

Abstract
Impact:
Low-cost spay–neuter clinics were first established nearly 50 years ago in response to the numbers of dogs and cats euthanized in animal shelters. Since then, high-quality, high-volume spay–neuter (HQHVSN) clinics have been established throughout the USA and have contributed to a significant reduction in animal euthanasia in shelters. These clinics, specializing in efficient systems and surgical techniques, provide an avenue for clients who cannot afford surgery to sterilize their pets. These clinics have also helped animal shelters with limited financial resources implement spay–neuter prior to adoption policies.
Response:
The veterinary profession’s reaction to HQHVSN clinics has been mixed; some practitioners question the quality of care provided or fear the loss of clientele, while others recognize the need for such clinics and support their development.
Challenges:
As veterinary education has become more expensive and veterinary care more sophisticated, the cost of veterinary care, including spay–neuter surgery, has risen. With increasing costs, the numbers of pets that receive little or no veterinary care has increased. Indeed, a 2018 survey by the Access to Veterinary Care Coalition documented that more than 25% of pet-owning households in the USA experienced difficulties obtaining veterinary care for their pets and the most frequent barrier was financial.
Aim:
This review looks at the reality of HQHVSN clinics and what this means for the private practitioner. By adopting similar systems and techniques that lower the cost of spay–neuter surgery, practitioners could potentially pass on cost savings to clients. Moreover, the same principles may be applied to other aspects of basic care to further address access to care issues.
Keywords: High-quality, high-volume, spay–neuter, access to care, private practitioner
Veterinary care – a luxury?
Humane and veterinary professional organizations are becoming increasingly aware of issues related to access to veterinary care. A recent white paper from the Access to Veterinary Care Coalition, entitled ‘Access to Veterinary Care: Barriers, Current Practices and Public Policy’, clearly documents the economic and other obstacles that limit access to care for millions of pets across the USA. 1 As veterinary care has become more expensive over the past several decades, increasingly more and more pet owners have difficulty obtaining even routine wellness care such as vaccinations, parasite control and spay–neuter surgery. Between 2016 and 2018, over 1 in 4 (27.9%) US households experienced difficulties obtaining veterinary care for their pets and the most common reason for these difficulties was financial. 1
There is a scarcity of literature related to the provision of veterinary care in underserved communities. A comprehensive review of the literature, published in 2017, discovered only 51 articles specifically related to this issue. 2 The most common reason cited for lack of veterinary care was cost. 2 In a recent roundtable discussion on veterinary practice conducted by the American Veterinary Medical Association (AVMA), Dr Michael Bailey, a member of the AVMA board of directors, went so far as to say ‘the cost of veterinary care could lead to veterinary care becoming a luxury’ (quoted in Burns 2019). 3 For cats, the access to care problem may be even greater when one considers colonies of community cats with caretakers but no one who claims ownership.
Before anyone was discussing access to care, low-cost, high-quality, high-volume spay–neuter (HQHVSN) clinics were being established across the USA in an effort to increase the availability of spay–neuter services in order to reduce pet overpopulation and euthanasia of unhomed pets in animal shelters. Nevertheless, the existence of HQHVSN clinics has been controversial within the profession; some practitioners contending unfair competition and the loss of clients, 4 and others contending that such clinics do not meet professional standards. 5

Current attitudes and ongoing concerns regarding HQHVSN
Much has changed since the early 1970s when the first spay–neuter clinics emerged (see box). Attitudes toward spay–neuter surgery have shifted, the public has become more aware of pet overpopulation, HQHVSN clinics have been established throughout the USA and the number of animals euthanized in animal shelters has dropped considerably. There remains some opposition to HQHVSN, however. Some in the profession contend that HQHVSN clinics take business away from the private practitioner, and some still express concerns about the quality of care provided at these clinics; others promote cooperative programs that benefit both the private practitioner and the HQHVSN clinic.4–7
Addressing the quality of care issue, in 2008, the Association of Shelter Veterinarians (ASV) published guidelines for spay–neuter programs in an effort to ensure that HQHVSN facilities were truly providing high-quality care along with high volume. 8 These comprehensive guidelines addressed preoperative care, anesthetic procedures, surgical care and postoperative care. The guidelines were updated in 2016, again with the intent of promoting high-quality care in spay–neuter clinics. 9 While little has been published in the veterinary literature regarding the incidence of postoperative complications associated with spay–neuter, a study of the results at one HQHVSN clinic that performed spay–neuter on 71,557 cats and 42,349 dogs over a 7-year period documented mortality rates approximately 1/10th of those reported at low-volume private veterinary practices. 10 Simply put, adhering to basic principles and performing the same procedures repeatedly, increases efficiency, improves quality and reduces complications.
