

Abstract
The spinal accessory nerve, considered part of the eleventh cranial nerve, provides motor innervation to sternocleidomastoid and trapezius. A comprehensive literature review and two cadaveric dissections were undertaken. The spinal accessory nerve originates from the spinal accessory nucleus. Its rootlets unite and ascend between the denticulate ligament and dorsal spinal rootlets. Thereafter, it can anastomose with spinal roots, such as the McKenzie branch, and/or cranial roots. The spinal accessory nerve courses intracranially via foramen magnum and exits via jugular foramen, within which it usually lies anteriorly. Extracranially, it usually crosses anterior to the internal jugular vein and lies lateral to internal jugular vein deep to posterior belly of digastric. The spinal accessory nerve innervates sternocleidomastoid, receives numerous contributions in the posterior triangle and terminates within trapezius. Its posterior triangle course approximates a perpendicular bisection of the mastoid-mandibular angle line. The spinal accessory nerve contains sensory nociceptive fibres. Its cranial nerve classification is debated due to occasional non-fusion with the cranial root. Surgeons should familiarize themselves with the variable course of the spinal accessory nerve to minimize risk of injury. Patients with spinal accessory nerve injuries might require specialist pain management.
Keywords: Accessory, Classification, Course, Nerve, Variation
Introduction
The accessory nerve is classified as the eleventh cranial nerve (Binder 2010; Netter 2006; Standring 2005). It was originally named because of its “accessory” cranial input (Hierons and Meyer 1962; Simon et al. 2011; Skinner 1961). It comprises the Spinal Accessory Nerve (SAN), providing motor innervation to sternocleidomastoid (SCM) and trapezius muscles, and a short cranial component, originating from the brainstem. This configuration has conventionally been taught to medical students for decades.
Its function is routinely tested in cranial nerve examinations by turning the head and shrugging the shoulders against resistance. Damage at any point along the nerve’s course results in functional deficit of SCM and trapezius. Pain and reduced range of shoulder motion post-injury can render routine activities like haircombing or dressing difficult (Donner and Kline 1993; Williams et al. 1996), thereby reducing quality of life. In 2007, SAN injury culminated in U.S. court settlements averaging $515,968, increasing to $15 million in recent years (Cesmebasi and Spinner 2015; Morris et al. 2008).
Reviewing the course of the SAN and its common variations will prove beneficial in updating our understanding of the nerve and determining which configuration should be taught in Medical Schools. Appreciating its variations and identifying vulnerable points along its course by means of preoperative imaging will also help prevent SAN injury.
This study provides an in-depth description of the SAN from its origin to its termination and discusses its surface anatomy, composition and questionable cranial nerve classification.
Materials and Methods
An independent review of the literature on the spinal accessory nerve was carried out using Medline, PubMed and Google Scholar including results from January 1946 to May 2023. Terms searched for included combinations of ‘spinal accessory nerve’, ‘cranial nerve XI’, ‘anatomy’, ‘surface anatomy’, ‘variation’, ‘classification’, ‘anastomosis’ ‘nerve injury’, ‘nerve damage’ and ‘imaging’. All primary studies found to be discussing the spinal accessory nerve or its variations, including cadaveric dissections, surgical case studies and ultrasound findings, were considered. References within these articles were also used to discover further relevant papers, including articles prior to 1946. This yielded a total of 121 results. Exclusion criteria were papers referencing distortion of anatomy due to tumours, previous surgery or nerve injury. Nineteen articles were excluded on this basis. This left 102 articles which were stratified into those discussing gross anatomy, surface anatomy, fibre type and cranial nerve classification and miscellaneous information.
A dissection was carried out on two embalmed female cadavers (aged 68 and 90) to accompany this review. On one cadaver, a superficial and deep lateral neck dissection was carried out on one side within the combined parameters of the anterior and posterior triangles of the neck to demonstrate the relationship between the accessory nerve and the surrounding nerves, vasculature and musculature. A deep dissection on the posterior neck was carried out on the other cadaver. The laminae of C1-6 were removed and the dura and arachnoid were reflected with pins to expose the dorsal spinal rootlets and origin of the accessory nerve. A segment of occipital bone superior to the foramen magnum was drilled away and one side of the cerebellum was removed to expose the course of the intracranial accessory nerve.
The authors hereby confirm that every effort was made to comply with all local and international ethical guidelines and laws concerning the use of human cadaveric donors in anatomical research.
The Spinal Accessory Nerve
Origin and Intradural Course
Early human embryo studies have demonstrated the SAN arising from the spinal accessory nucleus, which extends craniocaudally along the C1-6 ventral horns (Pearson et al. 1938). However, the caudal termination of the nucleus is now disputed. Some authors report termination at C5 (Binder 2010; Kiernan 2009; Routal and Pal 2000) and others at C7 (Pearson 1938; Pearson et al. 1964)—a likely reflection of potential variability in this region.
The nucleus gives rise to SAN rootlets (Fig. 1) which either course cranially before exiting the spinal cord or emerge directly from it (Saylam et al. 2009a, b). Classically, the rootlets are described as originating between C1-6 (Standring 2005). However, Saylam et al. found the inferior-most rootlet most commonly emerged from C3 (42.9%) and with progressively less common emergence from lower levels down as far as C5 (Saylam et al. 2009a, b). Established rootlets unite to form a common trunk that ascends cranially adjacent to the spinal cord, dorsal to the denticulate ligament and ventral to the dorsal spinal rootlets (Tubbs et al. 2008) (Fig. 1). There is no documented evidence of deviation from this relationship. The SAN then courses posterior to the vertebral artery (Saylam et al. 2007) and close to the Posterior Inferior Cerebellar Artery (PICA) (Fig. 1). PICA may be absent (Standring 2005) but when present it can course through the SAN rootlets (65%) (Fig. 2), between the vagus and SAN (20%) (Fig. 1) or between the glossopharyngeal and vagus nerves (12.5%) (Saylam et al. 2007) (Fig. 2). The SAN then courses intracranially via foramen magnum and exits through the jugular foramen (Fig. 1). Rarely, it can split and reform between these two foraminae (Tubbs, et al. 2017).
Fig. 1.

Dorsal spinal cord showing path of spinal accessory nerve (SAN) from its rootlets to the jugular foramen. Posterior inferior cerebellar artery (PICA) emerges between SAN and vagus nerve. Cere cerebellum, CNVII/VIII facial-vestibulocochlear nerve complex, CNIX glossopharyngeal nerve, CNX vagus nerve, CRs cranial roots of accessory nerve, DL denticulate ligament, DSR dorsal spinal rootlets, Dura and Arach dura and arachnoid mater, JF jugular foramen, PICA posterior inferior cerebellar artery, PSA posterior spinal artery. SAN spinal accessory nerve, SANr spinal accessory nerve rootlets, VA vertebral artery, IVth fourth ventricle
Fig. 2.

Photograph and Schematic of posterior inferior cerebellar artery penetrating spinal accessory nerve rootlets (A and B) and of posterior inferior cerebellar artery passing between glossopharyngeal and vagus nerves (C and D) (Saylam et al. 2007). B medulla oblongata (bulbous), BA basilar artery, C cerebellum, O olive, P posterior inferior cerebellar artery, VA vertebral artery, VII facial nerve, VIII vestibulocochlear nerve, IX glossopharyngeal nerve, X vagus nerve, XI spinal accessory nerve, Arrow anterior inferior cerebellar artery, Arrowheads rootlets of hypoglossal nerve
The cranial root of the accessory nerve (present in 80% of cases (Tubbs et al. 2017)) emerges from the medulla as 2–9 rootlets (Liu et al. 2014a, b). These emerge singly (34%) or as a union of 2–4 filaments (66%) (Liu et al. 2014a, b) (Fig. 3). The cranial root ascends and fuses with the main trunk of the SAN before entering the jugular foramen; however, they remain as two distinct nerves microscopically (Ong et al. 2010). Conventionally, the cranial root fuses with the superior vagal ganglion at the jugular foramen (Lobstein’s anastomosis (Olry 1995)) and later provides branches supplying the pharynx, larynx and thoracic structures (Katsuta et al. 1997; Kim et al. 2003; Liu et al. 2015; Restrepo et al. 2015; Tubbs et al. 2014b).
