

Abstract
Purpose
We aimed to design, develop, and evaluate an internet of things-enabled patch (IoT patch) for real-time remote monitoring of adherence (or patch wear time) during patch treatment in child participants in clinical trials. This study provides healthcare providers with a tool for objective, real-time, and remote assessment of adherence and for making required adjustments to treatment plans.
Methods
The IoT patch had two temperature microsensors and a wireless chip. One sensor was placed closer to the skin than the other, resulting in a temperature difference depending on whether the patch was worn. When the patch was worn, it measured temperatures every 30 seconds and transmitted temperature data to a cloud server via a mobile application every 15 seconds. The patch was evaluated via 2 experiments with 30 healthy adults and 40 children with amblyopia.
Results
Excellent monitoring accuracy was observed in both adults (mean delay of recorded time data, 0.4 minutes) and children (mean, 0.5 minutes). The difference between manually recorded and objectively recorded patch wear times showed good agreement in both groups. Experiment 1 showed accurate monitoring over a wide range of temperatures (from 0 to 30°C). Experiment 2 showed no significant differences in wearability (ease-of-use and comfort scores) between the IoT and conventional patches.
Conclusions
The IoT patch offers an accurate, real-time, and remote system to monitor adherence to patch treatment. The patch is comfortable and easy to use. The utilization of an IoT patch may increase adherence to patch treatment based on accurate monitoring.
Translational Relevance
Results show that the IoT patch can enable real-time adherence monitoring in clinical trials, improving treatment precision, and patient compliance to enhance outcomes.
Keywords: occlusion therapy, strabismus, compliance, amblyopia, microsensor
Introduction
Patch treatment is commonly used for amblyopia and strabismus.1,2 In this treatment, high adherence is key to achieving optimal treatment outcomes.3 However, it is challenging to ensure that patients adhere to the prescribed therapy duration. Objective monitoring of adherence can be helpful in addressing this challenge. Such monitoring would help identify barriers to adherence and enable healthcare providers to develop targeted interventions to improve adherence.4,5 It can also improve our understanding of the optimal duration of therapy for enhanced visual and developmental treatment outcomes.5,6
Currently, adherence is often monitored through parental reports.7 This approach has limitations because of potential inaccuracies in reporting and inconsistencies over time. In addition, reporting may be unreliable or incomplete during periods when the child is in the care of someone else, for example, when at school or day care. To address these limitations, previous studies have explored the use of electronic devices for objective monitoring of patch treatments.8,9 Various methods, including electrocardiographic electrodes or temperature sensors under a patch, have been applied.8,10 However, these methods have practical limitations: (1) they need a separate reading station for analyzing stored data; (2) they lack a data transmission function, thereby preventing real-time remote monitoring of adherence; and (3) monitoring is unreliable in extreme ambient temperatures (e.g. 0°C or 30°C).
The integration of internet of things (IoT) technology in patch treatments can be a promising solution to these limitations.11 An IoT-enabled patch (or IoT patch) can enable real-time remote monitoring of patch usage while allowing to objectively assess adherence and adjust the treatment plan as necessary.11 This study seeks to contribute to the advancement of patch treatment by integrating IoT technology in patch treatments.
In this study, we designed an IoT patch with a wireless chip and two temperature microsensors that periodically detect skin contact and wirelessly transmit contact information to smartphones (or cloud servers via smartphones), allowing for accurate, real-time, and objective monitoring of adherence. In our design, one sensor was placed closer to the skin than the other, resulting in a temperature difference depending on whether the patch was worn. This approach allows for reliable accuracy over a wide range of environmental temperatures. In this study, we evaluated the accuracy and wearability of an IoT patch for the real-time monitoring of occlusion therapy in children with amblyopia.
Methods
For the real-time monitoring of patch wear time (or adherence to patch treatment) using IoT patches, two experiments were conducted. The first experiment was conducted to analyze the effect of environmental temperature on the accuracy of monitoring the patch wear time. The second experiment was conducted to analyze the accuracy and wearability of the patch. This study complies with the tenets of the Declaration of Helsinki, and its protocol and informed consent forms were approved by the institutional review board of Kangwon National University Hospital (KNUH-B202207-013-003 and KNUH-A-2022-06-006-004). Informed consent was obtained from the adult participants, the parent, or guardian of child participants aged 7 to 12 years, and child participants themselves. Only participants and their guardians who fully understood the nature of the study and agreed to participate were included.
