

This 8-month-old boy (Fig. 1) was admitted for evaluation of progressive hypotonia and failure to thrive, with a weight well below the fifth percentile for his age despite a normal food intake. He was born at 37 weeks' gestation after an uncomplicated vaginal birth, and there were no concerns about his growth or development until 7 months, when the family physician realized that the boy had been regressing developmentally over the last month. He was not yet sitting, had almost stopped rolling over and had decreased head control. There was no history of seizures or serious illnesses. Neurological examination revealed a marked central and peripheral hypotonia and normal deep tendon reflexes in his arms and legs. His skin was dry and lax, and his hair was quite coarse and wiry (Fig. 2). There were no abnormal birthmarks. The complete blood count and levels of electrolytes, calcium, magnesium, phosphate, albumin, prealbumin, total protein, liver enzymes, blood urea nitrogen and creatinine were all within normal limits. The serum copper level was 7.1 (normally 11–28) μmol/L, and the ceruloplasmin level was 120 (normally 170–660) mg/L. Examination of a strand of hair under light microscopy (Fig. 3) revealed a twisted, hypopigmented shaft.

Figure 1. Photo: Courtesy: Erik Swartz

Figure 2. Photo: Courtesy: Erik Swartz
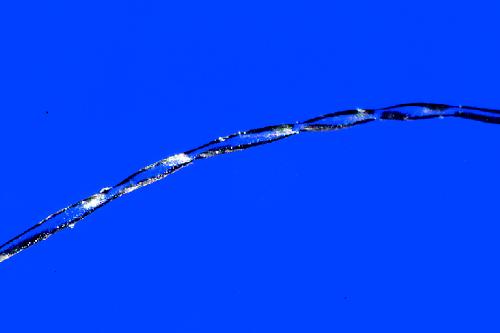
Figure 3. Photo: Courtesy: Erik Swartz
Menkes' syndrome (also known as kinky-hair syndrome) was diagnosed, and investigations were initiated to identify other features consistent with the disease. Ultrasonography of the bladder showed several small diverticula. A skeletal survey revealed wormian bones (small irregular bones along the cranial sutures), incomplete fusion of the thoracic vertebrae and metaphyseal sclerosis of the humeri and femora. Magnetic resonance angiography showed marked tortuosity of the right vertebral, internal carotid and middle and anterior cerebral arteries. The boy began to receive daily subcutaneous injections of copper histidine and, 6 months later, he continues to be followed by his pediatrician and our metabolic diseases team.
Menkes' syndrome is an X-linked recessive genetic disorder of copper metabolism first described in 1962.1,2 It is a rare condition (incidence rate of 1 in 298 000 live births).3 Mutations in the ATP7A gene, which encodes a copper membrane transporter protein,4 lead to deficiencies in intestinal absorption of copper and in intracellular processing of copper in the central nervous system and connective tissues, where enzymes requiring copper as a cofactor no longer function properly.
Clinical manifestations usually begin within the first 1–2 months of life and include failure to thrive due to feeding difficulties, twisted hair (pili torti, also described as “coarse” or “steely” hair), skin laxity, joint hypermobility, cerebral vessel tortuosity, bladder diverticula, osteoporotic bones with flared metaphyses (there may also be wormian bones) and progressive cerebral atrophy (leading to mental retardation, seizures, hypotonia and optic atrophy).5 The condition is suspected in infants with low serum copper and ceruloplasmin levels and is confirmed by means of copper uptake studies on fibroblast cultures. Menkes' syndrome is characterized by progressive deterioration, and death usually occurs by 3 years of age.
Oral copper treatment is not effective, but subcutaneous injections of copper histidine appear to provide encouraging results in preventing neurodegeneration and prolonging survival,6 especially if started within 1 month of life. Copper treatment unfortunately does not prevent the connective tissue complications associated with the syndrome, and many patients subsequently die of these complications.
Erik N. Swartz Resident in Pediatrics University of Alberta Edmonton, Alta.
Footnotes
[Permission was obtained from the boy's family to not conceal his face.]
References
- 1.Menkes JH, Alter M, Steigleder GK, Weakley DR, Sung JH. A sex-linked recessive disorder with retardation of growth, peculiar hair and focal cerebral and cerebellar degeneration. Pediatrics 1962;29:764-79. [PubMed]
- 2.Bankier A. Menkes disease. J Med Genet 1995; 32:213-5. [DOI] [PMC free article] [PubMed]
- 3.Tonnesen T, Kleijer WJ, Horn N. Incidence of Menkes disease. Hum Genet 1991;86:408-10. [DOI] [PubMed]
- 4.Vulpe C, Levinson B, Whitney S, Packman S, Gitschier J. Isolation of a candidate gene for Menkes disease and evidence that it encodes a copper-transporting ATPase. Nature Genet 1993; 3: 7-13. [DOI] [PubMed]
- 5.Tumer Z, Horn N. Menkes disease: recent advances and new aspects. J Med Genet 1997;34: 265-74. [DOI] [PMC free article] [PubMed]
- 6.Christodoulou J, Danks DM, Sarkar B, Baerlocher KE, Casey R, Horn N, et al. Early treatment of Menkes disease with parenteral copper-histidine: long-term follow-up of four treated patients. Am J Med Genet 1998;76:154-64. [PubMed]