Fig. 3.
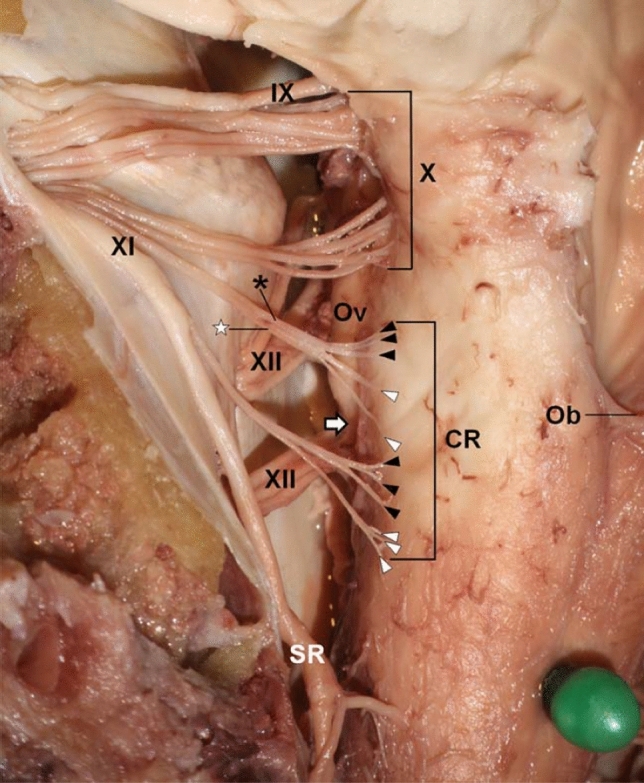
Accessory nerve cranial filaments (arrowheads), rootlets (asterisks) and roots (Liu et al. 2014a) (permission received from publisher for redistribution). CR cranial root, Ob obex, Ov olive, SR spinal root, IX glossopharyngeal nerve, X vagus nerve, XI accessory nerve, XII hypoglossal nerve, Uppermost and next rootlets are indicated by black and white colours respectively. Associated filaments are labelled with the same respective colours
During its ascent, the SAN undergoes numerous anastomoses with spinal rootlets of which the most clinically significant is the McKenzie branch where the SAN fuses with the ventral C1 rootlet (Fig. 4) (Saylam et al. 2009a, b). Its incidence was initially estimated at 50% (McKenzie 1954) but is now thought to vary between 3–7% (Friedman et al. 1993; Oh et al. 2003; Saylam et al. 2009a, b). The assumption that motor fibres coursed from the C1 ventral rootlet into the SAN along the McKenzie branch (McKenzie 1954) has been supported by electrical studies where stimulation of the C1 ventral rootlet resulted in SCM contraction (Friedman et al. 1993). Sometimes, the McKenzie branch causes a debilitating condition called Spasmodic Torticollis or Cervical Dystonia (Freckmann & Hagenah 1986). This involves intermittent, involuntary SCM contraction resulting in a sometimes painful tilting or pulling of the head (DystoniaSociety 2019). Treatment involves severing the McKenzie branch in an operation called Intradural Selective Rhizotomy (Oh et al. 2003).
Fig. 4.

McKenzie branch linking the spinal accessory nerve to a ventral C1 rootlet. a shows accessory nerve in situ, b and c show accessory nerve reflected. Saylam et al. (2009a, b) (permission received from publisher for redistribution). C2 dorsal C2 root, dl denticulate ligament, SC spinal cord, va vertebral artery, XI pinal accessory. Asterisk anterior spinal medullary artery, nerve, Thin arrow McKenzie branch, Thick arrowheads ventral C1 rootlets
Anastomoses also occur with dorsal rootlets. One study documents dorsal rootlet anastomoses occurring 28% medial to the SAN trunk and 2.7% laterally, where medial anastomoses were sensory and lateral anastomoses were predominantly motor (Tubbs et al. 2017) (Fig. 5). Anastomoses were most common between the dorsal C1 rootlet and the SAN (68%) (Ouaknine and Nathan 1973) and occurred at a decreased frequency every level caudal to this until C6 (Oh et al. 2001). The clinical significance of dorsal root anastomoses is currently unknown.
Fig. 5.
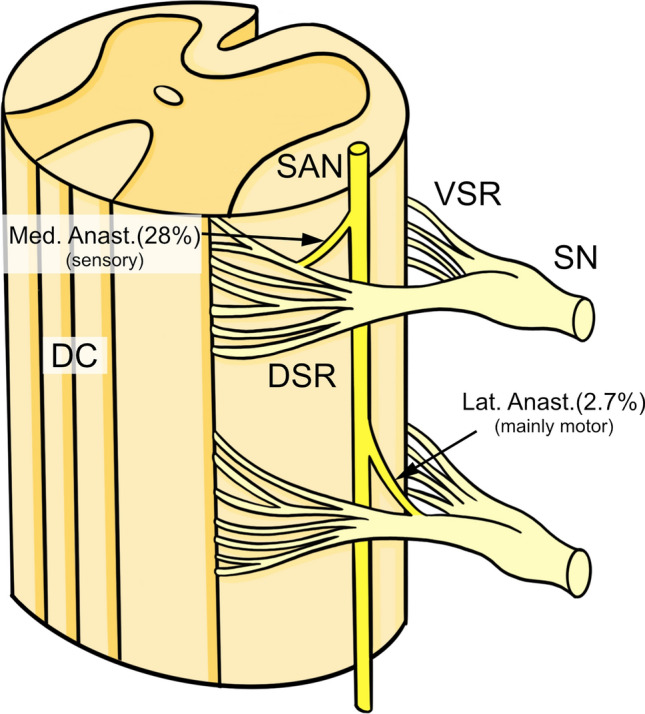
Dorsal root anastomoses occurring medial and lateral to the spinal accessory nerve (SAN) trunk. DC Dorsal Collumn, DSR dorsal spinal root, Lat Anast lateral anastomosis, Med Anast. medial anastomosis, SAN spinal accessory nerve, SN spinal nerve, VSR ventral spinal root
Extradural Course
The course and variation of the SAN in the neck is well documented but its more complicated relationships within the jugular foramen continue to be studied. Within the jugular foramen, Saman et al. (2011) found the nerve coursing anteromedial to the Internal Jugular Vein (IJV) in the majority of cadavers (87%) and posterior to the IJV in a minority (11%). (Fig. 6B). Yigit et al. (2018) found the SAN most commonly coursing anterior to IJV (51.4%) and identified a greater number of variants than the former study with incidences ranging from 1–51% (Fig. 6A). Importantly, both studies concur that surgeons should be particularly vigilant when exploring the anterior jugular foramen to minimize risk of SAN injury.
Fig. 6.

