

Abstract
The coexistence of Parkinson's disease (PD) and myasthenia gravis (MG) is rare. When similar symptoms of both diseases overlap, it is challenging to make a concomitant diagnosis of PD and MG. The present study describes the case of a patient with concomitant PD and MG. In addition, a systematic literature review was conducted by searching PubMed and Embase for reports on all patients with concomitant PD and MG, which were then grouped and compared according to different preexisting diseases. Finally, a total of 47 cases of concomitant PD and MG (35 men; 12 women), including the present case, were analyzed. The median age of the patients at first diagnosis was 66.59±9.91 years. The interval between the two diseases varied from 2 months to 22 years. Based on the sequential occurrence of these two diseases, the patients were categorized into three groups: The prePD-MG (30 cases), preMG-PD (12 cases), and coPD-MG (5 cases) groups. In the prePD-MG group, the onset age of MG was older and head drop was more common. In the preMG-PD group, the patients were more likely to have comorbid immune diseases.
Keywords: PD, MG, coexistence, immune dysfunction, case report
Introduction
Parkinson's disease (PD) is a chronic, progressive degenerative disease associated with dopaminergic neuron loss of the substantia nigra, striatum and other brain structures, in which the balance between dopamine and acetylcholine neurotransmitters is disrupted. It is most common in middle-aged and older adults, and is characterized by resting tremors, muscle rigidity, bradykinesia and postural instability (1,2). Myasthenia gravis (MG) is a B cell-mediated, acquired autoimmune disease associated with antibodies that are directed mainly against the acetylcholine receptor (AChR) in the postsynaptic membrane at the neuromuscular junction. It occurs in patients of all ages, and is associated with partial or whole skeletal muscle weakness and fatigue (3). The coexistence of PD and MG is an uncommon phenomenon since they differ in their etiological and pathological features. Moreover, they share some similar clinical symptoms, such as fatigue, ocular symptoms, dysphagia, dysarthria and head drop (4), which may overlap and lead to diagnostic ambiguity, making co-diagnosis of PD and MG more challenging.
It is currently unclear whether the coexistence of PD and MG is coincidental or etiologically related. The imbalance between cholinergic and dopamine systems may link PD and MG. Notably, trihexyphenidyl (THP), which can reduce acetylcholine levels in the treatment of PD, has been reported to induce MG symptoms (5,6), and pyridostigmine, which can increase acetylcholine levels in the treatment of MG, can exacerbate PD symptoms (6,7). However, most patients develop the diseases without the being treated with such drugs (8-13), suggesting other mechanisms are involved in the coexistence of the two diseases. Multiple lines of evidence have indicated that immune system dysfunction serves as a critical component in susceptibility to and progression of PD, including shared molecular pathways (such as NLRP3 inflammasome activation) and polygenic risk variants (such as LRRK2 and PRKN genes) with autoimmune diseases, increased risk of PD in patients with autoimmune diseases, impaired humoral and cellular immunity, activated microglia in the brain, altered gut microbiota and inflammatory markers in the feces, as well as a lower risk after treatment with anti-inflammatory drugs and immunosuppressants (14). MG is a classic mainly AChR antibody-mediated disorder at the neuromuscular junction, which is accompanied by an activated immune response with the support of autoreactive B cells (15-17). Therefore, some links, such as immune system dysfunction, might result in the coexistence of the two diseases, even though they initially appear quite different in terms of pathogenesis.
To the best of our knowledge, there are only a few studies on MG comorbidity in patients with PD (4-13,18-28), and fewer studies (9,13,18) have summarized the clinical features of PD and MG coexistence. The present study describes the case of a patient with concomitant PD and MG, and a literature search was conducted to identify reports on all patients diagnosed with concomitant PD and MG in an attempt to analyze the clinical characteristics and explore the possible mechanisms of such comorbidity. The present study aims to alert clinicians to this potential overlap between PD and MG, with the purpose of improving diagnostic accuracy and optimizing the management of both diseases.
Case report
A 68-year-old man developed right-hand resting tremor, bradykinesia, hypomimia, constipation and sleep disturbance in January 2015, showing decreased function of dopamine transporters in the bilateral caudate nuclei, and bilateral posterior and anterior putamen as revealed by 11C-CFT PET/CT (Fig. 1). The patient was therefore diagnosed with PD. The patient responded well to levodopa (LD) (125 mg tid) and entacapone (100 mg tid). A total of 6 months before admission, the patient gradually developed fluctuating double eyelid drooping without diplopia or abnormality of ocular movements, and ophthalmic examination showed no abnormality. The patient experienced weakness in the neck muscles, with problems raising their head soon afterward, and the symptoms of muscle weakness gradually deteriorated. Furthermore, no improvement was observed after adjusting the anti-PD drugs (LD, 125 mg tid; pramipexole, 0.25 mg tid; entacapone, 200 mg tid). On admission to Tongji Hospital (Wuhan, China) in January 2021, besides ptosis and head drooping, the patient complained of symptoms of bulbar palsy (such as choking and dysphagia) and mild dyspnea. Considering the fluctuating and deteriorating muscle weakness, a neostigmine test was performed, which was positive. Repetitive nerve stimulation (RNS) revealed a progressive decrement in low-frequency RNS in both the accessory and facial nerves (Fig. 2). Nerve conduction studies were normal. Thymic hyperplasia and thymoma were not observed. There were no obvious abnormalities in thyroid function or serum creatine levels. Furthermore, tumors, autoimmune disorders (including rheumatoid arthritis, systemic lupus erythematosus and Sjogren's syndrome) or systemic autoimmune antibodies (such as antinuclear antibody) were not detected. The serum anti-AChR antibody was 30.9 nmol/l (normal range <0.40 nmol/l, enzyme-linked immunosorbent assay) and the anti-muscle specific tyrosine kinase (MuSK) antibody was negative. The patient was finally diagnosed with MG based on fluctuating weakness, positive neostigmine test results and the classical decrement in low-frequency RNS, as well as the positive anti-AChR antibody. Following treatment with intravenous immunoglobulin (IVIG, 0.4 g/kg/day for 5 days), cholinesterase inhibitors (pyridostigmine, 60 mg tid), steroids (prednisone, 20 mg qd) and immunosuppressant therapy (tacrolimus, 3 mg qd), the symptoms of MG improved, as evidenced by no drooping eyelids or drooping head, and an improvement in swallowing.
