. 2014;19(Suppl 1):S83–90. [PMC free article] [PubMed] [Google Scholar]
- 26.Palma E, Simonetti V, Franchelli P, Pavone D, Cicolini G. An observational study of family caregivers’ quality of life caring for patients with a stoma. Gastroenterol Nurs. 2012;35:99–104. doi: 10.1097/SGA.0b013e31824c2326. [DOI] [PubMed] [Google Scholar]
- 27.McMullen CK, Schneider J, Altschuler A, Grant M, Hornbrook MC, Liljestrand P, et al. Caregivers as healthcare managers: Health management activities, needs, and caregiving relationships for colorectal cancer survivors with ostomies. Support Care Cancer. 2014;22:2401–8. doi: 10.1007/s00520-014-2194-3. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28.Tiruneh TE, Alem G, Taddele M, Tizazu ZM, Minale FK, Alemu KD. Knowledge, attitude, perceived responsibilities, and associated factors regarding colostomy care among nurses working in surgical units at amhara region general and referral hospitals, Ethiopia: A mixed method study. Nurs Res Rev. 2022;12:191–206. [Google Scholar]
- 29.Duruk N, Uçar H. Staff nurses’ knowledge and perceived responsibilities for delivering care to patients with intestinal ostomies: A cross-sectional study. J Wound Ostomy Continence Nurs. 2013;40(6):618–22. doi: 10.1097/WON.0b013e3182a9a7ed. [DOI] [PubMed] [Google Scholar]
- 30.Shirozhan S, Arsalani N, Maddah SS, Mohammadi-Shahboulaghi F. Rehabilitation nursing care in the acute phase of diseases with physical disabilities: A concept analysis study. Int J Nurs Knowl. 2024;35:83–92. doi: 10.1111/2047-3095.12417. [DOI] [PubMed] [Google Scholar]
- 31.Di Gesaro A. The psychological aspects of having a stoma: A literature review. Gastrointest Nurs. 2016;14:38–44. [Google Scholar]
- 32.Soares-Pinto IE, Moreira Queirós SM, Pereira Alves PJ, Sousa Carvalho TM, Vilaça de Brito Santos CS, Correia de Brito MA. Nursing interventions to promote self-care in a candidate for a bowel elimination ostomy: Scoping review. Aquichan. 2022;22:e2212. [Google Scholar]
- 33.McKenna H, Pajinkihar M, Murphy F. John Wiley & Sons; 2014. Fundamentals of Nursing Models, Theories and Practice. with Wiley e-text. [Google Scholar]
- 34.Nuopponen A. Methods of concept analysis-A comparative study. LSP J. 2010;1:1–12. [Google Scholar]
- 35.Bahramnezhad F, Asgari P, Sanaie N, Fathi A. Futilecare: A conceptanalysis with Walker and Avant's approach. Iran J Cancer Nurs. 2019;1:48–54. [Google Scholar]
- 36.Walker LO, Avant KC. Boston: Pearson; 2005. Strategies for Theory Construction in Nursing. [Google Scholar]
- 37.Lindberg SI. Mapping accountability: Core concept and subtypes. Int Rev Adm Sci. 2013;79:202–26. [Google Scholar]
- 38.Sarabi N. Tehran: Tarbiat Modares University; 2017. Designing an Adjustment Caring Model Forpatients with an Ostomy, in Nursing; p. 244. [Google Scholar]
- 39.Cetolin SF, Beltrame V, Cetolin SK, Presta AA. Social and family dynamic with patients with definitive intestinal ostomy. ABCD. Arq Bras Cir Dig. 2013;26:170–2. doi: 10.1590/s0102-67202013000300003. [DOI] [PubMed] [Google Scholar]
- 40.Cucolo DF, Perroca MG. Factors involved in the delivery of nursing care. Acta Paul Enferm. 2015;28:120–4. [Google Scholar]
- 41.Nathaniel AK, Andrews T. How grounded theory can improve nursing care quality. J Nurs Care Qual. 2007;22:350–7. doi: 10.1097/01.NCQ.0000290417.27393.91. [DOI] [PubMed] [Google Scholar]
- 42.Venes D. FA Davis; 2017. Taber's Cyclopedic Medical Dictionary. [Google Scholar]
- 43.Island T. StatPearls Publishing. 2022 Jan; PMID. [Google Scholar]
- 44.Virgin-Ellison T, Rolls N, James-Reid S, Kane M. Peterborough: Coloplast; 2019. Stoma Care Nurse Specialist: The Hidden Value of this Expert Nursing Role and Service. [Google Scholar]
- 45.Johnson T. Follow-up care of stoma patients: A systematic literature review. Gastrointest Nurs. 2012;10:30–6. [Google Scholar]
- 46.Burch J. Stoma care in the community. Br J Community Nursing. 2014;19:396–400. doi: 10.12968/bjcn.2014.19.8.396. [DOI] [PubMed] [Google Scholar]
- 47.Burch J. The community nurse and stoma care. Br J Community Nurs. 2022;27:165–8. doi: 10.12968/bjcn.2022.27.4.165. [DOI] [PubMed] [Google Scholar]