Relationship between spinal accessory nerve (SAN) and internal jugular vein (IJV) within the jugular foramen according to (A) Yigit et al. (2018) and (B) Saman et al. (2011) (exterior skull base views), CA carotid artery, IJV internal jugular vein
The SAN emerges from the jugular foramen into the anterior triangle of the neck posterior to the styloid process (Bodner et al. 2002; Kim et al. 2003) and between the IJV and Internal Carotid Artery (ICA) (Leung et al. 2004). It most commonly crosses the IJV anteriorly (56–96%) (Caliot et al. 1989; Kierner et al. 2000; Soo et al. 1986), although one study reports posterior crossing as most frequent (57.4%) (Lee et al. 2009). Less commonly (2.8%), the SAN may pass through a fenestration in the IJV (Iseri et al. 2007; Lee et al. 2009). Rarely, the IJV may be duplicated (0.4% (Prades et al. 2002)) with the SAN traversing inbetween or around the two components (Ibrahim et al. 2016) (Fig. 7).
Fig. 7.

Relationship between the spinal accessory nerve and the internal jugular vein. A and B SAN crossing the IJV anteriorly and posteriorly; C and D SAN passing through/around IJV duplication; E SAN passing through IJV fenestration. IJV internal jugular vein, SAN spinal accessory nerve
Further caudally, the SAN courses deep to the posterior belly of digastric muscle. Here, it most commonly lies lateral to the IJV (70–96%) according to the majority of authors (Agur 2006; Ebling 1997; Hinsley and Hartig 2010; Hone et al. 2001; Kierner et al. 2000; Levy et al. 2001; Netter 2006; Cornelius et al. 1997; Taylor et al. 2013; Yigit et al. 2018) (Fig. 8). Some also report anterior (Agur 2006; Kierner et al. 2000; Netter 2006; Cornelius 1997; Saman et al. 2011; Yigit et al. 2018), posterior (Kierner et al. 2000; Saman et al. 2011; Standring 2005; Yigit et al. 2018) and medial (Ebling 1997; Kierner et al. 2000; Lee et al. 2009) locations as common.
Fig. 8.

Cadaveric dissection showing anterior crossing of spinal accessory nerve (SAN) over internal jugular vein (IJV) and lateral positioning relative to IJV at the posterior belly of digastric muscle. ACIR inferior root of ansa cervicalis, ACSR superior root of ansa cervicalis, CNVII(st) facial nerve stump, CNIX glossopharyngeal nerve, CNIXStPh glossopharyngeal nerve branch to stylopharyngeus muscle, CNX vagus nerve, FA facial artery, ICA internal carotid artery, IJV internal jugular vein, LON lesser occipital nerve, PBoD posterior belly of digastric muscle, SAN spinal accessory nerve, SCM sternocleidomastoid muscle, SCMbr sternocleidomastoid branch of occipital artery, SMG submandibular gland, StH stylohyoid muscle, StPh stylopharyngeus muscle, StP(r) styloid process (reflected), TB temporal bone
The SAN continues inferiorly to innervate SCM. Commonly, branches originating from C1-4, including cervical plexus branches, course adjacent to and sometimes anastomose with the SAN at this point, supplying additional motor fibres to SCM (Kim et al. 2003; Leung et al. 2004; Tubbs et al. 2014b, 2011). The SAN courses deep to SCM and either penetrates the muscle or supplies a branch to innervate its deep surface (Guo et al. 2003; Kim et al. 2003; Lee et al. 2009). It is thought 8% of the SAN fibres terminate to supply SCM and 92% continue to supply the trapezius (Wang et al. 2014). Rarely, the SAN may split into superior and inferior branches prior to SCM, where the former supplies SCM and latter supplies trapezius (Brennan et al. 2015). Interestingly, one case documents an aberrant facial nerve branch innervating SCM, thought to arise due to developmental digastric and SCM fusion (Cvetko 2015).
Termination
The SAN emerges from the posterior border of SCM between a third and half way down the muscle and around 7.5-9 cm superior to the clavicular head (Donner et al. 1993; Leung et al. 2004; Wang et al. 2014). It emerges superior to the Erb’s Point (Aramrattana et al. 2005; Durazzo et al. 2009; Salgarelli et al. 2009), where cervical plexus branches loop around the posterior border of SCM. The SAN then courses obliquely along the posterior triangle, deep to the investing layer of deep cervical fascia (Fig. 9) and superficial to the prevertebral fascia and levator scapulae (Kim et al. 2003; Leung et al. 2004) The average length of the SAN in the posterior triangle ranges from 4.4 to 8.2 cm (Durazzo et al. 2009; Mirjalili et al. 2012; Popovski et al. 2017; Wang et al. 2014), although its tortuous path means its length increases when stretched (Wang et al. 2014).
Fig. 9.

Extradural course and termination of the spinal accessory nerve (SAN). ACSR superior root of the ansa cervicalis, Br.Pl brachial plexus, CbTrap cervical branch to trapezius muscle, CNVII facial nerve stump, CNIX glossopharyngeal nerve, CNX vagus nerve, CP cervical plexus, DSN dorsal scapular nerve, EJV(st) external jugular vein stump, ICA internal carotid artery, IJV internal jugular vein, LON lesser occipital nerve, LS levator scapulae muscle, LTN long thoracic nerve, OmH omohyoid, PBoD posteror belly of digastric muscle, PN phrenic nerve, SAN spinal accessory nerve, ScAnt scalenus anterior muscle, SCM sternocleidomastoid muscle, ScMed scalenus medius muscle, ScPost scalenus posterior muscle, SMG submandibular gland, SSA suprascapular artery, SSV suprascapular vein, St.(r) reflected styloid process, StH stylohyoid, StPh stylopharyngeus, Trap trapezius muscle
The SAN receives numerous anastomoses in the posterior triangle (Brown 2002), prompting Brown (2002) to coin the term “spinal accessory plexus”. Specifically, it can receive contributions from C2-3 branches (Williams et al. 1990), cervical plexus (predominantly the greater auricular nerve (Brown 2002)), brachial plexus, sympathetic chain and other cranial nerves (Brown 2002).
The SAN enters trapezius around 1.5 cm medial to the midclavicular line (Wang et al. 2014) and 4.5 cm from the clavicle (Aramrattana et al. 2005). It innervates all three divisions of the trapezius, whereas the upper and middle portions also receive contributions from C2-3 (Kim et al. 2003). This may explain findings of 90% muscle function being retained after SAN transection (Wang et al. 2014).
Surface Anatomy and Intraoperative Identification
Appreciation of SAN anatomy relative to surrounding landmarks helps minimize risk of iatrogenic injury during procedures like lymph node biopsy and radical neck dissection.
The SAN emerges and exits the posterior triangle 2 cm above and 2 cm below an imaginary horizontal line transecting the thyroid notch (King and Motta 1983). The nerve’s path in the posterior triangle lies approximately along the course of a line joining the transverse process of C2 (just below the mastoid process) and either the tip of the shoulder (Donner et al. 1993; Kim et al. 2003; Sheen et al. 1997) or anterior border of trapezius 3-5 cm superior to the clavicle (Standring 2008). It can also be approximated by a perpendicular bisection of the mastoid-mandibular angle line (Fig. 10) (Chandawarkar et al. 2003).
Fig. 10.

A Line joining C2 transverse process with tip of shoulder. B Perpendicular bisection of mastoid-mandibular angle line (modified from Chandawarkar et al. (2003), permission received from publisher for modification and redistribution)
The significance of where the bisection and posterior SCM intersect is disputed in literature. Some describe it as the emergence of SAN into the posterior triangle (Chandawarkar et al. 2003) whereas others describe it as Erb’s point (Baring et al. 2007; Salsche 1988). This highlights that these descriptions are merely guides and are not wholly accurate. Symes et al. comment that SAN variation within the posterior triangle precludes a working definition of surface anatomy (Symes and Ellis 2005). Clinical estimates of surface anatomy should therefore always be considered in conjunction with conventional neurophysiological methods and imaging.