Study Materials (IoT Patch)
We designed and developed an IoT patch with two built-in temperature microsensors that enabled real-time monitoring of patch wear time by periodically detecting skin contact with the sensors. As shown in Figure 1, one sensor (skin temperature sensor) was located closer to the skin than the other (ambient temperature sensor). The underlying concept of skin contact detection is that when the patch is worn, the values of the skin temperature sensor are higher than the values of the ambient temperature sensor, and thus, the difference between the values of the sensors increases. However, when the patch is not worn, the difference decreases.
Figure 1.

IoT Patch. (1) Disposable occlusion patch and (2) non-disposable miniature motherboard. The miniature motherboard can be adhesively attached to, or easily detached from, the occlusion patch.
The IoT patch consists of a disposable occlusion patch and a non-disposable miniature motherboard. The patch was made from the same material as a commercially available patch, with a small modification made to the shape. The patch had additional spaces with a hole encircled by circular adhesive parts. These parts allow the motherboard to be adhesively attached in a releasable manner ensuring easy detachability. When not attached, the motherboard is in sleeping mode (or low battery mode). When the motherboard is attached, it automatically wakes up from sleep mode, switches to active mode, and periodically measures and wirelessly transmits ambient and skin temperatures. When the patch operates in active mode for 8 hours per day (e.g. 8 hours of daily patching), the battery lasts for 126 days. When continuously operating in the active mode (e.g. 24 hours of daily patching), the battery lasts for 42 days. When the battery is running low, a notification is displayed in the application.
The size of the motherboard was 22.3 mm × 18.6 mm, and the weight was 2 g. The board comprised two built-in temperature microsensors, a Bluetooth low-energy (BLE) chip, and a coin battery. One sensor was placed at the bottom of the board to measure the skin temperature. Another sensor was placed at the top of the board to measure the ambient temperature. It took 2 seconds for the sensors to respond to a change in environmental temperature. The BLE chip and battery were placed between the two sensors. The cost of the board is US $60 per unit.
The temperatures were measured every 30 seconds by both sensors and wirelessly transmitted to a mobile application once every 15 seconds using the BLE chip. For the first use, before the patch begins wirelessly transmitting data, the application must be manually activated. After this first activation, it operates continuously in the background, eliminating the need for further manual activation. Before our experiments, during the development process, we confirmed that wireless communication between the application and the IoT patch operated continuously for more than a day.
Once the application received the temperature data, it classified the patch wearing status using a threshold equation (see Results section) and remotely transmitted the temperatures and the status to a cloud server. Using the classified patch wearing status, the patch wear time was calculated. When the patch wearing status was calculated as being worn, 15 seconds were added to the current patch wear time. The application also allowed adherence information (two temperature values) to be exported as comma-separated values (*.csv format).
Experiment 1: Effect of Environmental Temperatures on Accuracy of Monitoring Patch Wear Time
To analyze the effect of environmental temperatures on the accuracy of monitoring IoT patch wear time, 30 adult participants were recruited. Participants were eligible if they were healthy and aged 18 to 65 years. After obtaining consent, the participants were asked to wear the IoT patch for 8 minutes in rooms with room temperatures of 0, 15, 25, 30, and 40°C. They entered the room at each temperature and waited for 8 minutes. After the waiting period, they wore the patch for 8 minutes and then removed it, followed by another 3-minute waiting period. Next, they took a 20-minute break in a room with an average temperature of 25°C.
Experiment 2: Accuracy and Wearability of Monitoring Patch Wear Time
To assess the accuracy of real-time remote IoT patch wear time monitoring and patch wearability, 40 child participants (12 girls and 19 boys; age = 7–12 years) were recruited. Exclusion criteria were the presence of ophthalmic and systemic diseases and previous optic nerve diseases, such as glaucoma. After consent was obtained, the child participants wore either the IoT patch or a commercially available patch in a room with normal temperatures (21–26°C). Subsequently, they wore the other patch they had not previously worn for an equal duration in the same room. The order of patch wearing was randomly assigned. The patch wear time was randomly selected as 30, 45, and 60 minutes. After wearing each patch, as shown in the Table, participants completed a 12-item questionnaire. The questionnaire includes 6 items each for measuring ease-of-use and comfort, with responses provided on a 5-point Likert scale.
