

Abstract
Case series summary
A retrospective study was undertaken to review outcomes of keratectomy and corneoconjunctival transposition in cats with superficial and deep corneal sequestra. Information including pertinent history, signalment, ophthalmological findings and postoperative outcome was collected from medical records. Follow-up was obtained by clinical examination, contact with the referring veterinarians and review of medical records or telephone contact with owners. Ninety-seven cats (109 eyes) were included from 2005–2015. The most commonly affected breeds included Persian, Burmese and Himalayan. The mean age at the time of surgery was 6.8 years (median 6.5 years; range 8.0 months–18.0 years). A corneal sequestrum in the contralateral eye was diagnosed in 28 cats (28.9%). Recurrent corneal sequestration was diagnosed in eight cats (nine eyes), with recurrence occurring a mean of 703 days after surgery (range 29–1750 days). Age, sex, breed, depth of sequestration and concurrent ocular disease in the contralateral eye were compared between cats with and without recurrence, with no risk factors for recurrence identified.
Relevance and novel information
Excellent surgical outcomes have previously been described in a series of 17 cats with superficial and mid-stromal corneal sequestra. This paper adds further information to the literature by describing a larger series of cats, with corneal sequestra affecting the full range of corneal thickness, and good long-term postoperative outcomes.
Introduction
Corneal sequestration is a common feline disease affecting the corneal stroma, with and without associated epithelial loss.1,2 Characteristic lesion discolouration ranges from translucent amber to opaque and black, 3 representing focal stromal collagen degeneration and necrosis (Figure 1). 4 The pathogenesis of sequestrum formation is not understood, 4 although predisposing and associated factors include ulcerative keratitis, lagophthalmos, entropion, trichiasis, tear film abnormalities, prior grid keratotomy, 5 genetics 6 and feline herpesvirus-1 (FHV-1).7,8
Figure 1.
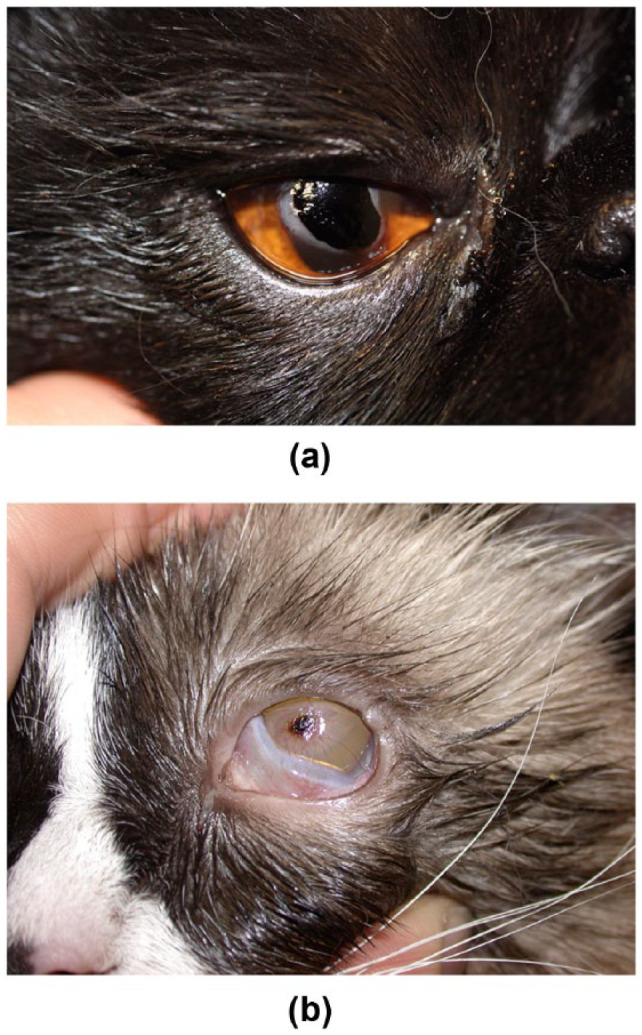
Variable appearance of corneal sequestra presentation. (a) A large, dense sequestrum with associated corneal oedema and reflex uveitis; (b) smaller, less well demarcated sequestrum with corneal stromal infiltrate and neovascular reaction
Treatment of corneal disease aims to restore structural integrity with minimal alteration in corneal transparency. 9 Many surgical techniques for treatment of corneal sequestra have been described, including keratectomy with placement of a conjunctival graft, 4 corneoconjunctival transposition (CCT), 10 porcine small intestinal submucosal (SIS) graft, 11 amniotic membrane transplantation, 12 heterologous penetrating keratoplasty 13 and bovine pericardial patch. 9 Surgery is recommended if there is discomfort and/or the lesion appears deep. 4
Treatment evaluation is reported less frequently.4,10 Use of conjunctival or SIS did not reduce recurrence rates, 4 while no recurrence was noted following CCT in 17 cats with corneal sequestration of the anterior and mid-stroma. 10 We aimed to report surgical outcomes of keratectomy and CCT for treatment of feline corneal sequestration affecting superficial, deep and full-thickness lesions, and evaluate risk factors for sequestra recurrence.
