

Abstract
Health literacy (HL) is crucial in achieving the Sustainable Development Goal of reducing one-third of premature mortality by 2030 from Non-Communicable Diseases (NCDs) and improving Universal Health Coverage. Low health literacy is linked to poor health outcomes, and evidence shows that levels of limited HL are high, even among highly educated individuals. This study aims to assess HL levels and related factors among patients with NCDs at Tribhuvan University Teaching Hospital (TUTH) in Nepal. A cross-sectional survey was conducted at TUTH among 303 patients with NCDs with Cardiovascular Diseases, Chronic Obstructive Pulmonary Disease, Diabetes Mellitus, Hypertension, Epilepsy, Asthma and Cancer who came for follow-up from December 2022 to February 2023. Data was collected via face-to-face interviews by the trained enumerators using a structured Health Literacy Questionnaire (HLQ) containing 44 items (divided into nine domains). Multivariate logistic regression analysis was performed using SPSS version 26, with statistical significance at 0.05, to determine the associated factors of HL. The mean ±SD age of the respondents was 47.4±16.18 years. More than half of the respondents were female (56.1%). The patients had higher HL in all HL domains except ‘Navigating the healthcare system’. Educational status was significantly associated with six out of nine HL domains. Co-morbidity, attendance at health-related seminars, regular physical activity, and social connectedness were associated with at least one of the domains of HL. This study identified the important factors of HL, such as socio-demographic and medical factors among patients with NCDs. This highlights the need for a comprehensive approach to address identified gaps in HL, considering its multifaceted and composite nature and promoting interventions to improve HL in high-risk populations.
Introduction
The world is striving towards achieving the Sustainable Development Goal (SDG) target 3.4 to ‘reduce by one-third premature mortality from non-communicable diseases (NCDs) by the year 2030’ [1]. NCDs account for 74% of the global mortality, with 17 million deaths occurring before the age of seventy. Of these premature deaths, 86% are concentrated in low-and middle-income countries (LMICs) [1]. Authorities in the last two decades have been unable to progress significantly and attain the global voluntary NCD targets. The complexities in addressing NCD services were further exacerbated by the COVID-19 pandemic, as evidenced by the high burden among NCD patients [2]. The rapid upsurge of misinformation and disinformation spread through social media has impeded initiatives aimed at preventing and managing NCDs, leading to the amplification of health disparities on a global scale [3].
Health literacy (HL) is defined as ‘the cognitive and social skills which determine the motivation and ability of individuals to gain access to, understand and use information in ways which promote and maintain good health’ [4]. The World Health Organization (WHO) has emphasised the significance of HL in achieving SDG 3 and its importance in enhancing Universal Health Coverage (UHC) [5] as HL comprises various skills that influence the capability of patients to assess health care and use the healthcare system [6]. HL is fundamental in reducing the impact and lowering the risk of NCDs. The majority of premature deaths from NCDs, accounting for more than one-fourth of all fatalities worldwide, may have been prevented by enhancing HL, which enables individuals to take an active role in their health [7, 8]. HL is an important determinant of people’s health condition, affecting health status and demonstrating social hierarchy [9].
A systematic review of the literature indicates that the elderly population with low levels of HL experiences worse health status, resulting in increased mortality [10]. Additionally, an inadequate HL among hospitalised patients is independently associated with adverse outcomes, such as higher hospital readmission rates [11]. In Nepal, only 27% of chronic disease patients had adequate HL [12], while 61% of university students reported having limited HL [13]. Similarly, a study conducted in the provinces of Calabria and Sicily revealed that only 35% of the Mediterranean general population had adequate HL [14]. In Europe, a population-based study on HL revealed that 47% of the individuals had limited HL [15]. Surprisingly, general education level doesn’t reliably predict an individual’s HL; even those with postgraduate qualifications were found to have poor HL skills [16].