Figure 1.
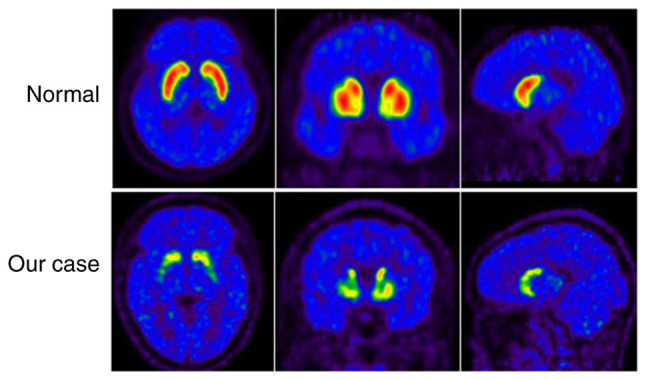
11C-CFT PET/CT. Decreased function of dopamine transporters in the bilateral heads of caudate nuclei, and bilateral anterior and posterior putamen. The normal images were obtained from healthy individuals at the medical examination center in Tongji Hospital, and individuals provided written informed consent for the publication of these images.
Figure 2.
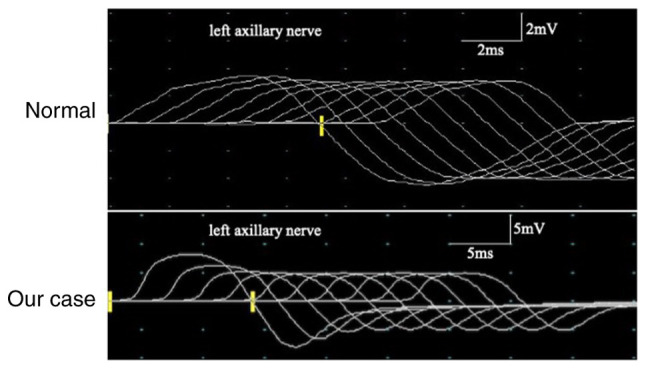
Repetitive nerve stimulation at 3 Hz showed a >10% decrease in the wave amplitudes of the left axillary nerve. The normal images were obtained from healthy individuals at the medical examination center in Tongji Hospital, and individuals provided written informed consent for the publication of these images.
After a 3-year follow-up, both MG and PD symptoms remained stable. At this time point, the patient had discontinued the steroid treatment, whereas a low dosage of tacrolimus (1 mg daily) and pyridostigmine (60 mg, twice daily) was maintained to prevent MG relapse. For PD treatment, LD (125 mg tid), pramipexole (0.25 mg tid) and Stalevo (325 mg tid) were used as maintenance medications.
Subsequently, a systematic literature review was conducted by searching the PubMed (https://pubmed.ncbi.nlm.nih.gov/) and Embase (http://www.embase.com). databases for reports on all patients with concomitant PD and MG up to October 31, 2023. Search terms included ‘Parkinson's disease’ or ‘Parkinson's syndrome’ or ‘Parkinsonism’ AND ‘myasthenia gravis’ or ‘myasthenia’. The reference lists of the included articles were also reviewed. All cases of concomitant PD and MG were summarized and analyzed, then grouped and compared according to different preexisting diseases.
Finally, a total of 47 cases of concomitant PD and MG, including the current case, were analyzed. The patients were categorized into three groups based on the sequential occurrence of these two diseases. In the prePD-MG group, 30 patients were initially diagnosed with PD, followed by a subsequent diagnosis of MG (Table I). In the preMG-PD group, MG was diagnosed in 12 patients, followed by a subsequent PD diagnosis (Table II). The remaining 5 cases failed to note the order of diagnosis occurrence and were considered the coPD-MG group (Table III).
Table I.
Demography and clinical characteristics of the prePD-MG group.
| First author, year | Sex/Age, years | PD symptoms | PD treatment | Comorbidities | Interval | MG antibodies | Ocular symptoms | Dysphagia | Dysarthria | Head drop | MG treatment | (Refs.) |
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Ueno, 1987 | M/55 | RT + Hm | THP, LD | DM | 5.5 years | AChR: P | Y | Y | N | Y | Pyd | (5) |
| Tasić, 1991 | M/74 | RT + R | THP, amantadine | Tuberculous lymphadenitis | 3 years | NR | Y | Y | Y | N | Pyd | (21) |
| Kao, 1993 | F/54 | R + RT + Hm + BK | THP, Sinemet | NR | 7 years | AChR: P | Y | Y | Y | Y | Pyd, CS | (6) |
| Levin, 2003 | M/76 | RT + R | LD | NR | 5 years | AChR: P | N | N | N | Y | Pyd, AZA | (8) |
| Levin, 2003 | M/62 | R + RT | LD, pergolide, selegiline, amantadine | NR | 4 years | AChR: P | Y | N | N | N | Pyd | (8) |
| Levin, 2003 | M/61 | R | LD | GD, hyperthyroidism | NR | NR | Y | N | N | N | Pyd | (8) |
| Fasano, 2008 | F/53 | RT + R + BK | NR | NR | 5 years | AChR: Ne; MuSK: Ne | N | N | N | Y | Pyd, CS, AZA, PE | (19) |
| Unal-Cevik, 2009 | M/80 | RT + R + BK | NR | Hypothyroidism, HPT | 4 years | AChR: Ne | N | N | N | Y | Pyd | (22) |
| Uludag, 2011 | M/66 | RT + R | LD, benserazide | HPT, COPD, hyperlipidemia | 9 years | AChR: P | N | N | N | Y | IVIG, Pyd | (10) |
| Lanfranconi, 2011 | M/70 | RT + BK + R + Hm | LD | NR | 3 years | AChR:Ne; MuSK: P | Y | Y | Y | N | CS | (11) |
| Zis, 2014 | M/64 | R | NR | HPT, RA | 5 years | AChR: P; Musk: Ne | N | N | N | Y | Pyd, CS | (20) |
| Neuman, 2014 | F/68 | RT + R + BK | LD | NR | 7 years | AChR: P | N | N | N | Y | Pyd, AZA, IVIG | (12) |
| Sciacca, 2016 | F/57 | NR | NR | NR | 9 years | NR | Y | N | N | N | Pyd | (18) |
| Sciacca, 2016 | M/60 | NR | NR | NR | 3 years | NR | Y | N | N | Y | Pyd | (18) |
| Sciacca, 2016 | M/67 | NR | NR | NR | 3 years | AChR: P | Y | N | N | N | Pyd | (18) |
