

Abstract
Background
Information on the determinants of ill-health among elderly, if available, would certainly provide a useful guide to policy makers in their plan for appropriate interventions for this subgroup of the population. This study therefore assessed ill-health status and its associated factors among the elderly in Osun State Nigeria.
Methodology
The study design was a descriptive cross-section involving 491 elderly drawn from a simple random sample of five local government areas LGAs in Osun State Nigeria, in 2017. Self-reported illness (es) two weeks before the survey was taken as measure of ill-health among the elderly. Bivariate and multivariate statistical methods were used for data analysis, p< 0.05 was reckoned statistically significant.
Results
Overall, 228 (46.4%) reported one health issue or the other two weeks before the survey. Regular source of income [OR=0.63, 95% CI=0.43, 0.95], ever smoked [OR=2.35, 95% CI=1.31, 4.21] and having any source of worry [OR=2.52, 95% CI=1.68, 3.79] were significantly associated with self-reported ill-health among elderly. Whereas, having regular source of income, engaging in physical exercise, and being satisfied with residential status were all found to be protective against illnesses by crude statistical analysis, only having a source of regular income had independent protective association against illness.
Conclusions
Prevalence of ill-health among elderly was considerably high. Factors significantly associated with ill-health include not having a regular source of income, ever smoked, and having any source of worry. Financial empowerment schemes and health education for elderly on harmful effect of smoking and excessive worrying on their health are hereby recommended.
Keywords: Elderly, Ill-Health, Determinants
Introduction
Globally, the proportion of people aged 60 years and above is growing faster than the other age groups. Between 2000 and 2050, the proportion of the world's population over 60 years will double from about 11% to 22% with absolute increase in number from 605 million to 2 billion over the same period (1). This increase in the proportion of the elderly has been projected to occur more in developing countries, including Nigeria. Improvement in certain health indices, which include control of perinatal and infant mortality, a decline in birth rates, improvement in nutritional status, basic health care, and the control of many infectious diseases is responsible for an increasing number and proportion of persons surviving into advanced stages of life (2).
Currently, in Nigeria life expectancy for male individuals is 51 years and 53 years for female (3,4).
Increase in life expectancy has been associated with increasing prevalence of chronic diseases, disability dependent life, increased cost of health care and increased utilization of health care services (5). As many individuals can now look forward to longer lives, the risk of having at least one chronic disease increases. Older people are prone to non-communicable diseases such as heart disease, cancer, and diabetes, rather than from infectious and parasitic diseases. In addition to several medical problems, such as co-morbidity of diabetes and hypertension, older people are often faced with social and mental health problems (1). The rise in number and proportion of older people has led to concerns about societal and health consequences. The increasing number of elderly persons and their attendant health problems have implication on public health programs in developing countries including Nigeria.
The health needs of older citizens need to be addressed as their vulnerability is reflected in a higher ill-health burden and disability (6). However, there is limited information on morbidity pattern of the elderly residing in the urban and rural areas of Nigeria. As a greater proportion of the population survives to very old ages, the public health impact of the burden of disease and need for supportive and long-term care have become an important concern (5). There is limited information on the health status of the elderly from rural and urban communities in Nigeria, as many previous studies focused mainly on patients accessing care in hospitals.
Information on specific illnesses among elderly, if available, would inform the development of appropriate interventions and health care strategies especially at the community level. The aim of the study was to assess the burden of self-reported ill-health among the elderly and to identify its determinants in Osun State Nigeria.
Materials and Methods
The study was carried out in five randomly selected local government areas in Osun state. Osun state is in the Southwestern part of Nigeria and is bounded by Ogun, Kwara, Oyo and Ondo in the South, North, West and East respectively. According to the 2006 National Population Census (NPC), Osun state was estimated to be about 3 million. Majority of the inhabitants were farmers and traders. All adults that were sixty years and above who consented to be part of the study were included. Elderly aged 60 years and above were individually briefed on the objectives of the survey and were also informed that participation was completely voluntary. Consent was recorded as ''yes'' or ''no'' on an individual form designed for the collection of basic demographic data. For those who refused to participate, no further questions were asked, and no information was recorded.