However, to our knowledge, there is limited information about the HL of individuals with NCDs in Nepal. This study assessed the Health Literacy Level (HLL) and associated factors among patients with NCDs visiting a tertiary-level health centre in Nepal.
Materials and methods
Study design and site
A cross-sectional study was conducted at Tribhuvan University Teaching Hospital (TUTH) from December 2022 to February 2023. TUTH is one of the pioneering and largest tertiary-level hospitals in Nepal. It provides integrated clinical services, outpatient services, education, and research facilities to around 2500 outpatients daily. People from all over Nepal visit TUTH to receive various healthcare services.
Study population
The study population for this study were patients with NCDs- Cardiovascular Diseases (CVDs), Chronic Obstructive Pulmonary Disease (COPD), Diabetes Mellitus (DM), Hypertension, Epilepsy, Asthma and Cancer. Patients aged 18 years and above with NCDs who provided informed consent and were currently undergoing follow-up care at the outpatient department of TUTH were recruited for this study. However, patients with cognitive impairments or hearing disabilities were excluded from the study as it limits their capability to participate in the study.
Sample size and sampling technique
The sample size was calculated using the one-proportion formula n = Z2 p q / d2, with the following assumptions: p = 0.27 (12), q = 0.73, and z = 1.96 at 95% CI and d = 0.05. Assuming a 10% non-response rate, the sample size was 334. A purposive sampling technique was used to select study participants, as it was not feasible to establish a sampling frame for the random sampling methods in the hospital’s outpatient department setting.
Data collection tools and techniques
HL was measured using a 44-item multi-dimensional Health Literacy Questionnaire (HLQ) after receiving approval from Swinburne University of Technology [17]. This questionnaire, developed by Osborne and the team, evaluates nine aspects of HL and has also been validated in Nepal [18]. The nine domains of HLQ include:
Feeling understood and supported by healthcare providers (4 items)
Having sufficient information to manage my health (4 items)
Actively managing own health (5 items)
Social support for health (5 items)
Appraisal of Health Information (5 items)
Ability to actively engage with healthcare providers (5 items)
Navigating the healthcare system (6 items)
Ability to find good health information (5 items)
Understanding health information well enough to know what to do (5 items) [17].
Participants in the study were asked to indicate their level of agreement with statements in domains 1 to 5 using a scale where 1 = strongly disagree, 2 = disagree, 3 = agree, and 4 = strongly agree. For domains 6 to 9, participants responded on a scale where 1 = always difficult, 2 = usually difficult, 3 = sometimes difficult, 4 = usually easy, and 5 = always easy [17].
To calculate the mean score for each domain, the item scores were added together, multiplied by the total number of items within the domain, and then divided by the maximum possible score for that domain [19]. Participants who scored at or above the mean score for each domain of the HLQ were categorised as having ’high Health Literacy Level (HLL)’, while those who scored below the mean score were classified as having ’low HLL’.
There is no single total HL score, as the multidimensional nature of the construct is better represented by separate scores for each of the nine domains. These domains are conceptually distinct, and separate scores provide insights into the strengths and limitations of the respondents [17, 20]. The Nepali version of the HLQ, along with socio-demographic and health-related information sources (healthcare providers, internet, books, family, friends, television, radio), was used to collect the information from the participants. The Cronbach’s alpha for each domain was more than 0.8, indicating a higher level of internal consistency among the items in each domain. Data from the respondents were collected through a paper-based structured questionnaire via face-to-face interviews conducted by the trained enumerators.