| Tung-Chen, 2016 | F/71 | BK + Hm + R + RT | LD | Anemia | 19 years | AChR: Ne | Y | Y | Y | N | Pyd, CS, AZA, IVIG | (13) |
| Aiba, 2016 | F/71 | R + BK | LD | NR | 5 years | AChR: P | N | N | N | Y | Pyd, CS | (23) |
| Hogg, 2017 | M/75 | BK + Hm + R | NR | Myopathy | 3-4 months | AChR: P | Y | Y | Y | Y | Pyd | (24) |
| Urban, 2018 | M/76 | NR | NR | NR | 6 years | AChR: P | N | Y | N | N | Pyd, CS, IVIG, AZA | (25) |
| Urban, 2018 | M/90 | NR | NR | NR | 5 years | AChR: P | N | Y | N | N | Pyd, CS | (25) |
| Urban, 2018 | M/78 | NR | NR | NR | 5 years | AChR: P | N | Y | N | N | Pyd, CS. AZA | (25) |
| Urban, 2018 | M/74 | NR | NR | NR | 7 years | AChR: P | N | Y | Y | N | Pyd, IVIG, CS, AZA | (25) |
| Marano, 2019 | M/65 | RT + BK + R | LD | NR | 8 years | AChR: P | Y | Y | N | Y | Pyd, CS, AZA | (26) |
| Odajiu, 2019 | M/49 | BK + R + Hm | Stalevo, ropinirole rasagiline | Crohn's disease | 11 years | AChR: P | Y | N | N | N | Pyd | (9) |
| Odajiu, 2019 | F/64 | BK + RBD + Hm + R | Stalevo, pramipexole, rasagiline | HPT | 4 years | AChR: Ne | Y | Y | Y | N | Pyd | (9) |
| Odajiu, 2019 | M/52 | RT + BK + R | Stalevo, rasagiline, THP | DM, HPT | 3 years | AChR:Ne; MuSK: Ne | Y | N | N | N | Pyd | (9) |
| Alshaikh, 2021 | M/61 | NR | NR | Vitamin B12 deficiency | 6 years | AChR: P | Y | Y | Y | N | NR | (4) |
| Alshaikh, 2021 | M/61 | NR | NR | Neuropathy, vitamin B12 deficiency | 1 year | AChR: P | Y | Y | Y | Y | NR | (4) |
| Alshaikh, 2021 | M/82 | NR | NR | NR | NR | AChR: P | NR | Y | Y | N | NR | (4) |
| Current case | M/62 | RT + BK | LD, entacapone | None | 6 years | AChR: P; MuSK: Ne | Y | Y | N | Y | Pyd, CS, IVIG, tacrolimus (FK506) |
F, female; M, male; PD, Parkinson's disease; Hm, hypomimia; R, rigidity; RT, resting tremor; BK, bradykinesia; LD, levodopa; THP, trihexyphenidyl; RBD, rapid eye movement sleep behavior disorder; DM, diabetes mellitus; GD, Graves' disease; HPT, hypertension; RA, rheumatoid arthritis; COPD, chronic obstructive lung disease; MG, myasthenia gravis; AChR, acetylcholine receptor; MuSK, muscle-specific kinase; AZA, azathioprine; CS, prednisone/methylprednisolone; Pyd, pyridostigmine; IVIG, intravenous immunoglobulin; NR, not reported; P, positive; Ne, negative; Y, yes; N, No.
Table II.
Demography and clinical characteristics of the preMG-PD group.
| First author, year | Sex/Age, years | MG antibodies | Ocular symptoms | Dysphagia | Dysarthria | Head drop | MG treatment | Comorbidities | Interval | PD symptoms | PD treatment | (Refs.) |
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Iwasaki, 1988 | F/62 | AChR: P | Y | N | N | N | Pyd | NR | 2 months | R + RT + BK | None | (7) |
| Levin, 2003 | F/68 | AChR: P | Y | N | N | N | Pyd, AZA | NR | 3 years | R + restlessness | LD | (8) |
| Neuman, 2014 | M/72 | AChR: P | Y | N | N | N | Pyd | NR | 4 years | RT + R + BK | NO | (12) |
| Ozer, 2016 | M/67 | NR | N | N | Y | N | Pyd | Chronic subdural hematoma | 16 months | BK | LD, benserazide | (27) |
| Alshaikh, 2021 | M/70 | AChR: P | Y | N | N | Y | NR | Thyroid disease | 8 years | NR | NR | (4) |
| Alshaikh, 2021 | M/66 | AChR: P | Y | Y | Y | N | NR | Neuropathy, thyroid disease, vitamin B12 deficiency, childhood polio | 1 year | NR | NR | (4) |
| Alshaikh, 2021 | M/66 | AChR: P | Y | Y | Y | Y | NR | Neuropathy, thyroid disease, vitamin B12 deficiency | 8 years | NR | NR | (4) |
| Alshaikh, 2021 | F/85 | AChR: P | Y | Y | Y | Y | NR | Neuropathy | 4 years | NR | NR | (4) |
| Alshaikh, 2021 | M/49 | SN | Y | Y | Y | N | NR | Thyroid disease | 22 years | NR | NR | (4) |
| Alshaikh, 2021 | F/55 | NR | Y | Y | N | N | NR | Neuropathy | 19 years | NR | NR | (4) |
| Alshaikh, 2021 | M/59 | SN | N | Y | N | N | NR | Neuropathy, thyroid disease, Lyme disease | 10 years | NR | NR | (4) |
| Alshaikh, 2021 | M/52 | NR | Y | N | N | N | NR | Thyroid disease, vitamin B12 deficiency | 20 years | NR | NR | (4) |
F, female; M, male; PD, Parkinson's disease; R, rigidity; RT, resting tremor; BK, bradykinesia; LD, levodopa; SN, seronegative; MG, myasthenia gravis; AChR, acetylcholine receptor; MuSK, muscle-specific kinase; NR, not reported; P, positive; Y, yes; N, No.
Table III.