Techniques for intraoperative SAN identification are invaluable during procedures like radical neck dissection. The most reliable and widely-used marker in surgery is the relationship between the SAN and Erb’s point (Chen et al. 2009; Durazzo et al. 2009; Guo et al. 2003; Hone et al. 2001; Leung et al. 2004; Popovski et al. 2017) (Fig. 11).
Fig. 11.

Spinal accessory nerve (SAN) exiting the posterior border of sternocleidomastoid superior to Erb’s point. CbTrap cervical branch to trapezius, EJV external jugular vein, GAN greater auricular nerve, LON lesser occipital nerve, PN phrenic nerve, PrVF prevertebral fascia, SAN spinal accessory nerve, SCM sternocleidomastoid muscle, SCNs supraclavicular nerves, Superf. V. superficial veins, TCN transverse cervical nerve, Trap trapezius muscle, asterisk Erb’s point
Most studies report SAN lying 0.9–2.0 cm superior to Erb’s point (Chaukar et al. 2006; Chen et al. 2009; Durazzo et al. 2009; Hill and Olson 1979; Hone et al. 2001; Mirjalili et al. 2012; Popovski et al. 2017; Soo et al. 1990, 1986) with a range of 0–3.9 cm (Aramrattana et al. 2005; Salgarelli et al. 2009). In the submandibular region, the SAN usually lies just anterior to the C2 transverse process (77.5%) (Durazzo et al. 2009). It emerges into the posterior triangle at a ratio of 0.34–0.53 craniocaudally along the posterior SCM border (Chaukar et al. 2006; Chen et al. 2009; Hale et al. 2010; Mirjalili et al. 2012) and enters trapezius at the junction between the middle and lower third of its anterior border (Hale et al. 2010). One author reports the latter relationship as one of the most reliable (Durazzo et al. 2009). In practice, neurophysiologic.
Fibre Type
The SAN is conventionally taught as being composed solely of motor fibres innervating SCM and trapezius. This has long-since been recognized and demonstrated through electrical stimulation (Andrei and Marc 2017). However, it is now thought the SAN may be a mixed nerve with a sensory component (Pu et al. 2008; Tubbs et al. 2011), most likely due to anastomoses with the cervical plexus and dorsal spinal roots (Bremner-Smith et al. 1999; Caliot et al. 1989). Embryologically, the SAN is thought to develop as a mixed nerve and the degree to which the sensory component migrates to the dorsal roots determines the proportion of sensory fibres in the SAN. Bremner-Smith et al. (Bremner-Smith et al. 1999) found numerous unmyelinated fibres and small myelinated Ad fibres in the SAN, both of which are sensory and play a key role in nociception. Furthermore, neuronal cell bodies are observed along the SAN which are known to convey nociceptive stimuli from animal studies. Froriep’s ganglion, the existence of which is debated in humans (O'Rahilly and Müller 1984; O’Rahilly and Müller 2007; Pearson 1938; Streeter 1905; Tubbs et al. 2014a), is an embryological structure thought to ultimately form the nociceptive component of the SAN (Wetmore and Elde 1991). Its degeneration in 6–7 week embryos (Sensenig 1957) and visible absence in adults (Cho et al. 2015) is likely a result of programmed autolysis and the degree to which this occurs may explain the limited and variable presence of nociceptive pathways in adults (Cho et al. 2015).
Is the Accessory Nerve Really a Cranial Nerve?
Galen, the early Greek physician, was first to document the presence of cranial nerves. He described seven pairs and defined them as ‘nerves which pass from the brain or brainstem as opposed to the spinal cord (Goss 1966).’ The accessory nerve was given its independent cranial nerve status in 1778 by Soemmering (Soemmerring 1778), whose classification system for cranial nerves is still used today (Eugene 1967; Shaw 1992; Simon et al. 2011). However, the cranial component wasn’t recognised until 1838 when Arnold published a series of elaborately drawn plates showing two components to the accessory nerve (Arnold 1838), that were later eluded to in the first edition of Gray’s Anatomy (Gray 1858).
The cranial root emerges from the medulla and ultimately fuses with the vagus nerve, whereas the SAN emerges from the upper spinal cord. Using Galen’s definition, the cranial root must fuse with the SAN to justify its cranial nerve classification or these structures should be considered as dorsal vagal rootlet and atypical intracranial spinal nerve respectively.
The existence of the eleventh cranial nerve is debated in literature with reports of the cranial root existing in all specimens (Liu et al. 2014a, b), the majority of cases (Tubbs et al. 2014a), variably (Wiles et al. 2007), the minority of cases (Ryan et al. 2007), or not at all (Lachman et al. 2002). Liu et al. (2014a, b) found the cranial root always fused with the SAN and was morphologically distinct from the vagus nerve. However, Lachman et al. (2002) found the cranial root always merged with the vagus nerve without SAN fusion. Such differences can perhaps be attributed to differing investigatory techniques and whether or not the cadaver was embalmed.
Studies describing cranial root existence in the minority of cases were based on small cadaver numbers (n = 11–15) (Lachman et al. 2002; Liu et al. 2014a, b; Wiles et al. 2007) whereas those proposing cranial root existence in the majority involved larger numbers (n = 25–43) (Liu et al. 2014a, b; Tubbs et al. 2014a). Since conventional cranial nerve definition draws upon morphology alone, demonstrating cranial root and SAN fusion in these larger studies could be argued as sufficient justification for the eleventh cranial nerve classification.
However, since the cranial root originates from the same nuclei as the vagus (nucleus ambiguus and dorsal motor nucleus) (Binder 2010; de Oliveira et al. 1985) and has similar functions to the vagus (Kim et al. 2003; Liu et al. 2015; Restrepo et al. 2015; Tubbs et al. 2014b), the cranial root could be considered as a dorsal vagal rootlet. Lachman et al. (2002) suggest that the need for meticulous dissection of the accessory nerve may be a reason for authors having accepted and re-referenced previous literature documenting the existence of the eleventh cranial nerve over the years. Interestingly, in Nkx2.9 gene knockout mice, cranial root development is inhibited whilst the SAN still forms (Dillon et al. 2005; Pabst et al. 1998, 2003; Schubert and Kaprielian 2001), further suggesting disjunction between the two components.
Discussion
The course of the SAN is documented briefly in numerous articles, occasionally alluding to common variations in the posterior triangle, but few papers discuss variations along its entire course. This study offers a contemporary review of articles detailing an account of the nerve’s course from its origin to its termination, referring to literature on anatomical variations at each stage. This may be invaluable for surgeons operating close to the SAN, helping them appreciate its most common and possible configurations, thereby reducing risk of injury.
Due to its variability, classical surface anatomy merely approximates the nerve’s course. Pre-operative ultrasound tracing can result in quicker nerve localization but landmarks often become shifted following the raising of skin flaps (Salgarelli et al. 2009). Intraoperative landmarks can be reliably employed for SAN identification but these can be distorted by scarring from previous surgery (Kretschmer et al. 2001).
The discovery of nociceptive fibres in the spinal accessory nerve suggests the presence of an additional sensory component to the SAN. Their existence should validate the reclassification of the SAN from its conventional entirely motor nerve status to a mixed nerve. Direct injury to nociceptive fibres in SAN injury might explain post-injury shoulder pain—a symptom previously explained by traction neuritis secondary to shoulder droop (Bremner-Smith et al. 1999). This knowledge may change treatment plans for patients with post-operative pain and help provide more targeted management, which could be subject for further studies.