It is more difficult to address the issue of unfair competition. Very little hard data are available documenting the economic impact of HQHVSN clinics on private veterinary practices. One study published in 2016 reported that the majority of cats sterilized through a reduced-cost spay–neuter program in Massachusetts, USA, had never been seen by a veterinarian previous to the sterilization surgery and that the primary reason was the cost of services. 11 Anecdotally, some veterinarians will contend that they rarely perform spays and neuters any longer, since they are all performed at high-volume clinics. Certainly, HQHVSN clinics that work closely with, or are associated with, animal shelters are primarily responsible for the trend for animal shelters to have pets spayed or neutered prior to adoption, a critical approach in reducing pet overpopulation. In communities without an HQHVSN clinic, however, the private practitioner can still play a major role in ensuring sterilization of shelter animals prior to adoption.
Veterinarians are becoming more aware of issues of access to care, but disagree on solutions. In a 2018 survey, 94.9% of veterinary respondents agreed or strongly agreed that ‘all pets deserve some of level of veterinary care’ but only 47% agreed that ‘society has a responsibility to help poor people and their pets’ and even fewer (27%) agreed that ‘everyone regardless of circumstances should be able to own a pet’. 1 Clearly, there is a disparity between the concepts that all pets deserve care and that society has a responsibility to help. Perhaps a more accurate assessment of the attitude is that while pets deserve care it is not veterinarians’ responsibility to bear the cost of that care.
The question becomes, will private practitioners play a role in providing basic care, including spay–neuter surgery, to the growing population of pet owners that currently cannot afford to take their pet to full-service veterinary clinics? Forsaking those potential clients will have one of two potential consequences: either a growing number of pets will go without basic care; or low-cost clinics will increase in number and in services offered.
Basic principles for efficient spay–neuter
Close examination of the operations of HQHVSN clinics reveals that the primary reason they can charge less than full-service clinics is because they have developed extremely efficient methods, not because many are tax-exempt non-profits. The private veterinary practice can adopt the same efficient systems and the same surgical techniques as the HQHVSN clinics and, therefore, perform spay–neuter surgeries at a much lower cost.
Factors that influence the efficiency of spay–neuter include the skill of the technical staff and the veterinary surgeon, the age of the surgical patients and the specific surgical techniques utilized. Key principles in developing efficiency in spay–neuter surgery include designating a block of time devoted to spay–neuter, performing the surgeries at an earlier age and adopting very efficient surgical techniques.
Designate a block of time specifically for spay–neuter surgeries
Having designated specific time for spay–neuter surgeries, schedule all sterilizations for that block of time and schedule nothing else. As an example, designate Tuesday mornings as the devoted spay–neuter time. All cats scheduled for surgery would have an appointment between 7.30 and 8 am that day. Clinic staff would admit the patients and initiate the medical records. The veterinarian(s) would perform physical examinations and determine if each cat is a safe anesthetic and surgical candidate.
Once physical examinations are completed, technical staff begin to anesthetize and prepare patients for surgery, and the surgeries begin. The goal would be to minimize delays between one surgery and the next. So, as surgery is being performed on patient 1, patient 2 is being anesthetized, prepared for surgery and positioned on a second surgery table. The veterinarian, upon finishing the first surgery, moves to the second table, changes surgery gloves and, using a new sterile pack of instruments, begins surgery 2. At the same time, technical staff remove patient 1 from the surgery table, clean and prepare the table for the next surgery and begin to recover patient 1.