- 48.Lindberg C, Fagerström C, Sivberg B, Willman A. Concept analysis: Patient autonomy in a caring context. J Adv Nurs. 2014;70:2208–21. doi: 10.1111/jan.12412. [DOI] [PubMed] [Google Scholar]
- 49.Lopez P. Australian council of stoma associations inc. (ACSA) report. J Stomal Ther Aust. 2011;31(4):22. [Google Scholar]
- 50.Taneja C, Netsch D, Rolstad BS, Inglese G, Eaves D, Oster G. Risk and economic burden of peristomal skin complications following ostomy surgery. J Wound Ostomy Continence Nurs. 2019;46:143–9. doi: 10.1097/WON.0000000000000509. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 51.Taneja C, Netsch D, Rolstad BS, Inglese G, Eaves D, Oster G. Clinical and economic burden of peristomal skin complications in patients with recent ostomies. J Wound Ostomy Continence Nurs. 2017;44:350–7. doi: 10.1097/WON.0000000000000339. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 52.SecuriCare, Stoma care clinical nursing standards. 2019 [Google Scholar]
- 53.Shirozhan S, Arsalani N, Maddah SS, Mohammadi-Shahboulaghi F. Barriers and facilitators of rehabilitation nursing care for patients with disability in the rehabilitation hospital: A qualitative study. Frontiers in Public Health. 2022;10:931287. doi: 10.3389/fpubh.2022.931287. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 54.Myatt R. Nursing and midwifery council revalidation. Nurs Stand. 2015;30:52–9. doi: 10.7748/ns.30.7.52.s48. [DOI] [PubMed] [Google Scholar]
- 55.Augestad KM, Sneve AM, Lindsetmo R-O. Telemedicine in postoperative follow-up of STOMa PAtients: A randomized clinical trial (the STOMPA trial) J Br Surg. 2020;107:509–18. doi: 10.1002/bjs.11491. [DOI] [PubMed] [Google Scholar]
- 56.Osbourne W, Theresa B, Judy H, Gilly T, Julia W. Stoma Care Nursing Standards and Audit Tool For the Newborn to Elderly. 2015 [Google Scholar]
- 57.Babaei S, Abolhasani S. Family's supportive behaviors in the care of the patient admitted to the cardiac care unit: A qualitative study. J Caring Sci. 2020;9:80–6. doi: 10.34172/jcs.2020.012. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 58.Jeong S-K. Concept analysis of Tae-um in nurses. J Korea Acad Indus Cooperation Soc. 2018;19:482–91. [Google Scholar]
- 59.Abdolrahimi M, Ghiyasvandian S, Zakerimoghadam M, Ebadi A. Therapeutic communication in nursing students: A Walker & Avant concept analysis. Electron Physician. 2017;9:4968–77. doi: 10.19082/4968. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 60.O’Driscoll M, Allan H, Liu L, Corbett K, Serrant L. Compassion in practice—Evaluating the awareness, involvement and perceived impact of a national nursing and midwifery strategy amongst healthcare professionals in NHS Trusts in England. J Clin Nurs. 2018;27:e1097–109. doi: 10.1111/jocn.14176. [DOI] [PubMed] [Google Scholar]
- 61.Cross HH, Roe CA, Wang D. Staff nurse confidence in their skills and knowledge and barriers to caring for patients with ostomies. J Wound Ostomy Continence Nurs. 2014;41:560–5. doi: 10.1097/WON.0000000000000065. [DOI] [PubMed] [Google Scholar]
- 62.Tsujinaka S, Tan KY, Miyakura Y, Fukano R, Oshima M, Konishi F, et al. Current management of intestinal stomas and their complications. J Anus Rectum Colon. 2020;4:25–33. doi: 10.23922/jarc.2019-032. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 63.Momeni Pour R, Darvishpour A, Mansour-Ghanaei R, Kazemnezhad Leyli E. The effects of education based on the nursing process on ostomy self-care knowledge and performance of elderly patients with surgical stoma. Nurs Res Pract. 2023;2023:2800796. doi: 10.1155/2023/2800796. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 64.Mota MS, Gomes GC, Petuco VM, Heck RM, Barros EJL, de Oliveira Gomes VL. Facilitators of the transition process for the self-care of the person with stoma: Subsidies for nursing. Rev Esc Enferm USP. 2015;49:82–8. doi: 10.1590/S0080-623420150000100011. [DOI] [PubMed] [Google Scholar]