Case series description
Medical records of all cats diagnosed with corneal sequestra treated with CCT at a small animal referral hospital between July 2005 and May 2015 were reviewed. Ninety-seven cats (109 eyes) were identified. Data collected included breed, age, sex, affected eye, ophthalmic findings, location, depth and previous treatment of sequestra.
All cats were premedicated with an opioid (methadone [0.3–0.5 mg/kg IM; Physeptone, Aspen Pharma] or buprenorphine [0.02–0.03 mg/kg IM; Temgesic, Reckitt Benckiser]). Anaesthesia was induced using propofol (4–6 mg/kg IV; Propofol, Sandoz) and/or thiopentone (4 mg/kg IV; Pentothal, Link Medical Products) to effect. Each cat was intubated and anaesthesia maintained with inhalational isoflurane and oxygen. Atracurium besylate (0.2 mg/kg IV; Hospira Australia) was administered to achieve neuromuscular blockade with additional doses (0.1 mg/kg) to facilitate globe positioning. Surgery was performed by a veterinary ophthalmologist using a Zeiss operating microscope. The eye and periocular tissues were prepared for surgery using 5% povidine–iodine solution. The globe was stabilised with 6/0 silk stay sutures (Ethicon Australia). A corneal sliding flap was prepared to a depth of 40–50% in the dorsal cornea, unless a ventral or lateral sequestrum indicated preparation with more accessible conjunctiva and corneal tissue, and mobilised on a conjunctival pedicle (Figure 2). The sequestrum was delineated using a crescent knife or beaver blade and a keratectomy performed to remove all discoloured cornea (Figure 3). In cases seen in the period 2005–2012, the transposition was sutured into the corneal defect using polyglycolic acid (12 eyes [8/0-10/0 Biosorb; Alcon Laboratories]) or polyglactin 910 (29 eyes [9/0 Vicryl; Johnson & Johnson Medical]) based on surgeon preference, and from 2012 onwards, polyglycolic acid (64 eyes [9/0-10/0 Safil; B Braun Australia]) or polyglactin 910 (four eyes [9/0 Vicryl; Johnson & Johnson Medical]) was used. An interrupted (12 eyes) or combination of interrupted and continuous (98 eyes) suture pattern was used.
Figure 2.
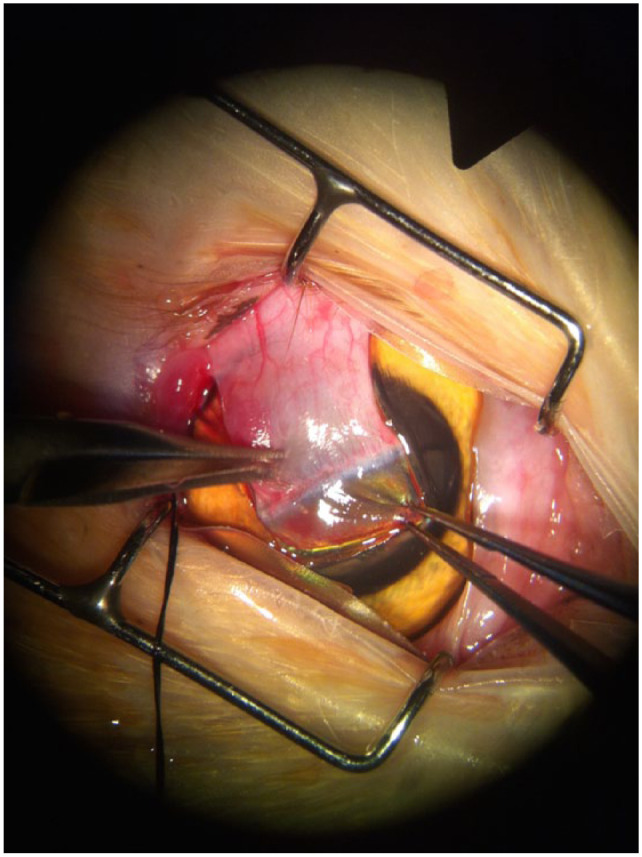
Mobilisation of the corneoconjunctival graft to fill the corneal defect made following removal of the sequestrum
Figure 3.
