

Abstract
Background:
Lymphoma is a common malignant proliferative disease in which bone marrow infiltration will upstage the disease and thus affect prognosis of the disease. As of now bone marrow biopsy is considered as a reference standard to find out bone marrow involvement in lymphoma. Performing an invasive and painful intervention in all newly diagnosed lymphoma patients is controversial. PET-CT is a non-invasive technique that gives functional information about the cells using the glucose metabolism. It can detect early bone marrow and extra medullary organ involvement which can lead to restaging of the disease. These advantages make PET-CT a valuable adjunct in diagnosis of lymphoma.
Aims and Objectives:
Our study aims to evaluate the usefulness of 18 F-FDG PET-CT, a non-invasive, semi quantitative whole body imaging technique for detection of early bone marrow and extra medullary organ involvement in lymphoma patients which in turn can obviate the need for bone marrow study (BMS). The primary objective of study is to categorise FDG uptake in bone marrow as diffuse /unifocal /multifocal / no uptake and to correlate pattern of FDG uptake to bone marrow study. Our study also assesses the role of FDG PET/CT in staging of lymphoma.
Materials and Methods:
Thirty patients with newly diagnosed lymphoma in the age group 18 to 75 years of both sexes within 3 months of diagnosis and who have not been started on any treatment was included in the study. Marrow uptake on FDG PET/CT has been categorized as diffuse, unifocal, multifocal and no uptake. Agreement between bone marrow study and FDG PET/CT has been assessed by reliability analysis using Cohen’s kappa. Sensitivity, specificity, PPV, NPV of PET/CT in detecting marrow involvement have been calculated.
Results:
The sensitivity, specificity, PPV, NPV and accuracy of 18 F-FDG PET-CT in detecting marrow involvement of lymphoma cases are 86.6%, 77.7%, 68.4%, 91.3% and 80.9% respectively. 18 F-FDG PET-CT detected bone marrow involvement in 86.6% (13 out of 15 total positive cases) cases of lymphoma which included both HL and NHL. Reliability analysis using Cohen’s kappa is used to test the agreement between bone marrow study and 18F-FDG PET/CT. k value of 0.6 was obtained which showed a moderate agreement between bone marrow study and 18F-FDG PET/CT in marrow assessment.
Conclusion:
18F‐FDG PET/CT is a highly sensitive imaging modality which can pick up extra‐nodal organ and BMI in patients with lymphoma and can upstage the disease and alter treatment strategies. PET‐CT cannot completely replace the bone marrow study. However, being an invasive painful procedure, BMB can be avoided in cases with unifocal or multifocal marrow involvement on PET‐CT.
Keywords: 2-(fluorine-18) fluoro-2-deoxy-D-glucose positron emission tomography/computed tomography, Bone marrow aspiration, bone marrow biopsy
Introduction
Lymphomas are the heterogeneous group of neoplasms that arise from the constituent cells of immune system or from their precursors.[1] They are broadly divided into two main categories: Non-Hodgkin’s lymphoma (NHL) and Hodgkin’s lymphoma (HL). Lymphomas as a group account for one of the most common malignant disease of the world comprising 3.37% of all malignancies worldwide.[2,3] They have widely varied clinical features, histology, immunophenotypes, and genetic abnormalities. HL has a steady annual incidence of 3 cases/100,000 persons, whereas NHL incidence is increasing annually and accounts for approximately 2.6% of all cancer deaths.[4] Staging of lymphomas is important for providing appropriate therapy and for predicting prognosis. Diagnostic imaging modalities play a very important role in the staging of lymphomas. One of the most used imaging modalities for staging lymphoma is computed tomography (CT). The criteria for predicting nodal involvement in anatomical imaging modalities such as CT and magnetic resonance imaging (MRI) are primarily based on size of the lymph nodes. However, tiny lymph nodes (<1 cm size) can be sometimes metastatic, whereas large lymph nodes can be benign. These factors contribute to the low specificity in detecting nodal involvement based on anatomical imaging modalities such as CT and MRI. These imaging modalities are also not very reliable in predicting bone marrow involvement (BMI) and CT subjects the patient to increased doses of ionizing radiations.
The use of functional imaging modalities like 2-(fluorine-18) fluoro-2-deoxy-D-glucose positron emission tomography/CT (18F-FDG PET-CT) helps in detecting metabolic changes in malignant cells before structural abnormalities become evident and thereby helps in proper staging and disease evaluation. PET-CT can pick up more metabolically active lymph nodes, bone marrow, splenic, skeletal, and gastrointestinal involvement which will upstage the stage of disease.