The exact cranial nerve classification of the accessory nerve is not definitive. The outcome of the debate also largely depends on how a cranial nerve is defined. The microscopic composition of the accessory nerve roots was analyzed in one Korean study, revealing that cranial root fibres most commonly split to combine with the vagus and with the SAN separately (Fig. 12) (Liu et al. 2014a, b). Despite the racial bias, these findings supported the current consensus that the accessory nerve should be classified as a cranial nerve with its two components considered functionally separate (Binder 2010; Standring 2005).
Fig. 12.
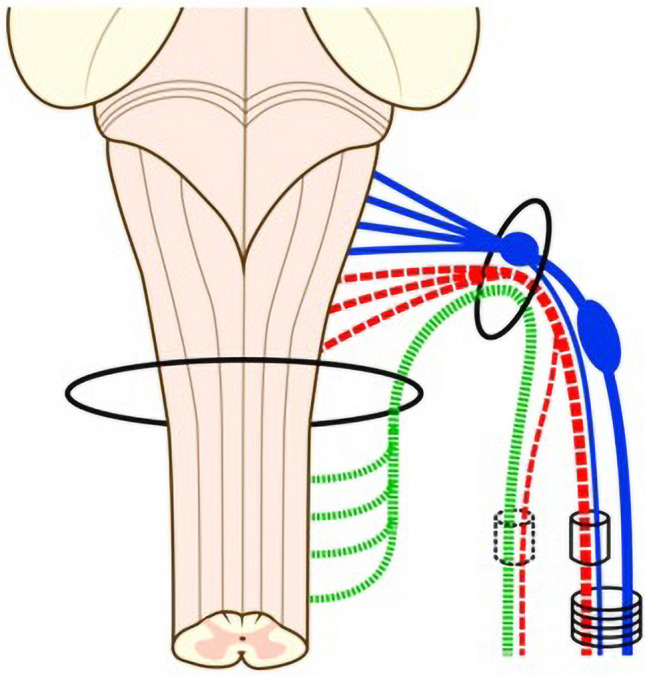
Commonest distribution of the spinal accessory nerve (SAN) cranial root Liu et al. (2014b) (permission received from publisher for redistribution). Blue vagus nerve. Green spinal root of accessory nerve, Red cranial root of accessory nerve
Conclusion
The SAN has a variable course, especially at its origin and adjacent to the IJV. It is suggested that surgeons familiarize themselves with common variations of the SAN to best avoid nerve damage. The SAN should be redefined as a mixed nerve. Its cranial nerve classification is still largely debateable, however, microscopic studies suggest is should be considered as a cranial nerve with two components.
Acknowledgements
No funding or financial grants were received for this project. Thanks to Mrs Sarah Wilson for her support in the dissecting room. The authors sincerely thank those who donated their bodies to science so that anatomical research could be performed. Results from such research can potentially increase mankind's overall knowledge that can then improve patient care. Therefore, these donors and their families deserve our highest gratitude.
Authors contributions
The idea for the article was devised by both authors. S Roberts performed the literature search and analysis. A Cardozo critically revised the work.
Data availability
Not applicable.
Declarations
Conflict of interest
The authors declare that they have no conflict of interest. All authors certify that they have no affiliations with or involvement in any organization or entity with any financial interest or non-financial interest in the subject matter or materials discussed in this manuscript. All cadaveric subjects had provided informed consent and anonymity was preserved at all times. The authors hereby confirm that every effort was made to comply with all local and international ethical guidelines and laws concerning the use of human cadaveric donors in anatomical research.
Ethics approval
Cadavers were kindly donated to the University of Leeds whose ethics board facilitated the necessary approval. The procedures used in this study adhere to the tenets of the 1964 Declaration of Helsinki.
Footnotes
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
References
- Agur AMR. Grant’s atlas of anatomy. 12. Lippincott: Williams & Wilkins; 2006. [Google Scholar]
- Andrei B, Marc S. Functional anatomy of the accessory nerve studied through intraoperative electrophysiological mapping. J Neurosurg. 2017;126(3):913–921. doi: 10.3171/2015.11.JNS15817. [DOI] [PubMed] [Google Scholar]
- Aramrattana A, Sittitrai P, Harnsiriwattanagit K. Surgical anatomy of the spinal accessory nerve in the posterior triangle of the neck. Asian J Surg. 2005;28:171–173. doi: 10.1016/S1015-9584(09)60336-5. [DOI] [PubMed] [Google Scholar]
- Arnold F (1838) Icones nervorum capitis. Sumptibus Auctoris
- Baring DE, Johnston A, O'Reilly BF. Identification of the accessory nerve by its relationship to the great auricular nerve. J Laryngol Otol. 2007;121(9):892–894. doi: 10.1017/S0022215107006251. [DOI] [PubMed] [Google Scholar]
- Binder DK. Cranial Nerves: Anatomy. Pathology and Imaging: Thieme; 2010. [Google Scholar]
- Bodner G, Harpf C, Gardetto A, Kovacs P, Gruber H, Peer S, Mallhoui A. Ultrasonography of the accessory nerve: normal and pathologic findings in cadavers and patients with iatrogenic accessory nerve palsy. J Ultrasound Med. 2002;21(10):1159–1163. doi: 10.7863/jum.2002.21.10.1159. [DOI] [PubMed] [Google Scholar]
- Bremner-Smith A, Unwin A, Williams W. Sensory pathways in the spinal accessory nerve. J Bone Joint Surg Br. 1999;81(2):226–228. doi: 10.1302/0301-620X.81B2.0810226. [DOI] [PubMed] [Google Scholar]
- Brennan PA, Blythe SJ, J, Alam P, Green B, Parry D. Division of the spinal accessory nerve in the anterior triangle: a prospective clinical study. Brit J Oral Maxillofac Surg. 2015;53(7):633–636. doi: 10.1016/j.bjoms.2015.04.010. [DOI] [PubMed] [Google Scholar]
- Brown H. Anatomy of the spinal accessory nerve plexus: relevance to head and neck cancer and atherosclerosis1. Exp Biol Med. 2002;227(8):570–578. doi: 10.1177/153537020222700804. [DOI] [PubMed] [Google Scholar]
- Caliot P, Bousquet V, Midy D, Cabanie P. A contribution to the study of the accessory nerve: surgical implications. Surg Radiol Anat. 1989;11(1):11–15. doi: 10.1007/BF02102238. [DOI] [PubMed] [Google Scholar]
- Cesmebasi A, Spinner RJ. An anatomic-based approach to the iatrogenic spinal accessory nerve injury in the posterior cervical triangle: How to avoid and treat it. Clin Anat. 2015;28(6):761–766. doi: 10.1002/ca.22555. [DOI] [PubMed] [Google Scholar]
- Chandawarkar R, Cervino L, Pennington G. Management of iatrogenic injury to the spinal accessory nerve. Plast Reconstr Surg. 2003;111(2):611–617. doi: 10.1097/01.PRS.0000041943.47622.EB. [DOI] [PubMed] [Google Scholar]
- Chaukar DA, Pai A, D'Cruz AK. A technique to identify and preserve the spinal accessory nerve during neck dissection. J Laryngol Otol. 2006;120(6):494–496. doi: 10.1017/S0022215106000879. [DOI] [PubMed] [Google Scholar]
- Chen DT, Chen PR, Wen IS, Wu HP, Yang PK, Lee CF, Chou YF. Surgical anatomy of the spinal accessory nerve: is the great auricular point reliable? J Otolaryngol Head Neck Surg. 2009;38(3):337–339. [PubMed] [Google Scholar]
- Cho KH, Jang HS, Cheong JS, Rodriguez-Vazquez JF, Murakami G, Abe H. Sensory pathways in the human embryonic spinal accessory nerve with special reference to the associated lower cranial nerve ganglia. Chil Nerv Sys. 2015;31(1):95–99. doi: 10.1007/s00381-014-2546-9. [DOI] [PubMed] [Google Scholar]
- Cornelius RPGR. Hollingshead’s textbook of anatomy. 5. Lippincott: Williams & Wilkins; 1997. [Google Scholar]
- Cvetko E. Sternocleidomastoid muscle additionally innervated by the facial nerve: case report and review of the literature. Anat Sci Int. 2015;90(1):54–56. doi: 10.1007/s12565-013-0224-8. [DOI] [PubMed] [Google Scholar]
- de Oliveira E, Rhoton AL, Jr, Peace D. Microsurgical anatomy of the region of the foramen magnum. Surg Neurol. 1985;24(3):293–352. doi: 10.1016/0090-3019(85)90042-4. [DOI] [PubMed] [Google Scholar]
- Dillon AK, Fujita SC, Matise MP, Jarjour AA, Kennedy TE, Kollmus H, Kaprielian Z. Molecular control of spinal accessory motor neuron/axon development in the mouse spinal cord. J Neurosci. 2005;25(44):10119–10130. doi: 10.1523/JNEUROSCI.3455-05.2005. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Donner T, Kline D. Extracranial spinal accessory nerve injury. Neurosurg. 1993;32(6):907–911. doi: 10.1227/00006123-199306000-00004. [DOI] [PubMed] [Google Scholar]
- Durazzo MD, Furlan JC, Teixeira GV, Friguglietti CUM, Kulcsar MAV, Magalhaes RP, Brandao LG. Anatomic landmarks for localization of the spinal accessory nerve. Clin Anat. 2009;22(4):471–475. doi: 10.1002/ca.20796. [DOI] [PubMed] [Google Scholar]
- DystoniaSociety (2019) Neck problems.