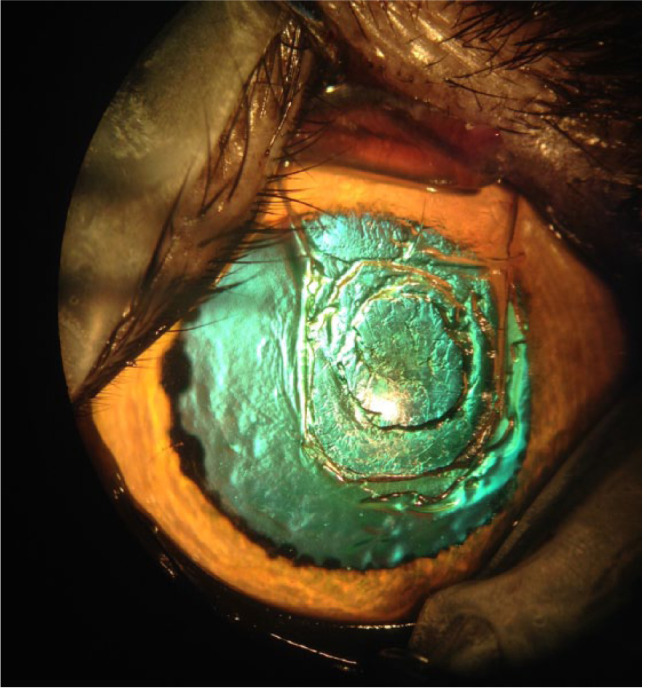
Corneal defect with no evidence of stromal discolouration with deeper keratectomy at the centre of the keratectomy site to ensure complete removal of the sequestrum
Recurrence was defined as any discolouration associated with, or separate to, the transposition in that eye. Time to recurrence was calculated from surgery to the date on which recurrent sequestra were diagnosed. Referring veterinarians were provided with detailed clinical notes, including plans and recommendations for monitoring. Owners were instructed on clinical signs for which to monitor.
Follow-up in the immediate postoperative period was by clinical examination with a veterinary ophthalmologist. All referring veterinarians were contacted after completion of the study, except when the cat had been examined by an ophthalmologist in the month prior. Attempts were made to contact all owners except when medical records indicated the cat was deceased. Owners were asked whether they were satisfied with the cosmetic outcome and whether further treatment was required in either eye.
Age, breed, sex, prior surgery, contralateral ocular disease and depth of sequestra were compared between cats with and without disease recurrence. Student’s t-tests were used for continuous data, Fisher’s exact test for categorical data and Pearson’s χ2 test to determine the significance of depth on recurrence of corneal sequestration. For all tests, a P value <0.05 was considered significant. Kaplan–Meier plots were generated to further evaluate the potential association between age (categorised as either <4 years and 4 years and older) and the difference in time to event between age groups were compared with a log rank test. All variables were further evaluated for their association with time to recurrence with bivariate Cox’s proportional hazard model.
There were 73 brachycephalic cats (Persian [20 cats, 22 eyes], Himalayan [18 cats, 19 eyes], Burmese [17 cats, 21 eyes], exotic breeds [eight cats, nine eyes], British Shorthair [four cats], Australian Mist [three cats, four eyes], Chinchilla [two cats, three eyes], one Bombay) and 24 non-brachycephalic cats (Abyssinian [two cats], Sphynx [one cat, two eyes] and one Siamese, Tonkinese, Devon Rex, Russian Blue, Norweigan Forest Cat and Birman). Fifteen cats (16 eyes) were not pedigree bred.