Early detection of BMI is crucial as it can alter staging and clinical management and thereby affects the prognosis of the disease. Lymphoma is a common malignant proliferative disease in which bone marrow infiltration will upstage Ann Arbor staging to stage IV and thus affect the prognosis of the disease. Bone marrow study which includes both bone marrow aspiration (BMA) and bone marrow biopsy (BMB) plays an important role in staging of lymphoma. Although BMA cannot replace BMB, it is usually considered complementary to BMB.[5,6] BMA is primarily useful for cytological assessment of bone marrow cells. BMB is an invasive procedure which allows histological examination of small portion of bone marrow from the posterior iliac crest or sternum. Performing a BMA along with biopsy helps in earlier and easier availability for bone marrow examination and provides a larger amount of the marrow that can be examined by combining both the procedures.[7] BMI in lymphoma can be focal or diffuse. Hence, there are high chances of sampling error in both BMA and BMB, especially if the marrow involvement in lymphoma is focal or not limited to pelvic bones. As of now BMB is considered as a reference standard to find out BMI in lymphoma. Performing an invasive and painful intervention in all newly diagnosed lymphoma patients is controversial. The present study aims to evaluate the usefulness of 18F-FDG PET-CT, a noninvasive, semi quantitative whole body imaging technique for the detection of early bone marrow and extra medullary organ involvement which in turn can obviate the need for bone marrow study. Over the last few years multiple studies have shown the superiority of PET-CT over BMB for assessing BMI in HL and NHL patients.[8,9,10,11,12] Recent study by Elamir et al. showed that PET-CT can detect more BMI in lymphoma compared with BMB and can replace BMB, especially when there is multifocal marrow involvement in both HL and NHL.[13] As of now, there are no standard international guidelines for indication of PET-CT and BMB in lymphoma patients.[14] Our study aims to add more evidence to the existing study by correlating FDG uptake in PET-CT with bone marrow study in newly diagnosed lymphoma patients.
Aim of the study
The aim of the study is to categorize FDG uptake in bone marrow and to correlate the FDG uptake with bone marrow study. This study also aims to assess the effect of 18F FDG PET-CT on initial staging of lymphoma.
Materials and Methods
This study was conducted in the Department of Nuclear Medicine in collaboration with the Departments of Radiotherapy and Community and Family Medicine, AIIMS, Raipur. Patients were recruited from March 2020 to August 2021 over a period of 18 months. Written informed consent was obtained from all the participants included in the study. Prior permission and approval from the Institutional Ethics Committee was obtained. All newly diagnosed cases of lymphoma (HL and NHL) who presented in the Nuclear Medicine and Radiotherapy departments for 18F-FDG PET-CT scan and who satisfied the inclusion criteria and consented to participate were recruited in the study. All newly diagnosed cases of lymphoma within 3 months of diagnosis are advised to undergo 18F-FDG PET-CT whole body scan and BMA/biopsy with an interval ≤1 month between two studies.
Inclusion criteria
Newly diagnosed lymphoma patients within 3 months of diagnosis who have not been started on any treatment
Aged 18–75 years who are willing to give consent.
Exclusion criteria
Age <18 years and >75 years
Pregnant and lactating females
Patients with relapsed lymphoma
Previous/concurrent malignant or granulomatous disease.
2-(Fluorine-18) fluoro-2-deoxy-D-glucose positron emission tomography/computed tomography
Newly diagnosed cases of lymphoma in the age group of 18–75 years of both sexes within 3 months of diagnosis who have not been started on any treatment were subjected to 18F-FDG PET-CT scan
Patients were kept fasting for at least 6 h and fasting blood sugar of <200 mg/dL were given FDG injection
Each patient who was included in the study underwent 18F-FDG PET-CT on GE DISCOVERY MIDR PET-CT scanner. PET- and contrast-enhanced CT images (Vertex to mid-thigh) were acquired 45 min to 1 h following the injection of 0.15 mCi/kg of 18F-FDG. Analysis of FDG uptake was performed semi quantitatively by calculating maximum standardized uptake value (SUV max) value (g/mL) corrected for dose administered and patients body weight
Bone marrow FDG uptake was assessed visually in comparison to liver uptake. Focal and diffuse uptake more than liver uptake was considered as positive
-
FDG uptake on the bone marrow was interpreted under the following headings:
(1) Diffuse (2) Unifocal (3) Multifocal (4) No uptake.
-
PET-CT was considered as true positive (TP) if it satisfied the following criteria:
Positive bone marrow study (either BMA or BMB) with focal FDG uptake corresponding to the area of involvement
Presence of CT morphological changes corresponding to the area of uptake
Resolution of lesions on follow-up PET/CT after treatment
Diffuse heterogeneous marrow FDG uptake with sites of intense focal involvement with corresponding positive BMB or BMA or CT morphological changes.
Remaining case with positive FDG uptake will be considered as false positive (FP)
PET-CT will be taken as false negative (FN) when BMB/BMA is positive and PET-CT is negative
True negative (TN) cases are those with negative BMB/BMA and negative PET-CT
All scans and SUV calculations were independently verified by two experienced nuclear medicine physicians who were blinded to the pathological diagnosis from BMB
Patients were discharged immediately after the scan, as per the radiation safety norms prescribed by the Atomic Energy Regulatory Board for diagnostic nuclear imaging. PET-CT is routinely performed throughout the world and there have been no adverse side effects in subjects having this procedure.
