

Abstract
Introduction:
Women show a gender-specific risk for co-occurring opioid use disorder (OUD) and posttraumatic stress disorder (PTSD). Expert groups have called for the development of integrated treatments for women with OUD/PTSD, but there remains limited information on such interventions.
Methods:
This mixed-methods study interviewed and surveyed 10 women with current or past OUD and co-occurring posttraumatic stress symptoms (PTSS) and 16 providers who work with these women. Interviews and surveys queried patient participants’ and providers’ experiences of OUD/PTSS and how to best design an integrated, trauma-focused treatment for OUD/PTSD.
Results:
Patient participants (90 % white, 90 % mothers, Mage = 45.70) met criteria for severe, lifetime OUD and 40 % met a provisional diagnosis for PTSD. Four themes emerged for participants’ experiences of OUD/PTSS: 1) numerous stressors; 2) shame; 3) multiple motivations to use opioids; and 4) a cycle of trauma and opioid use. Four themes emerged regarding patient participants’ perceptions on the development of an OUD/PTSD treatment: 1) mixed attitudes towards medications for OUD; 2) barriers to treatment (e.g., insufficient treatments and contextual factors); 3) treatment facilitators (e.g., social support); and 4) preferences in treatment (e.g., trauma-focused, gender-focused, family content, ambivalence around group therapy). Providers (Mage = 38.94) were primarily white women (76.5 %). Two themes emerged from their experiences working with women with OUD/PTSS: 1) perceiving women to use opioids to regulate emotions and 2) gender differences in trauma types. Three themes emerged for providers’ perceptions on the development of an OUD/PTSD treatment: 1) barriers to treatment (e.g., chaotic lives, contextual factors, family); 2) treatment facilitators (e.g., trust and external motivations); and 3) desired treatment modifications (e.g., stabilization, early skills in therapy, flexibility in therapy, social supports, safety guidelines, and assistance in identifying an index trauma). Most participants (90.0 %) and providers (93.5 %) preferred working on OUD/PTSD symptoms simultaneously rather than separately.
Conclusions:
Findings demonstrate the need to modify integrated treatments to meet the preferences of providers and women with OUD/PTSS and OUD/PTSD. Treatments should consider therapeutic content, structure, contextual factors, social support, and PTSD severity to enhance uptake and reach.
Keywords: Opioid use disorder, Women, Posttraumatic stress disorder, Qualitative, Integrated treatment
1. Introduction
1.1. Gender differences in opioid use disorder
There is an urgent need to develop gender-focused interventions for women with opioid use disorder (OUD) and co-occurring mental health conditions (Barbosa-Leiker, Campbell, McHugh, Guille, & Greenfield, 2021; Humphreys et al., 2022). Epidemiological data show that from 2013 to 2020, deaths from synthetic opioids increased 2209 % for males and 991 % for females (D’Orsogna, Bottcher, & Chou, 2023). Although males had more fatal overdoses from opioids than females (Butelman et al., 2023), females showed higher rates of intentional opioid-related overdose deaths (Han et al., 2022)— purposeful attempts to engage in more substance use for self-injury (National Institute on Drug Abuse, 2017). Sex differences in opioid overdoses underscore some of the underlying gendered disparities in OUD (Huhn & Dunn, 2020). Relative to men with OUD, women with OUD have more psychiatric comorbidities, including posttraumatic stress symptoms (PTSS), posttraumatic stress disorder (PTSD), depression, and anxiety, and experience more violence and childhood trauma (Braciszewski et al., 2022; Huhn, Berry, & Dunn, 2019; Huhn & Dunn, 2020; Santo et al., 2021). Women are also more likely than men to be prescribed opioids at a stronger dosage and for a longer period of time (Office on Women’s Health, 2017), show a faster progression from using opioids to meeting diagnostic criteria for a disorder (i.e., telescoping) (Barbosa-Leiker et al., 2021; Campbell et al., 2018; Mazure & Fiellin, 2018), have more severe withdrawal symptoms, have lower odds of receiving medications for OUD (MOUD), and have more negative side effects from MOUD (Dunn et al., 2020; Giacomuzzi et al., 2005; Huhn et al., 2019; Jones, Han, Baldwin, Einstein, & Compton, 2023). Further, women with OUD experience greater difficulty entering mental health treatment due to gendered structural barriers (e.g., childcare) and greater stigma. Even when women with OUD do gain access to treatment, they unfortunately show poorer treatment outcomes (Barbosa-Leiker et al., 2021; Huhn & Dunn, 2020; Mazure & Fiellin, 2018; Terplan, 2017). Taken together, these studies show that women with OUD experience more barriers to OUD treatment (Chatterjee, Yu, & Tishberg, 2018; Huhn & Dunn, 2020; Springer, Biondi, Frank, & El-Bassel, 2020) and are more likely to experience the negative medical and psychosocial costs of OUD at a quicker rate than their male counterparts.
1.2. Women with opioid use disorder and posttraumatic stress symptoms
Trauma exposure and the subsequent development of PTSS or PTSD frequently co-occurs with OUD where both conditions independently, and conjointly, disproportionately impact women. Longstanding research shows that women experience more severe lifetime traumatic events, such as sexual abuse, relative to men (Evans, Grella, Washington, & Upchurch, 2017; López-Castro, Saraiya, & Hien, 2017; Overstreet, Berenz, Kendler, Dick, & Amstadter, 2017; Tolin & Foa, 2006), and that women have a two-fold increased risk for lifetime PTSD and thus, double the lifetime prevalence rate (10.4 % vs 5 % for men) (Kessler, Sonnega, Bromet, Hughes, & Nelson, 1995; McLean, Asnaani, Litz, & Hofmann, 2011; Olff, 2017; Tolin & Foa, 2006). Growing evidence indicates that women’s independent risk for OUD and PTSS/PTSD compounds to increase their joint risk for co-occurring OUD/PTSS or OUD/PTSD. In a chart review of primary care patients (N = 100; 46 % women), 81 % of women with OUD reported a traumatic event and 52 % met criteria for PTSD (Hooker et al., 2020). Additionally, among a sample using opioids, women showed an increased likelihood of PTSD diagnosis, sexual abuse, and exposure to three or more adverse childhood experiences (e.g., parent in jail, neglect), events which do not always rise to the definition of a criterion A trauma for a PTSD diagnosis (Evans, Goff, Upchurch, & Grella, 2020). Together, this work has shown that women with OUD often experience traumatic and distressing events which yield PTSS and PTSD.
Women with PTSS/PTSD also show a gender-specific risk for opioid use. A secondary analysis of data (N = 34,566) from wave two of the National Epidemiological Survey on Alcohol and Related Conditions (NESARC) showed that women with past year PTSD had a two-fold increased risk for non-medical prescription opioid use and an OUD diagnosis relative to men (Smith, Smith, Cercone, McKee, & Homish, 2016). In comparison, there was no significant association between past year PTSD and subsequent OUD among men (Smith et al., 2016). Another study showed that among a predominantly female sample, every 10 % increase in PTSD symptoms was associated with a 36 % increased risk of missing a week of methadone maintenance treatment (Peirce, Brooner, King, & Kidorf, 2016). This finding demonstrates how PTSD symptoms among individuals with OUD directly influence treatment attendance. Neurobiological evidence has also shown shared underpinnings of OUD/PTSD (Danovitch, 2016; Elman & Borsook, 2019) that are complicated by the fact that women demonstrate biological differences in stress reactivity which predispose them to develop PTSS (Bale & Epperson, 2015; Heck & Handa, 2019). Such theories have noted the need to develop gender-specific theories that capture gender-specific pathways in trauma, subsequent chronic stress (e.g., PTSS or PTSD), and OUD.
1.3. Current Treatments for OUD/PTSD
Emerging research shows promise for the use of trauma-focused treatments among individuals with co-occurring OUD/PTSD, but none of these treatments have been designed to the needs of women, for dimensional levels of PTSS, nor focused on integrating trauma therapies with substance use disorder therapies. Exposure-based treatments, where patients are asked to systematically and repeatedly revisit the trauma memory during therapy (i.e., imaginal exposures) and approach trauma-related stimuli in the environment in-between sessions (i.e., in vivo exposures), efficaciously reduce PTSD symptoms among individuals with OUD/PTSD (Meshberg-Cohen, Ross MacLean, Schnakenberg Martin, Sofuoglu, & Petrakis, 2021). Among small samples of participants with OUD/PTSD, the provision of evidence-based exposure-based therapies is acceptable and efficacious with significant reductions in opioid use, PTSD symptoms, and enhanced retention on MOUD (Peck et al., 2023; Peck, Schumacher, Stasiewicz, & Coffey, 2018; Schacht et al., 2023; Schacht, Brooner, King, Kidorf, & Peirce, 2017; Schiff, Nacasch, Levit, Katz, & Foa, 2015). In addition, one mindfulness-based intervention showed cognitive reappraisal mediated reductions in PTSD symptoms in individuals with OUD/PTSD (Parisi, Hudak, Froeliger, & Garland, 2023). Despite the efficacy of these interventions, less is known about how such interventions could be gender focused.
There are several reasons a gender-focused intervention may be clinically useful. First, as stated above, women show a gender-specific risk for OUD/PTSS and OUD/PTSD. Second, although there is scant work on gender-differences in psychosocial treatment outcomes for co-occurring OUD/PTSD, women show poorer treatment outcomes to pharmacological treatments for OUD, including more adverse side effects, a higher risk to opioid relapse, poorer treatment retention, and have more psychiatric comorbidities requiring adjunctive treatment than men (Huhn et al., 2019). In addition, there are gender differences in psychosocial treatment outcomes. Among women with co-occurring alcohol use disorder and PTSD, women show poorer reductions in substance use relative to men (Livingston et al., 2021). This finding adds to growing literature on gender differences in treatment interventions for co-occurring substance use disorders and PTSD (Saraiya et al., 2023). For these reasons, it is useful to examine if integrated interventions, which combine trauma-focused treatment with substance use treatment, could be adapted and efficacious among women with OUD/PTSS and OUD/PTSD.
Concurrent Treatment of PTSD and Substance Use Disorders Using Prolonged Exposure (COPE; Back et al., 2014) is an evidence-based integrated treatment that combines Relapse Prevention for substance use disorders (Kadden et al., 1992) and Prolonged Exposure therapy for PTSD (Foa, Hembree, Rothbaum, & Rauch, 2019). In several trials, COPE has reduced PTSS/PTSD symptoms and demonstrated equivalent or greater reductions in substance use (Back et al., 2019; Mills et al., 2012; Norman et al., 2019; Ruglass et al., 2017). However, COPE has not been modified for individuals with OUD/PTSS or OUD/PTSD, and stakeholder feedback has not been gathered on how to best modify COPE for those with OUD/PTSS or OUD/PTSD in opioid treatment programs. Prior work has established that women with histories of trauma exposure, PTSS/PTSD, and OUD, have an interest in gender-specific, trauma-focused treatment, but community health care providers felt burdened to deliver such treatments and lacked the necessary resources (Saraiya et al., 2020). This prior work was limited in its lack of assessment of patients’ and providers’ experiences with OUD/PTSS and how an existing intervention, such as COPE, could be modified to increase uptake and receipt. Accordingly, this mixed methods study interviewed women with OUD/PTSS symptoms and providers who work with women with OUD/PTSS. Research questions asked about patients’ and providers’ (1) experiences of having, or working with, co-occurring OUD/PTSS, and (2) perceptions and desired changes for a modified version of COPE for individuals with OUD/PTSS and OUD/PTSD.
2. Method
2.1. Participants
Patient participants (N = 10) and provider participants (N = 16) were interviewed in person or virtually. Participant eligibility criteria included self-report of being 1) 18–65 years old; 2) self-identifying as a woman; 3) current or past opioid misuse; 4) current or past difficulty reducing opioid use as measured by questions on the Mini International Neuropsychiatric Interview (MINI; Sheehan et al., 1998); 5) history of criterion A trauma exposure as measured by the Life Events Checklist-5 (LEC-5; Weathers et al., 2013); and 6) at least one posttraumatic stress symptom (PTSS) on the PTSD-Checklist for DSM-5 (PCL-5; Weathers et al., 2013). Provider eligibility criteria included self-reported experience working with patients with OUD, PTSD, or both conditions. Eligibility criteria was intentionally broad to capture diverse experiences and dimensional levels of posttraumatic stress symptoms (PTSS).