Table.
The 12-Item Questionnaire to Measure Wearability
| Category | Questions |
|---|---|
| Ease-of-use | The patch is hard to wear (R) |
| The patch sticks on well | |
| The patch is too large (R) | |
| It is easy to wear the patch and my glasses at the same time | |
| I can peek through the patch | |
| I have trouble keeping the patch on (R) | |
| Comfort | The patch is comfortable |
| My skin is red or sore after I take the patch off (R) | |
| It hurts when I take the patch off (R) | |
| It feels heavy when I put on the patch (R) | |
| I am reluctant to put on the patch (R) | |
| The eye patch does not touch my eyelid or eyelashes |
Each item is rated on a scale from “strongly disagree” (1 point), “disagree” (2 points), “neither agree nor disagree” (3 points), “agree” (4 points), to “strongly agree” (5 points).
(R) indicates questions that are scored in reverse, ranging from strongly disagree (5 points) to strongly agree (1 point).
Statistical Analysis
The temperature differences comparison analysis across environmental temperatures and questionnaire for wearability comparison analysis of the IoT patch versus the commercial patch was analyzed by repeated measures ANOVA. For the comparison, we calculated and used the average value of the total sum of six items for each category (ease of use or comfort). For the effect size, we measured and reported Cohen's d. The accuracy of the sensor-based wear time judgment technique was analyzed by the Bland–Altman plot.
Results
Experiment 1: Effect of Environmental Temperatures on the Accuracy of Monitoring Patch Wear Time
Our study yielded promising results for skin-contact detection (e.g. by determining whether the IoT patch is worn), particularly in conditions where the environmental (or room) temperatures ranged from 0°C to 30°C. However, it was unreliable when the environmental temperature was extremely high (i.e. 40°C). As shown in Figure 2, when the patch was not worn, the skin sensor temperatures were comparable to the ambient sensor temperatures. Statistical analysis indicated no significant differences in temperature differences between both sensor temperatures across environmental temperatures (F (1, 28) = 0.10, P = 0.75). Before the patch was worn, the average temperature differences (SD) between ambient and skin sensor temperatures were −0.17°C (1.16), −0.17°C (0.81), 0.06°C (0.51), 0.01°C (0.68), and −0.23°C (0.49) at environmental temperatures of 0°C, 15°C, 25°C, 30°C, and 40°C, respectively. In contrast, there were noticeable temperature differences when the patch was worn. Statistical analysis indicated significant differences in temperature differences across environmental temperatures (F (1, 28) = 633.55, P < 0.001). Furthermore, the difference decreased as the environmental temperature increased, ultimately reaching almost zero at an environmental temperature of 40°C. During the times that the patch was worn, the average temperature differences (SD) were 5.92°C (1.27), 4.43°C (1.30), 2.58°C (0.56), 1.85°C (0.64), and -0.52°C (0.49) at environmental temperatures of 0°C, 15°C, 25°C, 30°C, and 40°C, respectively.
Figure 2.

Temperature differences between ambient and skin sensor temperatures. Temperature differences were noticeable when environmental temperature was not extremely high.
Overall, the above-mentioned findings provided an important insight for patch wearing status (i.e. detecting skin contact with the IoT patch) at various environmental temperatures and led to the development of the following threshold equation: −0.15 × ambient sensor temperature + 5.87 = threshold. To develop this threshold equation, we conducted a linear regression analysis. In this analysis, the difference between ambient and skin sensor temperatures was included as the independent variable, whereas the ambient sensor temperature was treated as the dependent variable. This equation demonstrates the correlation between the temperature difference and patch wearing status based on the ambient sensor temperature, as shown in Figure 3. Using this equation, if the difference between ambient and skin sensor temperatures was greater than or equal to the threshold (or the equation result), the patch wearing status was classified as being worn. As shown in Figure 3, for environmental temperature conditions below 40°C, we were able to accurately identify the patches that were being worn. Agreements between calculated and manually recorded patch wearing status were 99% when the 40°C temperature condition was excluded. When including the 40°C environmental temperature condition, the agreement was 88%.