The process is continued until all surgeries are completed. Without distractions and without conflicting assignments during this block of time, the technical staff will become adept at performing these tasks and maintaining the flow of surgeries. With repetition, the veterinary surgeon will become more efficient.
Perform spay–neuter surgery on cats prior to 5 months of age
While traditionally veterinarians have sterilized cats at 6 months of age or older, there is, at present, no scientifically sound basis for waiting that late to sterilize cats and no contraindications for spay–neuter surgery at 4–5 months of age. Anesthetic concerns about juvenile surgery voiced in the 1960s and 1970s are no longer valid. There are many anesthetic drugs and protocols in use today that are safe in cats as young as 6 weeks of age. 9 Old fears that castration of juvenile male cats would predispose to urinary obstruction were disproven in the 1990s. 12
There are numerous known health benefits for spay–neuter in cats, in addition to the population management benefits. In the words of Steve Dale, pet journalist and certified animal behavior consultant, there is ‘no evidence to suggest that gonadectomy by 5 months of age is linked to any increased risk of disease.’ 13 A survey conducted in 2000 of veterinarians who were already, at that time, spaying and neutering cats under 5 months of age, confirmed that the surgeries were easier, faster and had fewer complications than spay–neuter of cats at 6 months of age or older. 14 The AVMA, American Animal Hospital Association (AAHA), American Association of Feline Practitioners (AAFP) and ASV, as well as numerous humane organizations, have all endorsed the concept of sterilizing cats by 5 months of age.15–17 Put simply, the surgeries are faster, safer and easier.
Adopting efficient surgical techniques
Some of the surgical techniques used in HQHVSN clinics (see box) are significantly different from the techniques taught in many veterinary schools. Students are mostly taught how to perform spays and neuters at a point in their education when they are very inexperienced surgeons. In view of this inexperience, students are taught techniques that are designed to compensate for poor surgical skills and lack of knowledge. For example, they are taught to double ligate vessels because instructors do not trust their ligatures. Indeed, a recent study confirmed that over 50% of ligatures tied by students early in their surgical training did not create full occlusion. 20 Also, students are taught interrupted suture patterns because instructors recognize that it takes considerable practice to reach a point where students are consistently tying secure knots. They are taught to perform long incisions in order to provide extensive exposure and better acquaint them with abdominal anatomy.
As veterinarians gain experience in surgery they become much more efficient, but often fail to abandon those techniques that were designed to compensate for lack of experience. Many of those techniques can be replaced by ones that are much more efficient.

Techniques
Patient positioning, cat spay
Position the cat in dorsal recumbency with the rear limbs tied to one end of the table. Do not tie the font limbs. Stretching the forelimbs forward with any amount of tension, tenses the muscles of the back and makes exteriorizing the ovaries through small incisions more difficult.
Patient positioning, cat castration
Position the cat in dorsal recumbency with the rear limbs pulled forward. This provides easy access to the scrotum.
Location and size of the cat spay incision
The factor that determines the ideal location for a spay incision is which structures in the female reproductive tract are most difficult to exteriorize. In the cat, the uterine body is more difficult to exteriorize than the ovaries. The spay incision, therefore, should be located more caudally along the abdominal midline. The center of the skin incision should be at the midpoint between the umbilicus and the cranial brim of the pubis (Figure 1). With practice, ovariohysterectomy in the cat can be performed through a small (1–2 cm) appropriately placed skin incision. Upon exposure of the linea alba the linea is elevated, nicked with a scalpel and the linea incision extended.
Figure 1.

The center of the cat spay incision should be the midpoint between the umbilicus and cranial brim of the pubis
Use of the spay hook
A spay hook allows the veterinarian to perform a spay through a very small incision. With the hook facing forward, pass the instrument through the abdominal incision and along the right lateral abdominal wall to the dorsum of the abdomen. Once the dorsum is reached, turn the hook toward the midline and gently slide or bounce the hook toward the midline. At the midline, elevate the hook out of the abdominal cavity and gently remove any tissue that is not associated with the reproductive tract from the hook. Grasp the captured uterine horn (or broad ligament) with your fingers and proceed to perform the spay. (The American Society for the Prevention of Cruelty to Animals [ASPCA] has produced a video demonstrating the use of a spay hook to locate the uterus in spay surgery, available at: aspcapro.org/resource/how-use-spay-hook-surgery.)