Sampling was completed in two phases. In phase one, we interviewed 10 patient participants and 11 provider participants to assess gender-specific needs in OUD/PTSS and how to modify an integrated treatment for women with OUD/PTSD. In phase two, we sought a second sample of five clinical researchers with expertise in integrated treatment and OUD/PTSD to assess their perception of the needs of individuals with OUD/PTSS and provide input on modifications for integrated treatment for OUD/PTSD. Recruitment of the second sample was validated emerging themes from the first sample in accordance with theoretical sampling principles of Grounded Theory (Chun Tie, Birks, & Francis, 2019). The definition of saturation was the emergence of no new themes (Saunders et al., 2018). Research procedures were identical across both sets of providers, except that questions were not gender-specific for the second sample of providers to assess if gender-specific needs emerged naturally. Extracted themes are presented across both samples. The Standards for Reporting Qualitative Research (O’Brien, Harris, Beckman, Reed, & Cook, 2014) are reported in Supplementary Table 1.
2.2. Procedure
2.2.1. Patient participants
Social media advertisements, clinician referrals, and flyers recruited patient participants. Flyers stated the study was seeking women with trauma exposure and using opioids. The flyer included a survey link to complete a RedCap screening questionnaire and the research team’s contact information. The screening questionnaire included a statement of consent followed by questions assessing contact information, eligibility, and ending with local and national referrals. Individual interviews were scheduled with eligible participants. At the study appointment, participants provided informed consent followed by an interview and a brief online survey. The first author completed all interviews with an interview guide. Interviews were audio recorded. Interviews lasted on average M = 69:74 (SD = 11:71) minutes. Compensation was $25.
2.2.2. Provider participants
Emails and flyers were sent to several clinics (e.g., outpatient PTSD clinic, outpatient substance use clinic) and clinicians. Emails and flyers stated the study was for providers who work with women with opioid use/OUD and co-occurring trauma exposure/PTSD. Eligibility screening for interested providers was over the phone; all interested providers were eligible. Most providers (11/16) completed an individual interview, and two groups of providers (2–3 participants in each) completed a focus group. At the study appointment, providers completed informed consent, an audio-recorded interview, and a brief online survey. The first author completed all interviews with an interview guide. Interviews were audio recorded. Interviews were an average of M = 56:29 (SD = 16:41) minutes. Compensation was $50. The Institutional Review Board approved all study procedures.
2.2.3. Researcher description
One licensed, doctoral clinical psychologist and two bachelor’s level research assistants composed the research team. The clinical psychologist oversaw the study and completed interviews with participants. The clinical psychologist had significant research experience in OUD/PTSD and women’s health. Two research assistants had no prior professional experience with women with OUD/PTSS. Coding consisted of the clinical psychologist and two trained research assistants to mitigate potential bias from each team member’s background or experience level in the topic area (see below).
2.3. Measures
2.3.1. Interviews
The interview guide for Back et al. (2014) and Saraiya et al. (2020) was adapted for this study’s interview guide. An expert in co-occurring substance use disorder and PTSD research provided feedback on the initial interview guide followed by final use. Interview guides asked about each patient participant’s history of OUD, trauma and PTSS, gender differences in OUD/PTSS or OUD/PTSD, treatment experiences, and what they would like to see in treatments, including a modification of COPE. Providers were asked about gender differences in OUD/PTSD, their experiences providing treatment to women with OUD/PTSS, and what they would like to see in treatment, including modifications to COPE (Back, Killeen, et al., 2014). The interviewer described COPE to all patients and providers.
2.3.2. Surveys
Patient participant surveys assessed demographics, trauma exposure, PTSS, diagnostic criteria for OUD, and desired treatment modifications in an integrated treatment. A demographic form assessed age, race, ethnicity, preferred pronouns, education, gender, sexual orientation, employment, current/past substance use, and treatment history. The LEC-5 assessed trauma exposure (Weathers, Litz, et al., 2013). At the end of the LEC-5, patient participants identified which traumatic event was the most distressing to ascertain the index traumatic event. The event chosen by the patient participant was the anchor for the assessment of PTSS on the PCL-5 (Weathers, Litz, et al., 2013). The PCL-5 provides a provisional diagnosis of PTSD based on cutoff scores of 33 or above (Weathers, Litz, et al., 2013). Patient participants also completed the MINI (Sheehan et al., 1998) to assess current and lifetime OUD.
Provider participant surveys assessed demographics and desired treatment modifications in an integrated treatment. A demographic measure assessed age, race, ethnicity, preferred pronouns, education, gender identity, sexual orientation, employment, work setting, years of experience, and number of patients each provider has seen with OUD, PTSD, or both conditions.
Both patient and provider participants completed a study-developed measure based on Back, Killeen, et al. (2014) to assess patient and provider preferences in designing an integrated treatment for women with co-occurring OUD/PTSD. This measure included 25 items of major content areas of COPE (Back, Killeen, et al., 2014) and open-ended questions (see Table 3). Participants and providers were asked to rate: “How important do you feel it would be to include each of the following topics?” on a scale of 0 = Not at all to 4 = Extremely. The internal consistency of this measure was high for patient participants (Cronbach’s α=0.95) and providers (Cronbach’s α=0.90).
Table 3.
Desired treatment changes (N = 26).
| Item | Patients (n = 10) | Providers (n = 16) | ||
|---|---|---|---|---|
|
|
|
|
||
| M (SD) | Fa | p | ||
|
| ||||
| Ways to manage feelings of guilt or shame | 3.90 (0.32) | 3.19 (0.75) | 8.03 | 0.009 |
| Strategies to identify and effectively manage negative thoughts (e.g., depressive, doubtful, or pessimistic thoughts) | 3.80 (0.63) | 3.38 (0.96) | 1.54 | 0.227 |
| What to do in case of a “slip” or relapse during treatment | 3.70 (0.68) | 3.63 (0.72) | 0.07 | 0.793 |
| Strategies to help manage physical pain | 3.60 (0.70) | 2.75 (1.00) | 5.50 | 0.028 |
| Gradually learning to confront things you fear that contribute to your PTSD symptoms (i.e., in vivo exposures) | 3.60 (0.52) | 2.75 (1.13) | 4.99 | 0.035 |
| How to anticipate and handle situations where you might be tempted to use drugs (i.e., high risk situations) | 3.60 (0.70) | 3.44 (0.81) | 0.27 | 0.607 |
| Education about what PTSD is | 3.60 (0.52) | 3.38 (0.72) | 0.74 | 0.399 |
| Education about what addiction is | 3.50 (0.71) | 3.19 (0.91) | 0.85 | 0.365 |
| Ways to manage cravings and urges to use opioids | 3.50 (0.71) | 3.44 (0.81) | 0.04 | 0.843 |
| Ways to manage thoughts about wanting to use opioids | 3.50 (0.97) | 3.31 (0.79) | 0.29 | 0.596 |
| Strategies to identify and effectively manage anger | 3.50 (1.08) | 2.56 (1.03) | 4.91 | 0.036 |
| Ways to improve communication with loved ones or family members | 3.50 (0.71) | 2.88 (1.03) | 2.85 | 0.104 |
| Problem solving skills | 3.40 (0.97) | 2.94 (1.06) | 1.25 | 0.275 |
| Ways to become more assertive | 3.20 (0.79) | 2.75 (1.18) | 1.12 | 0.300 |
| Ways to have healthy romantic relationships | 3.20 (0.63) | 2.75 (0.93) | 1.80 | 0.192 |
| Repeatedly revisiting the memory of the trauma during sessions in a therapeutic way so that the memory no longer overwhelms you (i.e., imaginal exposures) | 3.10 (1.10) | 3.00 (1.03) | 0.06 | 0.817 |
| Ways to manage childcare | 3.00 (1.25) | 2.94 (0.93) | 0.02 | 0.885 |
| Effective ways to turn down offers to use drugs (i.e., drug refusal skills) | 3.00 (1.16) | 2.75 (1.07) | 0.32 | 0.578 |
| Strategies to help improve sleep | 3.00 (0.94) | 2.88 (1.03) | 0.10 | 0.758 |
| Strategies to remember taking opioid use medications | 2.90 (1.29) | 2.44 (0.89) | 1.18 | 0.289 |
| Relaxation techniques, such as breathing exercises | 2.80 (1.48) | 2.63 (1.41) | 0.09 | 0.765 |
| Have “homework” to do in between sessions to practice new skills | 2.80 (1.48) | 2.50 (1.10) | 0.35 | 0.558 |
| Be stabilized on MOUD (e.g., buprenorphine/suboxone, methadone, etc.) prior to starting therapy | 2.70 (1.16) | 2.75 (1.48) | 0.01 | 0.929 |
| Invite loved ones and/or family members to join a few sessions | 2.70 (1.57) | 1.94 (1.06) | 2.20 | 0.151 |
| Engage in role plays and practice new skills during the sessions | 2.40 (1.43) | 2.75 (0.86) | 0.62 | 0.440 |
Note: MOUD = medications for opioid use disorder. Participants were asked, “How important do you feel it would be to include each of the following topics?” on a scale of 0 = Not at all important, 1 = a little important, 2 = moderately important, 3 = Important, 4 = Very Important. Questions were similar across participants and providers, except providers’ questions were shortened as shown in parentheses. Mean responses in table are organized from most to least important based on patients’ ratings. Bolded responses are significant at p < .05.
Degrees of freedom = 1, 25.
2.4. Data analysis
Nvivo’s Transcription Services transcribed audio files. Research assistants de-identified and double-checked transcripts for accuracy and to remove any identifying information. Qualitative analyses used Grounded theory and the Framework Method (Chun Tie et al., 2019; Gale, Heath, Cameron, Rashid, & Redwood, 2013). Grounded theory uses qualitative data to generate a theory and theoretical sampling to gather appropriate data to answer the research question. The Framework Method uses a combination of deductive and inductive coding to extract themes.
The study open coded qualitative data based on an initial codebook developed from the semi-structured interviews (i.e., deductive coding) followed by focused coding that abstracted overlapping codes into major categories defined by the research questions. Specifically, during the first step of initial coding, the study developed two separate codebooks for patient participant and provider interviews. The coding team added inductive codes to codebooks as needed. The clinical psychologist team member trained both research assistants followed by each team member coding one patient participant interview and one provider interview independently to achieve pilot coding. After independent coding, members discussed discrepancies for each code until each code showed a kappa value of 0.80. After reaching the kappa threshold for pilot coding, the two research assistant coders coded the remaining transcripts with the clinical psychologist overseeing coding. All three team members discussed discrepancies in all remaining codes. The study calculated kappa for all remaining transcripts. For participants transcripts, kappa was 0.94. For provider transcripts, kappa was 0.93.
Following initial coding, the coding team charted codes into a matrix. Codes were then abstracted into categories to answer the two research questions. Categories to inform coding matrices were (a) experiences in treatment, (b) barriers in treatment, (c) facilitators of treatment, and (d) desired treatment modifications. Codes within each category were collapsed and charted into a new matrix sheet for participants and providers, respectively. All three team members analyzed categories for themes. Comparative analysis and team discussion polished themes until they reached consensus. There were several major themes and sub-themes (Fig. 1). No major theme or sub-theme was considered until over 50 % of the sample reported the theme. Coding of the second theoretical sample of clinical researchers mirrored coding of the first sample except that the coding team coded transcripts based on the major themes and sub-themes extracted from the first sample of data. Due to the significant overlap in qualitative themes by providers in the second subset of five providers, the study combined data into one sample in one matrix table. The research team selected exemplary quotes which they lightly edited for readability and confidentiality (Lingard, 2019).
Fig. 1.