Statistical analysis
Data collected through clinical history, clinical examination, laboratory, histopathological, and immunochemistry investigations were entered in MS EXCEL spreadsheet and were analyzed using the SPSS software-version 21. (IBM; Chicago; Illinois; USA.) Mean ± standard deviation is used for representing the quantitative data. Graphs and frequencies are used for representing qualitative data. For comparison, the Chi-square test for qualitative data and t-test for quantitative data and other appropriate statistical tests were applied. Reliability testing was done using Cohen’s kappa coefficient for qualitative data. P ≤ 0.05 is considered statistically significant.
Results
Out of 42 patients included in the study, 23 (55%) were male and 19 (45%) were female. The mean age group of the study sample was 46.8 ± 17.1 years (Range: −18–75 years). Fourteen out of 42 cases are HL (M:F −2.5:1), whereas remaining 28 are NHL (M:F −0.9:1). Out of 14 cases of HL, 11 (79%) cases are nodular sclerosing variant and the remaining 3 cases (21%) cases are nodular lymphocyte-predominant Hodgkin lymphoma cases. Out of 28 cases of NHL, 13 cases (46%) are diffuse large B-cell lymphoma (DLBCL) subtype, 7 cases (25%) are follicular subtype, and the remaining 31% comprised of other variants such as T-cell lymphoma, mantle cell lymphoma, anaplastic large cell lymphoma, and plasmacytic and low-grade variant [Figure 1].
Figure 1.
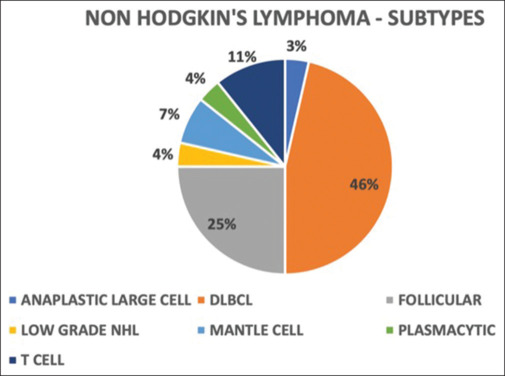
Pie chart depicting subtypes of Non-Hodgkin’s lymphoma in percentage. DLBCL: Diffuse large B-cell lymphoma
Most common clinical presentation was lymphadenopathy (29 out of 42 cases of lymphoma, 69%) and the most common lymph nodal group involved was cervical (17 out of 29 cases which presented with lymphadenopathy, 58%).
Out of 42 cases who had undergone either BMA or BMB or both, 39 patients were subjected to both BMA and BMB, whereas the remaining three patients had undergone BMA alone. BMI was considered positive if either of BMB or BMA shows marrow involvement. A total of eight patients showed marrow involvement in either BMA or BMB or both. Out of these eight patients, 4 showed positive BMB and BMA and the remaining 4 showed only positive BMB. Out of the remaining 34 patients, BMA and BMB were negative in 31 patients and BMB was not done in the remaining three patients with negative BMA.
All patients included in the study were subjected to 18F-FDG PET-CT within 3 months of initial diagnosis of lymphoma (both HL and NHL). PET-CT was done either before or after the bone marrow study. Nighteen out of 42 patients showed positive marrow uptake (>liver uptake) and the rest showed either no uptake or uptake ≤liver uptake and considered as negative. For BMI, pattern of FDG uptake was categorized visually as unifocal, multifocal, diffuse, and no uptake.
Hemoglobin (Hb) in g/dL was documented for all the 42 patients. The mean Hb value was 11.3 ± 2.1 with values ranging from 4.4 g/dL to 14.9 g/dL. Hb values <12 g/dL are considered as anemic irrespective of sex. Six out of seven patients with diffuse FDG uptake on bone marrow were found to have Hb values <12 g/dL (85% cases were anemic). 100% of cases with unifocal and 55% with multifocal marrow uptake were found to be anaemic (Hb <12 g/dL).
In this study, out of eight patients who showed involvement in bone marrow study (either BMB or BMA or both), six patients with FDG marrow uptake were considered as TP and the remaining 2 with no FDG marrow uptake were considered as FN. Among these 6 TP cases, four patients showed multifocal, 1 showed unifocal, and 1 showed diffuse FDG marrow uptake [Figure 2]. TP cases also include seven patients with no marrow involvement on bone marrow study but showed focal FDG uptake (all 7 cases showed multifocal marrow uptake) on 18F-FDG PET-CT with CT morphological changes and few of them showing resolution of marrow uptake in follow up PET-CT. A total of 13 patients (6 + 7) were considered as TP and the remaining 2 cases were considered as FN. Six patients with diffuse bone marrow FDG uptake, negative bone marrow study, and no CT morphological changes were considered as FP. The remaining 21 cases with negative bone marrow study and no FDG marrow uptake in PET-CT were considered as TN. Figure 3 representing case distribution of marrow involvement assessed by bone marrow study (BMS) (BMA and/or BMB) and 18F-FDG PET-CT. The sensitivity, specificity, positive predictive value (PPV), negative predictive value (NPV), and accuracy of 18F-FDG PET-CT for predicting BMI for all lymphoma cases are found to be 86.6%, 77.7%, 68.4%, 91.3%, and 80.9%, respectively.