The study design was a descriptive cross sectional of all eligible elderly persons, 60 years and above who had resided in Osun state for at least one year before the study. The study was carried out from May to August 2017, which spanned the rainy season. Prior to data collection, grass root sensitization and mobilizations at community level had been carried out in the selected LGAs to draw the attention of the elderly to the planned health outreach. All eligible and consented elderly persons in the five LGAs selected by simple random sampling from the thirty in the states were met at designated primary health care center in their respective LGA. The health outreach was organized by a group of medical and public health researchers in the College of Health Sciences of the University, with the Department of Community Medicine as the coordinating center. The project involved free distribution of hematinics, vitamins and treatment of minor ailments following both physical, medical and laboratory investigations by clinicians and laboratory scientists in the research team. General health counseling towards improved health status was also given to all participants. Ethical clearance was obtained from the Institutional Review Board IRB of Ladoke Akintola University of Technology, Osogbo, Nigeria. Following informed consent by the study participants, information was sought on the main outcome variable - self-reported illness two weeks before the survey among other question items, using a semi-structured interviewer-administered questionnaire. Diagnosis of diseases was made on the basis of medical history, clinical evaluation, laboratory investigations, available medical reports conducted elsewhere. A minimum sample size of 363 would be required at 95% confidence interval with a precision of 5% and a prevalence of 62% being the proportion of the elderly that reported one health problem or the other in previous study. (7) Overall, a sample of 491 elderly drawn across the three senatorial districts of the state participated in the study. Frequency distribution table and appropriate charts were used to illustrate salient features of the sample data. Bivariate association between selected factors and the outcome variable was determined using Chi-square test. Variables that were found statistically significantly associated with self-reported ill-health two weeks before survey using Chi-square test were fitted into logistic regression model. Odd ratios and appropriate 95% confidence interval were reported and p<0.05 was reckoned as statistically significant.
Results
Overall, dataset of sample of 491 elderly drawn from across the three senatorial districts in Osun State were analyzed. The mean age of the study participants in years was 68.9 ± 7.2 SD, male were older 79.5 ± 8.3 SD than their female 68.2 ± 6.7 SD counterparts.
From Table 1, most of the study participants 369 (75.2%) were young old, 60-74 years, 110 (22.4%) were old-old, 75-84 years and only 12 (2.4%) were very old, more than 84 years. More than three-quarter 385 (78.4%) of the respondents were females. Whereas only 57 (11.6%) had a minimum monthly income of 20 000 naira, 280 (57%) did not have regular source of income and the remaining 146 (29.7%) earned less than 20,000 naira a month. Slightly over half 251(51.1%) were residing in the rural setting and most 332 (67.6%) lacked basic formal education. Whereas 202 (41.1%) of the study participants were married and living with the spouse(s) at the time of this study, 253(51.5%) were married but widowed.
Table 1:
Socio-demographic and personal characteristics of the study participants
| Characteristics | Frequency | Percentage | ||||
|---|---|---|---|---|---|---|
| Age groups | ||||||
| 60-74 years | Young old | 369 | 75.2 | |||
| 75-84 years | Old old | 110 | 22.4 | |||
| > 84 years | Very old | 12 | 2.4 | |||
| Sex | ||||||
| Male | 108 | 21.6 | ||||
| Female | 385 | 78.4 | ||||
| Location | ||||||
| Rural | 251 | 51.1 | ||||
| Urban | 240 | 48.9 | ||||
| Highest Educational Status | ||||||
| None | 332 | 67.8 | ||||
| Primary | 98 | 20.0 | ||||
| Secondary | 34 | 6.9 | ||||
| Tertiary | 27 | 5.5 | ||||
| Monthly Income | ||||||
| <20, 000 | 146 | 29.7 | ||||
| ≥ 20,000 | 57 | 20.0 | ||||
| No regular income | 288 | 58.7 | ||||
| Local Government Area | ||||||
| Ede North | 96 | 19.6 | ||||
| Obokun | 78 | 15.9 | ||||
| Olrunda | 85 | 17.3 | ||||
| Orolu | 90 | 18.3 | ||||
| Ejigbo | 142 | 28.9 | ||||
| Marital Status | ||||||
| Never married | 6 | 1.2 | ||||
| Married & living with partner | 202 | 41.1 | ||||
| Married but widowed | 253 | 51.5 | ||||
| Separated | 25 | 5.1 | ||||
| Divorced | 5 | 1.0 | ||||
| Regular source of income | ||||||
| Yes | 211 | 43.0 | ||||
| No | 280 | 57.0 | ||||
| Satisfied with present residential status | ||||||
| Yes | 292 | 59.5 | ||||
| No | 199 | 40.5 | ||||
| Loneliness | ||||||
| Yes | 63 | 12.8 | ||||
| No | 428 | 87.2 | ||||
| Ever used alcoholic drink | ||||||
| Yes | 105 | 21.4 | ||||
| No | 386 | 78.6 | ||||
| Any source of worry | ||||||
| Yes | 196 | 39.9 | ||||
| No | 295 | 60.1 | ||||
| Do exercise | ||||||
| Yes | 184 | 37.5 | ||||
| No | 307 | 62.5 | ||||
| Sick 2 weeks before survey | ||||||
| Yes | 228 | 46.2 | ||||
| No | 263 | 53.6 | ||||
One hundred and ninety-nine, 199 (40.5%) of the elderly were not satisfied with their present residential status and 63 (12.8%) claimed they were lonely. Whereas 105 (24.4%) attested they had used alcohol before only 31(10.7%) owned up to still taking it. Similarly, 92 (18.7%) had smoked before and only 4 (1.3%) were current smokers. Table 1 also shows that, in all, 196 (39.9%) declared to have one source of worry or the other.