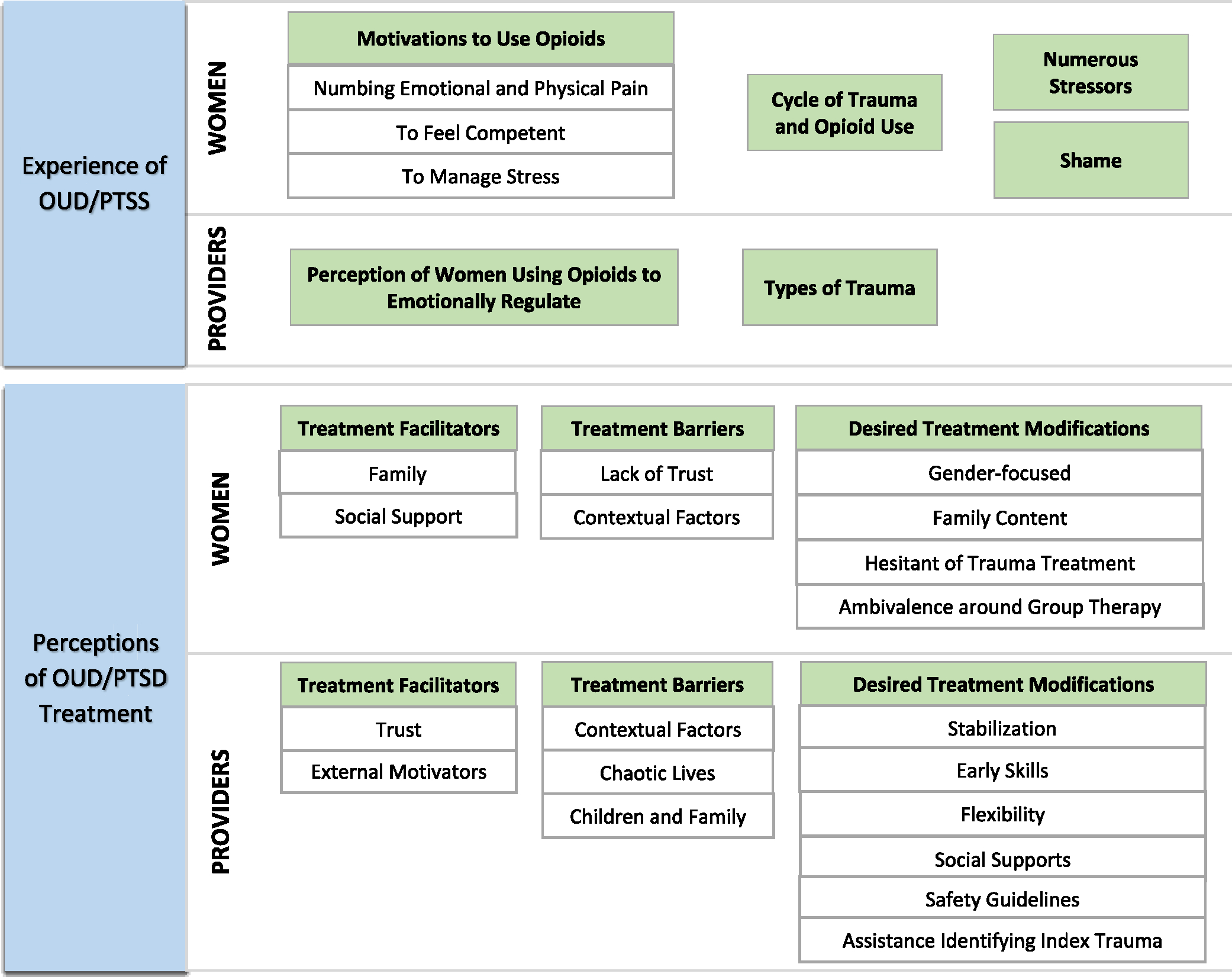
Summary of patient and provider participants themes and sub-themes. Blue boxes indicate research questions. Green boxes indicate major themes. White boxes indicate sub-themes.
Descriptive statistics present patient participant and provider characteristics. One-way ANOVA compared patient participant and provider responses on modifications to an integrated treatment. Alpha was 0.05. SPSS v26 completed analyses.
3. Results
3.1. Demographics
Patient participants (N = 10) were M = 45.70 (SD = 9.32) years old; 90 % identified as white and 10 % as Black/African American (Table 1). Ninety percent were mothers with an average of 2.80 (SD = 2.70) children. Half of the sample met DSM-5 criteria for severe, lifetime OUD and 50 % met criteria for severe, current OUD. Ninety percent reported past-year opioid use. The most used opioids were: Oxycontin (50 %), heroin (40 %), Vicodin (40 %), Dilaudid (30 %), Percodan (20 %), and methadone (20 %). In addition, 70 % of the women reported an opioid-related overdose with an average of 2.30 (SD = 2.63) lifetime overdoses. Seventy percent reported past OUD treatment with 50 % reporting current or past MOUD. Seventy percent endorsed chronic pain. Regarding trauma exposure, participants reported M = 10.60 (SD = 4.12) lifetime traumatic events. All women endorsed sexual assault and ‘another uncomfortable sexual experience.’ The most reported index trauma was physical assault (40 %) followed by sexual assault (20 %) and a life-threatening illness or injury (20 %). Forty percent met a provisional diagnosis of PTSD and 40 % reported past trauma/PTSD treatment. Patient participants with a provisional PTSD diagnosis endorsed a significantly higher number of “happened to me” events on the LEC-5 (M = 8.75, SD = 2.06) than those without the provisional diagnosis (M = 5.00, SD = 1.10), F(1,8) = 14.40, p = .005.
Table 1.
Patient descriptives (N = 10).
| Variables | N (%) / M (SD; Range) |
|---|---|
|
| |
| Demographic characteristics | |
| Age | 45.70 (9.32, 30–57) |
| Women | 10 (100 %) |
| Race | |
| Black/African American | 1 (10 %) |
| White | 9 (90 %) |
| Ethnicity (% non-Hispanic) | 10 (100 %) |
| Sexual orientation | |
| “Straight” (heterosexual) | 10 (100 %) |
| Education | |
| Completed high school/GED | 1 (10 %) |
| Some college/associate degree | 5 (50 %) |
| Bachelor’s degree | 2 (20 %) |
| Doctoral degree | 2 (20 %) |
| Marital status | |
| Dating | 2 (20 %) |
| Living with partner | 2 (20 %) |
| Married | 1 (10 %) |
| Widowed | 1 (10 %) |
| Separated | 1 (10 %) |
| Divorced | 5 (50 %) |
| Children (% yes) | 9 (90 %) |
| Number of children | 2.80 (2.70; 1–10) |
| Primary caregiver of children (% yes) | 4 (40 %) |
| Employment status | |
| Full-time | 5 (50 %) |
| Unemployed | 4 (40 %) |
| On disability/military veteran | 1 (10 %) |
| Annual personal income (US Dollars) | $53,714.29 ($55,526.91; $0–$145,000) |
| Clinical characteristics | |
| Past year substance use (yes/no) | |
| Opioids | 9 (90 %) |
| Cocaine/Crack | 5 (50 %) |
| Tobacco | 4 (40 %) |
| Alcohol | 4 (40 %) |
| Cannabis | 4 (40 %) |
| Benzodiazepines | 4 (40 %) |
| Ecstasy | 4 (40 %) |
| Methamphetamines | 3 (30 %) |
| Kratom | 2 (20 %) |
| Ketamine | 1 (10 %) |
| Methylenedioxypyrovalerone (MDPV) | 1 (10 %) |
| Commonly used opiates in lifetimea | |
| Oxycontin | 5 (50 %) |
| Heroin | 4 (40 %) |
| Vicodin | 4 (40 %) |
| Dilaudid | 3 (30 %) |
| Methadone | 2 (20 %) |
| Percodan | 2 (20 %) |
| Current Opioid Use Disorder, severe | 5 (50 %) |
| Lifetime Opioid Use Disorder, severe | 5 (50 %) |
| Age of first use of opiates (years) | 30.10 (10.94; 13–45) |
| Age of opioid dependence (years) | 31.30 (11.02; 14–46) |
| Lifetime Overdose (% yes) | 7 (70 %) |
| Number of overdoses | 2.30 (2.63; 0–8) |
| Chronic pain (% yes) | 7 (70 %) |
| Past opioid use treatment (medication or therapy %) | 7 (70 %) |
| Past trauma/PTSD treatment (medication or therapy %) | 4 (40 %) |
| Lifetime Traumatic Events (% yes; LEC-5)b | |
| Natural disaster | 5 (50 %) |
| Fire or explosion | 3 (30 %) |
| Transportation accident | 8 (80 %) |
| Serious accident at work, home, or during recreational activity | 6 (60 %) |
| Exposure to toxic substance | 3 (30 %) |
| Physical assault | 9 (90 %) |
| Assault with a weapon | 6 (60 %) |
| Sexual assault | 9 (90 %) |
| Other unwanted or uncomfortable sexual experience | 9 (90 %) |
| Combat or exposure to a warzone | 3 (30 %) |
| Captivity | 4 (40 %) |
| Life-threatening illness or injury | 7 (70 %) |
| Severe human suffering | 3 (30 %) |
| Sudden violent death | 7 (70 %) |
| Sudden accidental death | 6 (60 %) |
| Serious injury, harm, or death you caused to someone | 1 (10 %) |
| Any other very stressful event/experience | 7 (70 %) |
| Total Lifetime Traumatic Eventsb | 10.60 (4.12; 5–17) |
| Self-reported Index Trauma | |
| Physical assault | 4 (40 %) |
| Sexual assault | 2 (20 %) |
| Combat | 1 (10 %) |
| Life-threatening illness or injury | 2 (20 %) |
| Sudden accidental death (e.g., overdose) | 1 (10 %) |
| Any other very stressful event/experience (e.g., birth trauma) | 1 (10 %) |
| Posttraumatic Stress Disorder Symptoms (PCL-5) | 37.10 (23.14, 9–80) |
Note: LEC-5 = Life Events Checklist for DSM-5; PCL-5 = Posttraumatic Stress Disorder Checklist-5 for DSM-5.
As reported on MINI 7.0.0 (Sheehan et al., 1998). Participants could endorse more than one opioid as the most frequently used.
Frequency or sum of sample that endorsed each respective lifetime traumatic event happened to me, witnessed it, learned about it, or part of my job.
As shown in Table 2, provider participants (N = 16) were an average of 38.94 (SD = 8.71) years old and 76.5 % identified as a woman. Most provider participants were white (76.5 %) followed by Asian/Asian American (11.8 %) and Black/African American (5.9 %). Most provider participants were psychologists with a Ph.D. (56.3 %) followed by physicians with an M.D./D⋅O (25 %). Provider participants had M = 10.63 (SD = 13.04) years of experience working with patients with OUD and 8.63 (SD = 6.63) years working with patients with trauma/PTSD. The most frequently provided OUD treatment was Relapse Prevention therapy (87.5 %), and the most frequently provided PTSD treatment was Prolonged Exposure therapy (43.8 %). Over a third (37.5 %) of the sample had provided COPE. All providers reported experience with co-occurring OUD/PTSD.
Table 2.