- 65.Salvadalena G, Hendren S, McKenna L, Muldoon R, Netsch D, Paquette I, et al. WOCN society and ASCRS position statement on preoperative stoma site marking for patients undergoing colostomy or ileostomy surgery. J Wound Ostomy Continence Nurs. 2015;42:249–52. doi: 10.1097/WON.0000000000000119. [DOI] [PubMed] [Google Scholar]
- 66.Readding LA. Stoma siting: What the community nurse needs to know. Br J Community Nurs. 2003;8:502–11. doi: 10.12968/bjcn.2003.8.11.11820. [DOI] [PubMed] [Google Scholar]
- 67.Rojanasarot S. The impact of early involvement in a postdischarge support program for ostomy surgery patients on preventable healthcare utilization. J Wound Ostomy Continence Nurs. 2018;45:43–9. doi: 10.1097/WON.0000000000000395. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 68.Yan M-H, Lv L, Zheng MC, Jin Y, Zhang JE. Quality of life and its influencing factors among Chinese patients with permanent colostomy in the early postoperative stage: A longitudinal study. Cancer Nurs. 2022;45:E153–61. doi: 10.1097/NCC.0000000000000893. [DOI] [PubMed] [Google Scholar]
- 69.Diniz IV, Costa IKF, Nascimento JA, Silva IPD, Mendonça AEO, Soares MJGO. Factors associated to quality of life in people with intestinal stomas. Rev Esc Enferm USP. 2021;55:e20200377. doi: 10.1590/1980-220X-REEUSP-2020-0377. [DOI] [PubMed] [Google Scholar]
- 70.Naholi RM, Nosek CL, Somayaji D. Stress among new oncology nurses. Clin J Oncol Nurs. 2015;19:115–7. doi: 10.1188/15.CJON.115-117. [DOI] [PubMed] [Google Scholar]
- 71.Yang A-H, Yan M, Qin Y-H. The development status of specialized nursing in ostomy care both in China and abroad. Chin Nurs Res. 2016;3:117–20. [Google Scholar]
- 72.Waller S, Chalmers F, Jowett A, Disley H. Achieving RCN accreditation for SecuriCare stoma care clinical nursing standards. gastrointestinal nursing. 2009 Feb;7(1):36–9. [Google Scholar]
- 73.Hibbert D. View from here: Caring for persons with ostomies in Saudi Arabia. J Wound Ostomy Continence Nurs. 2016;43:398–9. doi: 10.1097/WON.0000000000000243. [DOI] [PubMed] [Google Scholar]
- 74.Hesselink G, Smits M, Doedens M, Nijenhuis SMT, van Bavel D, van Goor H, et al. Environmental needs, barriers, and facilitators for optimal healing in the postoperative process: A qualitative study of patients’ lived experiences and perceptions. HERD. 2020;13:125–39. doi: 10.1177/1937586719900885. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 75.Shreef AMA, Abdallah HMA, Shaib SEM. Effects of bowel stoma care education program on nurses’ practice at Khartoum state governmental hospitals-Sudan. Saudi J Nurs Health Care. 2022;5:1–6. [Google Scholar]
- 76.Culha I, Kosgeroglu N, Bolluk O. Effectiveness of self-care education on patients with stomas. J Nurs Health Sci. 2016;5:70–6. [Google Scholar]
- 77.Nam KH, Kim HY, Kim JH, Kang KN, Na SY, Han BH. Effects of social support and self‐efficacy on the psychosocial adjustment of Korean ostomy patients. Int Wound J. 2019;16(Suppl 1):13–20. doi: 10.1111/iwj.13038. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 78.Persson E. Quality of care after ostomy surgery: A perspective study of patients. Ostomy Wound Manage. 2005;51:40–8. [PubMed] [Google Scholar]
- 79.Kieft RA, de Brouwer BB, Francke AL, Delnoij DM. How nurses and their work environment affect patient experiences of the quality of care: A qualitative study. BMC Health Serv Res. 2014;14:249. doi: 10.1186/1472-6963-14-249. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 80.Brown F. Psychosocial health following stoma formation: A literature review. Gastrointest Nurs. 2017;15:43–9. [Google Scholar]
- 81.Jang S-N, Avendano M, Kawachi I. Informal caregiving patterns in Korea and European countries: A cross-national comparison. Asian Nurs Res. 2012;6:19–26. doi: 10.1016/j.anr.2012.02.002. [DOI] [PubMed] [Google Scholar]
- 82.Bonill-de-las-Nieves C, Celdrán-Mañas M, Hueso-Montoro C, Morales-Asencio JM, Rivas-Marín C, Fernández-Gallego MC. Living with digestive stomas: Strategies to cope with the new bodily reality. Rev Lat Am Enfermagem. 2014;22:394–400. doi: 10.1590/0104-1169.3208.2429. [DOI] [PMC free article] [PubMed] [Google Scholar]