Figure 1 provides information on the elderly foremost sources of worry and these include; health (48%), family/children/sibling (29%) and finances (10%).
Figure 1:
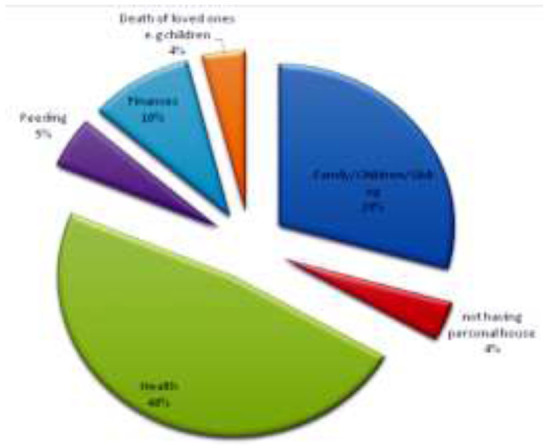
Sources of worry among the elderly
With respect to illness status of the elderly, whereas 228 (46.4%) were sick two weeks before the survey, 375 (76.4%) submitted they had one health condition or the other. Self-reported health problems include musculoskeletal conditions (arthritis, joint pain) 159 (32.4%), cardiovascular 142 (28.9%), eye related – vision 44 (9.0%) and gastro-intestinal (ulcer, piles) 23 (4.7%).
However, figure 2 shows illnesses elderly complained within two weeks before the survey to be: joint pain 189 (38.5%), headache 145 (29.5%), blurred vision 107 (21.8%) and muscle pain 100 (20.4%). It should be noted here that those that were sick two weeks before the survey reported more than one illness in most cases.
Figure 2:
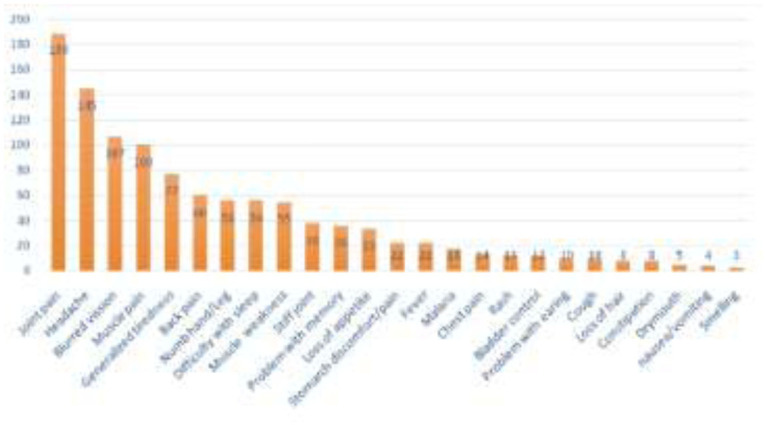
Illnesses or symptoms reported two weeks before the survey.