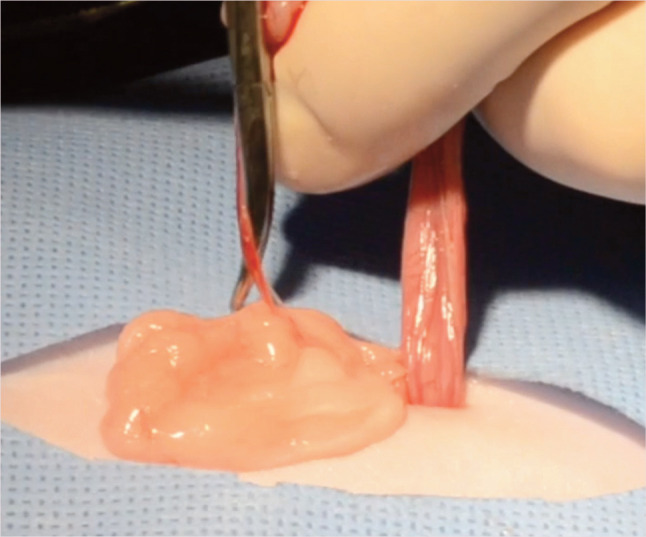
Clamping the proper ligament and cutting the suspensory ligament
Once the first uterine horn is exteriorized, gentle upward tension will exteriorize the first ovary. There is a ligament between the ovary and the uterine horn (the proper ligament) that is contiguous with the suspensory ligament. Place a mosquito hemostat on the proper ligament and use that to apply gentle upward tension. This will fully expose the respective ovary and will tense the suspensory ligament, making it easier to palpate and visualize. Cut the suspensory ligament with either scissors or a scalpel. (A video showing clamping of the proper ligament and cutting the suspensory ligament is available as supplementary material.)
Pedicle tie
The pedicle tie is an efficient and safe method of ligating the ovarian vessels of the cat.9,18,19 With the ovary delivered through the abdominal incision and the suspensory ligament cut, make a fenestration in the broad ligament just caudal to the ovarian vessels. Hold the ovary in your non-dominant hand and gently pull the ovary toward you. Using the dominant hand, a curved hemostat is crossed over the ovarian vessels into the hole in the broad ligament and underneath and behind the vessels. The hemostat should be held closed, with the tip of the hemostat facing away from you. The tip of the hemostat is then directed above the vessels as the hemostat is rotated counterclockwise to end up facing you (for left-handed surgeons the hemostat is rotated in a clockwise motion). The hemostat is opened and used to clamp the ovarian vessels. The vessels are cut between the hemostat and the ovary, and the knot is gently pushed off the tip of the hemostat. The knot should be pulled tight before releasing the hemostat (Figure 2). (A video of the pedicle tie is available as supplementary material.) Gentle caudal retraction on the uterine horn will expose the uterine body and the second uterine horn. Expose, ligate and transect the second ovarian pedicle, as done with the first.
Figure 2.
The pedicle tie is an efficient and safe method for ligating the ovarian vessels of the cat
Modified Miller’s knot
The uterine body is ligated using a modified Miller’s knot. There is no need to place any hemostatic forceps on the uterine body as the modified Miller’s knot is a very secure, self-locking knot. To place a modified Miller’s knot, pass the suture under the uterine body, and bring the suture back over the tissue and under the body one more time. This creates a loop of suture above the uterine body. Position the needle holder through that loop, wrap the long strand once around the needle holder, grasp the short strand of suture with the needle holder and pull the needle holder toward you while pulling the long strand of suture away from you. Gentle upward tension while pulling this knot tight facilitates placement of the ligature. Complete the knot by placing three or four square knot throws (Figure 3). 19 (A video of the modified Miller’s knot is available as supplementary material.)
Figure 3.