- Ebling DEA. Neck Dissections. Netherlands: Elsevier WB Saunders Company; 1997. [Google Scholar]
- Eugene SF. Historical Observations on the Cranial Nerves. J Neurosurg. 1967;27(4):285–297. doi: 10.3171/jns.1967.27.4.0285. [DOI] [PubMed] [Google Scholar]
- Freckmann N, Hagenah R. Relationship between the spinal accessory nerve and the posterior root of the first cervical nerve in spasmodic torticollis and common autopsy cases. Zentralbl Neurochir. 1986;47(2):134–138. [PubMed] [Google Scholar]
- Friedman AH, Nashold BS, Jr, Sharp R, Caputi F, Arruda J. Treatment of spasmodic torticollis with intradural selective rhizotomies. J Neurosurg. 1993;78(1):46–53. doi: 10.3171/jns.1993.78.1.0046. [DOI] [PubMed] [Google Scholar]
- Goss CM. On anatomy of nerves by galen of pergamon. Am J Anat. 1966;118(2):327–335. doi: 10.1002/aja.1001180202. [DOI] [PubMed] [Google Scholar]
- Gray H. Anatomy, Descriptive and Surgical. 1. Parker and Son, USA: John W; 1858. [Google Scholar]
- Guo CB, Zhang Y, Zhang L, Zou LD. Surgical anatomy and preservation of the accessory nerve in radical functional neck dissection. Chin J Stomat. 2003;38(1):12–15. [PubMed] [Google Scholar]
- Hale SJM, Mirjalili SA, Stringer MD. Inconsistencies in surface anatomy: the need for an evidence-based reappraisal. Clin Anat. 2010;23(8):922–930. doi: 10.1002/ca.21044. [DOI] [PubMed] [Google Scholar]
- Hierons R, Meyer A. Some priority questions arising from Thomas Willis' work on the brain. Proc R Soc Med. 1962;55:287–292. [PMC free article] [PubMed] [Google Scholar]
- Hill J, Olson N. The surgical anatomy of the spinal accessory nerve and the internal branch of the superior laryngeal nerve. Laryngoscop. 1979;89(12):1935–1942. doi: 10.1288/00005537-197912000-00006. [DOI] [PubMed] [Google Scholar]
- Hinsley ML, Hartig GK. Anatomic relationship between the spinal accessory nerve and internal jugular vein in the upper neck. Otolaryng Head Neck Surg. 2010;143(2):239–241. doi: 10.1016/j.otohns.2010.03.033. [DOI] [PubMed] [Google Scholar]
- Hone SW, Ridha H, Rowley H, Timon CL. Surgical landmarks of the spinal accessory nerve in modified radical neck dissection. Clin Otolaryngol Allied Sci. 2001;26(1):16–18. doi: 10.1046/j.1365-2273.2001.00396.x. [DOI] [PubMed] [Google Scholar]
- Ibrahim B, Berania L, Moubayed SP, Christopoulos A, Ayad T. Internal jugular vein duplication: anatomic relationship with the spinal accessory nerve. J Oral Maxillofac. 2016;74(7):1501–1504. doi: 10.1016/j.joms.2016.03.002. [DOI] [PubMed] [Google Scholar]
- Iseri M, Ustundag E, Aydin O. A rare anatomical variation of the spinal accessory nerve. J Laryngol Otol. 2007;121(3):277–278. doi: 10.1017/S002221510600418X. [DOI] [PubMed] [Google Scholar]
- Katsuta T, Rhoton AL, Jr, Matsushima T. The jugular foramen: microsurgical anatomy and operative approaches. Neurosurg. 1997;41(1):149–201. doi: 10.1097/00006123-199707000-00030. [DOI] [PubMed] [Google Scholar]
- Kiernan, JEA. 2009. Barr's The Human Nervous System. An Anatomical Viewpoint. the Point.