From Table 2, compared to not having a regular source of income, having a regular source of income is significantly protective against self-reported illnesses two weeks before the survey, [OR = 0.51, 95% CI = 0.35, 0.73]. Elderly that were lonely had over three-fold risk of reported-illnesses two weeks before the survey [OR = 3.07, 95% CI = 1.74, 5.44], so also those who had ever taken alcohol had about twice the risk of illness two weeks before the survey compared to those who had never taken alcohol, [OR=1.73, 95% CI = 1.12, 2.68].Elderly that ever smoked had slightly over three-fold risk of fallen sick than those who had never smoked [OR=3.28, 95%CI = 2.01, 5.33]. Engaging in physical activities or exercise was found to be significantly protective against illness among the elderly, [OR= 0.67, 95% CI= 0.46, 0.97], similarly those who were satisfied with their residential status had a significantly lower risk of coming down with sickness, [OR= 0.55, 95% CI= 0.38, 0.79]. Although the odds of illness were higher for being very old, being a female, living in urban setting and chewing kola nut, however, none of these was found to be statistically significant, as P>0.05 in each case.
Table 2:
Factors associated with self-reported illnesses among the elderly.
| Sick 2 weeks before Survey | ||||||
|---|---|---|---|---|---|---|
| Factors | No (%) | Yes (%) | 2df | OR [95% CI (OR)] | P-value | |
| Age group (years) | ||||||
| 60-74 | 192(51.9) | 178(48.1) | ||||
| 75 and above | 71(58.7) | 50(41.3) | 1.69 | 1 | 0.76(0.501, 1.1511) | 0.194 |
| Sex | ||||||
| Male | 62(58.5) | 44(41.5) | ||||
| Female | 201(52.2) | 184(47.8) | 1.32 | 1 | 1.29(0.843, 1.993) | 0.251 |
| Location | ||||||
| Rural | 108(43.0) | 143(57.0) | ||||
| Urban | 120(50.0) | 20(50.0) | 2.40 | 1 | 0.76(0.523, 1.081) | 0.122 |
| Educational status | ||||||
| Not Educated | 161(48.5) | 171(51.5) | ||||
| Educated | 67(50.0) | 92(57.9) | 1.75 | 1 | 1.290(0.882,1.894) | 0.186 |
| Income source | ||||||
| Not regular | 130(46.4) | 150(53.6) | ||||
| Regular | 133(63.0) | 78(37.0) | 13.34 | 1 | 0.508(0.353,0.732) | 0.0001 |
| Loneliness | ||||||
| No | 244(57.0) | 184(53.6) | ||||
| Yes | 19(30.2) | 44(69.8) | 15.92 | 1 | 3.070(1.735,5.436) | 0.0001 |
| Any source of worry? | ||||||
| No | 191(64.7) | 104(35.7) | ||||
| Yes | 72(36.7) | 124(63.3) | 37.15 | 1 | 3.163(2.172,4.607) | 0.0001 |
| Ever used alcoholic drinks? | ||||||
| No | 218(56.5) | 168(43.5) | ||||
| Yes | 45(42.9) | 60(57.1) | 6.16 | 1 | 1.730(1.119,2.675) | 0.013 |
| Ever smoked | ||||||
| No | 235(58.9) | 164(41.1) | ||||
| Yes | 28(30.4) | 64(69.6) | 24.35 | 1 | 3.275(2.013,5.329) | 0.0001 |
| Take kolanut | ||||||
| No | 182(55.8) | 144(44.2) | ||||
| Yes | 81(49.1) | 84(50.9) | 2.00 | 1 | 1.311(0.900, 1.908) | 0.157 |
| Do exercise | ||||||
| No | 153(49.8) | 154(50.2) | ||||
| Yes | 110(58.8) | 74(40.2) | 4.58 | 1 | 0.667(0.462,0.968) | 0.032 |
| Satisfied with residential status | ||||||
| No | 89(44.7) | 110(55.3) | ||||
| Yes | 174(59.6) | 118(40.4) | 10.51 | 1 | 0.549(0.381,0.790) | 0.001 |
Whereas as shown in Table 3 above, having regular source of income had an independent protective association with self-reported illness among the elderly, ever smoked and having any source of worry were found risk factors.