Statistical analysis
The collected data were initially entered in Excel and subsequently imported into IBM SPSS version 26 for further analysis. Both descriptive and inferential analyses were performed to gain insights from the dataset. Descriptive analysis was conducted to determine the frequencies and percentages of participants’ sociodemographic characteristics. The normality of the data was assessed using the Shapiro-Wilk test. Multicollinearity tests were performed for all independent variables before data analysis. The Variance Inflation Factor (VIF) was <10, and the tolerance test yielded values less than one for each independent variable. The nine domains of the HLQ were treated as dependent variables. At the same time; age, gender, educational status, religion, ethnicity, occupation, economic status, residence, chronic disease profile, presence of co-morbidity, complications arising from NCDs, involvement in social activities, regular engagement in physical activities, attendance at health-related seminars, and social connectedness were considered as independent variables. The association between categorical HL score and categorical independent variables was assessed using the Chi-square test at the 95% significance level. Independent variables that demonstrated statistical significance were subsequently included in binary logistic regression. The multivariate logistic regression model fitted those variables with p-values less than 0.1 in the bivariate analysis.
Ethical approval
Ethical approval was obtained from the Institutional Review Committee (Ref:329(6–11)E2) of the Institute of Medicine, Tribhuvan University, Nepal. Participants were informed that their participation was voluntary and assured of their anonymity and the confidential treatment of their responses before consent. A license to administer HLQ was obtained from Swinburne University of Technology.
Results
A total of 303 participants attending the outpatient department consented to participate, resulting in a response rate of 90%.
Socio-demographic characteristics
A total of 303 patients attending the outpatient department were included in the study. The mean ±SD age of the respondent was 47.4±16.18 years, with 56.1% female. A notable portion had higher education (26.1%), while 27.4% were illiterate. The majority of patients were Hindu (86.1%), with 29% belonging to the ‘Chhetri’ ethnic group. Most patients were homemakers (35.3%), and 72.3% were from the urban municipality, as presented in Table 1. (S1 File).
Table 1. Socio-demographic and medical characteristics of the respondents (n = 303).
| Characteristics | Category | Number (%) |
|---|---|---|
| Age | 18–44 | 121(39.9) |
| 45–64 | 137 (45.2) | |
| 65 and above | 45 (14.9) | |
| Gender | Female | 170 (56.1) |
| Male | 133 (43.9) | |
| Educational status | Illiterate | 83 (27.4) |
| Basic level | 72 (23.8) | |
| Secondary level | 69 (22.8) | |
| Higher education | 79 (26.1) | |
| Marital status | Married | 258 (85.2) |
| Unmarried | 45 (14.8) | |
| Religion | Hindu | 261 (86.1) |
| Buddhism | 29 (9.6) | |
| Others | 13(4.3) | |
| Ethnicity | Chhetri | 88 (29) |
| Brahmin | 86 (28.4) | |
| Janajati | 85 (28.1) | |
| Others* | 44 (14.5) | |
| Occupation | Housewife | 107 (35.3) |
| Unemployed | 38 (12.5) | |
| Employed | 67 (22.1) | |
| Agriculture | 43 (14.2) | |
| Others | 48 (15.8) | |
| Economic status | Below poverty line (< $ 2.15 USD/day) | 31 (10.2) |
| Above poverty line (> $ 2.15 USD/day) | 272 (89.8) | |
| Residence | Rural municipality | 84 (27.7) |
| Municipality | 219 (72.3) | |
| Type of NCDs | CVDs | 36 (11.9) |
| Diabetes | 81 (26.7) | |
| Hypertension | 95 (31.4) | |
| Asthma | 62 (20.5) | |
| Others** | 78 (25.7) | |
| Presence of co-morbidity | Yes | 106 (35) |
| Complications from NCDs | Yes | 84 (27.7) |
| Involving in social activities | Yes | 211 (69.6) |
| Regular exercise | Yes | 197 (65) |
| Attending health related seminars | Yes | 119 (39.3) |
| Social connectedness | Yes | 262 (86.5) |
Others* Tharu, Dalit, Thakuri; Others** Cancer, COPD, Epilepsy
Medical history
About the medical history of the patients, 35% had comorbidities, hypertension (31.4%) and diabetes (26.7%) being the most prevalent conditions. The majority (69.6%) engaged in social activities, and 65% participated in regular physical activities. Additionally, 86.5% reported having social connections and interpersonal relationships, as presented in Table 1.