- Kierner AC, Zelenka L, Heller S, Burian M. Surgical anatomy of the spinal accessory nerve and the trapezius branches of the cervical plexus. Arch Surg. 2000;135(12):1428–1431. doi: 10.1001/archsurg.135.12.1428. [DOI] [PubMed] [Google Scholar]
- Kim D, Cho YJ, Tiel R, Kline D. Surgical Outcomes of 111 Spinal Accessory Nerve Injuries. Neurosurg. 2003;53(5):1106–1113. doi: 10.1227/01.NEU.0000089058.82201.3D. [DOI] [PubMed] [Google Scholar]
- King RJ, Motta G. Iatrogenic spinal accessory nerve palsy. Ann Roy Coll Surg Eng. 1983;65(1):35–37. [PMC free article] [PubMed] [Google Scholar]
- Kretschmer T, Antoniadis G, Braun V, Rath SA, Richter HP. Evaluation of iatrogenic lesions in 722 surgically treated cases of peripheral nerve trauma. J Neurosurg. 2001;94(6):905–912. doi: 10.3171/jns.2001.94.6.0905. [DOI] [PubMed] [Google Scholar]
- Lachman N, Acland RD, Cornelius R. Anatomical evidence for the absence of a morphologically distinct cranial root of the accessory nerve in man. Clin Anat. 2002;15(1):4–10. doi: 10.1002/ca.1084. [DOI] [PubMed] [Google Scholar]
- Lee SH, Lee JK, Jin SM, Kim JH, Park LS, Chu HR, Rho YS. Anatomical variations of the spinal accessory nerve and its relevance to level IIb lymph nodes. Otolaryng Head Neck Surg. 2009;141(5):639–644. doi: 10.1016/j.otohns.2009.07.005. [DOI] [PubMed] [Google Scholar]
- Leung M, Dieu T, Cleland H. Surgical Approach to the Accessory Nerve in the Posterior Triangle of the Neck. Plast Reconstr Surg. 2004;113(7):2067–2070. doi: 10.1097/01.PRS.0000122236.00292.F7. [DOI] [PubMed] [Google Scholar]
- Levy D, Vacher C, Lezy JP. Relations of the accessory nerve with the internal jugular vein: surgical implications in cervical lymph node clearances. Surg Radiol Anat. 2001;23(3):155–157. doi: 10.1007/s00276-001-0155-2. [DOI] [PubMed] [Google Scholar]
- Liu HF, Won HS, Chung IH, Kim IB, Han SH. Morphological characteristics of the cranial root of the accessory nerve. Clin Anat. 2014;27(8):1167–1173. doi: 10.1002/ca.22451. [DOI] [PubMed] [Google Scholar]
- Liu HF, Won HS, Chung IH, Oh CS, Kim IB. Variable composition of the internal and external branches of the accessory nerve. Clin Anat. 2014;27(1):97–101. doi: 10.1002/ca.22308. [DOI] [PubMed] [Google Scholar]
- Liu HF, Won HS, Chung IH, Kim IB, Han SH. Distribution of the internal branch of the human accessory nerve. Anat Sci Int. 2015;90(3):180–186. doi: 10.1007/s12565-014-0244-z. [DOI] [PubMed] [Google Scholar]
- McKenzie KG. The surgical treatment of spasmodic torticollis. Clin Neurosurg. 1954;2:37–43. [PubMed] [Google Scholar]
- Mirjalili SA, Muirhead JC, Stringer MD. Ultrasound visualization of the spinal accessory nerve in vivo. J Surg Res. 2012;175(1):11–16. doi: 10.1016/j.jss.2011.10.046. [DOI] [PubMed] [Google Scholar]
- Morris LG, Ziff DJ, DeLacure MD. Malpractice litigation after surgical injury of the spinal accessory nerve: an evidence-based analysis. Arch Otolaryngol Head Neck Surg. 2008;134(1):102–107. doi: 10.1001/archotol.134.1.102. [DOI] [PubMed] [Google Scholar]
- Netter F. Atlas of human anatomy. 4. Netherlands: Saunders Elsevier; 2006. [Google Scholar]
- O’Rahilly R, Müller F. The development of the neural crest in the human. J Anat. 2007;211(3):335–351. doi: 10.1111/j.1469-7580.2007.00773.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Oh CS, Chung IH, Koh KS, Kim HJ, Kim SS. Intradural anastomoses between the accessory nerve and the posterior roots of cervical nerves: their clinical significance. Clin Anat. 2001;14(6):424–427. doi: 10.1002/ca.1078. [DOI] [PubMed] [Google Scholar]
- Oh CS, Chung IH, Lee KS. Topographical anatomy on the communicating branch between the spinal accessory nerve and the anterior root of the first cervical nerve. Surg Radiol Anat. 2003;25(3–4):207–209. doi: 10.1007/s00276-003-0108-z. [DOI] [PubMed] [Google Scholar]
- Olry R. Dictionary of anatomical eponyms. USA: Gustav Fischer; 1995. [Google Scholar]
- Ong CK, Chong VFH. The glossopharyngeal, vagus and spinal accessory nerves. Eur J Radiol. 2010;74(2):359–367. doi: 10.1016/j.ejrad.2009.05.064. [DOI] [PubMed] [Google Scholar]
- O'Rahilly R, Müller F. The early development of the hypoglossal nerve and occipital somites in staged human embryos. Am J Anat. 1984;169(3):237–257. doi: 10.1002/aja.1001690302. [DOI] [PubMed] [Google Scholar]
- Ouaknine G, Nathan H. Anastomotic connections between the eleventh nerve and the posterior root of the first cervical nerve in humans. J Neurosurg. 1973;38(2):189–197. doi: 10.3171/jns.1973.38.2.0189. [DOI] [PubMed] [Google Scholar]
- Pabst O, Herbrand H, Arnold HH. Nkx2-9 is a novel homeobox transcription factor which demarcates ventral domains in the developing mouse CNS. Mech Dev. 1998;73(1):85–93. doi: 10.1016/S0925-4773(98)00035-5. [DOI] [PubMed] [Google Scholar]
- Pabst O, Rummelies J, Winter B, Arnold HH. Targeted disruption of the homeobox gene Nkx2.9 reveals a role in development of the spinal accessory nerve. Develop. 2003;130(6):1193–1202. doi: 10.1242/dev.00346. [DOI] [PubMed] [Google Scholar]
- Pearson AA. The spinal accessory nerve in human embryos. J Compar Neurol. 1938;68(2):243–266. doi: 10.1002/cne.900680206. [DOI] [Google Scholar]
- Pearson AA, Sauter RW, Herrin GR. The Accessory nerve and its relation to the upper spinal nerves. Am J Anat. 1964;114:371–391. doi: 10.1002/aja.1001140302. [DOI] [PubMed] [Google Scholar]
- Popovski V, Benedetti A, Popovic-Monevska D, Grcev A, Stamatoski A, Zhivadinovik J. Spinal accessory nerve preservation in modified neck dissections: surgical and functional outcomes. Acta Otolaryngol Ital. 2017;37(5):368–374. doi: 10.14639/0392-100X-844. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Prades JM, Timoshenko A, Dumollard JM, Durand M, Merzougui N, Martin C. High duplication of the internal jugular vein: clinical incidence in the adult and surgical consequences, a report of three clinical cases. Surg Radiol Anat. 2002;24(2):129–132. doi: 10.1007/s00276-002-0020-y. [DOI] [PubMed] [Google Scholar]
- Pu YM, Tang EY, Yang XD. Trapezius muscle innervation from the spinal accessory nerve and branches of the cervical plexus. Int J Oral Maxillofac Surg. 2008;37(6):567–572. doi: 10.1016/j.ijom.2008.02.002. [DOI] [PubMed] [Google Scholar]
- Restrepo CE, Tubbs RS, Spinner RJ. Expanding what is known of the anatomy of the spinal accessory nerve. Clin Anat. 2015;28(4):467–471. doi: 10.1002/ca.22492. [DOI] [PubMed] [Google Scholar]
- Routal RV, Pal GP. Location of the spinal nucleus of the accessory nerve in the human spinal cord. J Anat. 2000;196:263–268. doi: 10.1046/j.1469-7580.2000.19620263.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Ryan S, Blyth P, Duggan N, Wild M, Al-Ali S. Is the cranial accessory nerve really a portion of the accessory nerve? Anatomy of the cranial nerves in the jugular foramen. Anat Sci Int. 2007;82(1):1–7. doi: 10.1111/j.1447-073X.2006.00154.x. [DOI] [PubMed] [Google Scholar]
- Salgarelli AC, Landini B, Bellini P, Multinu A, Consolo U, Collini M. A simple method of identifying the spinal accessory nerve in modified radical neck dissection: anatomic study and clinical implications for resident training. Oral Maxillofac Surg. 2009;13(2):69–72. doi: 10.1007/s10006-009-0152-x. [DOI] [PubMed] [Google Scholar]
- Salsche SJ. Surgical Anatomy of the Skin. Appleton & Lange. 1988;12(116–117):263–265. [Google Scholar]
- Saman M, Etebari P, Pakdaman MN, Urken ML. Anatomic relationship between the spinal accessory nerve and the jugular vein: a cadaveric study. Surg Radiol Anat. 2011;33(2):175–179. doi: 10.1007/s00276-010-0737-y. [DOI] [PubMed] [Google Scholar]
- Saylam C, Ucerler H, Orhan M, Cagli S, Zileli M. The relationship of the posterior inferior cerebellar artery to cranial nerves VII–XII. Clin Anat. 2007;20(8):886–891. doi: 10.1002/ca.20541. [DOI] [PubMed] [Google Scholar]
- Saylam CY, Orhan M, Aktan Ikiz ZA, Uçerler H, Zileli M. Connection types between the spinal root of the accessory nerve and the posterior roots of the C2–C6 spinal nerves. Surg Radiol Anat. 2009;31(6):419–423. doi: 10.1007/s00276-009-0460-8. [DOI] [PubMed] [Google Scholar]
- Saylam CY, Orhan M, Ikiz Z, Ucerler H, Zileli M. The incidence and anatomical features of the McKenzie branch: a cadaver study. Turk Neurosurg. 2009;19(1):42–44. [PubMed] [Google Scholar]
- Schubert W, Kaprielian Z. Identification and characterization of a cell surface marker for embryonic rat spinal accessory motor neurons. J Comp Neurol. 2001;439(3):368–383. doi: 10.1002/cne.1356. [DOI] [PubMed] [Google Scholar]
- Sensenig EC (1957) The development of the occipital and cervical segments and their associated structures in human embryos, Washington.