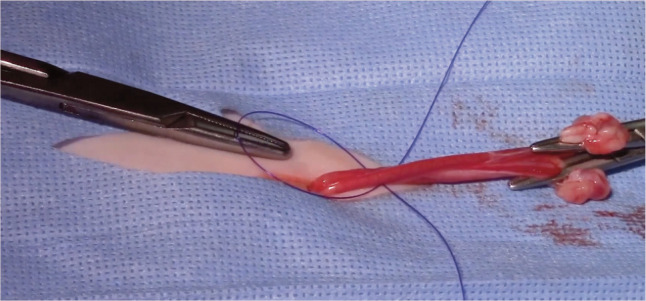
The modified Miller’s knot is a very secure, self-locking knot
Closure
Closure of a small abdominal wall incision can generally be accomplished with one or two cruciate sutures. The skin incision can be closed with one or two buried simple interrupted subcuticular sutures.
Tattoo or ear tip
It is recommended that veterinarians tattoo all cats when they are spayed or castrated. The ASV recommends the use of green tattoo ink placed in or adjacent to the ventral abdominal incision for a spay and, for cat castrations, a ventral abdominal tattoo on or near the midline. 9 A simple technique to tattoo the cat is to make a partial thickness incision in the skin adjacent to the spay incision. The incision should not penetrate the full thickness of the dermis. Then, using either a sterilization indicator strip (Steri-Strip) from the surgery pack or the back of a sterile scalpel blade, apply a small amount of green tattoo ink into the incision and seal with skin glue (Figure 4). (A video of the scoring technique is available as supplementary material.) The only exception to tattooing sterilized cats is in feral (community) cats, which should be ear tipped. The purpose of the tattoo or ear tip is to communicate to other veterinarians that the cat has been sterilized.
Figure 4.
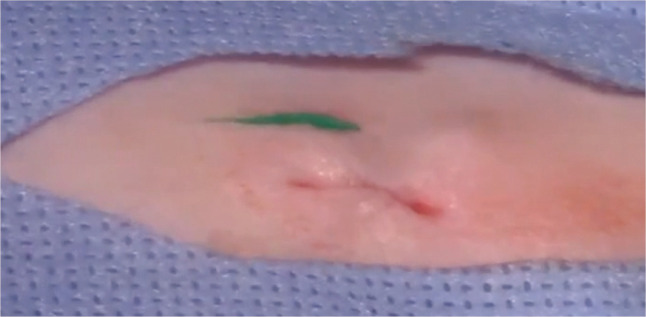
Scoring tattoo. A small tattoo on the ventral abdomen identifies that the cat has been sterilized

Successes
The surgical techniques developed in HQHVSN clinics are efficient and safe. They have been used successfully by the ASPCA’s National Spay/Neuter Response Team’s network of approximately 150 HQHVSN clinics, which have performed collectively over 6 million surgeries across the USA, with minimal complications. In the author’s opinion, the techniques are easy to learn and can be used by anyone performing spays and neuters in private veterinary practice.
The number of animals euthanized annually in animal shelters has dropped from between 22 and 24 million in the early 1970s to the current estimate of 1.5 million. 21 Many factors have contributed to the dramatic decrease in euthanasia rates in shelters and HQHVSN is only one of them. Increased public awareness of pet overpopulation, increased acceptance of spay–neuter surgery, improvements in shelter management, transport programs moving adoptable animals from high intake shelters to low intake shelters, and an increased tendency to adopt rather than purchase have all played a role. The success of HQHVSN clinics in this effort is that they have provided an avenue for individuals who cannot afford the fees at full-service clinics to have their pets spayed or neutered at a lower cost. Likewise they have provided a means for shelters with limited financial resources to get animals in their care sterilized prior to adoption and a means for caretakers of community cat colonies to get unowned community cats sterilized.
