

Abstract
A 1-year-old domestic longhair cat presented to our hospital with a 4-month history of progressive exercise intolerance and coughing. Two-dimensional echocardiography confirmed the presence of an intrapericardial cyst and cardiac tamponade. Tamponade was relieved via percutaneous aspiration of the cyst. The cyst was surgically excised 4 days later, and histopathology was consistent with a biliary cyst. The cat's clinical signs completely resolved following surgery.
A 1-year-old, female spayed domestic longhair cat presented to Colorado State University Veterinary Medical Center with a 4-month history of progressive exercise intolerance and coughing. The owner reported the cat would stop playing and begin open-mouth breathing after only a few seconds of activity. Thoracic radiographs taken by the primary care veterinarian 2 weeks prior revealed a severely enlarged and globoid cardiac silhouette, marked compression of the mainstem bronchi, and dorsal elevation of the trachea. Complete blood count showed mild neutropenia (2418; reference range: 2500–12,500/μl). Chemistry profile and total thyroxine (T4) were within normal limits.
On physical examination, the cat appeared quiet, alert, and responsive. Displacement of the precordial impulse to the right axillary region was noted, and although heart sounds were normal in this area, these sounds were decreased elsewhere. Femoral pulses were synchronous but weak. Lung sounds were decreased ventrally and bilaterally, and the cat was mildly tachypneic and dyspneic at rest. No murmur or gallop was ausculted, and the heart rate was normal (200 beats/min) with a regular rhythm. The remainder of the physical examination was unremarkable.
Two-dimensional (2D) echocardiography revealed a large, fluid-filled and loculated cyst within the pericardium (Fig. 1a). The loculations were separated by thin septae and contained predominantly anechoic fluid. The heart was displaced to the cranioventral aspect of the right hemithorax. The loculated fluid was compressing the right atrium (RA) during atrial diastole and the right ventricle (RV) during ventricular diastole resulting in cardiac tamponade (Fig. 1b).
Fig 1.
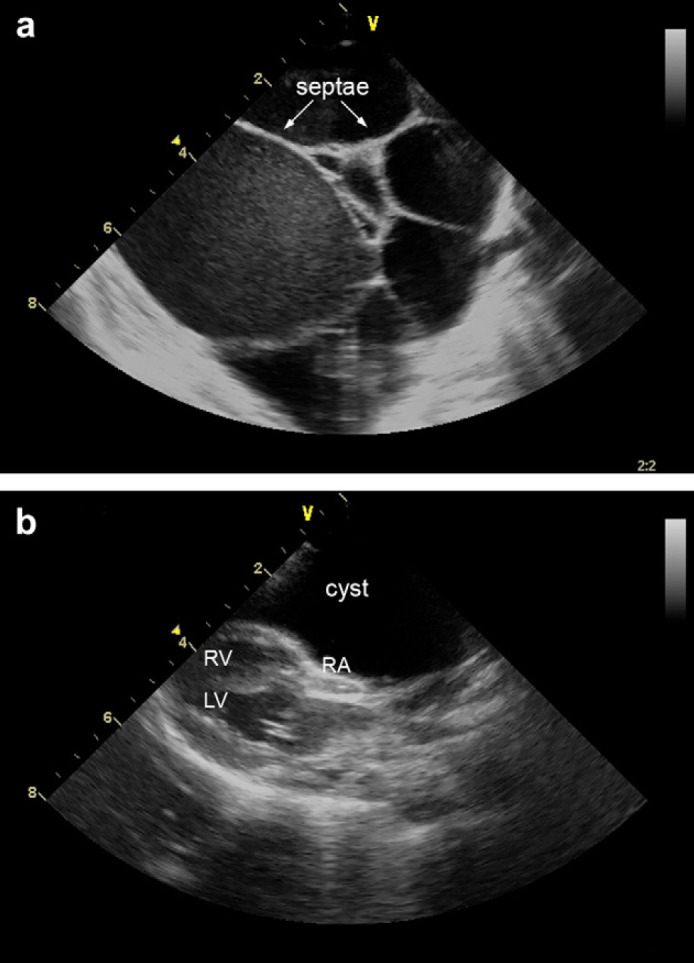
(a): 2D echocardiographic image showing an intrapericardial fluid-filled cyst with compartments separated by septae. (b): 2D echocardiographic image showing compression of the RA and RV by an intrapericardial fluid-filled cyst. LV = 1, left ventricle.
Ultrasonography of the cat's cranial abdomen was performed to evaluate for diaphragmatic herniation. The diaphragm appeared intact. All liver lobes were visualized within the abdomen, but the gall bladder could not be identified. In addition, the caudal vena cava was distended and non-collapsing.
Emergency management included percutaneous aspiration of the cyst to relieve the tamponade and associated clinical signs. Centesis of the cyst yielded 150 ml of clear, yellow fluid. Fluid analysis revealed a modified transudate with a total protein of 6.5 g/dl (albumin/globulin ratio=1.5) and nucleated cell count of 70/μl (mononuclear cells 97%, neutrophils 1%, lymphocytes 2%). No microorganisms or overtly neoplastic cells were seen. The cat's respiratory rate and effort and femoral pulse strength improved following aspiration of the cyst. Repeat echocardiography revealed marked reduction of the loculated fluid and improved right ventricular filling.