Provider descriptives (N = 16).
| Variables | n (%) / M (SD; Range) |
|---|---|
|
| |
| Age | 38.94 (8.71; 28–58) |
| Men | 3 (18.8 %) |
| Women | 13 (81.3 %) |
| Race | |
| Black/African American | 1 (6.3 %) |
| White | 13 (81.3 %) |
| Asian/Asian-American | 2 (12.5 %) |
| Ethnicity (% non-Hispanic) | 0 (100 %) |
| Education | |
| M.D./D.O. | 4 (25 %) |
| Masters | 2 (12.5 %) |
| Ph.D. | 9 (56.3 %) |
| Psy.D | 1 (6.3 %) |
| Employment (% full time) | 13 (81.3 %) |
| Work setting | |
| Academic medical center | 6 (37.5 %) |
| Community clinic | 1 (6.3 %) |
| Graduate program | 1 (6.3 %) |
| Hospital clinic | 2 (12.5 %) |
| Independent private practice | 1 (6.3 %) |
| Veterans administration | 5 (31.3 %) |
| Primary patient population | |
| Veterans | 5 (31.3 %) |
| Women with OUD | 14 (87.5 %) |
| Women with PTSD or trauma | 15 (93.8 %) |
| Women with OUD and PTSD or trauma | 14 (87.5 %) |
| Years of experience | |
| Working with individuals with opioid use/OUD | 10.63 (13.04; 1–55) |
| Working with individuals with trauma/PTSD | 8.63 (6.63; 1–25) |
| Annual case load of patients with OUD/PTSD (number of patients) | 41.94 (55.89; 0–200) |
| Annual case load of women patients with OUD/PTSD (number of patients) | 29.94 (49.19; 0–150) |
| OUD treatments provided | |
| Medications for OUD | 8 (50.0 %) |
| Relapse prevention therapy | 14 (87.5 %) |
| Contingency management | 2 (12.5 %) |
| Motivational interviewing | 13 (81.3 %) |
| Acceptance and commitment therapy | 2 (12.5 %) |
| Dialectical behavior therapy | 6 (37.5 %) |
| Mindfulness-based relapse prevention skills | 5 (31.3 %) |
| PTSD treatments provided | |
| Prolonged exposure therapy | 7 (43.8 %) |
| Cognitive processing therapy | 6 (37.5 %) |
| Trauma-focused cognitive behavioral therapy | 1 (18.8 %) |
| Psychodynamic trauma therapy | 1 (18.8 %) |
| Medications for PTSD | 5 (31.3 %) |
| Other (e.g., written exposure therapy, STAIR, ACT, present centered therapy) | 5 (31.3 %) |
| Integrated trauma and substance use treatments provided | |
| Seeking safety | 5 (31.3 %) |
| COPE | 6 (37.5 %) |
| Integrated PTSD and MET | 1 (6.3 %) |
Note: OUD = Opioid Use Disorder; PTSD = posttraumatic stress disorder; SUD = substance use disorder; COPE = Concurrent Treatment of PTSD and Substance Use Disorders Using Prolonged Exposure; STAIR = Skills Training in Affective and Interpersonal Regulation, ACT = Acceptance and Commitment Therapy, MET = Motivational and Enhancement Therapy.
3.2. Qualitative themes: Experience of OUD/PTSS
3.2.1. Patient participants
Four themes emerged in response to women’s experiences of co-occurring OUD/PTSS (Fig. 1). Patient participants reported experiencing 1) numerous stressors throughout their life; 2) feeling shame, self-blame, and worthlessness; 3) having multiple motivations to use opioids, including to numb emotional and physical pain, to feel competent in day-to-day activities, and to manage distress; and 4) a cycle of trauma and opioid use marked by violence and intergenerational trauma.
Many patient participants reported experiencing multiple traumas and stressors. Importantly, participants often discussed distressing events outside of the definition of Criterion A traumas in the DSM-5 during clinical interviews (American Psychiatric Association, 2022). Criterion A defines what traumatic experiences qualify as a traumatic event to receive a PTSD diagnosis. In interviews, many participants discussed adverse childhood experiences of emotional abuse, abandonment, or verbal abuse and some reported their personal divorce or the divorce of their parents as their most distressing experiences. This was surprising given that all participants were required to endorse a Criterion A event to be eligible for the study, and many self-reported physical or sexual assault as their most traumatic experience. However, during interviews, many women identified experiences that did not fit into the definition of a Criterion A trauma as the most distressing. One patient participant said, “I used to think to myself, ‘Why wouldn’t [my father] just hit me and shut up, you know, but he wasn’t physically abusive. Now his father was, but my dad wasn’t an abuser. He was more mentally, emotionally [abusive]…I used drugs because of my childhood.” Another patient participant expressed her parents’ divorce as the most distressing:
“My dad was very emotionally and verbally abusive and neglectful. You know, my mom wanted kids and that was her opportunity, and they ended up divorcing officially when I was 10. But they lived on separate floors of the house from when I was like six or seven…It wasn’t like super physical trauma, but definitely emotional trauma of not having a second parent. He just didn’t care for us, didn’t talk to us.”
Patient participants also reported shame, self-blame, and worthlessness throughout the interviews for the experiences they had gone through around opioid use and trauma. One patient participant said, “Oh, I’m so ashamed. So ashamed…It took me a long time, even after getting clean, to even get over [my opioid use]. I still felt like I wasn’t worth anything. I had no sense of worth at all.” Another patient participant became tearful during the interview and expressed feeling failure: “Excuse me, I’ll get upset because it was a really hard time in my life because that was not who I was. That was just not the person that I was…I was trying to juggle a full-time job, I was trying to be a good mom. I was trying to do all the things, but I was failing at every role that I played in this life.” Another patient participant differentiated the shame women may feel from men:
“Women experience things in active addiction that men don’t. I think our shame is different. I think we do things for drugs that men don’t do…I don’t think that men feel the way that women feel about themselves when we’re using. I mean…life is a feminine thing. You know because we have the children that we’re responsible for. And women are supposed to be women. We’re supposed to, you know, follow a certain script that men, with standards, that men are not held to.”
Patient participants also conveyed different motivations to engage in opioid use. One of these motivations was using opioids to numb emotional and physical pain. As one patient participant said, “What pain was it pushing it down? Emotional pain. Emotional pain…Like, my childhood or my teen years… it would be so bad that I would just curl up… it numbed that pain. They’re literally painkillers. So, pain is pain whether it’s emotional or physical.” Another said: “I want to not have to, you know, these heavy thoughts and memories […] Having these thoughts and memories physically hurts inside.”
Additionally, patient participants reported using opioids to feel competent in everyday tasks. Two women independently stated using opioids made them feel like “Wonder Woman.” One woman said:
“I think it [opioid use] was to help both the pain in my back and mental[ly] to kind of forget and just be able to move on and do other things. I got to say when I would take them, it was like I was Wonder Woman. At first, I would take it, I had no pain in my back. I could go do anything I wanted. I could forget about what was going on in my household. I think it helped [me] both mentally and physically. And that’s why I was starting to abuse it.”
The other woman said that when she used, she “felt like a cheerleader. I felt like I was on point and everything that I was doing was good and happy and bright. […] I was Wonder Mom and Wonder Woman and all that combined.” Finally, women also reported using opioids to manage stress, worry, and anxiety, often stemming from trauma. One patient participant said:
“I was having problems in my marriage and my stepdaughters and [my ex-husband] trying to get custody of [my stepdaughters] …So, I started using them to escape.” Another participant said, “[Opioid use] is what I’ve been looking for my whole life. […] It felt so good…I wasn’t worried about nothing. [Before that I worried about] everything, anything. ‘What does that person think about me? Oh, are they going to tease me? Is my dad going to scream at me tonight?’”
The final theme among patient participants was a cycle of trauma and opioid use, where experiencing trauma, including violence and intergenerational trauma, led to subsequent use, and often additional trauma exposure. One said: “See, I kind of lost my mind after my mom died. Using so many drugs and using drugs is traumatic, you know. I don’t know if anybody who hasn’t been there understands. Life is trauma. [My relationship with my previous partner] was just the relationship we had. He was abused, and his mother was abused. Oh, it’s a generational thing.” Another said, “When something didn’t work out, my husband was very verbally abusive. So, when he would be yelling at me and in my face, the next thing I knew I was going for my first…It would make me feel like I wasn’t as bad as he said I was.”
3.2.2. Provider participants
Two themes emerged from providers’ experiences working with women with OUD/PTSS: 1) perceiving that women used opioids to regulate their emotions and 2) identifying different types of traumas experienced by cis-gender men and women (Fig. 1). For the first theme, providers expressed that relative to men, women with OUD/PTSD seemed to feel a need to be more functional in their day-to-day lives. Provider participants noted that women needed to feel functional as caregivers, and thus used opioids to regulate their emotions and cope. As one provider said, “I think that a lot of the women that I see…are also very busy and active caregivers. And so, there’s this sense of I can’t be in withdrawal. I need to be functional.” another provider said, “I think it depends on why they’re using opiates, but a lot of ours have been dysregulation regarding emotions or trauma.”
Provider participants also noted that women with OUD/PTSD experienced different trauma types relative to men. Providers noted more interpersonal trauma, intimate partner violence, and other non-traditional traumas, such as adverse childhood experiences and birth-related traumas. One provider said:
“I see a lot of comorbid mood and anxiety disorders… and a lot of trauma in our patients. And that ranges from childhood traumas… and adverse childhood events and adult traumas. We are actually seeing increased rates of delivery-related traumas in the context of COVID. So, the full spectrum in terms of the traumas these women have experienced in their lifetime, often multiple traumas at different stages of life…But the majority is adverse childhood events and sexual traumas in childhood and/or adulthood.”
3.3. Perceptions of treatment
3.3.1. Patient participants
Four themes emerged regarding patient participants’ perceptions of OUD/PTSD treatment: 1) mixed attitudes towards MOUD; 2) treatment barriers, including the sub-themes of insufficient treatments that lead to a lack of trust and contextual factors; 3) treatment facilitators of family and social support; and 4) desired treatment modifications, including the sub-themes of an interest in, but hesitation towards trauma treatment, gender-focused treatments, adding family content, and ambivalence around group therapy (Fig. 1).
When patient participants were prompted about their attitudes towards MOUD, there was variability in responses. Some patient participants reported MOUD was beneficial such as this participant after her first dose of Suboxone:
“[My provider] was like, ‘You need to take this and put it underneath your tongue and… you will know.’ And so, me, I’m like…this man lying to me because I know I take four, five, eight pills a day and you’re trying to tell me this little strip…I had about four or five start dates before I actually believed that it would work. Well, that’s what took me so long to actually get started because the fear of getting sick [i.e., withdrawal symptoms] outweighed trying to get better…And then, I was like, oh my God, this actually works. I mean, I could have been the poster gal for Suboxone.”
Other patient participants expressed skepticism for staying on MOUD long-term and noted it did not reduce other substance use. One said, “I have mixed feelings about Suboxone…I guess if they were successfully using Suboxone and working with a therapist to go along with their Suboxone maintenance…but, just because the Suboxone stops you from using opiates, it doesn’t stop you from using other substances.”
For the theme of treatment barriers, two subthemes emerged: insufficient treatments due to lack of trust and contextual barriers. For the former, most patient participants shared experiences of treatments being too short, lacking compassion, being invalidating, or not being holistic which, at times, seemed to precipitate a lack of trust in healthcare. One said that prior to opioids she used alcohol. Her experience of treatment was:
“Whenever I would be in treatment, they would have an alcohol treatment plan and a mental health treatment plan…You couldn’t include any kind of mental health therapy, classes, or psychiatrist meetings because all they talk about is alcohol. I kept telling them that’s not just my problem. I need the other I think more than I need this. It’s never—it was never my choice. Choice was always made for me.”
In addition to difficulties with treatment plans in clinics, patient participants also reported several contextual factors that subverted access to or engagement in treatment. The most common contextual barriers reported were money and health insurance. As one patient participant said, “Money’s always an issue. I’m on disability, so I don’t make a whole lot of money. I have Medicare and Medicaid. If [therapy isn’t] covered by that, then I don’t foresee myself being able to take part.”
Themes regarding facilitation of treatment included family and social support. For family, participants were often motivated to seek out treatment to be a better family member or because of their family’s concerns. One patient participant said, “I want to be a good mom. I don’t want to be a train wreck. Anything that can empower me to be a decent mom, a better mom, and set a strong example for my girls and teach my son to be a good man…In order to make myself somebody that they would look up to. You know what I mean…I want to do it for my kids.” In addition, patient participants reported social support in the form of programs, sponsors, or peers sustained treatment gains and growth. One patient participant said:
“Right now, I’m in a [online chat] with other people who are in recovery from different substances. What I love about it is, if I’m having that moment, I could pull out my phone and go to [the online chat] and be like, ‘Hey guys I’m having a hard time. This is what’s going on and I need support. This is what that support would look like for me…and we talk about it. I love that. I love how it’s 24/7 and there’s people in different time zones so even in the middle of the night there’s someone there. It doesn’t even have to be someone who has letters behind their name. I just like talking to someone who has the experience that I’ve had. Ears rather than anything else.”