Challenges
The principal challenge associated with HQHVSN clinics is the perception of many veterinarians that they take clients away from the private practitioner. Evidenced-based statistics do not exist to either prove or disprove this perception. However, with the cost of veterinary services under increasing scrutiny, and the resulting financial barriers that millions of pet owners face in obtaining access to veterinary care, the private practitioner can embrace the challenge and play an increased role. There is a population of pet owners who cannot afford the current costs of spay–neuter surgery at full-service veterinary clinics. Simply forsaking those potential clients will have one of two potential consequences, as discussed earlier – either a growing number of pets will go without basic care or low-cost clinics will increase in number and in services offered. History has shown that humane organizations will step forward to close the gap in access to care, just as they did with spay–neuter (see box above). Foreseeably, HQHVSN clinics will begin to provide additional services or non-profit low-cost wellness and full-service clinics will spring up.
The issue of access to care still includes spay–neuter. In the 30 years since Dr Gordon Robinson’s article was published (see box), 5 HQHVSN clinics have been established all over the USA and euthanasia rates in shelters have decreased dramatically courtesy of systems and techniques that have been developed which greatly improve the efficiency of spay–neuter surgery. Improved efficiency means less time and, therefore, less expense. The private practitioner who adopts these efficient systems and techniques and passes the savings on to clients can maintain a spay–neuter clientele and perhaps acquire new clients who will use other veterinary services as well.
The same applies to the private practitioner who adopts the practice of spay–neuter of cats under 5 months of age and passes the savings on to clients. We have learned that not only is it safe to spay–neuter cats at an earlier age, it is beneficial to do so, and the AVMA, AAHA, AAFP, ASV and others have endorsed this practice. We also know that spay–neuter of cats less than 5 months of age is easier and faster than surgeries at the more traditional age of 6 months or older; it is, therefore, less expensive.
The impetus for private practitioners to face these challenges is growing. We are, for example, now seeing the establishment of walk-in veterinary clinics in Walmart Supercenters that offer ‘affordable services for dogs and cats that include vaccinations, grooming, diagnostics, preventive care and minor medical treatments’. 22 The options are to sit back and watch these clinics develop over the next 50 years, expressing concern about quality of care and fearing the loss of clients, or alternatively develop the efficient systems and techniques that lower the cost and pass those savings on to clients.
It is abundantly clear to this author that private practitioners can and must address the access to care issues, or someone else will.
Key Points
HQHVSN clinics have developed extremely efficient systems and surgical techniques that reduce time and cost, and which can easily be adopted by private veterinary practitioners.
Spay–neuter of cats prior to 5 months of age is easier, faster and safer than delaying surgery to 6 months of age or older. The concept has been endorsed by the AVMA, AAHA, AAFP, ASV and numerous humane organizations.
Efficient techniques for ovariohysterectomy in the cat include small, appropriately placed abdominal incisions, the use of a spay hook, cutting the suspensory ligaments, ligation of ovarian vessels using the pedicle tie and ligation of the uterine body with a modified Miller’s knot.
As the cost of veterinary education and veterinary care continues to rise, an increasing percentage of households cannot afford basic veterinary care for their pets.
Veterinarians are challenged to adopt efficient spay–neuter systems and techniques to reduce the cost of surgery. They are also more generally challenged to develop low-cost efficient systems for delivery of basic care.
Footnotes
The author declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding: The author received no financial support for the research, authorship, and/or publication of this article.
Ethical approval: This work did not involve the use of animals and therefore ethical approval was not required.
Informed consent: This work did not involve the use of animals and therefore informed consent was not required. No animals or humans are identifiable within this publication, and therefore additional informed consent for publication was not required.
References
- 1. Access to Veterinary Care Coalition. Access to veterinary care: barriers, current practices and public policy. http://avcc.utk.edu/avcc-report.pdf (2018, accessed May 6, 2019).
- 2. LaVallee E, Mueller MK, McCobb E. A systematic review of the literature addressing veterinary care for underserved communities. J Appl Anim Welf Sci 2017; 20: 381–394. [DOI] [PubMed] [Google Scholar]
- 3. Burns K. How to thrive in practice. J Am Vet Med Assoc 2019; 254: 1251–1257. [Google Scholar]
- 4. Burns K. Competition or coexistence? Relations strained between private practitioners, animal welfare organizations that provide veterinary services. https://www.avma.org/News/JAVMANews/Pages/120901a.aspx (2012, accessed June 5, 2019).