After a 4-day convalescence, an exploratory thoracotomy was performed to further characterize and treat the intrapericardial cyst. At surgery, a small (5 mm) defect in the diaphragm was found. The gall bladder, a small portion of liver, and a large (10×5×5 cm) cyst were identified within the pericardial cavity. The cyst was adjacent to the right side of the heart thereby preventing normal excursion of the right atrial and right ventricular walls. The herniated liver and cyst were excised (Fig. 2) and submitted for histopathology. The gall bladder was salvaged and replaced in the abdominal cavity, and the diaphragm was repaired. Histopathology was consistent with a biliary cyst, which is a benign lesion. Cystic fluid was submitted for hepatic biochemical analysis (ie, total bilirubin, alkaline phosphatase, alanine aminotransferase, aspartate aminotransferase, and gamma glutamyl transferase). Alkaline phosphatase was low (7; reference range: 11–61 IU/l), and all other parameters were within normal limits. The cat recovered from surgery without complication, and the owner reported complete resolution of clinical signs.
Fig 2.
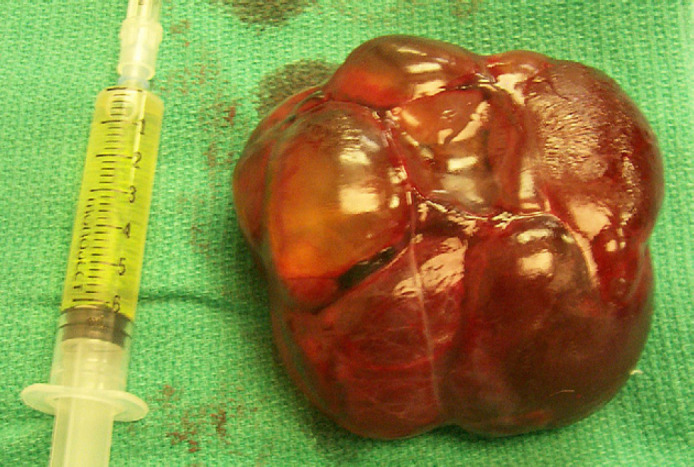
Biliary cyst and herniated liver following excision from the pericardial cavity. The adjacent syringe contains clear, yellow fluid which was aspirated from the cyst.
Cardiac tamponade describes a situation wherein ventricular filling is diminished due to increased intrapericardial pressure. 1,3 Intrapericardial pressure increases most commonly as a result of free fluid within the pericardial cavity; however, the presence of loculated or localized fluid within the pericardium can also result in tamponade. 1,4
Intrapericardial cyst is a rare pericardial congenital anomaly in both cats and dogs, but commonly causes cardiac tamponade in dogs when present. 2 Of the previously reported cases of intrapericardial cysts in cats, one of two cats had tamponade due to the cyst. 5,6 Pericardial cyst is also a reported cause of tamponade in humans. 4 Canine and feline intrapericardial cysts may share a common developmental mechanism. The previous report of intrapericardial cysts in dogs suggests a mechanistic link between congential herniation of abdominal tissue and formation of the cyst, and all three reported cases of intrapericardial cysts in cats have been associated with peritoneopericardial diaphragmatic hernia (PPDH). 2,5,6 The type of herniated abdominal tissue is variable. The histologic findings of canine intrapericardial cysts suggest that omentum or falciform ligament may be the tissue of origin. 2 Feline intrapericardial cysts, thus far, appear to originate from hepatobiliary tissue. 5,6
PPDH and chronic pericardial effusion were considered in this cat based on the history, physical examination, and thoracic radiographs. In contrast, acute pericardial effusion usually results in an abrupt onset of cardiogenic shock. 1 Ascites, while present in many dogs with chronic pericardial effusion, is less common and variable in cats. 3
The case described here represents the third report of intrapericardial cyst in a cat, and the second case of cardiac tamponade due to intrapericardial cyst. 5,6 The duration of clinical signs in the two previously reported cats was relatively short (ie, days to weeks). Uniquely, the cat in this report had chronic (ie, 4 months) signs of illness demonstrating that intrapericardial cyst may manifest as either acute or chronic disease. Intrapericardial cyst should be a differential diagnosis in any cat with an enlarged, globoid cardiac silhouette on radiographs and/or suspected to have cardiac tamponade. Additionally, cats with intrapericardial cyst may present for signs of respiratory disease (eg, coughing, dyspnea). Emergency management of tamponade includes percutaneous aspiration of the cyst. Fluid analysis can be performed to determine the general character of the fluid and to evaluate for evidence of infection and neoplasia. Although biochemical analysis of the cystic fluid can also be performed, this analysis may not provide specific information regarding the origin of the cyst. Surgical excision of intrapericardial cyst in cats is curative and carries an excellent prognosis.
References
- 1.LeWinter M.M., Kabbani S. Pericardial diseases. Zipes D.P., Libby P., Bonow R.O., Braunwald E. Braunwald's heart disease, 7th edn, 2005, Elsevier Saunders: Philadelphia, 1762–1765. [Google Scholar]
- 2.Sisson D., Thomas W.P., Reed J., Atkins C.E., Gelberg H.B. Intrapericardial cysts in dogs, J Vet Intern Med 7, 1993, 364–369. [DOI] [PubMed] [Google Scholar]
- 3.Kienle R.D. Pericardial disease and cardiac neoplasia. Kittleson M.D., Kienle R.D. Small animal cardiovascular medicine, 1st edn, 1998, Mosby: St Louis, 413–432. [Google Scholar]
- 4.Patel J., Park C., Michaels J., Rosen S., Kort S. Pericardial cyst: case reports and a literature review, Echocardiography 21, 2004, 269–272. [DOI] [PubMed] [Google Scholar]
- 5.Liptak J.M., Bissett S.A., Allan G.S., Zaki S., Malik R. Hepatic cysts incarcerated in a peritoneopericardial diaphragmatic hernia, J Feline Med Surg 4, 2002, 123–135. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Less R.D., Bright J.M., Orton E.C. Intrapericardial cyst causing cardiac tamponade in a cat, J Am Anim Hosp Assoc 36, 2000, 115–119. [DOI] [PubMed] [Google Scholar]