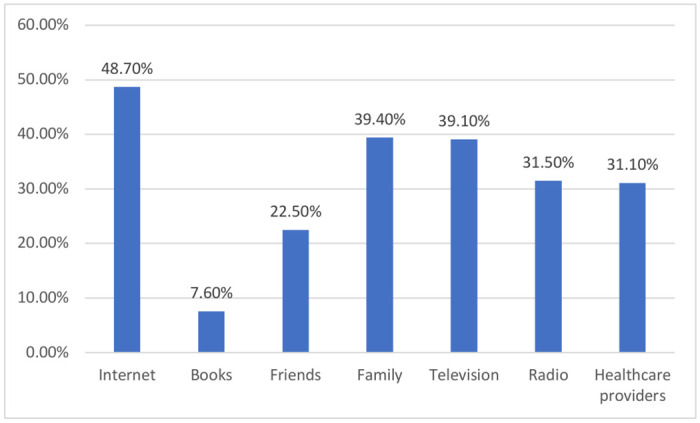
Sources of health information
Internet was the primary source of health information for most patients (48.7%), followed by family members (39.4%), with only 31.1% obtaining health information from healthcare providers, as depicted in Fig 1.
Fig 1. Distribution of sources of health information.
Health literacy level
The first five domains exhibited high HLL. The highest HLL was observed for ‘Appraisal of health information’ (79.5%), while the lowest was for ‘Feeling understood and supported by healthcare providers’ (60.4%). For the last four domains, the highest HLL was for ‘Ability to actively engage with healthcare providers’ (60.7%), while ‘Navigating the healthcare system’ (18.2%) had the lowest, as presented in Table 2.
Table 2. Health literacy level of respondents across different domains of HLQ (n = 303).
| HL domains | Mean (SD±) | HLL | |
|---|---|---|---|
| High HLL | Low HLL | ||
| 1. Feeling understood and supported by healthcare providers | 2.70 (0.477) | 60.4% | 39.6% |
| 2. Having sufficient information to manage my health | 2.78 (0.43) | 67.3% | 32.7% |
| 3. Actively managing own health | 2.71 (0.48) | 68% | 32% |
| 4. Social support for health | 2.69 (0.48) | 65.3% | 34.7% |
| 5. Appraisal of Health Information | 2.80 (0.42) | 79.5% | 20.5% |
| 6. Ability to actively engage with healthcare providers | 3.25 (0.80) | 60.7% | 39.3% |
| 7. Navigating the healthcare system | 2.69 (0.46) | 18.2% | 81.8% |
| 8. Ability to find good health information | 3.21 (0.91) | 58.7% | 41.3% |
| 9. Understand health information well enough to know what to do | 3.13 (0.88) | 55.8% | 44.2% |
Factors associated with health literacy domains
Gender was significantly associated with ‘Feeling understood and supported by healthcare providers’. Educational status was significantly associated with six domains of HL except ‘Actively managing own health’, ‘Appraisal of health information’, and ‘Navigating the healthcare system’. Respondents with a higher education level were more likely to have higher HL than illiterate respondents: 6.19 (95%CI: 2.30, 16.64) times more likely to have higher HL for ’Feeling understood and supported by healthcare providers’, 5.51(95%CI:2.04,14.98) times higher HL for ‘Having sufficient information to manage their health’, 5.62 (95%CI:2.15,14.76) times higher HL for ‘Social support for health’, 16.43 (95%CI:5.47,48.99) times higher HL for ‘Ability to actively engage with healthcare providers’, 38.79(95%CI:11.2,134) times higher HL for ability to ‘Find good health information’ and 14.84 (95%CI:5.07,43.54) times higher HL for ‘Understand health information well enough to know what to do’ than the illiterate respondents respectively as presented in Tables 3 and 4.