Mean age at presentation was 6.8 years (median 6.5 years; range 8.0 months to 18.0 years) and no sex predilection was identified: 46 males (53 eyes) and 51 female (56 eyes) cats. Four cats presented with bilateral sequestra. Corneal sequestration was diagnosed in the contralateral eye in 28 cats (28.9%), with 13 of these eyes undergoing surgical treatment (prior to the study period at a different institution) and two cases being treated medically. The remaining 13 eyes were included in this study. The left eye was affected in 53 cases and the right in 56 cases. Entropion or abnormal eyelid conformation occurred in 22 eyes (22.7%), with 14/22 eyes undergoing surgical treatment. The corneal sequestrum was located axially in 68 eyes (70.1%), elsewhere in the cornea in 26 eyes (26.8%) and the location not described in 15 eyes. The sequestrum was superficial or anterior stromal in 33 eyes (34.0%), deep stromal (>50% but not extending to Descemet’s membrane) in 15 eyes (15.5%), affecting Descemet’s membrane and/or resulting in corneal perforation in 17 eyes (17.5%), and depth not described in 44 eyes (45.4%).
Three eyes had a CCT performed previously in the affected eye at another veterinary hospital for a corneal sequestrum separate to where the new lesion was detected. Fifteen eyes had undergone corneal debridement for treatment of corneal ulceration or sequestration. Previous surgery was performed in 10 cats and included corneal (keratectomy [n = 3], grid keratotomy [n = 2], CCT for stromal ulcer [n = 1]) and/or adnexal surgery (third eyelid flap [n = 4], replacement of a prolapsed nictitans gland [n = 1]).
Postoperatively, all cats were treated with one or more topical antibiotics (chloramphenicol ointment 10 mg/g [Chlorsig; Aspen Pharma] and/or ofloxacin 3 mg/ml (Ocuflox; Allergan Australia), meloxicam (0.05 mg/kg PO q24h; Metacam 0.5 mg/ml [Boehringer Ingelheim]) and/or transmucosal buprenorphine (0.02–0.03 mg/kg q8–12 h [Temgesic; Reckitt Benckiser]). Additional medications included antibiotics: amoxicillin-clavulanate (15–25mg/kg PO q12h [Clavulox; Pfizer Australia]), doxycycline (5 mg/kg PO q12h [Vibravet; Pfizer Australia]) or famciclovir (30–50 mg/kg PO q12h [Famvir; Novartis Pharmaceuticals Australia]). Treatment for concurrent disease was prescribed/continued at the surgeon’s discretion.
Corneal sequestra recurred in the same eye in eight cats (nine eyes). Breeds in which recurrence was noted included six brachycephalics (Himalayan [three cats]; Exotic [one cat, two eyes]; a Persian and Burmese) and two non-brachycephalics (Sphynx and Abyssinian). Time from surgery to recurrence ranged from 29–1750 days (mean 703 days; median 700 days). Recurrence was associated with the CCT (n = 4), surrounding the CCT (n = 1) and not associated with the CCT (n = 2). Location of the recurrence was not reported in two eyes.
Treatment of recurrent corneal sequestration included chloramphenicol ointment with or without famciclovir (as described above) (n = 2); motorised corneal debridement using a diamond burr under topical anaesthesia (n = 3); and keratectomy with placement of a CCT (n = 2). Follow-up after recurrence of the sequestrum was diagnosed was not available in two cases.
Younger cats were more likely to develop recurrent corneal sequestration (P <0.05) and had longer follow-up (P <0.05). Age (categorised as <4 and 4 years and older) was not significantly associated with time to recurrence (log rank P = 0.4) (Figure 4). No other factor was significantly associated with recurrence (Table 1). No variable evaluated was significantly associated with recurrence using Cox’s proportional hazard model (age P = 0.2, follow-up time P = 0.2, remainder P >0.2).
Figure 4.