Table 3:
Multivariate analysis showing independent predictors of ill-health among elderly.
| Determinants | Odd Ratio (OR) | 95%CI (OR) | |
|---|---|---|---|
| Regular income source | |||
| Not regular | 1.000 | - | |
| Regular | 0.634 | 0.425,0.945 ** | |
| Satisfied with residential arrangement | |||
| No | 1.000 | - | |
| Yes | 0.863 | 0.571,1.303 | |
| Loneliness | |||
| No | 1.000 | - | |
| Yes | 1.760 | 0.944,3.281 | |
| Used alcohol | |||
| No | 1.000 | - | |
| Yes | 1.009 | 0.584,1.744 | |
| Ever smoked | |||
| No | 1.000 | - | |
| Yes | 2.351 | 1.311,4212** | |
| Any source of worry | |||
| No | 1.000 | - | |
| Yes | 2.522 | 1.683,3.794 ** | |
| Do Exercise | |||
| No | 1.000 | - | |
| Yes | 0.783 | 0.524,1.169 |
** Independent determinants of ill-health among elderly
Discussion
Socio-demographic and economic characteristics
There were more female participants than male in this study. Apart from the fact that this gender distribution agrees with the pattern observed in previous studies (2,7,8) it also reflects the fact that women have been found (9,10) to display a better health care seeking behaviour than their men counterparts. The proportion of rural dwellers was slightly higher than those residing in the urban settings. This sample distribution of geographical location of study participants was a clear reflection of the rural-urban Nigeria population. Majority of Nigerians dwell in the rural areas, in fact, the rural population in Nigeria as reported was 51.4 % of the entire population in 2016, according to the World Bank collection of development indicators (11). Similar distribution in respect of location of study participants was recorded by previous authors (7). Over two-third of the study participants were illiterates. This may not be unconnected with the fact that since majority of the study participants were women and girls' education in their days was so much unpopular. A higher proportion of 93.8% of the study participants with no formal education was however recorded in a similar study in a neighboring Oyo State (2). Over half of the elderly in the study were either widows or widowers. This however is much higher than 31.6%, a value recorded by previous authors (2).With about three out of every five elderly not having a regular source of income and another three in ten earning less than 20, 000 naira ($55, at the time of study) monthly, it was so obvious that majority of the elderly would have problem related to financing their daily needs.
Prevalence and Factors Associated with ill-health Status.
In this study, the prevalence of health status measured by self-reported illness two-weeks before the survey is quite high. This may not be unconnected with the fact that the elderly are more susceptible to ill health, as certain ill-health conditions are peculiar to old age. The prevalence of self-reported illness in this study fell below the value recorded by earlier authors (7) who had over half of their study participants as having one ill-health or the other. Self-reported illness in their study was however defined as any occasion of sickness thirty days before the survey in contrast to two weeks set as the threshold in this study. Foremost reported ill-health conditions two weeks before the survey were musculoskeletal conditions, headache, and eye related conditions. Similar pattern of ill-health was observed by a previous study (12). Although previous authors had reported a significant association between ill-health and older age group (7) and being women (7), this study only showed a likely pattern in that direction without establishing a significant association. The finding of this study showed that a higher proportion of women and a more elderly study participants were found to report ill-health more frequently two weeks before the survey compared to men and belonging to 'younger' age group respectively. Similarly, not having a formal education or living in urban setting have a higher likelihood or excess risk of ill-health, though not statistically significant. A systematic review of health literacy and health outcomes found that individuals with lower health literacy had poorer health-related knowledge and comprehension (13). They also had increased hospitalizations and emergency care, decreased preventive care, and, among the elderly, poorer overall health status and higher mortality (13).
The results of this study, both crude and adjusted analyses, showed having regular income and a monthly earning of more than $55 had a very significant protective effect on the health status of the aged. Elderly who were able to meet up with their basic financial needs would most likely have lesser issues to worry about. This ultimately would reduce the risk of ill-health conditions. The findings were consistent with (2) who had earlier identified low monthly income as a risk factor of ill-health. The World Health Organization WHO had also recognized and mentioned poverty as one of the five cardinal risks of ill-health among the elderly in an earlier article by the international health agency (1). Elderly who were lonely had a significant threefold risk of reporting ill-health compared to those who were not. This result was consistent with the findings (14), the authors noted that elderly who were lonely had higher risk of chronic illnesses compared to those living with their family members. Similarly, previous study (15) had observed that participants with mood disorders, lung disease, or heart disease had significantly higher loneliness scores than those without these conditions in their study of chronically ill rural adults. The authors further submit that loneliness is a contributing factor to various health problems in older adults, including complex chronic illness, functional decline, and increased risk of mortality.