Table 3. Multivariate logistic regression for factors associated with HL domain 1 to 5.
| Variables | Category | Domain 1 | Domain 2 | Domain 3 | Domain 4 | Domain 5 |
|---|---|---|---|---|---|---|
| AOR# (95%CI) | AOR# (95%CI) | AOR# (95%CI) | AOR# (95%CI) | AOR# (95%CI) | ||
| Age group | 18–44 | 1 | 1 | 1 | 1 | 1 |
| 45–64 | 0.74(0.37,1.49) | 1.42(0.68,2.93) | 0.85(0.42,1.73) | 1.33(0.66,2.64) | 1.87(0.80,4.38) | |
| ≥65 | 0.33(0.12,0.88)* | 0.82(0.31,2.19) | 0.49(0.19,1.28) | 1.46(0.57,3.77) | 1.16(0.38,3.50) | |
| Gender | Male | 1 | 1 | 1 | 1 | 1 |
| Female | 0.45(0.22,0.92)* | 0.99(0.48,2.03) | 0.74(0.36,1.28) | 1.24(0.62,2.50) | 0.68(0.29,1.60) | |
| Educational status | Illiterate | 1 | 1 | 1 | 1 | 1 |
| Basic level | 3.33(1.52,7.3)** | 3.85(1.72,8.62)** | 0.90(0.41,1.95) | 2.63(1.24,5.59)** | 2.15(0.82,5.63) | |
| Secondary level | 2.48(1.07,5.75)* | 4.53(1.86,11.00)** | 1.29(0.54,3.08) | 5.33(2.2,12.8)** | 1.27(0.47,3.44) | |
| Higher education | 6.18(2.30,16.64)** | 5.5(2.03,14.8)** | 2.01(0.73,5.52) | 5.6(2.15,14.6)** | 2.69(0.83,8.68) | |
| Occupation | Housewife | 1 | 1 | 1 | 1 | 1 |
| Employed | 0.94(0.37,2.39) | 0.73(0.28,1.89) | 1.66(0.62,4.39) | 1.49(0.58,3.82) | 1.33(0.43,4.12) | |
| Agriculture | 0.72(0.28,1.88) | 1.20(0.46,3.16) | 0.96(0.38,2.43) | 1.27(0.50,3.27) | 1.01(0.34,2.94) | |
| Others | 1.61(0.71,3.62) | 1.61(0.70,3.68) | 1.62(0.73,3.58) | 1.39(0.64,3.04) | 1.96(0.79,4.90) | |
| Residence | Rural | 1 | 1 | 1 | 1 | 1 |
| Urban | 1.78(0.97,3.31) | 1.51(0.81,2.81) | 1.42(0.78,2.61) | 1.08(0.59,1.97) | 0.99(0.49,2.00) | |
| Co-morbidity | Yes | 1 | 1 | 1 | 1 | 1 |
| No | 0.80(0.44,1.46) | 1.09(0.59,1.96) | 1.21(0.68,2.17) | 1.35(0.77,2.39) | 1.67(0.88,3.24) | |
| Involving in social activities | Yes | 1 | 1 | 1 | 1 | 1 |
| No | 0.81(0.42,1.55) | 2.24(1.09,4.59) | 1.57(0.87,3.06) | 1.08(0.57,2.06) | 1.52(0.70,3.30) | |
| Regular physical activity | Yes | 1 | 1 | 1 | 1 | 1 |
| No | 0.45(0.24,0.82)* | 0.51(0.28,0.92)* | 0.56(0.31,1.01) | 0.57(0.34,1.23) | 0.36(0.19,0.70) | |
| Attending health related seminar | Yes | 1 | 1 | 1 | 1 | 1 |
| No | 0.82(0.43,1.55) | 0.36(0.18,0.71)** | 0.43(0.22,0.84)* | 0.65(0.34,1.23) | 0.51(0.23,1.15) | |
| Social connectedness | Yes | 1 | 1 | 1 | 1 | 1 |
| No | 0.45(0.18,1.11) | 0.45(0.18,1.09) | 0.35(0.15,0.82)* | 0.61(0.26,1.42) | 0.37(0.15,0.92)* |
Domain1, Feeling understood and supported by healthcare providers; Domain2, Having sufficient information to manage my health; Domain3, Actively managing own health; Domain4, Social support for health; Domain5, Appraisal of Health Information
#AOR: Adjusted Odds Ratio,
*significantly associated at <0.05,
**significantly associated at <0.01,
1-Reference category
Table 4. Multivariate logistic regression for factors associated with HL domain 6 to 9.