Finally, in response to what treatment modifications they would like to see, patient participants expressed a conflicted simultaneous desire and hesitation for trauma treatment, gender-focused treatment, content on family, and reported ambivalence around group therapy. When probed about their desire for trauma treatment, one patient participant expressed a desire for coping: “Being able to cope with trauma on a day-to-day basis. It’s literally something I deal with every day. There’s not a day that goes by that the thought doesn’t come into my head about anything that’s happened to me.” However, the same participant when asked about COPE stated, “I think it sounds very triggering. I would think that it would take someone with substantial clean time to be able to deal with that [therapy].” Patient participants also expressed wanting gender-focused treatment, where one participant said she wanted to discuss “women specific issues that we can talk about amongst each other, you know that the men probably don’t even want to hear. I think it’s more of a nurturing environment for women to discuss sensitive issues with other women.” Patient participants also reported wanting more family-based therapy sessions or content in treatment. One said: “I’d be completely lying if I said my experiences haven’t affected the people around me…like dealing with one another you would need family type therapy in the best, healthiest way. Especially like for me and [my partner], I think that couples therapy would be super beneficial with just how we speak to one another in front of our kids.”
When asked about group therapy, patient participants expressed ambivalence. One woman said, “I don’t know. I think you can get a lot out of both [individual and group therapy] …I think both would be great, to have an option for both. But if I had to pick one, I’d probably say individual because I think if you get a lot of people with trauma together in a group and then they start sharing their trauma, you’re gonna start triggering people if you don’t have the right safeguards in place.”
3.3.2. Provider participants
A total of three themes emerged for provider participants’ perceptions of OUD/PTSD treatment: 1) treatment barriers, including the sub-themes of the chaotic lives of patients, children and family, and contextual factors; 2) treatment facilitators, including the sub-themes of external motivations and trust; and 3) desired treatment modifications, including the sub-themes of stabilization prior to treatment, early skills in therapy, flexibility in therapy delivery, integration of social supports, safety guidelines, and assistance in identifying an index trauma (Fig. 1).
When discussing challenges working with OUD/PTSD, provider participants expressed the chaos in the everyday lives of patients as a treatment barrier. One provider said, “They’re leading very chaotic lives, and it can often be hard to engage them in treatment as a result of that. So, using a lot of layered and multicomponent treatments are… really necessary to make any significant or long-term changes.” Providers also expressed that children and family could be barriers to entering or staying in treatment. As one provider said, “What we see maybe more often, at least in the beginning, is the finger-wagging family member who wants to tell on the patient and scold the patient.” Other providers agreed that childcare was a barrier to treatment. Providers also noted contextual factors hindered treatment engagement, such as internet access, housing, health insurance, and the constraints of the healthcare system. One provider said, “Looking for a therapist who can offer trauma-informed care might be kind of beyond the coordination capacity of an already understaffed [mental healthcare] system.” Another provider said, “Many of the women—unless they’re fully disabled—do not have the ability to come to the clinic. They can do telehealth, but then the barrier is do they have a phone that functions well enough and access to stable private internet to do this?”
In contrast to barriers, provider participants noted that treatment facilitators included external motivations to engage in care as well as trust patients may feel with providers or healthcare agencies. One provider said, “I find for women, [treatment] tends to be more externally motivated, so whether it’s a spouse saying something or whether it’s Department of Social Services. There’s a lot of other factors, at least in the patients that I have.” Several providers noted that establishing trust was an important facilitator for treatment engagement. One provider said, “This issue of safety and this issue of judgment was huge…This issue of trust, I feel was different [for women with OUD/PTSD]. It’s important with every client, but it was different [with them]. It was like you could feel the difference in the room and it was so much more important and so much more sensitive to many different things that could go wrong.”
Provider participants expressed several desires to modify COPE for patients with OUD/PTSD. This included increasing information on stabilization, early skills for emotion regulation, flexibility in the delivery of treatment, integrating social supports, increasing safety, and assistance with identifying the index trauma. Regarding stabilization, one provider said, “I’m actually more concerned about whether they’re psychosocially stable than I am [concerned about] whether they’re sober…I would want them to have some sort of marker that they actually felt like they can truly engage meaningfully in the therapy because otherwise I would say, let’s wait until you’re more stable.” An additional desired treatment modification was including early skills on emotion regulation and distress tolerance to help with treatment gains. One provider gave specific examples of skills, saying “I think in between sessions two and three just really put in some sort of like distress tolerance, coping, heavy stress management skills before doing the first exposure […] I think some deep breathing, some progressive muscle relaxation, maybe the Improve and Imagine skills from DBT [Dialectical Behavior Therapy].” Providers also expressed desiring flexibility in how the treatment was delivered. One provider said, “It’s a much greater challenge to bring women into a treatment like COPE, where it’s a pretty long protocol and it’s very structured, not super flexible. It might benefit women in particular to have a bit more flexibility or shorter sessions.”
Provider participants also expressed a need to integrate social supports. One provider said group therapy could provide peer support:
“You got a group of people who are going through the same thing as you, can kind of hear the perspectives of other people, you’re all supporting each other, holding each other accountable on getting the outside work done. I think that would be a cool model, ‘cause we’ve gotten feedback that it would be cool to have some interaction with other people who are going through this.”
In addition, provider participants requested having more explicit safety guidelines to assist them in feeling more comfortable providing trauma-focused therapy to women with OUD/PTSD. One provider expressed concern if substance use was increasing during treatment: “Like what to do if the substance use is increasing, and things aren’t going well? I think there has to be a way to either increase the level of substance treatment outside of COPE or have a way to break out, to stabilize it, or switch it around so they can focus more on how do you get from session to session without having increasing substance use?”
Finally, provider participants noted needing assistance in identifying the index trauma for PTSD treatment given the number of repeated traumas patients had experienced and patient difficulties in identifying the worst trauma they experienced. As one provider said, “I haven’t met anybody…who’s like, ‘Oh, I got this one trauma and that’s the one I need to work on.’ It’s like, ‘I got a dozen. Which one? This is the one that’s bothering me this month.’” Another provider said, “The majority of people in our program have had repetitive trauma. I think the repetitive trauma with the overlay of being on pharmacotherapy for a long time, can make it additionally difficult to find what [trauma] is causing most of the day-to-day concern.” Another provider said, “Obviously as part of [Prolonged Exposure therapy] we identify an index trauma. I think it is a challenge, but usually one can be found…I think the bigger challenge is convincing the patient that focusing on one makes sense given the range of their experiences. I think it seems artificial and insufficient…to pick one trauma.” Another provider echoed this difficulty for patients to pick one trauma stating, “I think that…all of our patients have struggled with…the idea of an index trauma and trying to find you know which is the one that’s causing the most distress. It’s often not the one that as a clinician you’re kind of sitting there going, ‘Oh that must be the one we’re going to work on.’ …Sometimes it takes the entirety of the COPE treatment to eventually arrive at, oh actually maybe it was the other [trauma].”
3.4. Survey of desired treatment changes
Table 3 shows patient and provider participant responses to desired changes in the COPE treatment. There were four items where patient participants and provider participants significantly differed from one another (p’s < 0.05): 1) strategies to identify and effectively manage anger; 2) strategies to help manage physical pain; 3) ways to manage feelings of guilt and shame; and 4) gradually learning to confront things you fear that contribute to your PTSD symptoms (i.e., in vivo exposures). Patient participants rated the importance of all items being added to the modified therapy intervention as higher than provider participants. Patient and provider participants were also asked what kind of treatment would work best for them or, for provider participants, patients with OUD/PTSD. For patient participants, 90.0 % reported working on both opioid use and PTSD symptoms together. For provider participants, 93.8 % reported both opioid use and PTSD symptoms together.
As part of this survey, patient participants and provider participants were given the option to suggest additional topics to include in treatment. Two patient participants made suggestions. One patient participant expressed wanting the treatment to address safe sex practices and harm reduction techniques for using and another suggested the treatment address “how to effectively work at a job while going through treatment.” Six provider participants made suggestions, including considering an Acceptance and Commitment Therapy approach, skills on emotion identification and regulation, boundary setting, distress tolerance skills, communication with MOUD prescribers and how to handle MOUD reductions, and treatment engagement.
4. Discussion
This mixed methods study examined a sample of women with current or past OUD/PTSS symptoms and a group of providers who work with them. The first research question assessed patient and provider participants’ lived experiences having, or working, with this comorbidity. A total of four themes emerged for patient participants and a total of two themes emerged for provider participants. Patient participants expressed many motivations to use opioids, numerous stressors throughout their life, a chronic cycle of trauma and opioid use, and feeling ashamed. Provider participants noted gender differences in the types of traumas women with OUD/PTSS experienced and perceived that women used opioids to manage emotions. The second research question assessed patients’ and providers’ perceptions and desired modifications to the integrated treatment, Concurrent Treatment of PTSD and Substance Use Disorders Using Prolonged Exposure (COPE; Back, Killeen, et al., 2014) for women with OUD/PTSD. A total of three themes emerged for patient and provider participants: treatment barriers, treatment facilitators, and desired changes. Within each theme, sub-themes showed that patient and provider participants requested greater flexibility in the treatment, additional distress tolerance and stabilization skills, help with identifying the index trauma, competing responsibilities that impede access to treatment, the need to consider contextual factors, the importance of developing trust with providers, and social support. In addition, patient participants expressed ambivalence around medications for OUD. Overall, both patient and provider participants expressed wanting an integrated treatment for OUD/PTSD with gender-specific components and modifications to the design and content of COPE. Namely, patient participants reported wanting a therapy with ways to manage feelings of guilt and shame, chronic pain, and anger in addition to learning how to approach things they avoid in daily life (i.e., in vivo exposures) significantly more than providers. Our findings align with the findings from prior qualitative studies (Greenfield, Cummings, Kuper, Wigderson, & Koro-Ljungberg, 2013; Morse et al., 2022) thereby supporting the evidence base on how integrated trauma-focused treatments need to be modified for this special population.
4.1. Clinical profiles of trauma and opioid use
The clinical profiles of the women in this study were marked by high trauma and stress exposure, opioid use, a cycle of trauma and opioid use, and high demands as caregivers. On average, women in this study reported over ten lifetime Criterion A traumatic events in addition to several distressing events outside the standard definition of traumatic events in the DSM-5 that influenced their opioid use. For instance, during interviews, many women reported using opioids to cope with rejection and emotional abuse. Women reported emotional trauma and divorce as painful and distressing, often more so than their Criterion A traumas, such as sexual assault. Others have found similar findings showing that adverse childhood experiences, general stress, namely household dysfunction, divorce, and emotional abuse, have felt distressing to women using opioids and triggered future opioid misuse (Chatterjee et al., 2018; Martin et al., 2023; Morse et al., 2022; Saraiya et al., 2021). These findings suggest that treatments for women with OUD/PTSD may need to consider women with other trauma types which would not qualify for the PTSD diagnosis and sub-threshold PTSS which may be left untreated due to lack of formal diagnosis. However, an alternate interpretation for the discrepancy between patient participants interviews and the traumas they endorsed in survey responses may be the interview setting. Patient participants may not have discussed their Criterion A traumatic events with the interviewer due to avoidance or feeling unsafe with the interviewer. The research team is cautious of this interpretation since we observed patient participants often struggling to answer self-report surveys. This may be due to several reasons, such as avoiding thinking about one’s mental health, inaccessible survey language or style, or lack of awareness of mental health symptoms.
In addition, all the women in this study reported feeling immense shame, blame, and worthlessness for the traumas they had experienced, their opioid use, their recovery journeys, and not living up to societal roles. Women in our sample felt strong societal pressure to follow social scripts, and when not meeting these expectations, feeling shame and low self-worth. These findings are supported by our quantitative findings which showed the highest endorsed desire in an integrated treatment for OUD/PTSD was “ways to manage guilt and shame.” These findings also align with prior work (Saraiya et al., 2020; Valeri et al., 2018) and point to the need for more research on shame in women with OUD/PTSS as well as the need to provide compassionate care for such women who feel highly critical of themselves. One study showed that both men and women with substance use disorders endorse shame, but solely women endorse feeling greater stigma and discrimination (Valeri et al., 2018). Thus, it will be imperative for treatments for women with OUD/PTSS to address stigma and shame, especially since shame increases isolation and withdrawal.
An additional finding in this study was that all the patient participants in this study met current or lifetime criteria for a severe OUD even though half of the women had not used opioids in the past year. The field of substance use does not have a clear definition of recovery, and from our findings it seems that cessation of use is not an adequate benchmark given the myriad of remaining issues and symptoms that patients with substance use disorders, including the women in this sample, experience. Our findings suggest that not using opioids is insufficient for meeting long-term recovery thresholds. It may be that not using opioids is solely one part of the recovery process whereas long-term recovery may include not meeting DSM-5 criteria for OUD. This remains an empirical question and will be important to examine as it warrants discussion on what recovery from OUD entails and whether it is an end-state or long-term process.