Demography and clinical characteristics of the co MG-PD group.
| First author, year | Sex | Age at diagnosis of PD/MG, years | Comorbidities | MG antibodies | Ocular symptoms | Dysphagia | Dysarthria | Head drop | (Refs.) |
|---|---|---|---|---|---|---|---|---|---|
| Albassam, 2021 | F | 72/72 | HPT, DM, dyslipidemia | AChR: N; MuSK: P | Y | Y | N | N | (28) |
| Alshaikh, 2021 | M | 78/- | Thyroid disease | AChR: P | Y | N | N | N | (4) |
| Alshaikh, 2021 | M | 60/- | Neuropathy, vitamin B12 deficiency, CVID | AChR: P | Y | Y | Y | N | (4) |
| Alshaikh, 2021 | M | -/- | Thyroid disease, hemophilia A | AChR: P | Y | Y | Y | N | (4) |
| Alshaikh, 2021 | M | 84/- | Thyroid disease | AChR: P | NR | NR | NR | NR | (4) |
F, female; M, male; PD, Parkinson's disease; MG, myasthenia gravis; AChR, acetylcholine receptor; MuSK, muscle-specific kinase; NR, not reported; CVID, common variable immunodeficiency; -, unknown; P, positive; NeY, yes; N, No.
The overall median age of patients at first diagnosis was 66.59±9.91 years (range: 49-90 years), with 35 (74.47%) men and 12 (25.53%) women (Table IV). Notably, some of the cases counted in the present study did not report detailed clinical information; therefore, proportions were calculated as the percentage of individuals reporting on that indicator. Various comorbidities were observed, particularly autoimmune diseases, with hypertension present in 6 patients (21.43%) of 28 patients, thyroid disease in 12 patients (42.86%), neuropathy in 7 patients (25.00%), and rheumatoid arthritis, Crohn's disease or myopathy in 1 patient each (3.58%).
Table IV.
General characteristics of PD combined with MG.
| Characteristic | Concomitant PD and MG (n=47) | PrePD-MG (n=30) | PreMG-PD (n=12) | CoPD-MG (n=5) | P-valuea |
|---|---|---|---|---|---|
| Mean ± SD PD-onset age, years | 68.76±9.44 | 66.60±9.81 | 72.58±6.72 | 73.50±10.25 | 0.061 |
| Mean ± SD MG-onset age, years | 69.67±10.25 | 71.91±9.92 | 64.25±9.78 | - | 0.030b |
| Sex, M/F | 35/12 | 23/7 | 8/4 | 4/1 | 0.505 |
| History diseases, % | |||||
| Hypertension | 21.43 | 35.71 | 0 | 20.00 | 0.039b |
| Diabetes mellitus | 10.71 | 14.29 | 0 | 20.00 | 0.360 |
| Other immune diseases, % | |||||
| Thyroid disease | 42.86 | 21.43 | 66.67 | 60.00 | 0.042b |
| Neuropathy | 25.00 | 7.14 | 55.56 | 20.00 | 0.018b |
| RA | 3.58 | 7.14 | 0 | 0 | 0.609 |
| Crohn's disease | 3.58 | 7.14 | 0 | 0 | 0.609 |
| Myopathy | 3.58 | 7.14 | 0 | 0 | 0.609 |
| Median disease interval, years | 5 | 5 | 5 | - | |
| PD symptoms, % | |||||
| R | 88.00 | 90.00 | 75.00 | 100.00 | 0.437 |
| RT | 64.00 | 70.00 | 50.00 | 0 | 0.407 |
| BK | 64.00 | 65.00 | 50.00 | 100.00 | 0.486 |
| Hm | 32.00 | 35.00 | 0 | 100.00 | 0.224 |
| PD treatment, % | |||||
| Levodopa | 85.71 | 93.75 | 50.00 | 100.00 | 0.088 |
| THP | 19.05 | 25.00 | 0 | 0 | 0.376 |
| DA | 14.29 | 18.75 | 0 | 0 | 0.491 |
| MAO-B | 19.05 | 25.00 | 0 | 0 | 0.376 |
| COMT | 19.05 | 25.00 | 0 | 0 | 0.376 |
| Amantadine | 9.52 | 12.50 | 0 | 0 | 0.632 |
| MG symptoms, % | |||||
| Ocular symptoms | 69.57 | 62.07 | 83.33 | 100.00 | 0.138 |
| Head drop | 54.54 | 71.43 | 25.00 | 0 | 0.013b |
| Dysphagia | 55.32 | 54.84 | 50.00 | 75.00 | 0.521 |
| Dysarthria | 38.30 | 35.48 | 41.67 | 50.00 | 0.485 |
| Limb weakness | 36.36 | 32.14 | 50.00 | 100.00 | 0.427 |
| MG-antibodies, % | |||||
| AChR-Ab | 77.50 | 76.92 | 77.78 | 80.00 | 0.670 |
| MuSK-Ab | 5.00 | 3.85 | 0 | 20.00 | 0.743 |
| MG-treatment, % | |||||
| Pyd | 96.88 | 96.30 | 100.00 | 100.00 | 0.871 |
| CS | 40.63 | 44.44 | 0 | 100.00 | 0.123 |
| IVIG | 12.8 | 18.52 | 0 | 100.00 | 0.475 |
| AZA | 31.25 | 29.63 | 25.00 | 100.00 | 0.673 |
aP-value, PrePD-MG vs. PreMG-PD.
bSignificant P-values (P<0.05). P-values were calculated using independent t-tests or Fisher's exact test. F, female; M, male; PD, Parkinson's disease; MG, myasthenia gravis; Hm, hypomimia; R, rigidity; RT, resting tremor; BK, bradykinesia; RA, rheumatoid arthritis; THP, trihexyphenidyl; DA, dopamine receptor agonist; MAO-B, monoamine oxidase-B inhibitor; COMT, catechol-O-methyltransferase inhibitor; AChR, acetylcholine receptor; MuSK, muscle-specific kinase; AZA, azathioprine; CS, prednisone/methylprednisolone; Pyd, pyridostigmine; IVIG, intravenous immunoglobulin.
The initial symptoms of PD included rigidity (88.00%), resting tremors (64.00%), bradykinesia (64.00%) and hypomimia (32.00%), which could be present in any combination with other symptoms. The anti-PD therapy was mainly LD (85.71%), THP (19.05%), dopamine receptor agonists (14.29%), monoamine oxidase-B inhibitors (19.05%), catechol-O-methyltransferase inhibitors (19.05%), and amantadine (9.52%).