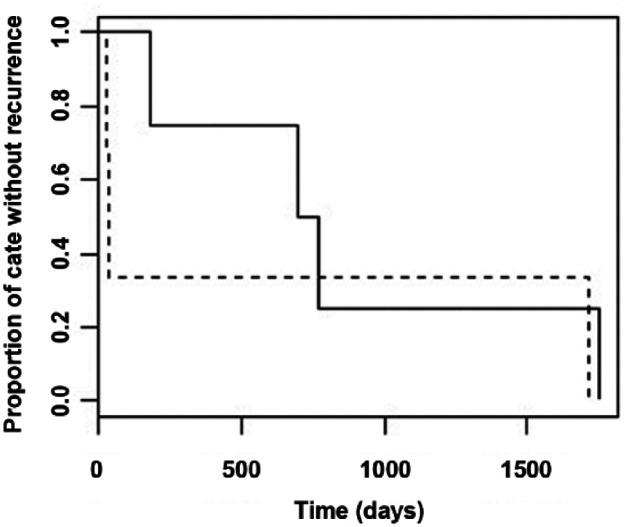
Kaplan–Meier plot demonstrating relationship between age group and time to recurrence of disease where age groups are <4 years (broken line) and 4 years and over (solid line)
Table 1.
Baseline comparison of cats with and without recurrent sequestration
| Overall (n = 97) |
Recurrence (n = 7) |
No recurrence (n = 90) | P value | |
|---|---|---|---|---|
| Age (years) | <0.05 | |||
| Mean | 6.8 | 4.2 | 7.0 | |
| Median | 6.0 | 3.0 | 6.5 | |
| Sex (female) | 51 (52.6) | 5 (71.4) | 46 (51.1) | 0.44 |
| Pedigree | 82 (84.5) | 7 (100) | 75 (83.3) | 0.59 |
| Prior ocular surgery | 26 (26.8) | 3 (42.9) | 26 (28.9) | 0.38 |
| Contralateral eye affected | 27 (27.8) | 1 (14.3) | 26 (28.9) | 0.67 |
| Corneal depth affected | 0.60 | |||
| NR | 40 (41.2) | 4 (57.1) | 34 (37.8) | |
| Superficial/mid-stromal | 29 (29.9) | 2 (28.6) | 27 (30.0) | |
| Deep stromal | 14 (14.4) | 1 (14.3) | 13 (14.4) | |
| Full thickness | 16 (16.5) | – | 16 (17.8) | |
| Follow-up (days) | <0.05 | |||
| Mean | 1332.5 | 1513.7 | 1093.0 | |
| Median | 1256 | 2004 | 842 |
Values are n (%) unless otherwise stated
NR = not reported; FHV-1 = feline herpesvirus-1
Follow-up data from owners, referring veterinarians or veterinary ophthalmologists ranged from 32.0 days to 9.3 years postoperatively (mean 3.6 years; median 3.4 years). This included 31 eyes last examined with a veterinary ophthalmologist, 51 eyes by a general veterinary practitioner and 22 eyes reported on by owners. All cats, except one cat experiencing recurrence, presented for the recommended follow-up with veterinary ophthalmologists. Reassessment with veterinary ophthalmologists ranged from 15 days to 5.7 years (mean 252.8 days; median 62 days). Follow-up beyond 100 days was not available in two cases. Where follow-up conversations were undertaken with owners (n = 67) all were happy with the appearance of the eye (Figure 5). Owners were not contacted when medical records noted the cat was deceased at study completion (n = 14). Where follow-up was made through referring veterinarians, there was no noted corneal discolouration or dissatisfaction with the postoperative appearance.
Figure 5.
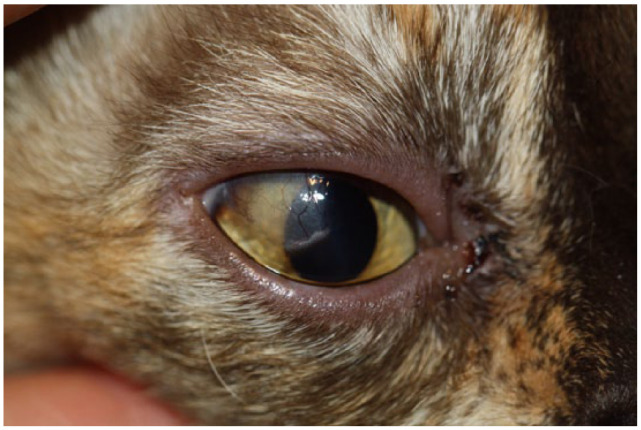
Healed corneoconjunctival transposition with normal vascularisation of the conjunctiva and good clearance of the corneal portion of the graft distal to the transposed limbus
Discussion
This study demonstrates a low rate of recurrent corneal sequestration among cats treated with keratectomy and CCT. Although multiple treatment options for corneal sequestra in cats have been reported, there is limited information regarding long-term outcome. To our knowledge, this is the largest published case series documenting surgical treatment of both superficial and deep corneal sequestration with CCT and shows good long-term outcomes with recurrence of sequestration reported in 8.3% of cats.