Figure 2.
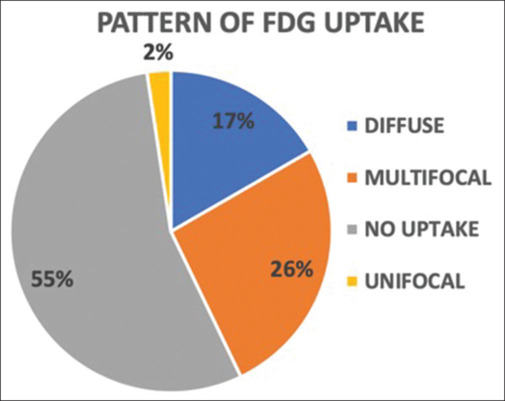
Pie chart showing percentage of different patterns of fluoro-2-deoxy-D-glucose uptake on positron emission tomography/computed tomography. FDG: Fluoro-2-deoxy-D-glucose
Figure 3.
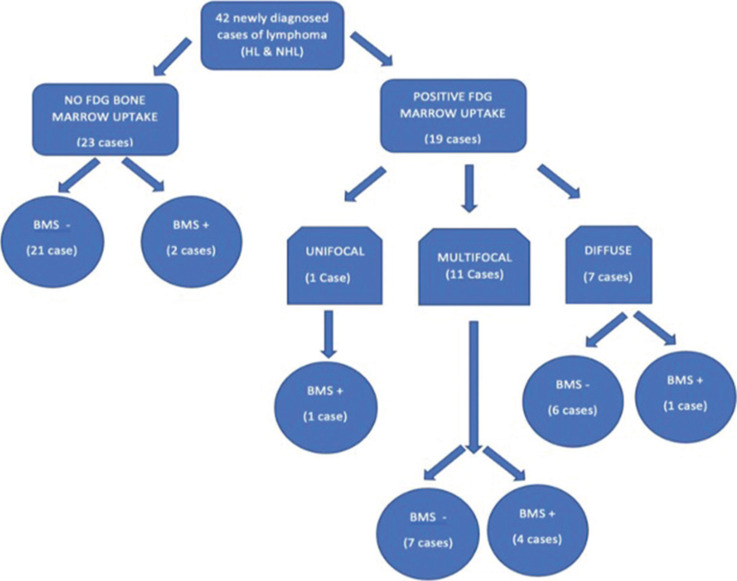
Case distribution of marrow involvement assessed by bone marrow study (bone marrow aspiration and/or bone marrow biopsy) and 2-(fluorine-18) fluoro-2-deoxy-D-glucose positron emission tomography/computed tomography. FDG: Fluoro-2-deoxy-D-glucose, NHL: NonHodgkin’s lymphoma, HL: Hodgkin’s lymphoma, BMS: Bone marrow study
Out of a total of 14 cases of HL, 3 cases showed involvement in BMB and PET-CT (all showed multifocal involvement) and 5 cases showed involvement in PET-CT only (all showed multifocal involvement) with associated CT morphological changes or follow up resolution of lesions. All these were considered as TPs. There were no FN cases. Among the remaining six patients, three patients who showed diffuse marrow uptake in PET-CT with negative BMB were considered as FPs. The remaining three patients with negative BMB and PET-CT were taken as TNs. The sensitivity, specificity, PPV, NPV, and accuracy of 18F-FDG PET-CT for predicting BMI for HL cases are found to be 100%, 50%, 72.7%, 100%, and 78.5%.
A total of 28 cases of NHL were included in the study. TP cases include two cases with BMI on BMS and PET/CT (1-unifocal and 1-diffuse) and 3 cases with BMI on PET/CT only (all showed multifocal involvement) but showed CT morphological changes or follow up resolution of lesions. Out of the remaining 23 patients, two patients (FN) showed involvement in BMS but with negative PET/CT marrow uptake. Three patients who showed diffuse FDG marrow uptake but with negative BMB were included in FP cases. Remaining 18 cases with negative PET/CT and BMB were considered as TNs. The sensitivity, specificity, PPV, NPV, and accuracy of 18F-FDG PET-CT for predicting BMI for NHL cases are found to be 71.4%, 85.7%, 62.5%, 90%, and 82.1%.