In terms of MG clinical signs, 32 patients (69.57%) had ocular symptoms, including ptosis and diplopia, 26 (55.32%) had dysphagia, 18 (38.30%) had dysarthria, 18 (54.54%) had head drop and 12 (36.36%) had limb weakness. Among the 40 patients who underwent antibody detection, 31 (77.50%) were positive for AChR antibodies and 2 (5.00%) were positive for MuSK antibodies. None of the patients had thymoma or thymic hyperplasia (data not shown). Anti-MG therapy was mainly pyridostigmine (96.88%), and some patients were treated with prednisone/methylprednisolone (40.63%), azathioprine (31.25%) or IVIG (6 cases, 12.8%).
In the prePD-MG group, the average age at diagnosis with MG was 71.91±9.92 years, which was older than that in the preMG-PD group. GraphPad Prism (v8.0.2; Dotmatics) was applied for the statistical analysis. P-values were calculated using independent t-tests or Fisher's exact test. The interval between PD and MG diagnosis ranged from 3-4 months to 20 years (median, 5 years). These patients were more prone to comorbidities, such as hypertension. Most patients had typical PD symptoms and anti-PD therapy was diverse. As for MG clinical signs, head drop was more common in this group than in the preMG-PD group. However, due to limited information, the present study could not determine which stage of PD was prone to MG and which type of MG was more likely to occur.
Patients in the preMG-PD group were more prone to immune disease comorbidities, such as thyroid disease and neuropathy, and there were higher proportion of women in this group than in the prePD-MG group. The interval from MG to PD diagnosis ranged from 2 months to 22 years (median, 5 years). Moreover, in this group, although there was no statistical difference, the proportion of ocular symptoms and limb weakness seemed higher, whereas PD symptoms were relatively fewer than those in the prePD-MG group and anti-PD therapy was relatively single (only LD) The present study attempted to analyze which type of MG was more prone to PD; however, due to limited information, conclusions could not be drawn.
Although the number of CoPD-MG cases was relatively low, their clinical characteristics was similar to that of the prePD-MG group. Both the basic treatment of MG and PD were effective in the three groups.
Discussion
The coexistence of neurodegenerative diseases and autoimmune diseases is not uncommon. However, as a rare disease, the incidence rate of MG worldwide was only 10-29 per million person-years based on data from the past decade (29), which makes the coexistence of PD and MG relatively rare. In clinical practice, the overlap of some indicators, such as ocular symptoms, limb weakness and head drop, leads to a misdiagnosis or delayed diagnosis; therefore, the actual reported cases of PD and MG comorbidity may be less. The present study described the case of a patient co-diagnosed as having PD and MG with positive anti-AChR antibodies. After searching the literature, 47 cases of PD and MG comorbidity, including the current case, were identified. Similar to previous studies (9,13,18), in order to better present the cases, the clinical data of each patient were listed in tables. In contrast to other studies, the present study added newly reported cases, summarized their demographic and clinical characteristics, and categorized and compared them based on different preexisting diseases. Overall, the average age of the three groups was relatively old. The interval between the two diseases varied from 2 months to 22 years. In addition to MG, autoimmune diseases, such as thyroid disease and rheumatoid arthritis, were also observed in these patients. AChR antibodies were the most common among those who underwent antibody testing. Consistent with recent studies, the present study revealed that most of the cases were male patients (30,31), and most patients were diagnosed with PD before being diagnosed with MG (30).
With varying initial diseases, each of the three groups exhibited distinct characteristics. The mean age at diagnosis of MG was older in the prePD-MG group than that in the preMG-PD group. One possible explanation for this phenomenon is the varying initial diseases, as PD tends to manifest in the older population. Moreover, hypertension was most frequently observed in this group, which may be due to the same reason as that aforementioned. Another possibility is the increase in the incidence of MG in older adults (32). The main clinical features of MG, such as ocular symptoms and limb weakness, were easily masked by bradykinesia and rigidity in the prePD-MG group, which challenged the diagnosis of MG in such a group. Moreover, the sign of head drop was more prominent in the prePD-MG group, which was consistent with a previous finding that the proportion of head drop in PD was higher than that in MG (33). Since the head drop was less affected by bradykinesia and rigidity, the comorbidity of MG should be considered once a fluctuation in head drop has been observed in patients with PD. In the preMG-PD group, it may be easier to make a certain diagnosis of both diseases because the symptoms related to MG are more clearly discernible in this pattern. Moreover, ophthalmoplegia and limb weakness appeared to be more common, as they were not masked by PD symptoms. Patients in this group were more prone to comorbid autoimmune diseases, with female patients being more susceptible to the preMG-PD pattern, which could be related to the fact that they were more prone to autoimmune diseases (34).
The mechanisms underlying concomitant PD and MG remain unknown. Whether it is a casual phenomenon or if there is a causative relationship between both diseases requires further clarification. Iatrogenic causes have been reported in some comorbidity cases (5-7). THP for treating PD has been reported to induce MG symptoms (5,6), and pyridostigmine for treating MG can exacerbate PD symptoms (6,7). Moreover, systematic immune dysfunction has been revealed in PD and MG comorbidity, with reports of thyroid disease, MG and PD (8), and rheumatoid arthritis, MG and PD comorbidities (20). However, it is currently unknown whether patients with PD and MG comorbidity share similar genetic associations, such as LRRK2 gene mutations, observed between PD and inflammatory bowel disease (35).
Some studies have detected autoantibodies to α-synuclein (36,37) and autoreactive T cells that recognize specific α-synuclein epitopes in patients with PD (38), thus indicating that immune reactions participate in the pathophysiology of PD. In addition, studies have revealed that B cells contribute to the pathogenesis of PD (39), including deposits of immunoglobulin G (IgG) found on dopaminergic neurons (40), Lewy bodies coated with IgG (41), and increased levels of anti-α-synuclein antibodies in the cerebrospinal fluid and the blood (36,37). Aberrant functioning of the immune system, as aforementioned, has been proposed as a critical component of susceptibility to and progression of PD (14). In addition, MG is a classic antibody-mediated disorder dependent on autoreactive B cells that require T-cell support (15,16), accompanied by an activated immune response in the neuromuscular junction from the early stage of the disease (17). Therefore, a common pathophysiological mechanism of immune dysfunction may result in PD and MG comorbidity.