Figure 3.
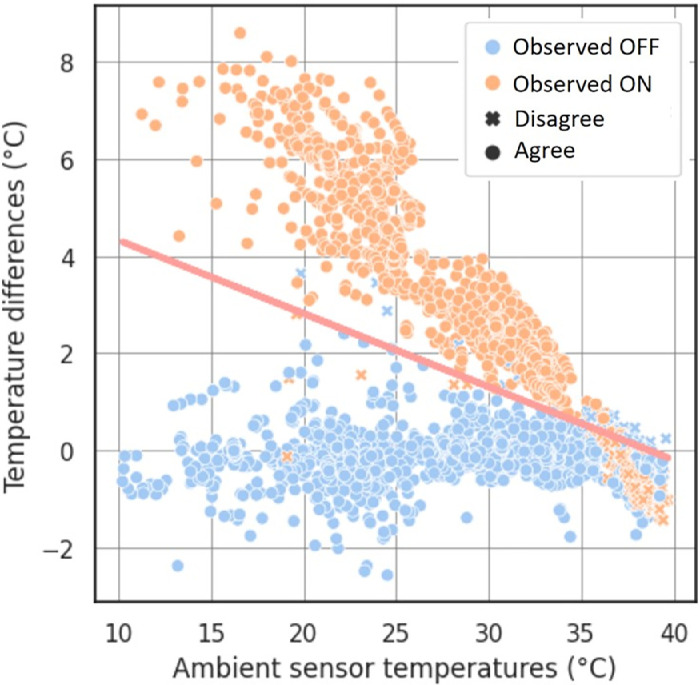
The threshold analysis plot from participants in experiment 1. Demonstrating good agreement between the manually recorded (observed ON/OFF) and the calculated patch-wearing status when ambient sensor temperatures were not extremely high.
Using the classified patch wearing status data, we calculated patch wear times and compared them with manually recorded patch wear times. Because temperatures were measured every 30 seconds, when the patch wearing status was identified as being worn, we calculated the time assuming that the patient had been wearing the patch for the past 30 seconds. The calculated patch wear times were highly accurate in that the times were comparable to the manually recorded times. The average calculated patch wear times (SD) were 482.07 seconds (11.14), 477.93 seconds (11.14), 481.03 seconds (12.63), 480.00 seconds (8.02), and 168.75 seconds (179.96) at environmental temperatures of 0°C, 15°C, 25°C, 30°C, and 40°C, respectively. Given that the IoT patch actually was worn for 480 seconds at each different environmental temperature condition, the average differences in the calculated patch wear times and manually recorded patch wear times were 2.07 seconds (11.14), -2.07 seconds (11.14), -1.03 seconds (12.63), 0 (8.02) and -311.25 seconds (180.00) at environmental temperatures of 0°C, 15°C, 25°C, 30°C, and 40°C, respectively.
Experiment 2: Accuracy of Real-Time Remote Monitoring of Patch Wear Time and Wearability of the Patch
Accuracy
The subjects comprised 21 girls and 19 boys aged between 5 and 12 years (mean age = 8.1 ± 2.0). Excellent accuracy of real-time remote patch wear time monitoring was observed among participants (mean delay of recorded time data = 0.4 minutes; Fig. 4).
Figure 4.

Image (a) shows agreement between manually recorded and cloud-recorded patch wear times. The upper and lower dotted lines show the 95% limit of agreement. The half-width of the 95% limit of agreement was ±1.37 minutes (range = −1.81 to –0.93 minutes). Image (b) shows manually recorded and cloud-recorded patch wear times.
Our application wirelessly received skin and ambient sensor temperatures from an IoT patch, classified patch wearing status using the equation, and remotely transmitted the temperatures and status to a cloud server. The patch wear time was calculated based on the patch-wearing status data in a cloud server. The difference in patch wear time between manual recording and cloud recording showed good agreement. In other words, as shown in Figure 4a, Bland–Altman analysis showed excellent precision, with a 95% limit of agreement (LoA) and half-width of 0.8 minutes.