Reliability analysis using Cohen’s kappa was used to test the agreement between bone marrow study and 18F-FDG PET/CT. K = 0.6 shows a moderate agreement between bone marrow study and 18F-FDG PET/CT in marrow assessment.
Discussion
BMI in lymphoma plays an important role in upstaging the disease. As of now, BMB is considered as the gold standard for detecting BMI. Performing an invasive and painful procedure in all newly diagnosed lymphoma patients is controversial. BMB allows the histological examination of only a small portion of marrow from the posterior iliac crest, and therefore, can miss marrow involvement in sites other than the posterior iliac crest.[15] This can sometimes down stage the disease and can lead to inappropriate therapy or treatment failure. BMA is considered complementary to BMB. Combining BMA with BMB helps to examine a larger amount of marrow than is done by either of the procedures alone. Both the procedures carry the risk of pain, anxiety, bleeding, and infections.[16] In this study, we assessed the usefulness of staging 18F-FDG PET-CT in picking up marrow involvement among newly diagnosed lymphoma patients. This is a noninvasive procedure which can examine the entire bone marrow and also helps in picking up extramedullary involvement.[17]
We recruited a total of 42 cases of newly diagnosed lymphoma patients (which included 14 Hodgkin’s and 28 NHL cases) within 3 months of diagnosis and compared bone marrow study and 18F-FDG PET-CT scan in evaluating bone marrow among these patients. In our study, there was a male preponderance in HL cases, whereas approximately equal number of both sexes was included in NHL cases. The most common histological subtype among HL cases is nodular sclerosing variant comprising 79% of total HL cases, whereas the most common subtype among NHL cases are DLBCL (46%) followed by follicular (25% of NHL cases) subtypes. The most common clinical presentation was lymphadenopathy (69% of total lymphoma cases) and the most common lymph nodal group involved are cervical lymph nodes (58%).
Previous study by Vishnu et al. showed a low sensitivity of PET/CT in picking marrow involvement as only BMB was taken as the reference standard.[16] In this study, we used CT morphological changes and follow-up evaluation of lesions in patients with negative BMB as additional standard criteria. PET/CT picked up additional 7 cases (53% of TP cases) with negative bone marrow study but with focal FDG uptake in the marrow with either associated CT morphological changes or follow-up resolution of lesions. This is approximately more than twice the number of additional TP cases (22%) picked up by PET-CT in the previous study by Purz et al.[18] However, there were two patients who had BMI on bone marrow study but with no marrow FDG uptake. Both were cases of NHL which included 1 case of low grade NHL and 1 case of follicular lymphoma. Previous studies by Kaddu-Mulindwa et al. showed very low FDG uptake in some histological variants like early follicular or low-grade lymphomas which can be missed in PET/CT as in our case.[19,20]
We had a total of seven cases with diffuse FDG uptake in the bone marrow. Previous studies by Chen-Liang et al., Elamir et al., Khan et al., and Cerci et al. showed BMI in lymphoma cases with diffuse FDG uptake in the marrow. These studies showed the importance of doing a bone marrow study (BMB/BMA) to rule out involvement in cases with diffuse marrow FDG uptake.[12,13,21,22] However, in our study, 6 out of 7 cases with diffuse FDG uptake in marrow showed negative bone marrow study with no CT morphological changes. Five out of these 6 cases were found to be anemic with a Hb value <12 g/dL. Diffuse marrow FDG uptake in these patients is likely due to reactive changes.
Staging of lymphomas is crucial for appropriate therapeutic management and prognostication. PET/CT plays an important role in the initial staging of lymphoma (both HL and NHL). In our study, out of 42 patients, 15 patients (35%) with limited disease (Stage I or II as per Lugano staging) were upstaged to advanced disease (Stage III or IV) after performing PET/CT scan. However, no change in stage was noted in 22 patients (52%).
As per our study, the calculated sensitivity, specificity, PPV, NPV, and accuracy of 18F-FDG PET-CT in detecting marrow involvement of lymphoma cases are 86.6%, 77.7%, 68.4%, 91.3%, and 80.9%, respectively. 18F-FDG PET-CT detected BMI in 86.6% (13 out of 15 total positive cases) cases of lymphoma which included both HL and NHL. The sensitivity of PET/CT in detecting marrow involvement as per our study is 87% which is consistent with a meta-analysis by Wu et al.[23,24] which included 32 studies and found a high sensitivity and specificity of 91.6 and 90.3, respectively. In our study, we got a comparable sensitivity of 87% but a low specificity of 77.7 due to relatively increased number of cases with diffuse marrow uptake which increased the FP outcome. Another meta-analysis study of 587 patients by Pakos et al. showed a sensitivity and specificity of PET/CT in picking up marrow involvement to be 51% and 91%, respectively.[25] As BMB was used as the only reference standard in this meta-analysis, PET/CT was not recommended to replace routine BMB as per this meta-analysis. This is in discordance with the results obtained from our study where we included additional reference standards along with BMB.