- Shaw JP. A history of the enumeration of the cranial nerves by European and British anatomists from the time of Galen to 1895, with comments on nomenclature. Clin Anat. 1992;5(6):466–484. doi: 10.1002/ca.980050607. [DOI] [Google Scholar]
- Sheen TS, Chung TT, Snyderman CH. Transverse process of the atlas(C1)–an important surgical landmark of the upper neck. Head Neck. 1997;19(1):37–40. doi: 10.1002/(SICI)1097-0347(199701)19:1<37::AID-HED7>3.0.CO;2-W. [DOI] [PubMed] [Google Scholar]
- Simon F, Mareckova-Stolcova E, Pac L. On the terminology of cranial nerves. Ann Anat. 2011;193(5):447–452. doi: 10.1016/j.aanat.2011.04.012. [DOI] [PubMed] [Google Scholar]
- Skinner H. The Origin of Medical Terms. 2. USA: The Williams & Wilkins Co.; 1961. [Google Scholar]
- Soemmerring S (1778) De basi encephali et originibus nervorum cranio egredientium libri quinque. Prostant apud Abr, Vandenhoeck viduam
- Soo KC, Hamlyn PJ, Pegington J, Westbury G. Anatomy of the accessory nerve and its cervical contributions in the neck. Head Neck Surg. 1986;9(2):111–115. doi: 10.1002/hed.2890090207. [DOI] [PubMed] [Google Scholar]
- Soo KC, Guiloff RJ, Oh A, Della Rovere GQ, Westbury G. Innervation of the trapezius muscle: a study in patients undergoing neck dissections. Head Neck. 1990;12(6):488–495. doi: 10.1002/hed.2880120607. [DOI] [PubMed] [Google Scholar]
- Standring SEA. Gray's Anatomy. 39. London: Churchill Livingstone; 2005. [Google Scholar]
- Standring S. Gray’s anatomy: The anatomical basis of clinical practice. Netherlands: Elsevier; 2008. [Google Scholar]
- Streeter GL. The development of the cranial and spinal nerves in the occipital region of the human embryo. Am J Anat. 1905;4(1):83–116. doi: 10.1002/aja.1000040106. [DOI] [Google Scholar]
- Symes A, Ellis H. Variations in the surface anatomy of the spinal accessory nerve in the posterior triangle. Surg Radiol Anat. 2005;27(5):404–408. doi: 10.1007/s00276-005-0004-9. [DOI] [PubMed] [Google Scholar]
- Taylor CB, Boone JL, Schmalbach CE, Miller FR. Intraoperative relationship of the spinal accessory nerve to the internal jugular vein: variation from cadaver studies. Am J Otolaryng. 2013;34(5):527–529. doi: 10.1016/j.amjoto.2013.05.008. [DOI] [PubMed] [Google Scholar]
- Tubbs RS, Pearson B, Loukas M, Shokouhi G, Shoja MM, Oakes WJ. Phrenic nerve neurotization utilizing the spinal accessory nerve: technical note with potential application in patients with high cervical quadriplegia. Childs Nerv Syst. 2008;24(11):1341–1344. doi: 10.1007/s00381-008-0650-4. [DOI] [PubMed] [Google Scholar]
- Tubbs RS, Shoja MM, Loukas M, Lancaster J, Mortazavi MM, Hattab EM, Cohen-Gadol AA. Study of the cervical plexus innervation of the trapezius muscle. J Neurosurg Spine. 2011;14(5):626–629. doi: 10.3171/2011.1.SPINE10717. [DOI] [PubMed] [Google Scholar]
- Tubbs RS, Benninger B, Loukas M, Cohen-Gadol AA. Cranial roots of the accessory nerve exist in the majority of adult humans. Clin Anat. 2014;27(1):102–107. doi: 10.1002/ca.22125. [DOI] [PubMed] [Google Scholar]
- Tubbs RS, Benninger B, Loukas M, Cohen-Gadol AA. Cranial roots of the accessory nerve exist in the majority of adult humans. Clin Anatomy. 2014;27(1):102–107. doi: 10.1002/ca.22125. [DOI] [PubMed] [Google Scholar]
- Tubbs RS, Ajayi OO, Fries FN, Spinner RJ, Oskouian RJ. Variations of the accessory nerve: anatomical study including previously undocumented findings-expanding our misunderstanding of this nerve. Brit J Neurosurg. 2017;31(1):113–115. doi: 10.1080/02688697.2016.1187253. [DOI] [PubMed] [Google Scholar]
- Wang C, Zhang Y, Nicholas T, Wu G, Shi S, Bo Y, Yuan W. Neurotization of the phrenic nerve with accessory nerve for high cervical spinal cord injury with respiratory distress: an anatomic study. Turk Neurosurg. 2014;24(4):478–483. doi: 10.5137/1019-5149.JTN.8335-13.1. [DOI] [PubMed] [Google Scholar]
- Wetmore C, Elde R. Detection and characterization of a sensory microganglion associated with the spinal accessory nerve: a scanning laser confocal microscopic study of the neurons and their processes. J COmp Neurol. 1991;305:148–163. doi: 10.1002/cne.903050114. [DOI] [PubMed] [Google Scholar]
- Wiles CC, Wrigley B, Greene JR. Re-examination of the medullary rootlets of the accessory and vagus nerves. Clin Anat. 2007;20(1):19–22. doi: 10.1002/ca.20260. [DOI] [PubMed] [Google Scholar]
- Williams P, Warwick R. Gray's Anatomy. 36. London: Churchill Livingstone; 1990. [Google Scholar]
- Williams WW, Twyman RS, Donell ST, Birch R. The posterior triangle and the painful shoulder: spinal accessory nerve injury. Ann R Coll Surg Engl. 1996;78(6):521–525. [PMC free article] [PubMed] [Google Scholar]
- Yigit E, Dursun E, Omeroglu E, Sunter AV, Edizer DT, Terzi S, Demirci M. The course of lower cranial nerves within the neck: a cadaveric dissection study. Eur Arch Otolaryngol. 2018;275(10):2541–2548. doi: 10.1007/s00405-018-5091-4. [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Data Availability Statement
Not applicable.