This study was similar to previous studies in that there was with no sex predilection, a variety of breeds represented and brachycephalic breeds were most commonly affected.14–16 Owing to the small number of cats experiencing a recurrence, the study was limited in its ability to evaluate risk factors for recurrence of corneal sequestra. Although those cats with recurrence were younger than cats without recurrence, this difference failed to achieve statistical significance in subsequent analysis.
No recurrence was reported in a series of 17 eyes undergoing keratectomy and CCT for treatment of corneal sequestration affecting the superficial and middle thirds of the stroma, with follow-up ranging from 30 days to 7 years after healing. 10 In our series, all cases undergoing keratectomy and CCT, up to and including full-thickness defects, were treated, demonstrating successful use of the technique for deeper lesions than previously reported. In addition to the larger number of cases, the depth of corneal involvement may be a factor in the different reported recurrence rates between these studies.
Comparison of the recurrence rates in this study with the existing literature is hampered by differences in the definition of recurrence. In our series, a recurrent corneal sequestrum was diagnosed if there was any corneal discolouration in that cornea following surgery; however, two cases of recurrence did not involve the CCT, suggesting involvement of other factors in sequestrum development. Featherstone et al defined recurrence as the need for a repeat surgical procedure, and documented 17% recurrence in eyes treated with a graft, which was not significantly different to those treated without a graft (25%). Using this definition, 4 the rate of recurrence in our case series would be 5/97 (5.2%). Reviewing the tabulated data, recurrent and using our definition, 4 there was recurrence in 21/41 (51.2%) eyes treated with keratectomy without a graft and in 10/30 (33.3%) eyes treated with a graft (conjunctival or SIS). This suggests that keratectomy with placement of a CCT results in lower recurrence (8.3%) compared with other described surgical techniques.
Conjunctival grafting appears to reduce the recurrence of sequestra after keratectomy and can provide tectonic support, although it is associated with secondary corneal scarring of varying densities. 4 The use of amniotic membrane has been associated with necrosis and perforation in a small number of eyes, 12 potentially attributable to suppression of myofibroblast differentiation by the amniotic membrane, resulting in corneal thinning and perforation. Other options reported in small numbers of cats include use of bovine pericardium and porcine SIS grafts.9,11 In addition to avoiding or minimising recurrence, the ideal treatment of corneal sequestra would reconstruct corneas while maintaining a clear visual axis. Advantages of CCT include considerable success, excellent cosmetic appearance, and ease and availability without requirements for donor materials.
Cosmesis was satisfactory in all cases where follow-up was available. CCT results in minimal corneal scarring compared with other surgical procedures used to treat corneal sequestra. 17 The precise mechanisms by which corneal transparency improves over time following CCT are unknown, although in humans with limbal injuries, corneal epithelial cells may replace conjunctival epithelium. 18
An important aspect of long-term preventive care should address any cause(s) of ocular irritation. 10 Although surgical correction of entropion was not performed on all eyes where concurrent entropion was diagnosed (typically secondary to corneal disease), there was no recurrence of sequestrum in eyes diagnosed with entropion.
The role of FHV-1 in the development of corneal sequestra remains unclear. FHV-1 polymerase chain reaction and/or immunohistochemistry on resected corneal tissue could have been, but was not, performed. Interpretation of FHV-1 is not straightforward as viral DNA can be found in clinically normal cats.19–21 It is not definitively known whether FHV-1 DNA is attributable to FHV-1 infection or is evidence of latency;1,22 FHV-1 infection remains, however, a possible causative factor, and further investigation is warranted.
It has been suggested that several procedures sequentially removing sections of deep sequestra to allow for extrusion over several weeks should be performed following removal of a superficial sequestrum, and deep stromal lesions (>0.3 mm) should not be resected in their entirety. 14 In all cases in this series keratectomy was performed to remove all clinically detectable abnormal cornea prior to placement of the CCT because of the importance of complete excision of the sequestrum. In one case of recurrent sequestration in the early postoperative period (4 weeks postoperatively), it is possible that there was incomplete excision, and earlier detection of discolouration was hindered by the vascular reaction of the healing CCT.