In this study, we included 14 cases of HL and 28 cases of NHL. Out of 14 cases of HL, 8 cases had BMI of which only 3 cases showed involvement in BMS and PET-CT, whereas the remaining 5 cases were found to have multifocal involvement in PET-CT alone with concurrent CT morphological changes. As per the above data, PET-CT was found to have a 100% sensitivity in picking up marrow involvement among HL cases. This is consistent with a study by Muzahir et al.[26] which included 122 cases of HL and the sensitivity of 18F-FDG PET-CT in the detection of marrow involvement was found to be 100%.
Among the 28 cases of NHL, the calculated sensitivity, specificity, PPV, NPV, and accuracy of PET-CT for the detection of marrow involvement were 71.4%, 85.7%, 62.5%, 90%, and 82.1%, respectively. PET-CT failed to pick up marrow involvement in two cases (one follicular variant and one low-grade lymphoma) with positive BMS which in turn resulted in a low sensitivity [Figure 4]. Previous study by Cortés-Romera et al. suggested that BMB is still necessary in PET/CT negative cases as there are chances that PET/CT may miss picking up involvement in cases with early limited infiltration of bone marrow.[15]
Figure 4.
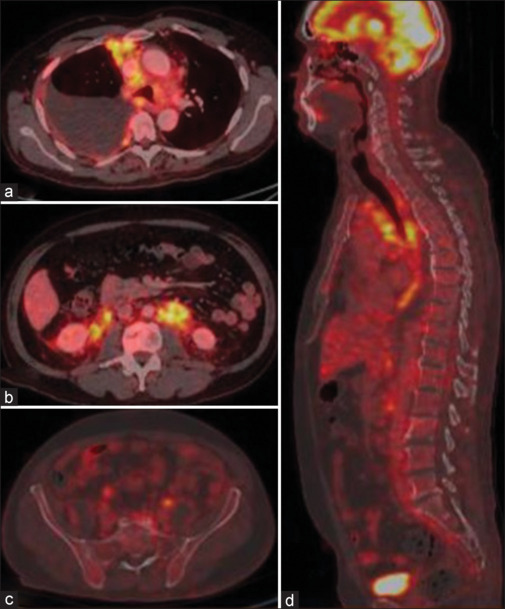
Negative 2-(fluorine-18) fluoro-2-deoxy-D-glucose positron emission tomography/computed tomography (FDG PET-CT) for BMI in indolent follicular variant. (a) Axial fused PET/CT showing FDG avid mediastinal lymph nodes with right pleural effusion, (b) Axial fused PET/CT showing FDG avid retroperitoneal lymphadenopathy, (c) Axial fused PET/CT showing no abnormal increased FDG uptake in pelvic bones, (d) Sagittal fused PET/CT image showing normal marrow
However, PET/CT picked up additional two cases with multifocal marrow involvement which was not detected in BMS [Figure 5].
Figure 5.
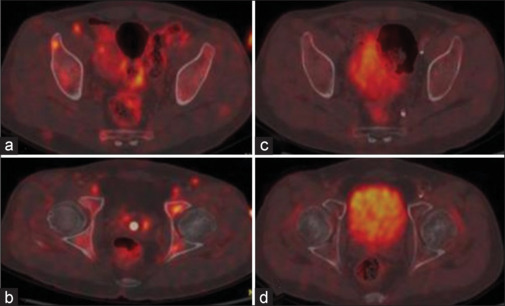
Multifocal marrow uptake in a patient with negative bone marrow study. (a and b) Axial fused positron emission tomography/computed tomography image showing multifocal marrow uptake which got resolved in follow up scan after 6 months (c and d)
In this study, we got a moderate agreement between BMS and PET/CT for the assessment of BMI using Cohen’s k computation. The value of Cohen’s kappa was found to be 0.6. Out of 42 cases of lymphoma included in the study, 34 cases (80%) showed concordant results whereas the remaining 8 cases (20%) showed discordant results. This is consistent with a study by Elamir et al. which included 145 patients and obtained a concordant result in 80.7% of the cases and discordant result in 19.3% of the cases.[13]
Conclusion
18F-FDG PET/CT is a highly sensitive imaging modality which can pick up extra-nodal organ and BMI in patients with lymphoma and can upstage the disease and alter treatment strategies
PET-CT should be done before considering bone marrow study as it can replace bone marrow study, especially in cases with focal marrow involvement
PET-CT-guided BMB will increase the likelihood of picking up marrow involvement, especially unifocal or multifocal involvement from sites other than the iliac crest
Bone marrow study should still be required in cases with diffuse marrow uptake to differentiate tumor infiltration of marrow from reactive marrow
BMA should be considered along with BMB as both the procedures allow examination of a larger amount of marrow and hence are complementary to each other
Bone marrow study can pick up early limited marrow infiltration seen in low-grade lymphomas and certain indolent variants which may be missed in PET-CT