Inflammatory mechanisms might also be involved in the process of concomitant PD and MG. An increase in cytokines, such as TNF-α, IL-1β and IL-6, in the peripheral blood has been detected and proven to have a significant role in the progression of PD (42). Adaptive immune components in the peripheral blood of patients with PD have also been observed, such as type 1 T-helper cells and interleukin-17-producing T-helper cells, contributing to high blood levels of interferon-γ and tumor necrosis factor (43). In a recent study, the neutrophil-to-lymphocyte ratio (NLR), a marker of peripheral inflammation, was used to detect peripheral inflammation in PD, and the NLR ratio was revealed to be higher in the PD group than that in the control group (44). Microglia, local innate immune cells in the brain, become activated in response to inflammation and are involved in dopaminergic neuron damage via various mechanisms in PD (14). Furthermore, different proinflammatory or inflammatory mediators have been reported to contribute to the pathogenesis of MG (45). The initial activation of peripheral immunocytes and cytokines in MG might infiltrate the brain parenchyma once the blood-brain barrier is compromised, thus leading to the subsequent activation of central inflammation, such as antigen-antibody reaction associated with α-synuclein, or the direct infiltration of the microglia, monocytes and dendritic cells (14).
Gut-derived inflammation may also be associated with the co-occurrence of PD and MG. The gut microbiota and its metabolites have been shown to be involved in the regulation of neuroinflammation, barrier function and neurotransmitter activity in PD (46). The microbiota-gut-brain axis, a form of bidirectional communication between the enteric nervous system and the central nervous system, may provide a pathway for the transmission of α-synuclein (46). Similarly, accumulating evidences has endorsed the key role of gut microbiota in the pathogenesis of MG (47,48), particularly the effects on T-helper 17/regulatory T cell balance, the imbalance of which can result in the progression of MG.
Taken together, it is plausible to assume that immune dysfunction and inflammatory mechanisms may contribute to the comorbidity of MG and PD, with the initial peripheral immune dysfunction or inflammation triggering neuroinflammation resulting in activation of the degenerative process. However, it is challenging to determine which mechanisms are involved in the different groups assessed in the present study.
The present study had some limitations. First, due to the small number of reported comorbidities and the lack of detailed patient-specific information, the analysis based on the existing data has a certain degree of bias, and it cannot be graded based on the severity of patients. However, the data of most patients were relatively detailed, and a small amount of unprovided data did not affect most results. Larger scale studies are required to examine the co-occurrence of PD and MG, which may improve understanding of this complication. Second, all mechanisms of PD and MG comorbidity were speculative based on current reported studies, and more basic research is required to understand the pathogenesis of the comorbidity. New immune-based therapeutic options may focus on eliminating circulating autoantibodies or inhibiting effector mechanisms by targeting B cells, B-cell growth factors or other immunosuppressive treatments in such comorbidities.
In conclusion, the coexistence of PD and MG is very rare. The overlapping symptoms of these two diseases can be challenging, especially when the initial disease is PD. Clinicians should pay attention to this potential overlap in order to improve the accuracy of PD and MG co-diagnosis, and to optimize the management of these two diseases. Immune dysfunction and inflammation may result in the coexistence of neurodegenerative and neuroimmune diseases due to interactions between the brain parenchyma and blood circulation. Further therapeutic interventions aimed at immune-associated mechanisms could be of great use to delay disease progression and pathological processes.
Acknowledgements
Not applicable.
Funding Statement
Funding: This study was supported by grants from the Natural Science Foundation of Hubei Province (grant no. 2020CFB744) and the National Natural Science Foundation of China (grant no. 81901303).
Availability of data and materials
The data generated in the present study may be requested from the corresponding author.
Authors' contributions
ZM and QN collected the data and confirm the authenticity of all the raw data. ZX processed the statistical data. ZM and ZL drafted and revised the manuscript. ZM and ZL designed and guided the study. All authors read and approved the final version of the manuscript.
Ethics approval and consent to participate
This study was approved by the Ethics Committee of Tongji Hospital, Tongji Medical College, Huazhong University of Science and Technology (approval no. TJ-IRB20211273).
Patient consent for publication
The patient and healthy individuals providing normal images provided written informed consent for publication.
Competing interests
The authors declare that they have no competing interests.
References
- 1.Armstrong MJ, Okun MS. Diagnosis and treatment of Parkinson disease: A review. JAMA. 2020;323:548–560. doi: 10.1001/jama.2019.22360. [DOI] [PubMed] [Google Scholar]
- 2.Jankovic J, Tan EK. Parkinson's disease: Etiopathogenesis and treatment. J Neurol Neurosurg Psychiatry. 2020;91:795–808. doi: 10.1136/jnnp-2019-322338. [DOI] [PubMed] [Google Scholar]
- 3.Gilhus NE. Myasthenia Gravis. N Engl J Med. 2016;375:2570–2581. doi: 10.1056/NEJMra1602678. [DOI] [PubMed] [Google Scholar]