The average room temperature at which each procedure was performed was 23.6 ± 1.2°C (range = 21.0–25.5°C). As shown in Figure 4b, the mean delay of attachment and detachment time was 0.7 ± 0.4 minutes (range = 8–113 seconds) and 1.2 ± 0.5 minutes (range = 30–140 seconds), respectively. The manually recorded and cloud-recorded times showed a strong positive correlation (R = 0.998, P < 0.001). In addition, there was no significant difference in absolute duration error between the recorded times (R = 0.072, P = 0.098).
Wearability
There was no statistical difference in wearability between the IoT and conventional patches. The ease-of-use score among children using the IoT patch (14.18 ± 2.29) was higher than that of the conventional patch (13.95 ± 2.17,)(F (1, 39) = 1.34, P = 0.25). The effect size was d = 0.18. Whereas the comfort score for the IoT patch (15.33 ± 2.89) was higher than that of the conventional patch (15.25 ± 2.56, F (1, 39) = 0.05, P = 0.83). The effect size was d = 0.03.
Discussion
In this study, we designed and developed an IoT patch to remotely monitor patch wear time (or the adherence to patch treatment) in real time. In particular, the IoT patch was designed to allow the separation of the sensor parts from the conventional eye patch shape, allowing it to be used in conjunction with disposable eye patches. The IoT patch and its mobile application were found to be reliable for real-time remote monitoring of patch wear time at varying environmental temperatures when the environmental temperatures were not extremely high (i.e. 40°C). The difference between manually recorded and cloud-recorded patch wear times was no more than 1.5 minutes. Furthermore, the accuracy of detecting patch wearing status (or skin contact) using the IoT patch was not impacted by the total patch wearing time, the age of the child, or the environmental temperature (between 0 and 30°C).
Our IoT patch is the first eye patch to utilize a real-time data collection system. The skin and ambient temperature sensor data were wirelessly transmitted to our mobile application via Bluetooth, and temperature data and patch wearing status were remotely transmitted to a cloud server via the application. IoT technology is widely used in the medical field, for example, in wearable devices that can continuously monitor vital signs, including heart rate, blood pressure, and oxygen levels.12 The collected data are sent to a secure cloud platform for remote access and analysis by healthcare providers, enabling the early detection of anomalies and informed treatment decision making.13
To monitor objective patch adherence, researchers from the United Kingdom and the Netherlands developed an occlusion dose monitor (ODM).2,5,14 In the ODM developed in the United Kingdom, skin electrodes were placed beneath the patch to monitor skin resistance.14 The ODM developed in the Netherlands used a disk attached to the top of the patch to measure temperature changes and monitor patch adherence.8,15,16 However, given that these ODMs are not available worldwide, the TheraMon microsensor (Hargelsberg, Austria) was subsequently developed, which was originally intended for use in dentistry and was proposed for patch adherence monitoring in 2013.10,17
The TheraMon microsensor has the advantages of a long battery life and a small size for measuring skin temperature.18 However, when using the TheraMon microsensor for patch treatment monitoring, there is a concern about discomfort because of the requirement of direct contact of the microsensor to the skin.19 In addition, there are limitations in that (1) a separate reading station is required and (2) real-time data cannot be transmitted to mobile devices or cloud servers.10 The IoT patch is hygienic as its occlusion patch (the part attached to the patient's skin) is disposable, and its body (miniature motherboard) can be attached and detached from the outside of the occlusion patch.20 It enables real-time data transmission. Accordingly, there is no need to purchase any additional items besides the IoT device.17 In addition, remote access is feasible, allowing for making adjustments to the treatment plan as necessary.
The IoT patch accurately measures patch wear time even when environmental temperatures are low (e.g. 0°C). Although previously developed patches relied on measuring skin temperatures to monitor patch adherence, there was potential for loss of accuracy in extreme environmental temperatures owing to the mechanism of temperature measurement.10 To overcome this limitation, the IoT patch incorporates two temperature microsensors that measure both internal and external temperatures (or skin and ambient temperatures), allowing for the evaluation of patch wearing status by comparing the difference between the two.