| Variables | Category | Domain 6 | Domain 7 | Domain 8 | Domain 9 |
|---|---|---|---|---|---|
| AOR# (95%CI) | AOR# (95%CI) | AOR# (95%CI) | AOR# (95%CI) | ||
| Age group | 18–44 | 1 | 1 | 1 | 1 |
| 45–64 | 1.05(0.53,2.11) | 1.02(0.45,2.31) | 0.55(0.26,1.19) | 0.63(0.31,1.29) | |
| ≥65 | 1.29(0.49,3.39) | 2.12(0.63,7.06) | 0.63(0.21,1.83) | 0.33(0.11,0.94) | |
| Gender | Male | 1 | 1 | 1 | 1 |
| Female | 0.61(0.29,1.26) | 0.81(0.36,1.82) | 0.51(0.23,1.15) | 0.55(0.26,1.15) | |
| Educational status | Illiterate | 1 | 1 | 1 | 1 |
| Basic level | 2.82(1.31,6.05)** | 0.87(0.26,2.85) | 5.47(2.25,13.3)** | 2.65(1.16,6.04)** | |
| Secondary level | 4.20(1.78,9.89)** | 1.77(0.54,5.74) | 17(6.22,46.6)** | 6.79(2.75,16.7)** | |
| Higher education | 16.4(5.47,48.9)** | 3.18(0.95,10.6) | 38.79(11.2,134)** | 14.8(5.06,43.5)** | |
| Occupation | Housewife | 1 | 1 | 1 | 1 |
| Employed | 1.03(0.39,2.74) | 2.15(0.76,6.06) | 1.33(0.44,4.00) | 1.15(0.43,3.12) | |
| Agriculture | 0.48(0.18,1.24) | 0.37(0.07,2.06) | 0.86(0.31,2.41) | 0.73(0.27,1.96) | |
| Others | 1.08(0.48,2.42) | 0.99(0.36,2.71) | 1.01(0.40,2.50) | 0.93(0.39,2.20) | |
| Residence | Rural | 1 | 1 | 1 | 1 |
| Urban | 1.16(0.63,2.14) | 0.86(0.39,2.71) | 1.59(0.79,3.17) | 1.08(0.56,2.06) | |
| Co-morbidity | Yes | 1 | 1 | 1 | 1 |
| No | 1.59(0.89,2.84) | 2.41(1.04,5.55* | 0.96(0.49,1.85) | 1.52(0.82,2.83) | |
| Involving in social activities | Yes | 1 | 1 | 1 | 1 |
| No | 0.80(0.42,1.53) | 1.04(0.47,2.31) | 0.63(0.30,1.31) | 0.93(0.46,1.88) | |
| Regular physical activity | Yes | 1 | 1 | 1 | 1 |
| No | 0.70(0.38,1.27) | 0.65(0.29,1.43) | 0.75(0.38,1.49) | 0.79(0.41,1.51) | |
| Attending health related seminar | Yes | 1 | 1 | 1 | 1 |
| No | 0.61(0.32,1.17) | 0.89(0.42,1.88) | 0.35(0.17,0.72)** | 0.57(0.29,1.11) | |
| Social connectedness | Yes | 1 | 1 | 1 | 1 |
| No | 0.80(0.33,1.94) | 0.16(0.02,1.34) | 2.04(0.75,5.54) | 0.40(0.14,1.12) |
Domain6, Ability to actively engage with healthcare providers; Domain7, Navigating the healthcare system; Domain8, Ability to find good health information; Domain9, Understand health information well enough to know what to do.