- 4.Alshaikh JT, Mills K. Coincident parkinsonism and myasthenia gravis: A case series. Parkinsonism Relat Disord. 2021;89:4–5. doi: 10.1016/j.parkreldis.2021.06.016. [DOI] [PubMed] [Google Scholar]
- 5.Ueno S, Takahashi M, Kajiyama K, Okahisa N, Hazama T, Yorifuji S, Tarui S. Parkinson's disease and myasthenia gravis: Adverse effect of trihexyphenidyl on neuromuscular transmission. Neurology. 1987;37:832–833. doi: 10.1212/wnl.37.5.832. [DOI] [PubMed] [Google Scholar]
- 6.Kao KP, Kwan SY, Lin KP, Chang YC. Coexistence of Parkinson's disease and myasthenia gravis: A case report. Clin Neurol Neurosurg. 1993;95:137–139. doi: 10.1016/0303-8467(93)90008-5. [DOI] [PubMed] [Google Scholar]
- 7.Iwasaki Y, Wakata N, Kinoshita M. Parkinsonism induced by pyridostigmine. Acta Neurol Scand. 1988;78(236) doi: 10.1111/j.1600-0404.1988.tb03653.x. [DOI] [PubMed] [Google Scholar]
- 8.Levin N, Karussis D, Abramsky O. Parkinson's disease associated with myasthenia gravis. A report of 4 cases. J Neurol. 2003;250:766–767. doi: 10.1007/s00415-003-1088-y. [DOI] [PubMed] [Google Scholar]
- 9.Odajiu I, Davidescu EI, Mitu C, Popescu BO. Patients with Parkinson's disease and myasthenia Gravis-A report of three new cases and review of the literature. Medicina (Kaunas) 2019;56(5) doi: 10.3390/medicina56010005. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Uludag IF, Korucuk M, Sener U, Zorlu Y. Myasthenia gravis as a cause of head drop in Parkinson disease. Neurologist. 2011;17:144–146. doi: 10.1097/NRL.0b013e3182173356. [DOI] [PubMed] [Google Scholar]
- 11.Lanfranconi S, Corti S, Baron P, Conti G, Borellini L, Bresolin N, Bersano A. Anti-MuSK-Positive myasthenia gravis in a patient with parkinsonism and cognitive impairment. Neurol Res Int. 2011;2011(859802) doi: 10.1155/2011/859802. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Neuman LA, Cheema FZ. Two cases of Parkinson disease and concurrent myasthenia gravis, generalized and ocular. Neurohospitalist. 2014;4:117–118. doi: 10.1177/1941874414522498. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Tung-Chen Y, Bataller L, Sevilla T, López-Aldeguer J. Co-occurrence of myasthenia gravis with Parkinson's disease: A not to be missed diagnosis. Geriatr Gerontol Int. 2016;16:528–530. doi: 10.1111/ggi.12558. [DOI] [PubMed] [Google Scholar]
- 14.Tan EK, Chao YX, West A, Chan LL, Poewe W, Jankovic J. Parkinson disease and the immune system-associations, mechanisms and therapeutics. Nat Rev Neurol. 2020;16:303–318. doi: 10.1038/s41582-020-0344-4. [DOI] [PubMed] [Google Scholar]
- 15.Gilhus NE, Verschuuren JJ. Myasthenia gravis: Subgroup classification and therapeutic strategies. Lancet Neurol. 2015;14:1023–1036. doi: 10.1016/S1474-4422(15)00145-3. [DOI] [PubMed] [Google Scholar]
- 16.Yi JS, Guptill JT, Stathopoulos P, Nowak RJ, O'Connor KC. B cells in the pathophysiology of myasthenia gravis. Muscle Nerve. 2018;57:172–184. doi: 10.1002/mus.25973. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Malaspina A, Puentes F, Amor S. Disease origin and progression in amyotrophic lateral sclerosis: An immunology perspective. Int Immunol. 2015;27:117–129. doi: 10.1093/intimm/dxu099. [DOI] [PubMed] [Google Scholar]
- 18.Sciacca G, Nicoletti A, Mostile G, Dibilio V, Raciti L, Luca A, Reggio E, Zappia M. Is it just a coincidence? Three new cases of Myasthenia Gravis associated with Parkinson's disease. Parkinsonism Relat Disord. 2016;28:166–168. doi: 10.1016/j.parkreldis.2016.04.005. [DOI] [PubMed] [Google Scholar]
- 19.Fasano A, Evoli A, Piano C, Tonali PA, Bentivoglio AR. Myasthenia gravis: An unrecognized cause of head drop in Parkinson's disease. Parkinsonism Relat Disord. 2008;14:164–165. doi: 10.1016/j.parkreldis.2007.02.009. [DOI] [PubMed] [Google Scholar]
- 20.Zis P, Argiriadou V, Temperikidis PP, Zikou L, Tzartos SJ, Tavernarakis A. Parkinson's disease associated with myasthenia gravis and rheumatoid arthritis. Neurol Sci. 2014;35:797–799. doi: 10.1007/s10072-014-1660-5. [DOI] [PubMed] [Google Scholar]
- 21.Tasić Z, Stefanović P, Apostoloski S. An unusual association of myasthenia gravis and Parkinsonism in a female patient with tuberculous lymphadenitis. Srp Arh Celok Lek. 1991;119:103–106. (In Serbian) [PubMed] [Google Scholar]
- 22.Unal-Cevik I, Temucin CM. Head drop in an elder Parkinson's disease after development of myasthenia gravis. Mov Disord. 2009;24:2025–2026. doi: 10.1002/mds.22704. [DOI] [PubMed] [Google Scholar]
- 23.Aiba Y, Iwakawa M, Sakakibara R, Tsuyusaki Y, Tateno F, Kishi M, Tateno H, Ogata T. Myasthenia gravis manifesting as head drop in an elderly adult with Parkinson's disease. J Am Geriatr Soc. 2016;64:e120–e122. doi: 10.1111/jgs.14359. [DOI] [PubMed] [Google Scholar]
- 24.Hogg EJ, Lewis RA, Bannykh S, Tagliati M. Head drop in Parkinson's disease complicated by myasthenia gravis and myopathy. J Neurol Sci. 2017;376:216–218. doi: 10.1016/j.jns.2017.03.026. [DOI] [PubMed] [Google Scholar]
- 25.Urban PP, Stammel O. Myasthenia gravis should be considered in cases of Parkinson's disease and progressive dysphagia. Nervenarzt. 2018;89:443–445. doi: 10.1007/s00115-017-0378-z. (In German) [DOI] [PubMed] [Google Scholar]
- 26.Marano M, Lanzone J, di Biase L, Pepe A, Di Santo A, Di Lazzaro V. A rare cause of axial worsening in Parkinson's disease: A case of myasthenic pseudo-parkinsonism. Clin Neurol Neurosurg. 2019;179:1–3. doi: 10.1016/j.clineuro.2019.02.009. [DOI] [PubMed] [Google Scholar]
- 27.Ozer AB, Catak T, Ozdemir M, Kilinc M. Anesthesia management in the coexistence of myasthenia gravis and parkinsonism. J Clin Anesth. 2016;34:350–351. doi: 10.1016/j.jclinane.2016.05.033. [DOI] [PubMed] [Google Scholar]