PET-CT cannot completely replace the bone marrow study. However, being an invasive painful procedure, BMB can be avoided in cases with unifocal or multifocal marrow involvement on PET-CT.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
References
- 1.Toma P, Granata C, Rossi A, Garaventa A. Multimodality imaging of Hodgkin disease and non-Hodgkin lymphomas in children. Radiographics. 2007;27:1335–54. doi: 10.1148/rg.275065157. [DOI] [PubMed] [Google Scholar]
- 2.Huh J. Epidemiologic overview of malignant lymphoma. Korean J Hematol. 2012;47:92–104. doi: 10.5045/kjh.2012.47.2.92. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.World Health Organization Global Cancer Observatory. 2021 Available from: https://gco.iarc.fr/ [Last accessed on 2022 Mar 15] [Google Scholar]
- 4.Cronin CG, Swords R, Truong MT, Viswanathan C, Rohren E, Giles FJ, et al. Clinical utility of PET/CT in lymphoma. AJR Am J Roentgenol. 2010;194:W91–103. doi: 10.2214/AJR.09.2637. [DOI] [PubMed] [Google Scholar]
- 5.Atac B, Lawrence C, Goldberg SN. Metastatic tumor: The complementary role of the marrow aspirate and biopsy. Am J Med Sci. 1991;302:211–3. doi: 10.1097/00000441-199110000-00003. [DOI] [PubMed] [Google Scholar]
- 6.Iancu D, Hao S, Lin P, Anderson SK, Jorgensen JL, McLaughlin P, et al. Follicular lymphoma in staging bone marrow specimens: Correlation of histologic findings with the results of flow cytometry immunophenotypic analysis. Arch Pathol Lab Med. 2007;131:282–7. doi: 10.5858/2007-131-282-FLISBM. [DOI] [PubMed] [Google Scholar]
- 7.Musolino A, Guazzi A, Nizzoli R, Panebianco M, Mancini C, Ardizzoni A. Accuracy and relative value of bone marrow aspiration in the detection of lymphoid infiltration in non-Hodgkin lymphoma. Tumori. 2010;96:24–7. doi: 10.1177/030089161009600104. [DOI] [PubMed] [Google Scholar]
- 8.Hamilton R, Andrews I, McKay P, Leach M. Loss of utility of bone marrow biopsy as a staging evaluation for Hodgkin lymphoma in the positron emission tomography-computed tomography era: A West of Scotland study. Leuk Lymphoma. 2014;55:1049–52. doi: 10.3109/10428194.2013.821201. [DOI] [PubMed] [Google Scholar]
- 9.Adams HJ, Kwee TC, de Keizer B, Fijnheer R, de Klerk JM, Littooij AS, et al. Systematic review and meta-analysis on the diagnostic performance of FDG-PET/CT in detecting bone marrow involvement in newly diagnosed Hodgkin lymphoma: Is bone marrow biopsy still necessary? Ann Oncol. 2014;25:921–7. doi: 10.1093/annonc/mdt533. [DOI] [PubMed] [Google Scholar]
- 10.Berthet L, Cochet A, Kanoun S, Berriolo-Riedinger A, Humbert O, Toubeau M, et al. In newly diagnosed diffuse large B-cell lymphoma, determination of bone marrow involvement with 18F-FDG PET/CT provides better diagnostic performance and prognostic stratification than does biopsy. J Nucl Med. 2013;54:1244–50. doi: 10.2967/jnumed.112.114710. [DOI] [PubMed] [Google Scholar]
- 11.Hong J, Lee Y, Park Y, Kim SG, Hwang KH, Park SH, et al. Role of FDG-PET/CT in detecting lymphomatous bone marrow involvement in patients with newly diagnosed diffuse large B-cell lymphoma. Ann Hematol. 2012;91:687–95. doi: 10.1007/s00277-011-1353-6. [DOI] [PubMed] [Google Scholar]
- 12.Khan AB, Barrington SF, Mikhaeel NG, Hunt AA, Cameron L, Morris T, et al. PET-CT staging of DLBCL accurately identifies and provides new insight into the clinical significance of bone marrow involvement. Blood. 2013;122:61–7. doi: 10.1182/blood-2012-12-473389. [DOI] [PubMed] [Google Scholar]
- 13.Elamir Y, Elazab M, Owis AS, Elsayed HF. PET/CT and bone marrow biopsy (BMB) in evaluating bone marrow in lymphoma. Egyp J Radiol Nucl Med. 2020;51:201. [Google Scholar]
- 14.Xiao-Xue W, Xinyue H, Lijun Z. Whole body FDG-PET/CT for the assessment of bone marrow infiltration in patients with newly diagnosed lymphoma. Med Clin (Barc) 2020;154:61–5. doi: 10.1016/j.medcli.2019.07.022. [DOI] [PubMed] [Google Scholar]