4.2. Attitudes towards treatment
When it came to treatment for OUD/PTSD, both patient and provider participants were interested in an integrated trauma-focused treatment modified to women with OUD/PTSD. Interestingly, some women expressed hesitation when the exposure-based components of COPE were described during interviews but at the same time expressed an interest in these same components in the surveys. This discrepancy is unsurprising since avoidance is a cardinal symptom of PTSD and engaging in exposure exercises can be difficult for patients. However, given that the avoidance symptom cluster is specifically associated with non-medical prescription opioid use among women (Smith et al., 2016), women with OUD/PTSS or OUD/PTSD may show a uniquely higher level of avoidance or greater barriers to engaging in exposure-based, trauma-focused treatments. One way to increase engagement may be the incorporation of contingency management incentives to increase attendance to exposure-based treatments (e.g., Peck et al., 2023; Schacht et al., 2017). However, since contingency management can be difficult to implement into real-world settings, additional work on how to increase engagement in exposure-based treatments is warranted (Becker, DiClemente-Bosco, Rash, & Garner, 2023).
An additional discrepancy among participants were patient participants attitudes towards MOUD. Although half of the participants reported being on MOUD, patient participants expressed ambivalence about the combination of MOUD with integrated treatment in interviews and rated stabilization on MOUD as of lower importance relative to other content areas in COPE. In addition, some patient participants also reported negative experiences with MOUD which led them to stop using MOUD. In contrast, providers strongly preferred MOUD with integrated treatment for safety and stabilization but did not rate it as the most important content area in a modification of COPE. One reason for this discrepancy may be gendered disparities in MOUD (Huhn et al., 2019). Being female and living in a rural area is associated with a lower odds of receiving MOUD (Jones et al., 2023). Given that the women in this sample lived in primarily rural areas, they may have been disadvantaged in having access to MOUD. Even among the women who had previously, or were currently, using MOUD, there seemed to be general concern of long-term use of MOUD. Providers were cognizant of this concern. Some providers noted that a modified, integrated treatment of COPE for OUD/PTSD may be most beneficial for women with OUD/PTSS when tapering off MOUD because women often experience an increase in PTSS. For this reason, it may be useful for a modified version of COPE for OUD/PTSD to incorporate treatment content on MOUD—ranging from how it may augment recovery to how to safely taper dosage for individuals in sustained recovery from OUD.
4.3. Social networks and connection
Another notable theme across the patient and provider participants was the importance of social networks and connection. Both women and providers noted that family members and children laid on a continuum of either negatively or positively influencing their opioid use and treatment engagement. For instance, many women reported that using opioids was a means to feel capable, like “Wonder Woman” or “Wonder Mom,” while others reported that they struggled to attain treatment due to a lack of structural supports for childcare. Other women expressed that their family encouraged them to seek treatment, demonstrating the myriad of ways in which family could both hinder and facilitate opioid use and opioid use treatment.
One interesting finding we noticed was the tendency for women participant’s mothers to have helped them in recovery. Many women in this study noted that their mothers watched their children and/or urged them to move in with them and find treatment. We observed an intergenerational support network of grandmothers and mothers attending to their adult children in need of OUD/PTSD treatment and their grandchildren. Other studies have shared these findings showing that due to the opioid epidemic and coinciding changes in the economy, grandparents are sought out to raise children while parents with OUD seek treatment (Davis, Warfield, Boguslaw, Roundtree-Swain, & Kellogg, 2020). Together, these findings point to the need to consider not only children, but also extended family, such as grandparents/parents, in the development and implementation of interventions for women with OUD/PTSD. Indeed, maternal PTSD can negatively influence child outcomes (Moser et al., 2023) and most children placed in the foster care system are there as a result of laws proclaiming child abuse for pregnant persons with substance use disorders (Sanmartin, Ali, Lynch, & Aktas, 2020). Thus, dyadic and family-based interventions that attend to mothers with OUD/PTSD are of vital need. Women’s Recovery Group is one example of an intervention that has done extensive work on the benefit of including family members and caregivers into group therapy treatment for women with SUD (Greenfield et al., 2014). Group therapy is more cost-effective than individual treatment, and Women’s Recovery Group has been shown to predict six-month follow-up outcomes (Valeri et al., 2018). Despite these benefits, in our study, women expressed a preference for individual, trauma-focused, integrated treatment in both surveys and qualitative interviews where social support in a group format is an adjunct to integrated, individual treatment. Future work should examine how to best integrate social support into COPE since social support bolsters clinical outcomes in COPE (Jarnecke et al., 2022).
4.4. Treatment modifications & clinical implications
A wealth of suggestions was provided to modify COPE. We provide some possible solutions in Fig. 2. A few points that were debated among provider and patient participants are noted here. Many providers expressed concern of engaging in trauma treatment with women with OUD/PTSD due to fear that such patients were not stabilized enough to begin such work. While patient readiness is important to consider, it is also important to contend how realistically ‘stable’ individuals with OUD/PTSD can get without trauma-focused treatment and whether the denial of trauma-focused treatment to patients with OUD/PTSD treatment may be detrimental to their long-term health. It has been repeatedly shown that trauma-focused treatments, integrated or concurrent, are successful among individuals with co-occurring PTSD and substance use disorders and that the provision of evidence-based PTSD treatment does not worsen substance use (Hien et al., 2023). Understandable hesitation remains among providers. Thus, additional work on understanding thresholds of stability will be useful alongside dissemination efforts to educate providers on the absence of risks when providing evidence-based PTSD treatment to individuals with substance use disorders.
Fig. 2.
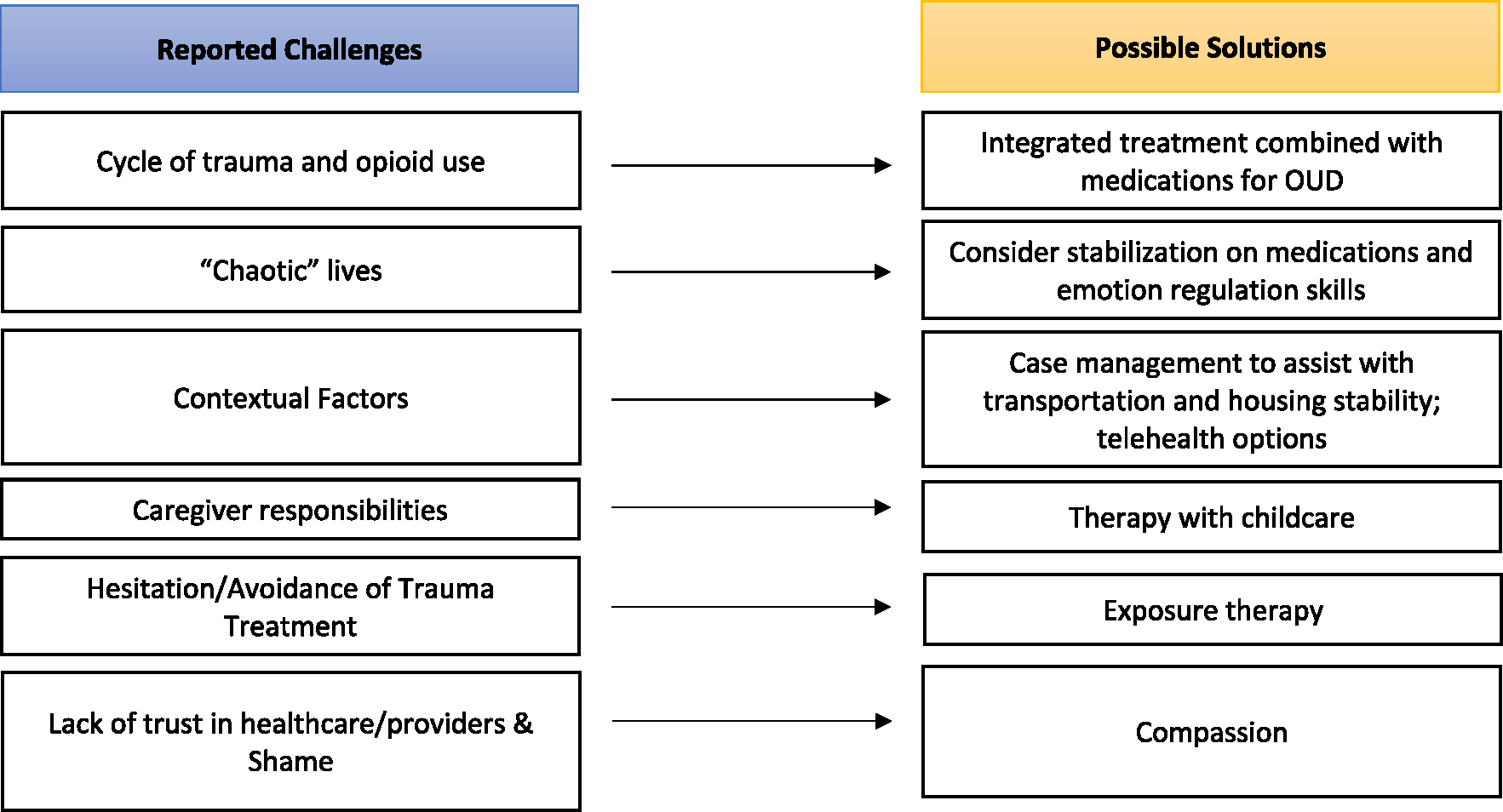
Summary of treatment barriers and possible solutions for women with OUD/PTSS.
Providers also expressed wanting additional distress tolerance and coping skills to help women with OUD/PTSD prior to exposure-based exercises. It may be critical to incorporate distress tolerance and coping skills for this population. However, it should be noted that less than half of the providers in our sample reported delivering PE or COPE. This may have influenced providers’ desire for incorporating distress tolerance skills into a modified version of COPE. Nevertheless, many of the providers trained in PE or other trauma-focused therapies reported a desire for incorporating greater distress tolerance skills. Thus, future work should examine how to mindfully incorporate such skills without delaying exposure. Future work should also distinguish between coping skills, which may be soothing and alleviate distress, and safety behaviors that may be used as an avoidance strategy and thereby reduce the efficacy of exposure exercises. Indeed, it may be beneficial to not only modify COPE, but to also augment it with a Dialectical Behavior Therapy group for women with OUD/PTSS considering our findings.
Furthermore, providers also expressed challenges in identifying the index trauma for women with OUD/PTSD and suggested including assistance on how to best identify these traumas. At present, COPE instructs providers to collaboratively work with patients to identify the index trauma which may generalize to other traumas. However, provider feedback suggests that multiple exposures for different trauma types may be warranted for women with OUD/PTSD. This was one reason why patient participants and providers also expressed a need for more flexible treatment protocols. Unfortunately, flexible protocols will not completely mitigate providers’ experiences of being under resourced and overburdened, which was found in a prior study as well (Saraiya et al., 2020). Systemic changes to interventions alongside public health initiatives that increase support of providers who work with women with OUD/PTSD and the women themselves must work in tandem to achieve long-term change.
4.5. Limitations
Several study limitations warrant consideration. The sample size was small, consisted of primarily white women, and the patient participants were well-educated. Thus, these findings and the corresponding clinical implications may not necessarily generalize to other patient samples as is common in qualitative research. However, it is a strength that many of these women lived in rural areas and showed a range in household income. Nevertheless, it is always imperative to capture multiple voices. Future work should purposively sample other demographic backgrounds. Another limitation of this study was our focus on self-identifying women, which may have inadvertently excluded individuals with other gender identities. Future work should purposively sample minoritized gender identities that are more likely to be stigmatized. An additional limitation in our sample was our inclusion of patient participants with dimensional levels of PTSS. Since not all women met full criteria for PTSD, these findings may not generalize to women with OUD/PTSD. In addition, some women discussed general distress rather than PTSD-specific symptoms. While this may be a limitation, a benefit of including individuals with PTSS is the ability to capture variation in responses to trauma exposure and attend to a larger group of patients than solely those diagnosed with PTSD. Indeed, COPE has been delivered to individuals with substance use disorders and co-occurring PTSS, and thus could be extended beyond individuals with PTSD solely (Ruglass et al., 2017). An additional observation in this study was the tendency for some self-report surveys to differ from information in qualitative interviews. Testing the reliability of self-report measures among women with OUD/PTSS is encouraged.