- 28.Albassam MS, Thabet SA, Hmoud M, Makkawi S. Anti-Muscle specific kinase (Anti-MuSK) positive myasthenia gravis overlapping with Parkinson's disease: A challenging diagnosis. Cureus. 2021;13(e14839) doi: 10.7759/cureus.14839. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29.Punga AR, Maddison P, Heckmann JM, Guptill JT, Evoli A. Epidemiology, diagnostics, and biomarkers of autoimmune neuromuscular junction disorders. Lancet Neurol. 2022;21:176–188. doi: 10.1016/S1474-4422(21)00297-0. [DOI] [PubMed] [Google Scholar]
- 30.Zhang Q, Xu E, Li HF, Chan P, Zhao Z, Ma J. Parkinson's disease and comorbid myasthenia gravis: A case report and literature review. Front Neurol. 2024;14(1303434) doi: 10.3389/fneur.2023.1303434. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 31.Iori E, Mazzoli M, Ariatti A, Salviato T, Rispoli V, Valzania F, Galassi G. Myasthenia Gravis crossing Parkinson's disease: A 20 year study from single Italian center. Int J Neurosci. 2024;134:429–435. doi: 10.1080/00207454.2022.2107517. [DOI] [PubMed] [Google Scholar]
- 32.Somnier FE. Increasing incidence of late-onset anti-AChR antibody-seropositive myasthenia gravis. Neurology. 2005;65:928–930. doi: 10.1212/01.wnl.0000176067.32186.a3. [DOI] [PubMed] [Google Scholar]
- 33.Drain JP, Virk SS, Jain N, Yu E. Dropped head syndrome: A systematic review. Clin Spine Surg. 2019;32:423–429. doi: 10.1097/BSD.0000000000000811. [DOI] [PubMed] [Google Scholar]
- 34.Berrih-Aknin S, Panse RL, Dragin N. AIRE: A missing link to explain female susceptibility to autoimmune diseases. Ann N Y Acad Sci. 2018;1412:21–32. doi: 10.1111/nyas.13529. [DOI] [PubMed] [Google Scholar]
- 35.Peter I, Dubinsky M, Bressman S, Park A, Lu C, Chen N, Wang A. Anti-Tumor necrosis factor therapy and incidence of Parkinson disease among patients with inflammatory bowel disease. JAMA Neurol. 2018;75:939–946. doi: 10.1001/jamaneurol.2018.0605. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 36.Akhtar RS, Licata JP, Luk KC, Shaw LM, Trojanowski JQ, Lee VM. Measurements of auto-antibodies to α-synuclein in the serum and cerebral spinal fluids of patients with Parkinson's disease. J Neurochem. 2018;145:489–503. doi: 10.1111/jnc.14330. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 37.Bach JP, Falkenburger BH. What autoantibodies tell us about the pathogenesis of Parkinson's disease: An Editorial for ‘Measurements of auto-antibodies to α-synuclein in the serum and cerebral spinal fluids of patients with Parkinson's disease’ on page 489. J Neurochem. 2018;145:433–435. doi: 10.1111/jnc.14340. [DOI] [PubMed] [Google Scholar]
- 38.Sulzer D, Alcalay RN, Garretti F, Cote L, Kanter E, Agin-Liebes J, Liong C, McMurtrey C, Hildebrand WH, Mao X, et al. T cells from patients with Parkinson's disease recognize α-synuclein peptides. Nature. 2017;546:656–661. doi: 10.1038/nature22815. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 39.Sabatino JJ Jr, Pröbstel AK, Zamvil SS. B cells in autoimmune and neurodegenerative central nervous system diseases. Nat Rev Neurosci. 2019;20:728–745. doi: 10.1038/s41583-019-0233-2. [DOI] [PubMed] [Google Scholar]
- 40.Brochard V, Combadière B, Prigent A, Laouar Y, Perrin A, Beray-Berthat V, Bonduelle O, Alvarez-Fischer D, Callebert J, Launay JM, et al. Infiltration of CD4+ lymphocytes into the brain contributes to neurodegeneration in a mouse model of Parkinson disease. J Clin Invest. 2009;119:182–192. doi: 10.1172/JCI36470. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 41.Orr CF, Rowe DB, Mizuno Y, Mori H, Halliday GM. A possible role for humoral immunity in the pathogenesis of Parkinson's disease. Brain. 2005;128(Pt 11):2665–2674. doi: 10.1093/brain/awh625. [DOI] [PubMed] [Google Scholar]
- 42.Collins LM, Toulouse A, Connor TJ, Nolan YM. Contributions of central and systemic inflammation to the pathophysiology of Parkinson's disease. Neuropharmacology. 2012;62:2154–2168. doi: 10.1016/j.neuropharm.2012.01.028. [DOI] [PubMed] [Google Scholar]
- 43.Kustrimovic N, Comi C, Magistrelli L, Rasini E, Legnaro M, Bombelli R, Aleksic I, Blandini F, Minafra B, Riboldazzi G, et al. Parkinson's disease patients have a complex phenotypic and functional Th1 bias: Cross-sectional studies of CD4+ Th1/Th2/T17 and Treg in drug-naïve and drug-treated patients. J Neuroinflammation. 2018;15(205) doi: 10.1186/s12974-018-1248-8. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 44.Kara SP, Altunan B, Unal A. Investigation of the peripheral inflammation (neutrophil-lymphocyte ratio) in two neurodegenerative diseases of the central nervous system. Neurol Sci. 2022;43:1799–1807. doi: 10.1007/s10072-021-05507-5. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 45.Huda R. Inflammation and autoimmune myasthenia gravis. Front Immunol. 2023;14(1110499) doi: 10.3389/fimmu.2023.1110499. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 46.Wang Q, Luo Y, Ray Chaudhuri K, Reynolds R, Tan EK, Pettersson S. The role of gut dysbiosis in Parkinson's disease: Mechanistic insights and therapeutic options. Brain. 2021;144:2571–2593. doi: 10.1093/brain/awab156. [DOI] [PubMed] [Google Scholar]
- 47.Kapoor B, Gulati M, Gupta R, Singla RK. Microbiota dysbiosis and myasthenia gravis: Do all roads lead to Rome? Autoimmun Rev. 2023;22(103313) doi: 10.1016/j.autrev.2023.103313. [DOI] [PubMed] [Google Scholar]
- 48.Chen P, Tang X. Gut Microbiota as Regulators of Th17/Treg balance in patients with myasthenia gravis. Front Immunol. 2021;12(803101) doi: 10.3389/fimmu.2021.803101. [DOI] [PMC free article] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Data Availability Statement
The data generated in the present study may be requested from the corresponding author.