Previous studies on ODM did not examine accuracy in cold temperatures (e.g. 0°C).8,9,14 A previous study using a TheraMon microsensor showed unreliable accuracy when environmental temperatures were lower than 7°C (or 45 F).10 Our IoT patch demonstrated excellent accuracy even at 0°C because it does not depend on the absolute value of skin temperature. Another study using a TheraMon microsensor showed low accuracy at high environmental temperatures of 27.7°C (82F) or higher. Our IoT patch demonstrated excellent accuracy at 30°C. However, our accuracy was also low when environmental temperatures were extremely high (i.e. 40°C).
The IoT patch demonstrated good real-time data transmission. There was no significant loss of data during patch treatment. The patches developed in previous studies sampled data every 5 or 10 minutes to prevent battery loss.9,10 Therefore, these patches could not record the patch wear time (or adherence) of 5 or 10 minutes when a child transitioned from wearing the patch to removing (not wearing) it, or vice versa. As a result, the error range of monitored treatment time in previous studies was much greater, 6.4 minutes, than that in our study. The IoT patch samples data every 30 seconds and transmits it in real time, resulting in very high accuracy. In addition, this result was not affected by temperature fluctuations.
The IoT patch demonstrated no difference in wearability compared with a conventional (or commercially available) patch. Wearability was evaluated in children who were the primary users of the conventional patch, indicating the excellent feasibility of the IoT patch in a clinical setting. Patches in previous studies could be considered complex and difficult to use, requiring specialized training for the patient and clinician.5 Given that for an IoT patch, an occlusion patch is attached to the skin and a device is attached externally, the IoT patch can be easily used by caregivers without any special skills.
Although this study made the first step toward real-time remote monitoring of adherence to patch treatment, our results should be carefully interpreted because of the following limitations. First, we included only 30 adult and 40 child participants.
This result may not be representative of a larger population, owing to the small study sample size. Second, we confirmed that during the development process, the IoT patch operates continuously for more than a day. However, further study is required to verify the reliability of the patch in monitoring adherence when worn for extended periods by children engaging in activities involving vigorous movements. Third, the high cost of implementing this technology in clinical settings is a hindrance to its widespread usage. Efforts to reduce the manufacturing cost and simplify the manufacturing process of the device are necessary to make it largely accessible and promote daily use. In addition, there may be privacy and security concerns regarding the handling of sensitive medical data collected by an IoT patch. Finally, in previous studies, the accuracy was affected by high ambient temperatures (>33°C). The IoT patch also showed a decrease in accuracy at ambient temperatures >30°C.
This study contributes to the advancement of patch treatment by integrating IoT technology into patch treatments. Our results indicate that the IoT patch can be a promising solution to remotely and accurately monitor patient adherence in real time, enabling adjustments to treatment plans as needed. In addition, by conducting a thorough analysis of the newly developed IoT patch, this study provided valuable information for both healthcare professionals and technology developers to assist in their efforts toward improving patient outcomes and advancing the field of amblyopia treatment.
Acknowledgments
Supported by an Institute for Information & Communications Technology Planning & Evaluation (IITP) grant funded by the Korea government (MSIT; No. 2022-0-01196, Regional strategic Industry convergence security core talent training business).