We found that two out of every five elderly do have one source of worry or the other. The foremost cause of worry was their health, family – children or siblings and their finances. Similar result was also reported (16) that elderly had a higher likelihood of worrying about the health and welfare of loved one compared to the younger age group of, 16-29 years. Brock et al, 2011(17) appreciated the fact that ageing presents with a lot of changes in the life of the elderly, ranging from everyday family and social life, changes in their financial status and their health. The authors also noted that of these inevitable changes, those with chronic conditions such as arthritis of the hip and knee were more prone to worry about their condition than the healthy ones. Whatever the source of worry is, an important finding of this study either by crude or adjusted analysis is the fact that worrying in elderly predisposes them to excess risk of having ill-health compared to those who refused to get worried by the situations around them.
The prevalence of elderly reported to have ever smoked cigarette in this study is far below that reported in Malaysia (18). The authors had put the prevalence of ex-smokers and current smokers among Malaysian aged 60 years and above to 24.4% and 11.9% respectively. The prevalence value of 1.3% for current smokers in this study may have been an under representation of the actual value as considerable proportion 38.1% of the study participants declined comment when asked about their current smoking status. The world health organization WHO had earlier reported a prevalence value of cigarette smoking of 3.7% among adults in the country (19). With respect to risk of illness, in this study, elderly who had ever smoked had over threefold significant risk of ill-health compared to non-smokers. Several studies have linked cigarette smoking with different chronic health conditions and even untimely death (20-23). Older adults who continue to smoke have more difficulty with diseases common to old age, such as diabetes, osteoporosis, and common respiratory problems.
In our study, only 21.4% of the elderly reported ever used alcohol. This result is far below the prevalence values of lifetime use of alcohol recorded by previous authors (24-25). The authors recorded prevalence values of 57.9% and 56% respectively. The observed disparity in prevalence values could reflect the variation in the target populations and the design strategies adopted which appeared to be different in both instances. Whereas previous studies included younger age groups from 15 years old, our study focused only on the elderly, 60 years and above. The prevalence value for current alcohol use of 10.7% recorded in our study is quite similar to 12.0% recorded for respondents aged 64 years and above (24). Although, relationship between drinking and health status have been described (26) as being 'complex' our study reported an excess risk of ill-health among elderly who had ever used alcohol compared to non-users. The world health organization WHO recognizes harmful use of alcohol and poor physical activities as among risk factors to developing chronic illnesses in elderly (27) Our study had also found that exercise and being satisfied with residential status respectively were protective against ill-health in the elderly.
Conclusion
We conclude that the prevalence of ill-health among the elderly is considerably high and need urgent attention of the stake holders. Determinants of ill-health were essentially financial, social, and behavioural (lifestyle). Financial empowerment: schemes and programmes that foster social interactions among the elderly would surely be of immense benefits towards improving the health status of the elderly. Since being satisfied with residential status promotes a more stable health among the elderly, provision of low-cost housing facility by the government and private corporations and make accessible especially to low-income earners will surely support a healthier aged population. Young people should be educated to desist from smoking and alcohol intake as this could have far-reaching adverse effect on their health later in life.
References
- 1.WHO 2015. The world population is rapidly ageing. www.WHO.int/ageing/about/facts/en, [Accessed 12 September 2019].
- 2.Abegunde K, Owoaje E. Health problems and associated risk factors in selected urban and rural elderly population groups of South-West Nigeria. Ann Afr Med. 2013; 12:90-97 [DOI] [PubMed] [Google Scholar]
- 3.Baiyewu O, Bella A, Adeyemi J, Bamigboye E, Jegede R. Health problems and socio-demographic findings in elderly Nigerians. Afr J Med Sci. 1997; 26:13-17 [PubMed] [Google Scholar]
- 4.Ogungbo B, Gregson B, Mendelow D, Walker R. Cerebrovascular disease in Nigeria: what do we know and what do we need to know? Trop Doct. 2003; 33:25-30 [DOI] [PubMed] [Google Scholar]