Our study is also limited in sampling providers working in an academic medical center. Such providers may be biased to have a high level of access to evidence-based treatment trainings for OUD/PTSD, and thus this small sample of providers may also not generalize to other providers. Nevertheless, prior work has sampled community service providers (e.g., Saraiya et al., 2020) and shown similar outcomes. Additionally, in the design of this study, participants were paid less than providers. This inequity was biased and should be avoided in future work so that patient participants and provider participants are paid equally. Finally, there is limited information on gender differences in psychosocial treatment outcomes for individuals with OUD/PTSD. Additional work in this area can provide further knowledge on how to design gender-focused treatments and whether they are beneficial.
4.6. Conclusion & future directions
In this study, women with OUD/PTSS and providers were interviewed on their experiences with having, or working with, OUD/PTSS and what they may desire in a modified, integrated treatment for OUD/PTSD. The next step will be to incorporate this feedback and modify the integrated treatment of COPE for women with OUD/PTSD followed by pilot testing the modified treatment with iterative modifications. In the design of such an intervention, the context of delivery should be evaluated given the growing diversity in opioid treatment program infrastructures. The modified intervention may also want to be flexible to a variety of symptom presentations, such as potentially traumatic events and dimensional PTSS. Developing this intervention may have large impact given that attending to women with OUD/PTSS could not only improve their lives, but also, indirectly improve the lives of their children and families as well.
Supplementary data to this article can be found online at https://doi.org/10.1016/j.josat.2024.209344.
Supplementary Material
Acknowledgements
We would like to thank the participants for sharing their experiences.
Funding
This work was funded in part by the Building Interdisciplinary Research Careers in Women’s Health (BIRCWH) K12 HD055885 (PI: McGinty) and the National Institute on Drug Abuse (NIDA) K23 DA055209 (PI: Saraiya). This publication’s contents are solely the responsibility of the authors and do not necessarily represent the official views of NIH.
Footnotes
Declaration of competing interest
The authors have no conflicts of interest to disclose.
CRediT authorship contribution statement
Tanya C. Saraiya: Writing – original draft, Supervision, Project administration, Methodology, Investigation, Funding acquisition, Formal analysis, Data curation, Conceptualization. Sarah Helpinstill: Writing – review & editing, Investigation, Formal analysis, Data curation. Daphne Gray: Investigation, Formal analysis, Data curation. Denise A. Hien: Writing – review & editing. Kathleen T. Brady: Writing – review & editing. Caitlyn O. Hood: Writing – review & editing. Sudie E. Back: Writing – review & editing, Supervision, Conceptualization.
References
- American Psychiatric Association. (2022). Diagnostic and statistical manual of mental disorders (5th ed., text rev.). American Psychiatric Publishing, Inc. 10.1176/appi.books.9780890425787.x07 [DOI] [Google Scholar]
- Back SE, Foa EB, Killeen T, Mills K, Teesson M, Dansky Cotton B, … Brady KT (2014). Concurrent treatment of PTSD and substance use disorders using prolonged exposure (COPE): Therapist manual. Oxford University Press. 10.1093/med:psych/9780199334513.001.0001 [DOI] [Google Scholar]
- Back SE, Killeen T, Badour CL, Flanagan JC, Allan NP, Ana ES, … Brady KT (2019). Concurrent treatment of substance use disorders and PTSD using prolonged exposure: A randomized clinical trial in military veterans. Addictive Behaviors, 90, 369–377. 10.1016/j.addbeh.2018.11.032 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Back SE, Killeen TK, Teer AP, Hartwell EE, Federline A, Beylotte F, & Cox E (2014). Substance use disorders and PTSD: An exploratory study of treatment preferences among military veterans. Addictive Behaviors, 39(2), 369–373. 10.1016/j.addbeh.2013.09.017 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Bale TL, & Epperson CN (2015). Sex differences and stress across the lifespan. Nature Neuroscience, 18(10), 1413–1420. 10.1038/nn.4112 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Barbosa-Leiker C, Campbell ANC, McHugh KR, Guille C, & Greenfield SF (2021). Opioid use disorder in women and the implications for treatment. Psychiatric Research and Clinical Practice, 3(1), 3–11. 10.1176/appi.prcp.20190051 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Becker SJ, DiClemente-Bosco K, Rash CJ, & Garner BR (2023). Effective, but underused: Lessons learned implementing contingency management in real-world practice settings in the United States. Preventive Medicine, 176, Article 107594. 10.1016/j.ypmed.2023.107594 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Braciszewski JM, Idu AE, Yarborough BJH, Stumbo SP, Bobb JF, Bradley KA, … Boudreau DM (2022). Sex differences in comorbid mental and substance use disorders among primary care patients with opioid use disorder. Psychiatric Services, 73(12), 1330–1337. 10.1176/appi.ps.202100665 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Butelman ER, Huang Y, Epstein DH, Shaham Y, Goldstein RZ, Volkow ND, & Alia-Klein N (2023). Overdose mortality rates for opioids and stimulant drugs are substantially higher in men than in women: State-level analysis. Neuropsychopharmacology, 48, 1639–1647. 10.1038/s41386-023-01601-8 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Campbell ANC, Barbosa-Leiker C, Hatch-Maillette M, Mennenga SE, Pavlicova M, Scodes J, … Greenfield SF (2018). Gender differences in demographic and clinical characteristics of patients with opioid use disorder entering a comparative effectiveness medication trial. The American Journal on Addictions, 27(6), 465–470. 10.1111/ajad.12784 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Chatterjee A, Yu EJ, & Tishberg L (2018). Exploring opioid use disorder, its impact, and treatment among individuals experiencing homelessness as part of a family. Drug and Alcohol Dependence, 188, 161–168. 10.1016/j.drugalcdep.2018.04.012 [DOI] [PubMed] [Google Scholar]
- Chun Tie Y, Birks M, & Francis K (2019). Grounded theory research: A design framework for novice researchers. SAGE Open Medicine, 7, Article 2050312118822927. 10.1177/2050312118822927 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Danovitch I (2016). Post-traumatic stress disorder and opioid use disorder: A narrative review of conceptual models. Journal of Addictive Diseases, 35(3), 169–179. 10.1080/10550887.2016.1168212 [DOI] [PubMed] [Google Scholar]
- Davis MT, Warfield ME, Boguslaw J, Roundtree-Swain D, & Kellogg G (2020). Parenting a 6-year old is not what I planned in retirement: Trauma and stress among grandparents due to the opioid crisis. Journal of Gerontology and Social Work, 63(4), 295–315. 10.1080/01634372.2020.1752872 [DOI] [PubMed] [Google Scholar]
- D’Orsogna MR, Bottcher L, & Chou T (2023). Fentanyl-driven acceleration of racial, gender and geographical disparities in drug overdose deaths in the United States. PLOS Global Public Health, 3(3), Article e0000769. 10.1371/journal.pgph.0000769 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Dunn KE, Weerts EM, Huhn AS, Schroeder JR, Tompkins DA, Bigelow GE, & Strain EC (2020). Preliminary evidence of different and clinically meaningful opioid withdrawal phenotypes. Addictive Biology, 25(1), Article e12680. 10.1111/adb.12680 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Elman I, & Borsook D (2019). The failing cascade: Comorbid post traumatic stress- and opioid use disorders. Neuroscience and Biobehavioral Reviews, 103, 374–383. 10.1016/j.neubiorev.2019.04.023 [DOI] [PubMed] [Google Scholar]
- Evans EA, Goff SL, Upchurch DM, & Grella CE (2020). Childhood adversity and mental health comorbidity in men and women with opioid use disorders. Addictive Behaviors, 102, Article 106149. 10.1016/j.addbeh.2019.106149 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Evans EA, Grella CE, Washington DL, & Upchurch DM (2017). Gender and race/ethnic differences in the persistence of alcohol, drug, and poly-substance use disorders. Drug and Alcohol Dependence, 174, 128–136. 10.1016/j.drugalcdep.2017.01.021 [DOI] [PubMed] [Google Scholar]
- Foa EB, Hembree EA, Rothbaum BO, & Rauch SAM (2019). Prolonged exposure therapy for PTSD: Emotional processing of traumatic experiences: Therapist guide (2nd ed.). Oxford University Press. 10.1093/med-psych/9780190926939.001.0001 [DOI] [Google Scholar]
- Gale NK, Heath G, Cameron E, Rashid S, & Redwood S (2013). Using the framework method for the analysis of qualitative data in multi-disciplinary health research. BMC Medical Research Methodology, 13(117), 1–8. 10.1186/1471-2288-13-117 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Giacomuzzi SM, Riemer Y, Ertl M, Kemmler G, Rossler H, Hinterhuber H, & Kurz M (2005). Gender differences in health-related quality of life on admission to a maintenance treatment program. European Addiction Research, 11(2), 69–75. 10.1159/000083035 [DOI] [PubMed] [Google Scholar]
- Greenfield SF, Cummings AM, Kuper LE, Wigderson SB, & Koro-Ljungberg M (2013). A qualitative analysis of women’s experiences in single-gender versus mixed-gender substance abuse group therapy. Substance Use & Misuse, 48(9), 750–760. 10.3109/10826084.2013.787100 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Greenfield SF, Sugarman DE, Freid CM, Bailey GL, Crisafulli MA, Kaufman JS, … Fitzmaurice GM (2014). Group therapy for women with substance use disorders: Results from the Women’s recovery group study. Drug and Alcohol Dependence, 142, 245–253. 10.1016/j.drugalcdep.2014.06.035 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Han B, Compton WM, Einstein EB, Cotto J, Hobin JA, Stein JB, & Volkow ND (2022). Intentional drug overdose deaths in the United States. American Journal of Psychiatry, 179(2), 163–165. 10.1176/appi.ajp.2021.21060604 [DOI] [PubMed] [Google Scholar]
- Heck AL, & Handa RJ (2019). Sex differences in the hypothalamic-pituitary-adrenal axis’ response to stress: An important role for gonadal hormones. Neuropsychopharmacology, 44(1), 45–58. 10.1038/s41386-018-0167-9 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Hien DA, Morgan-Lopez AA, Saavedra LM, Ruglass LM, Ye A, Lopez-Castro T, … Back SE (2023). Project harmony: A meta-analysis with individual patient data on behavioral and pharmacologic trials for comorbid posttraumatic stress and alcohol or other drug use disorders. American Journal of Psychiatry, 180(2), 155–166. 10.1176/appi.ajp.22010071 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Hooker S, Sherman MD, Lonergan-Cullum M, Sattler A, Liese BS, Justesen K, … Levy R (2020). Mental health and psychosocial needs of patients being treated for opioid use disorder in a primary care residency clinic. Journal of Primary Care & Community Health, 11, 1–8. 10.1177/2150132720932017 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Huhn AS, Berry MS, & Dunn KE (2019). Review: Sex-based differences in treatment outcomes for persons with opioid use disorder. The American Journal on Addictions, 28(4), 246–261. 10.1111/ajad.12921 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Huhn AS, & Dunn KE (2020). Challenges for women entering treatment for opioid use disorder. Current Psychiatry Reports, 22(12), 76. 10.1007/s11920-020-01201-z [DOI] [PubMed] [Google Scholar]
- Humphreys K, Shover CL, Andrews CM, Bohnert ASB, Brandeau ML, Caulkins JP, … Timko C (2022). Responding to the opioid crisis in north america and beyond: Recommendations of the Stanford–lancet commission. The Lancet, 399 (10324), 555–604. 10.1016/S0140-6736(21)02252-2 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Jarnecke AM, Saraiya TC, Brown DG, Richardson J, Killeen T, & Back SE (2022). Examining the role of social support in treatment for co-occurring substance use disorder and posttraumatic stress disorder. Addictive Behaviors Reports, 15, Article 100427. 10.1016/j.abrep.2022.100427 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Jones CM, Han B, Baldwin GT, Einstein EB, & Compton WM (2023). Use of medication for opioid use disorder among adults with past-year opioid use disorder in the US, 2021. JAMA Network Open, 6(8), e2327488. 10.1001/jamanetworkopen.2023.27488 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Kadden R, Carroll K, Donovan D, Cooney N, Monti P, Abrams D, Litt M, & Hester R (1992). Cognitive-behavioral coping skills therapy manual: A clinical research guide for therapists treating individuals with alcohol abuse and dependence. National Institute on Alcohol Abuse and Alcoholism. https://www.niaaa.nih.gov/sites/default/files/match03.pdf.