Disclosure: J. Hwang, None; K.-S. Jo, None; M.-S. Kim, None; S. Choi, None; J. Lee, None; A. Kim, None; Y.-J. Yoo, None
References
- 1. Pediatric Eye Disease Investigator Group, Wallace DK, Lazar EL, et al.. A randomized trial of increasing patching for amblyopia. Ophthalmology. 2013; 120: 2270–2277. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2. Wallace MP, Stewart CE, Moseley MJ, et al.. Compliance with occlusion therapy for childhood amblyopia. Invest Ophthalmol Vis Sci. 2013; 54: 6158–6166. [DOI] [PubMed] [Google Scholar]
- 3. Pradeep A, Proudlock FA, Awan M, Bush G, Collier J, Gottlob I.. An educational intervention to improve adherence to high-dosage patching regimen for amblyopia: a randomised controlled trial. Br J Ophthalmol. 2014; 98: 865–870. [DOI] [PubMed] [Google Scholar]
- 4. Awan M, Proudlock FA, Gottlob I.. A randomized controlled trial of unilateral strabismic and mixed amblyopia using occlusion dose monitors to record compliance. Invest Ophthalmol Vis Sci. 2005; 46: 1435–1439. [DOI] [PubMed] [Google Scholar]
- 5. Stewart CE, Moseley MJ, Georgiou P, Fielder AR.. Occlusion dose monitoring in amblyopia therapy: status, insights, and future directions. J AAPOS. 2017; 21: 402–406. [DOI] [PubMed] [Google Scholar]
- 6. Stewart CE, Moseley MJ, Stephens DA, Fielder AR.. Treatment dose response in amblyopia therapy: the Monitored Occlusion Treatment of Amblyopia Study (MOTAS). Invest Ophthalmol Vis Sci. 2004; 45: 3048–3054. [DOI] [PubMed] [Google Scholar]
- 7. Drews-Botsch CD, Celano M, Kruger S, Hartmann EE.. Adherence to occlusion therapy in the first six months of follow-up and visual acuity among participants in the Infant Aphakia Treatment Study (IATS). Invest Ophthalmol Vis Sci. 2012; 53: 3368–3375. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8. Fronius M, Bachert I, Luchtenberg M.. Electronic monitoring of occlusion treatment for amblyopia in patients aged 7 to 16 years. Graefes Arch Clin Exp Ophthalmol. 2009; 247: 1401–1408. [DOI] [PubMed] [Google Scholar]
- 9. Gharebaghi AH, Heidary F, Gharebaghi R, Heidary R.. Mehdi-ODM; a modified digital monitoring of the occlusion therapy for amblyopia. Graefes Arch Clin Exp Ophthalmol. 2011; 249: 945–946; author reply 947–948. [DOI] [PubMed] [Google Scholar]
- 10. Wang J, Xu H, De La, et al.. Improved monitoring of adherence with patching treatment using a microsensor and Eye Patch Assistant. J AAPOS. 2020; 24: 96e91–96e97. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11. Madakam S, Ramaswamy R, Tripathi S.. Internet of things (IoT): a literature review. Journal of Computer and Communications. 2015; 3(5): 164–173. [Google Scholar]
- 12. Sharma A, Badea M, Tiwari S, Marty JL.. Wearable biosensors: an alternative and practical approach in healthcare and disease monitoring. Molecules. 2021; 26: 748. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13. Abawajy JH, Hassan MM.. Federated internet of things and cloud computing pervasive patient health monitoring system. IEEE Communications Magazine. 2017; 55: 48–53. [Google Scholar]
- 14. Fielder AR, Irwin M, Auld R, Cocker KD, Jones HS, Moseley MJ.. Compliance in amblyopia therapy: objective monitoring of occlusion. Br J Ophthalmol. 1995; 79: 585–589. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15. Fronius M, Chopovska Y, Nolden J, et al.. Occlusion treatment for amblyopia: assessing the performance of the electronic occlusion dose monitor. Strabismus. 2006; 14: 65–70. [DOI] [PubMed] [Google Scholar]
- 16. Loudon SE, Fronius M, Looman CW, et al.. Predictors and a remedy for noncompliance with amblyopia therapy in children measured with the occlusion dose monitor. Invest Ophthalmol Vis Sci. 2006; 47: 4393–4400. [DOI] [PubMed] [Google Scholar]
- 17. Januschowski K, Bechtold TE, Schott TC, et al.. Measuring wearing times of glasses and ocular patches using a thermosensor device from orthodontics. Acta Ophthalmol. 2013; 91: e635–e640. [DOI] [PubMed] [Google Scholar]
- 18. Miller JM, Dennis LK, Hsu CH, Harvey EM.. Objective assessment of spectacle wear in infants and toddlers using a wearable sensor. Transl Vis Sci Technol. 2021; 10: 29. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19. Schramm C, Abaza A, Blumenstock G, et al.. Limitations of the TheraMon((R)) -microsensor in monitoring occlusion therapy. Acta Ophthalmol. 2016; 94: e753–e756. [DOI] [PubMed] [Google Scholar]
- 20. Januschowski K, Rickmann A, Emmerich C, et al.. The use of a microsensor in therapy of amblyopia. Klin Monbl Augenheilkd. 2019; 236: 1170–1173. [DOI] [PubMed] [Google Scholar]