Direct comparison of recurrence between eyes treated with CCT and those treated either medically or with keratectomy was not attempted owing to the absence of appropriate follow-up. Further studies to compare recurrence using different medical and surgical techniques will require a set definition of recurrence, as well as appropriate follow-up examination.
Despite being the largest reported case series to date, the relatively low number of cases remains a limitation. With the low rate of recurrence, the clinical significance of different factors that may be associated with recurrence is difficult to determine. There are limitations in the duration and type of follow-up. Surgical treatment is often curative and re-examinations with a veterinary ophthalmologist are usually not feasible or recommended. As long-term follow-up with an ophthalmologist was not available consistently, it remains possible that sequestration recurred or will recur without being diagnosed.
Owing to the retrospective nature of this study, there are limitations in interpreting results and drawing conclusions. While this study was undertaken to review the surgical success of the described technique in a large study sample, the significance of potential compounding factors is difficult to ascertain. Qualitative and quantitative tear film analyses were not performed and few reports on tear evaluation in cats have been published. 23 Grahn et al reported insignificance in linking goblet cell atrophy and qualitative tear film abnormalities with corneal sequestration in a small series. 24 However, experimentally induced FHV-1 infection in naïve cats was reported to have persistent and clinically important decreases in tear film stability and mucin content, 25 and recent publication of reference values, correlations and repeatability of results have now been reported in healthy cats. 26 Investigation of outcomes in cats with corneal sequestra, including objective data such as tear film measurements and testing for FHV-1 infection, would be beneficial.
Conclusions
CCT following keratectomy is a successful treatment modality for corneal sequestrum of all depths in the cat. CCT yields excellent cosmetic results, a typically clear visual axis with no reported visual defects and low rates of recurrence. No specific risk factor for recurrence was identified in this study.
Acknowledgments
We would like to thank Dr Andrea Harvey BVSc, DSAM (Feline), DipECVIM-CA, MRCVS, MANZCVS (Assoc) and Dr Richard Malik DVSc, DipVetAn, MVetClinStud, PhD, FACVSc, FASM, MASID for assistance with revision of the manuscript. Dr Celia B Harris BSc, PhD, Department of Cognitive Science, Macquarie University, is also thanked for her assistance with statistical analysis.
Footnotes
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding: The authors received no financial support for the research, authorship, and/or publication of this article.
Accepted: 25 March 2016
References
- 1. Stiles J, Townsend WM. Feline ophthalmology. In: Gelatt KN. (ed). Veterinary ophthalmology, vol II, 4th ed. Ames, IA: Blackwell Publishing, 2007, pp 1095–1164. [Google Scholar]
- 2. Gelatt KN, Peiffer RL, Stevens J. Chronic ulcerative keratitis and sequestrum in the domestic cat. J Am Anim Hosp Assoc 1973; 9: 204–213. [Google Scholar]
- 3. Glaze MB, Gelatt KN. Feline ophthalmology. In: Gelatt KN. (ed). Veterinary ophthalmology. Philadelphia, PA: Lippincott Williams & Wilkins, 1999, pp 997–1052. [Google Scholar]
- 4. Featherstone HJ, Sansom J. Feline corneal sequestra: a review of 64 cases (80 eyes) from 1993 to 2000. Vet Ophthalmol 2004; 7: 213–227. [DOI] [PubMed] [Google Scholar]
- 5. La Croix NC, van der Woerdt A, Olivero DK. Non healing corneal ulcers in cats: 29 cases (1991–1999). J Am Vet Med Assoc 2001; 218: 733–735. [DOI] [PubMed] [Google Scholar]
- 6. Vawer GD. Corneal mummification in colourpoint cats. Vet Rec 1981; 109: 413.. [DOI] [PubMed] [Google Scholar]