- 5. Robinson G. How to keep a humane society hospital out of your community. Vet Econ June 1990; 32–41. [Google Scholar]
- 6. Fricke I. Every animal deserves access to veterinary care. The Humane Society of the POINTS United States. https://www.animalsheltering.org/blog/every-animal-deserves-access-veterinary-care (2016, accessed June 6, 2019).
- 7. Phillips SC, Hedge Z, Peralta JM. The role of private practitioners in reducing numbers of homeless dogs and cats and shelter euthanasia rates [viewpoint]. J Am Vet Med Assoc 2018; 253: 404–408. [DOI] [PubMed] [Google Scholar]
- 8. Looney AL, Bohling MW, Bushby PA, et al. The Association of Shelter Veterinarians veterinary medical care guidelines for spay–neuter programs. J Am Vet Med Assoc 2008; 233: 74–86. [DOI] [PubMed] [Google Scholar]
- 9. Griffin B, Bushby PA, McCobb E, et al. The Association of Shelter Veterinarians’ 2016 veterinary medical care guidelines for spay–neuter programs. J Am Vet Med Assoc 2016; 249: 165–188. [DOI] [PubMed] [Google Scholar]
- 10. Levy JK, Bard KM, Tucker SJ, et al. Perioperative mortality in cats and dogs undergoing spay or castration at a high-volume clinic. Vet J 2017; 224: 11–15. [DOI] [PubMed] [Google Scholar]
- 11. Benka VA, McCobb E. Characteristics of cats sterilized through a subsidized, reduced-cost spay–neuter program in Massachusetts and of owners who had cats sterilized through this program. J Am Vet Med Assoc 2016; 249: 490–498. [DOI] [PubMed] [Google Scholar]
- 12. Root MV, Johnston SD, Johnston GR, et al. The effect of prepubertal and postpubertal gonadectmy on penile extrusion and urethral diameter in the domestic cat. Vet Radiol Ultrasound 1996; 37: 363–366. [Google Scholar]
- 13. Dale S. When to spay/neuter cats? Vet consensus says fix by five months. Vet Pract News. https://www.veterinarypracticenews.com/when-to-spayneuter-cats-vet-consensus-says-fix-by-five-months/ (2016, accessed June 7, 2019).
- 14. Land T, Wall S. Survey of the Coalition of Spay/Neuter Veterinarians. J Am Vet Med Assoc 2000; 216: 659–660.10707675 [Google Scholar]
- 15. AVMA. New recommendations for feline spay/neuter surgery. https://www.avma.org/blog/new-recommendations-feline-spayneuter-surgery (2017, accessed June 7, 2019).
- 16. Thomas CRS. AAFP position statement: early spay and castration. https://catvets.com/public/PDFs/PositionStatements/EarlySpay&Neuter.pdf (2012, accessed June 7, 2019).
- 17. Feline Fix by Five. Endorsements. https://www.felinefixbyfive.org/endorsements (accessed June 7, 2019).
- 18. Griffin B, DiGangi B, Bohling M. A review of neutering cats. In: August JR. (ed). Consultations in feline internal medicine. 6th ed. St Louis, MO: Elsevier Saunders, 2010, pp 776–790. [Google Scholar]
- 19. Shaver SL, Yamada N, Hofmeister EH. In vitro security of 3 surgical knots placed by novice veterinary students. Vet Surg 2018; 48. DOI: 10.1111/vsu.13143. [DOI] [PubMed] [Google Scholar]
- 20. Miller KP, Rekers W, Ellis K, et al. Pedicle ties provide a rapid and safe method for feline ovariohysterectomy. J Feline Med Surg 2015; 18: 160–164. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21. ASPCA. Pet statistics. Shelter intake and surrender. https://www.aspca.org/animal-home-lessness/shelter-intake-and-surrender/pet-statistics (accessed June 7, 2019).
- 22. Fiala J. Walk-in veterinary care proliferates inside Walmart Superstores. VIN News Service. https://news.vin.com/VINNews.aspx7articleId=53782 (2019, accessed October 6, 2019). [Google Scholar]