- 15.Cortés-Romera M, Sabaté-Llobera A, Mercadal-Vilchez S, Climent-Esteller F, Serrano-Maestro A, Gámez-Cenzano C, et al. Bone marrow evaluation in initial staging of lymphoma: 18F–FDG PET/CT versus bone marrow biopsy. Clin Nucl Med. 2014;39:e46–52. doi: 10.1097/RLU.0b013e31828e9504. [DOI] [PubMed] [Google Scholar]
- 16.Vishnu P, Wingerson A, Lee M, Mandelson MT, Aboulafia DM. Utility of bone marrow biopsy and aspirate for staging of diffuse large B cell lymphoma in the era of positron emission tomography with 2-deoxy-2-[fluorine-18]fluoro-deoxyglucose integrated with computed tomography. Clin Lymphoma Myeloma Leuk. 2017;17:631–6. doi: 10.1016/j.clml.2017.06.010. [DOI] [PubMed] [Google Scholar]
- 17.Ujjani CS, Hill EM, Wang H, Nassif S, Esposito G, Ozdemirli M, et al. (18)F-FDG PET-CT and trephine biopsy assessment of bone marrow involvement in lymphoma. Br J Haematol. 2016;174:410–6. doi: 10.1111/bjh.14071. [DOI] [PubMed] [Google Scholar]
- 18.Purz S, Mauz-Körholz C, Körholz D, Hasenclever D, Krausse A, Sorge I, et al. [18F]Fluorodeoxyglucose positron emission tomography for detection of bone marrow involvement in children and adolescents with Hodgkin’s lymphoma. J Clin Oncol. 2011;29:3523–8. doi: 10.1200/JCO.2010.32.4996. [DOI] [PubMed] [Google Scholar]
- 19.Kaddu-Mulindwa D, Altmann B, Held G, Angel S, Stilgenbauer S, Thurner L, et al. FDG PET/CT to detect bone marrow involvement in the initial staging of patients with aggressive non-Hodgkin lymphoma: Results from the prospective, multicenter PETAL and OPTIMAL >60 trials. Eur J Nucl Med Mol Imaging. 2021;48:3550–9. doi: 10.1007/s00259-021-05348-6. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Weiler-Sagie M, Bushelev O, Epelbaum R, Dann EJ, Haim N, Avivi I, et al. (18)F-FDG avidity in lymphoma readdressed: A study of 766 patients. J Nucl Med. 2010;51:25–30. doi: 10.2967/jnumed.109.067892. [DOI] [PubMed] [Google Scholar]
- 21.Cerci JJ, Györke T, Fanti S, Paez D, Meneghetti JC, Redondo F, et al. Combined PET and biopsy evidence of marrow involvement improves prognostic prediction in diffuse large B-cell lymphoma. J Nucl Med. 2014;55:1591–7. doi: 10.2967/jnumed.113.134486. [DOI] [PubMed] [Google Scholar]
- 22.Chen-Liang TH, Martin-Santos T, Jerez A, Senent L, Orero MT, Remigia MJ, et al. The role of bone marrow biopsy and FDG-PET/CT in identifying bone marrow infiltration in the initial diagnosis of high grade non-Hodgkin B-cell lymphoma and Hodgkin lymphoma. Accuracy in a multicenter series of 372 patients. Am J Hematol. 2015;90:686–90. doi: 10.1002/ajh.24044. [DOI] [PubMed] [Google Scholar]
- 23.Agrawal K, Mittal BR, Bansal D, Varma N, Srinivasan R, Trehan A, et al. Role of F-18 FDG PET/CT in assessing bone marrow involvement in pediatric Hodgkin’s lymphoma. Ann Nucl Med. 2013;27:146–51. doi: 10.1007/s12149-012-0665-5. [DOI] [PubMed] [Google Scholar]
- 24.Wu LM, Chen FY, Jiang XX, Gu HY, Yin Y, Xu JR. 18F-FDG PET, combined FDG-PET/CT and MRI for evaluation of bone marrow infiltration in staging of lymphoma: A systematic review and meta-analysis. Eur J Radiol. 2012;81:303–11. doi: 10.1016/j.ejrad.2010.11.020. [DOI] [PubMed] [Google Scholar]
- 25.Pakos EE, Fotopoulos AD, Ioannidis JP. 18F-FDG PET for evaluation of bone marrow infiltration in staging of lymphoma: A meta-analysis. J Nucl Med. 2005;46:958–63. [PubMed] [Google Scholar]
- 26.Muzahir S, Mian M, Munir I, Nawaz MK, Faruqui ZS, Mufti KA, et al. Clinical utility of ¹⁸F FDG-PET/CT in the detection of bone marrow disease in Hodgkin's lymphoma. Br J Radiol. 2012;85:e490–6. doi: 10.1259/bjr/29583493. [DOI] [PMC free article] [PubMed] [Google Scholar]