- 7. Nasisse MP. Feline herpesvirus ocular disease. Vet Clin North Am Small Anim Pract 1990; 20: 667–680. [DOI] [PubMed] [Google Scholar]
- 8. Nasisse MB, Glover TL, Moore CP, et al. Detection of feline herpesvirus 1 DNA in corneas of cats with eosinophilic keratitis or corneal sequestrum. Am J Vet Res 1998; 59: 856–858. [PubMed] [Google Scholar]
- 9. Dulaurent T, Azoulay T, Goulle F, et al. Use of bovicne pericardium (Tutopatch) graft for surgical repair of deep melting corneal ulcers in dogs and corneal sequestra in cats. Vet Ophthalmol 2014; 17: 91–99. [DOI] [PubMed] [Google Scholar]
- 10. Andrew SE, Tou S, Brooks DE. Corneoconjunctival transposition for the treatment of feline corneal sequestrate: a retrospective study of 17 cases (1990–1998). Vet Ophthalmol 2001; 4: 107–111. [DOI] [PubMed] [Google Scholar]
- 11. Goulle F. Use of porcine small intestinal submucosa for corneal reconstruction in dogs and cats: 106 cases. J Small Anim Pract 2012; 53: 34–43. [DOI] [PubMed] [Google Scholar]
- 12. Barachetti L, Giudice C, Mortellaro CM. Amniotic membrane transplantation for the treatment of feline corneal sequestrum: pilot study. Vet Ophthalmol 2010; 13: 326–330. [DOI] [PubMed] [Google Scholar]
- 13. Townsend WM, Rankin AH, Stiles J, et al. Heterologous penetrating keratoplasty for treatment of a corneal sequestrum in a cat. Vet Ophthalmol 2008; 11: 273–278. [DOI] [PubMed] [Google Scholar]
- 14. Pentlarge VW. Corneal sequestration in cats. Comp Cont Educ Pract 1989; 11: 24–32. [Google Scholar]
- 15. Souri EN. The feline corneal nigrum. Vet Med Small Anim Clin 1975; 70: 531–534. [PubMed] [Google Scholar]
- 16. Startup FG. Corneal necrosis and sequestration in the cat: a review and record of 100 cases. J Small Anim Pract 1988; 29: 476–486. [Google Scholar]
- 17. Wilkie DA, Whittaker C. Surgery of the cornea. Vet Clin North Am Small Anim Pract 1997; 27: 1067–1107. [DOI] [PubMed] [Google Scholar]
- 18. Dua HS. The conjunctiva in corneal epithelial wound healing. Br J Ophthalmol 1998; 82: 1407–1411. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19. Nasisse MP, Glover TL, Moore CP, et al. Detection of feline herpesvirus-1 DNA in corneas of cats with eosinophilic keratitis or corneal sequestration. Am J Vet Res 1998; 59: 856–858. [PubMed] [Google Scholar]
- 20. Weigler BJ, Babineau CA, Sherry B, et al. High sensitivity polymerase chain reaction assay for active and latent feline herpesvirus-1 infections in domestic cats. Vet Rec 1997; 140: 335–338. [DOI] [PubMed] [Google Scholar]
- 21. Stiles J, McDermott M, Bigsby D, et al. Use of nested polymerase chain reaction to identify feline herpsevirus in ocular tissue from clinically normal cats and cats with corneal sequestra or conjunctivitis. Am J Vet Res 1997; 58: 338–342. [PubMed] [Google Scholar]
- 22. Townsend WM, Stiles J, Guptill-Yoran L, et al. Development of a reverse transcriptase-polymerase chain reaction assay to detect feline herpesvirus-1 latency-associated transcripts in the trigeminal ganglia and corneas of cats that did not have clinical signs of ocular disease. Am J Vet Res 2004; 65: 314–319. [DOI] [PubMed] [Google Scholar]
- 23. Sebbag L, Kass PH, Maggs DJ. Reference values, interest correlations, and test-retest repeatability of selected tear film tests in healthy cats. J Am Vet Med Assoc 2015; 246: 426–435. [DOI] [PubMed] [Google Scholar]
- 24. Grahn BH, Sisler S, Storey E. Qualitative tear film and conjunctival goblet cell assessment of cats with corneal sequestra. Vet Ophthalmol 2005; 8: 167–170. [DOI] [PubMed] [Google Scholar]
- 25. Lim CC, Reilly CM, Thomasy SM, et al. Effects of feline herpesvirus type-1 on tear film break-up time, Schirmer tear test results, and conjunctival goblet cell density in experimentally infected cats. Am J Vet Res 2009; 70: 394–403. [DOI] [PubMed] [Google Scholar]
- 26. Sebbag L, Kass PH, Maggs DJ. Reference values, interest correlations, and test-retest repeatability of selected tear film tests in healthy cats. J Am Vet Med Assoc 2015; 246: 426–435. [DOI] [PubMed] [Google Scholar]