- 5.Joshi K, Kumar R, Avasthi A. Morbidity profile and its relationship with disability and psychological distress among elderly people in Northern India. Int J Epidemiol. 2003; 32:978-987 [DOI] [PubMed] [Google Scholar]
- 6.Kabir Z, Tishelman C, Aguero Torres H, Chowdhury A, Winbland B, Hojer B. Gender, and rural urban differences in reported health status by older people in Bangladesh. Arch Gerontol Geriatr. 2003; 37:77-91 [DOI] [PubMed] [Google Scholar]
- 7.Wandera SO, Golaz V, Kwagala B, and Ntozi J. Factors associated with self-reported ill health among older Ugandans: A cross sectional study. Arch Gerontol Geriatr. 2015; 61:231–239 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Abdulraheem IS. Health needs assessment and determinants of health-seeking behaviour among elderly Nigerians: A house-hold survey. Annals of African Medicine. 2007; 6:2:58-63 [DOI] [PubMed] [Google Scholar]
- 9.Gunnarsson R, Nordeman L, Stibrant Sunnerhagen K, Billhult A. Gender differences in care-seeking behavior and health care consumption after work-related whiplash injuries: Artur Tenenbaum. European Journal of Public Health. 2014; 2: 154-166 [Google Scholar]
- 10.Thompson A E, Anisimowicz Y, Miedema B, et al. The influence of gender and other patient characteristics on health care-seeking behaviour: a QUALICOPC study. BMC Family Practice. 2016; 17:38. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.https://tradingeconomics.com/nigeria/rural-population-percent-of-total-population-wb-data.html.September 2019. [Google Scholar]
- Accessed, 12 [Google Scholar]
- 12.Clausena F, Sandberga E, Ingstadb B, Hjortdahla P. Morbidity, and health care utilisation among elderly people in Mmankgodi village, Botswana. J Epidemiol Community Health. 2000; 54:58–63 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Zimmerman EB, Woolf SH, Haley A. Understanding the relationship between education and health: A review of the evidence and an examination of community perspectives. Agency for health care research and quality. https://www.ahrq.gov/professionals/education/curriculum-tools/population-health/zimmerman.html. Content last reviewed September 2015
- 14.Agrawal S. Effect of living arrangement on the health status of elderly in India: Findings from a national cross-sectional survey. Asian population studies 2012; 1:87-101 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Theeke LA Mallow J. Loneliness and quality of life in chronically ill rural older adults. Am J Nurs. 2013; 113:28-37 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Goncalves DC, Byrne GJ. Who worries most? Worry prevalence and patterns across the lifespan Int J Geriatr Psychiatry. 2013; 28 :41-9 [DOI] [PubMed] [Google Scholar]
- 17.Brock K, Clemson L, Cant R, et al. Worry in older community-residing adults. Int J Aging Hum Dev. 2011; 72:289-301. [DOI] [PubMed] [Google Scholar]
- 18.Lim KH,Jasvindar K, Cheong SM, et al. Prevalence of smoking and its associated factors with smoking among elderly smokers in Malaysia: findings from a nationwide population-based study. Tob Induc Dis. 2016; 14: 8. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.WHO report on the global tobacco epidemic, 2017. Country Profile: Nigeria Tobacco use data from the latest survey results as at http://www.who.int/tobacco/surveillance/policy/country_profile/nga.pdf, 12 September 2019
- 20.Husten CG, Shelton DM, Chrismon JH, et al. Cigarette smoking and smoking cessation among older adults: United States, 1965-94. Tob Control. 1997; 6:175-180 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Burns DM. Cigarette smoking among the elderly: disease consequences and the benefits of cessation. Am J Health Promot. 2000; 14:357-361 [DOI] [PubMed] [Google Scholar]
- 22.Bratzler DW, Oehlert WH, Austelle A. Smoking in the elderly: it's never too late to quit. J Okla State Med Assoc. 2002; 95:185-91 [PubMed] [Google Scholar]
- 23.Jha P, Ramasundarahettige C, Landsman V, et al. 21st-century hazards of smoking and benefits of cessation in the United States. N Engl J Med. 2013:368:341-350. [DOI] [PubMed] [Google Scholar]
- 24.Lasebikan VO, Ola BA. Prevalence and Correlates of Alcohol Use among a Sample of Nigerian Semirural Community Dwellers in Nigeria. Journal of Addiction 2016, Article ID 2831594, 6 pages [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.Gureje, L, Degenhardt, B, Olley et al. A descriptive epidemiology of substance use, and substance use disorders in Nigeria during the early 21st century, Drug and Alcohol Dependence. 2007; 91: 1–9 [DOI] [PubMed] [Google Scholar]
- 26.Gordon NP, Weisner C. Alcohol Consumption, Medical Conditions, and Health Behavior in Older Adults. Am J Health Behav. 2007; 31: 238–248 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27.World Health Organization WHO bulletin. Risk factors of ill-health among the elderly. http://www.euro.who.int/en/health-topics/Life-stages/healthy-ageing/data-and-statistics/risk-factors-of-ill-health-among-older-people. Accessed 09 September 2019.