- Kessler RC, Sonnega A, Bromet E, Hughes M, & Nelson CB (1995). Posttraumatic stress disorder in the national comorbidity survey. Archives of General Psychiatry, 52 (12), 1048–1060. 10.1001/archpsyc.1995.03950240066012 [DOI] [PubMed] [Google Scholar]
- Lingard L (2019). Beyond the default colon: Effective use of quotes in qualitative research. Perspectives on. Medical Education, 8(6), 360–364. 10.1007/s40037-019-00550-7 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Livingston NA, Simpson T, Lehavot K, Ameral V, Brief DJ, Enggasser J, … Keane TM (2021). Differential alcohol treatment response by gender following use of VetChange. Drug and Alcohol Dependence, 221, Article 108552. 10.1016/j.drugalcdep.2021.108552 [DOI] [PubMed] [Google Scholar]
- López-Castro T, Saraiya T, & Hien DA (2017). Women, trauma, and PTSD. In I. K. A. Kendall-Tackett, & L. M. (Eds.), Ruglass Women’s mental health across the lifespan: Challenges, vulnerabilities, and strengths (pp. 175–193). Routledge/Taylor & Francis Group. 10.4324/9781315641928-10. [DOI] [Google Scholar]
- Martin EL, Neelon B, Brady KT, Guille C, Baker NL, Ramakrishnan V, … McRae-Clark AL (2023). Differential prevalence of adverse childhood experiences (ACEs) by gender and substance used in individuals with cannabis, cocaine, opioid, and tobacco use disorders. The American Journal of Drug and Alcohol Abuse, 1–9. 10.1080/00952990.2023.2171301 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Mazure CM, & Fiellin DA (2018). Women and opioids: Something different is happening here. Lancet, 392(10141), 9–11. 10.1016/S0140-6736(18)31203-0 [DOI] [PubMed] [Google Scholar]
- McLean CP, Asnaani A, Litz BT, & Hofmann SG (2011). Gender differences in anxiety disorders: Prevalence, course of illness, comorbidity and burden of illness. Journal of Psychiatric Research, 45(8), 1027–1035. 10.1016/j.jpsychires.2011.03.006 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Meshberg-Cohen S, Ross MacLean R, Schnakenberg Martin AM, Sofuoglu M, & Petrakis IL (2021). Treatment outcomes in individuals diagnosed with comorbid opioid use disorder and posttraumatic stress disorder: A review. Addictive Behaviors, 122, Article 107026. 10.1016/j.addbeh.2021.107026 [DOI] [PubMed] [Google Scholar]
- Mills KL, Teesson M, Back SE, Brady KT, Baker AL, Hopwood S, … Ewer PL (2012). Integrated exposure-based therapy for co-occurring posttraumatic stress disorder and substance dependence: A randomized controlled trial. JAMA, 308(7), 690–699. 10.1001/jama.2012.9071 [DOI] [PubMed] [Google Scholar]
- Morse DS, Cerulli C, Hordes M, El-Bassel N, Bleasdale J, Wilson K, … Przybyla SM (2022). “I was 15 when I started doing drugs with my dad”: Victimization, social determinants of health, and criminogenic risk among women opioid intervention court participants. Journal of Interpersonal Violence, 8862605211052053. 10.1177/08862605211052053 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Moser DA, Graf S, Glaus J, Urben S, Jouabli S, Pointet Perrizolo V, … Schechter DS (2023). On the complex and dimensional relationship of maternal posttraumatic stress disorder during early childhood and child outcomes at school-age. European Psychiatry, 66(1), Article e20. 10.1192/j.eurpsy.2023.8 [DOI] [PMC free article] [PubMed] [Google Scholar]
- National Institute on Drug Abuse. (2017). February 13. Unintentional Overdose Deaths: Intentional vs. https://nida.nih.gov/research-topics/trends-statistics/overdose-death-rates/intentional-vs-unintentional-overdose-deaths. [Google Scholar]
- Norman SB, Trim R, Haller M, Davis BC, Myers US, Colvonen PJ, … Mayes T (2019). Efficacy of integrated exposure therapy vs integrated coping skills therapy for comorbid posttraumatic stress disorder and alcohol use disorder: A randomized clinical trial. JAMA Psychiatry, 76(8), 791–799. 10.1001/jamapsychiatry.2019.0638 [DOI] [PMC free article] [PubMed] [Google Scholar]
- O’Brien BC, Harris IB, Beckman TJ, Reed DA, & Cook DA (2014). Standards for reporting qualitative research: A synthesis of recommendations. Academic Medicine, 89(9), 1245–1251. 10.1097/ACM.0000000000000388 [DOI] [PubMed] [Google Scholar]
- Office on Women”s Health. (2017). Final report: Opioid use, misuse, and overdose in women. Department of Health and Human Services: U.S. https://www.rmtlc.org/wp-content/uploads/2017/08/final-report-opioid-508.pdf. [Google Scholar]
- Olff M (2017). Sex and gender differences in post-traumatic stress disorder: An update. European Journal of Psychotraumatology, 8(sup4), 1351204. 10.1080/20008198.2017.1351204 [DOI] [Google Scholar]
- Overstreet C, Berenz EC, Kendler KS, Dick DM, & Amstadter AB (2017). Predictors and mental health outcomes of potentially traumatic event exposure. Psychiatry Research, 247, 296–304. 10.1016/j.psychres.2016.10.047 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Parisi A, Hudak J, Froeliger B, & Garland EL (2023). Mindfulness-oriented recovery enhancement reduces post-traumatic stress via reappraisal among patients with chronic pain and co-occurring opioid misuse. Nature Mental Health, 1(7), 489–500. 10.1038/s44220-023-00084-2 [DOI] [Google Scholar]
- Peck KR, Badger GJ, Cole R, Higgins ST, Moxley-Kelly N, & Sigmon SC (2023). Prolonged exposure therapy for PTSD in individuals with opioid use disorder: A randomized pilot study. Addictive Behaviors, 143, Article 107688. 10.1016/j.addbeh.2023.107688 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Peck KR, Schumacher JA, Stasiewicz PR, & Coffey SF (2018). Adults with comorbid posttraumatic stress disorder, alcohol use disorder, and opioid use disorder: The effectiveness of modified prolonged exposure. Journal of Traumatic Stress, 31(3), 373–382. 10.1002/jts.22291 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Peirce JM, Brooner RK, King VL, & Kidorf MS (2016). Effect of traumatic event reexposure and PTSD on substance use disorder treatment response. Drug and Alcohol Dependence, 158, 126–131. 10.1016/j.drugalcdep.2015.11.006 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Ruglass LM, Lopez-Castro T, Papini S, Killeen T, Back SE, & Hien DA (2017). Concurrent treatment with prolonged exposure for co-occurring full or subthreshold posttraumatic stress disorder and substance use disorders: A randomized clinical trial. Psychotherapy and Psychosomatics, 86(3), 150–161. 10.1159/000462977 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Sanmartin MX, Ali MM, Lynch S, & Aktas A (2020). Association between state-level criminal justice-focused prenatal substance use policies in the US and substance use-related foster care admissions and family reunification. JAMA Pediatrics, 174(8), 782–788. 10.1001/jamapediatrics.2020.1027 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Santo T, Campbell G, Gisev N, Tran L, Colledge S, Di Tanna GL, & Degenhardt L (2021). Prevalence of childhood maltreatment among people with opioid use disorder: A systematic review and meta-analysis. Drug and Alcohol Dependence, 219, Article 108459. 10.1016/j.drugalcdep.2020.108459 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Saraiya TC, Back SE, Jarnecke AM, Blakey SM, Bauer AG, Brown DG, … Hien DA (2023). Sex and gender differences in co-occurring alcohol use disorder and PTSD. Current Addiction Reports. 10.1007/s40429-023-00511-5 [DOI] [Google Scholar]
- Saraiya TC, Jarnecke AM, Jones J, Brown DG, Brady KT, & Back SE (2021). Laboratory-induced stress and craving predict opioid use during follow-up among individuals with prescription opioid use disorder. Drug and Alcohol Dependence, 225, Article 108755. 10.1016/j.drugalcdep.2021.108755 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Saraiya TC, Swarbrick M, Franklin L, Kass S, Campbell ANC, & Hien DA (2020). Perspectives on trauma and the design of a technology-based trauma-informed intervention for women receiving medications for addiction treatment in community-based settings. Journal of Substance Abuse Treatment, 112, 92–101. 10.1016/j.jsat.2020.01.011 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Saunders B, Sim J, Kingstone T, Baker S, Waterfield J, Bartlam B, Burroughs H, & Jinks C (2018). Saturation in qualitative research: exploring its conceptualization and operationalization. Quality & quantity, 52(4), 1893–1907. 10.1007/s11135-017-0574-8 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Schacht RL, Brooner RK, King VL, Kidorf MS, & Peirce JM (2017). Incentivizing attendance to prolonged exposure for PTSD with opioid use disorder patients: A randomized controlled trial. Journal of Consulting and Clinical Psychology, 85(7), 689–701. 10.1037/ccp0000208 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Schacht RL, Wenzel KR, Meyer LE, Mette M, Mallik-Kane K, Rabalais A, … Fishman M (2023). A pilot test of written exposure therapy for PTSD in residential substance use treatment. The American Journal on Addictions, 32(5), 488–496. 10.1111/ajad.13442 [DOI] [PubMed] [Google Scholar]
- Schiff M, Nacasch N, Levit S, Katz N, & Foa EB (2015). Prolonged exposure for treating PTSD among female methadone patients who were survivors of sexual abuse in Israel. Social Work in Health Care, 54(8), 687–707. 10.1080/00981389.2015.1058311 [DOI] [PubMed] [Google Scholar]
- Sheehan DV, Lecrubier Y, Sheehan KH, Amorim P, Janavs J, Weiller E, … Dunbar GC (1998). The mini-international neuropsychiatric interview (M.I.N.I.): The development and validation of a structured diagnostic psychiatric interview for DSM-IV and ICD-10. Journal of Clinical Psychiatry, 59 Suppl 20, 22–57. [PubMed] [Google Scholar]
- Smith KZ, Smith PH, Cercone SA, McKee SA, & Homish GG (2016). Past year non-medical opioid use and abuse and PTSD diagnosis: Interactions with sex and associations with symptom clusters. Addictive Behaviors, 58, 167–174. 10.1016/j.addbeh.2016.02.019 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Springer SA, Biondi BE, Frank C, & El-Bassel N (2020). A call to action to combat the opioid epidemic among women. Journal of Addiction Medicine, 14(5), 364–366. 10.1097/adm.0000000000000622 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Terplan M (2017). Women and the opioid crisis: Historical context and public health solutions. Fertility and Sterility, 108(2), 195–199. 10.1016/j.fertnstert.2017.06.007 [DOI] [PubMed] [Google Scholar]
- Tolin DF, & Foa EB (2006). Sex differences in trauma and posttraumatic stress disorder: A quantitative review of 25 years of research. Psychological Bulletin, 132(6), 959–992. 10.1037/0033-2909.132.6.959 [DOI] [PubMed] [Google Scholar]
- Valeri L, Sugarman DE, Reilly ME, McHugh RK, Fitzmaurice GM, & Greenfield SF (2018). Group therapy for women with substance use disorders: In-session affiliation predicts women’s substance use treatment outcomes. Journal of Substance Abuse Treatment, 94, 60–68. 10.1016/j.jsat.2018.08.008 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Weathers FW, Blake DD, Schnurr PP, Kaloupek DG, Marx BP, & Keane TM (2013). The life events checklist for DSM-5 (LEC-5). National Center for PTSD. https://www.ptsd.va.gov.
- Weathers FW, Litz BT, Keane TM, Palmieri PA, Marx BP, & PP. S. (2013). The PTSD checklist for DSM-5 (PCL-5). National Center for PTSD. www.ptsd.va.gov. [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.