

Introduction
Circumscribed acral hypokeratosis (CAH) is a rare skin condition with an unknown cause, with fewer than 100 reported cases to date. Typically found on the thenar and hypothenar eminences of middle-aged females, it manifests as asymptomatic depressed erythematous patches with well-demarcated borders [1]. There may be one of more lesions, which persist for extended periods. While malignant transformation is rare, it has been documented in a few cases. Histologically, the epidermal depression corresponds to a reduction in the cornified layer, and the elevated borders indicate hyperkeratosis between the lesion and normal skin [2].
Dermoscopically, the central depressed area exhibits an erythematous pattern with dotted vessels and vascular loops, likely due to thinning of the horny layer and dilatation of dermal capillaries. White dots correspond to the acrosyringium. The peripheral border displays a “stair step” or “geological strata” configuration with skin layer thickening [3]. These distinctive dermoscopic features facilitate the differentiation between circumscribed palmoplantar hypokeratosis and common differentials such as Bowen disease and porokeratosis of Mibelli [4].
Case Presentation
We present 2 cases of CAH and our considerations about the correlation between clinical-dermatoscopic features and the disease activity.
A 78-year-old female presented with 2 depressed erythematous patches on the thenar eminence, with evident elevated scaling borders and atrophy in the middle. Dermoscopy showed erythema and a vascular pattern characterized by dotted vessels and white loops in the center and geological strata aspects in the periphery. The patient reported that these lesions had appeared 4 months before and were increasing in size (Figure 1, A and B).
Figure 1.
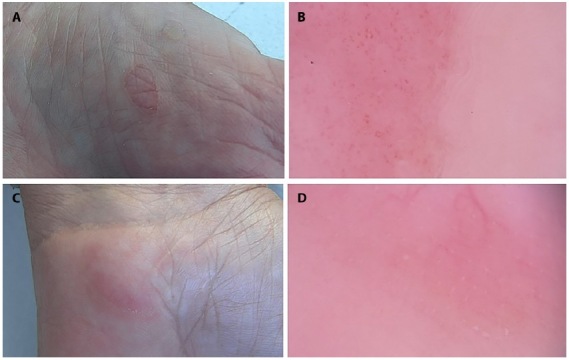
Clinical and dermoscopic aspects of circumscribed palmoplantar hypokeratosis at different stages of evolution. (A) In the first patient, depressed erythematous patches on the thenar eminence, evident elevated scaling borders and atrophy in the middle (B), and dermoscopic features of erythema, dotted vessels, and white loops in the center, and geological strata aspect in the periphery. (C) In the second patient, sightly erythematous atrophic patches with scaly borders on the hypothenar eminence. (D) Dermoscopy showed uniform erythematous pattern, telangiectasia, and borders without a geological strata aspect.
Figure 2.
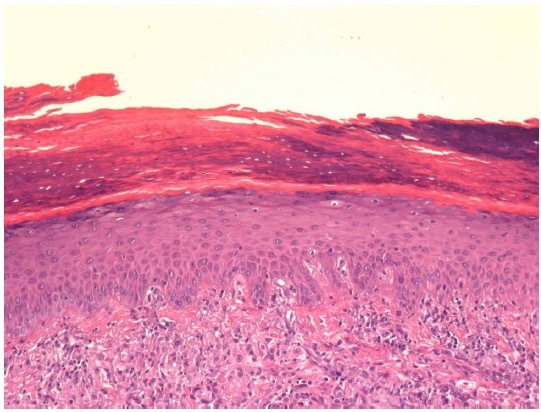
Histological sections of the first patient with active disease: reduction of the cornified layer with a ridge of hyperkeratosis between the lesion and the normal skin.
A 60-year-old female presented with 2 lesions on the hypothenar eminences of both hands, which looked like 2 slightly erythematous atrophic patches with scaly borders. Dermoscopy showed a uniform erythematous pattern with some telangiectasias and a border without the typical geological strata look. There lesions were reported to have been stable for 2 years (Figure 1, C and D).
Conclusions
We hypothesize that the different onset date and evolution might be connected to the slightly different aspects of the lesions. The first patient shows 2 evolving lesions with recent onset, presenting a clear elevated border with the geological strata feature and a rich vascular pattern, while the second had a more stable condition and less evident vessels and peripherical borders. Our hypothesis is that these characteristics, in particular the one on the border, are connected to disease activity, showing a more erythematous vascular pattern with well elevated borders when the lesions are evolving and increasing, and with a low slightly scaly border without a rich vascular aspect in the quiescent phase. This theory fits perfectly with the timing of disease activity in our patients.
Our longstanding lesion findings differ from those recently described by Majluf-Cáceres et al., who reported elongated white structures and a fine white pseudonetwork and hypothesized a correlation with increasing collagen proliferation and thickening [5].
Further research should be conducted with more clinical cases in order to confirm our hypothesis and to deepen our knowledge of the pathogenesis and the evolution.
Footnotes
Funding: None.
Competing Interests: None.
Authorship: All authors have contributed significantly to this publication.
References
- 1.Abignano G, Kapadia A, Lettieri G, et al. Use of optical coherence tomography for the diagnosis of preclinical lesions of circumscribed palmar hypokeratosis. Clin Exp Dermatol. 2017;42(2):192–195. doi: 10.1111/ced.13027. [DOI] [PubMed] [Google Scholar]
- 2.Urbina F, Pérez A, Requena L, Rütten A. Circumscribed Palmar or Plantar Hypokeratosis 10 Years After the First Description: What Is Known and the Issues Under Discussion. Actas Dermo-Sifiliográficas (English Edition) 2014;105(6):574–582. doi: 10.1016/j.adengl.2014.05.015. [DOI] [PubMed] [Google Scholar]
- 3.Topin-Ruiz S, Debarre J-M, Blanchard E, et al. Hypokératose acrale circonscrite (HAC) : utilité diagnostique de la dermoscopie. Annales de Dermatologie et de Vénéréologie. 2017 March;144(3):197–202. doi: 10.1016/j.annder.2016.09.034. [DOI] [PubMed] [Google Scholar]
- 4.Dávila-Rodríguez JJ, García L, Posso D, Argenziano G. Dermoscopy of Circumscribed Acral Hypokeratosis. Dermatol Pract Concept. 2020;11(1):e2020087. doi: 10.5826/dpc.1101a87. Published 2020 Dec 7. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Majluf-Cáceres P, Vera-Kellet C, González-Bombardiere S. New Dermoscopic Keys for Circumscribed Acral Hypokeratosis: Report of Four Cases. Dermatol Pract Concept. 2021;11(2):e2021010. doi: 10.5826/dpc.1102a10. Published 2021 Mar 8. [DOI] [PMC free article] [PubMed] [Google Scholar]