# AOR: Adjusted Odds Ratio,
* significantly associated at <0.05,
** significantly associated at <0.01,
1-Reference category
Co-morbidity status and social connectedness were also associated with specific health literacy domains. Respondents with no co-morbidities were 2.41 (95%CI: 1.05, 5.52) times more likely to have higher HL for ‘Navigating the healthcare system’. Compared with the respondents having social connectedness, those without social connection had 0.35 (95% CI: 0.15, 0.82) times lower HL for ‘Actively managing own health’ and 0.38 (95% CI: 0.15, 0.93) times lower HL for ‘Appraisal of health information’.
Compared to respondents who had attended a health-related seminar, respondents who had not participated had 0.36 (95%CI: 0.18, 0.72) times lower HL for ‘Having sufficient information to manage their health’, 0.43 (95%CI: 0.22, 0.84) times lower HL for ‘Social support for health’, and 0.36 (95%CI: 0.17, 0.73) times lower HL for ‘Ability to find good information’, as represented in Tables 3 and 4.
Discussion
This study assessed the HLL and uncovered key factors linked to varying levels of HL among patients with NCD visiting the tertiary level of health care in Nepal. Our study identified that the patients with NCDs had more than half of high HLL for all the domains of HLQ except the domain ‘Navigating the healthcare system’. The major findings revealed that educational attainment, regular physical activity, participation in health-related seminars, and a strong sense of social connectedness emerged as positive contributors to higher HLL across various domains. Conversely, comorbidities exhibited a negative association with HL, underscoring the intricate interplay between personal factors and HL outcomes.
Our study identified that the patients with NCDs scored high HLL for all the domains of HLQ except the domain ‘Navigating the healthcare system’. These findings reflected that they excel in understanding health information, establishing trust with healthcare providers, ensuring understanding and making informed decisions. They are skilled at identifying reliable information and can resolve any conflicting information [17]. The scores for each domain provide a clear picture of where individuals with NCDs may need help, making it easier to identify areas where support can be offered. These insights contribute to the comprehension and application of health information, thereby promoting practices that lead to good health [19]. The lower HL score for ‘Navigating the healthcare system’ might suggest that the individuals face challenges in advocating for themselves and struggle to navigate the healthcare system to address their health needs [17].
There is constant evidence of a relationship between educational status and HL [15, 21–24]. This study identified that the educational status of the study participant is significantly associated with all the domains of HLQ except domains ‘Actively managing own health’, ‘Appraisal of health information’ and ‘Navigating the healthcare system’. Our study reported higher odds of HLL among individuals with higher educational levels for domains ‘Actively engaging with healthcare provider’ and ‘Understanding health information’, consistent with the findings from the studies in Ethiopia [19] and Denmark [25] conducted among patients with chronic disease. This implies that the respondents with higher educational attainment had higher abilities to assess and evaluate health systems and information. They have a higher level of trust, better communication and shared treatment decisions with health service providers [26]. They tend to be more informed about health-related hazards and prevention programs, improving their overall HL [27]. In contrast, respondents with lower educational attainment were likely to engage in unhealthy behaviours [24] and had delayed access to healthcare services, leading to poorer health outcomes [28].
The respondents above the age of 65 years were 67% less likely to have high HLL as compared with the respondents below 45 years for the domain ‘Feeling understood and supported by healthcare providers’, which is consistent with the findings of the study in Europe [15], and in remote Australia which revealed HLL was strongly associated with all the domains of HLQ for respondents less than 55 years [8]. The possible explanation could be age-related cognitive changes brought on by ageing and the increasing prevalence of sensory abnormalities, making it harder for older persons to communicate effectively with healthcare personnel [29]. The other possible explanation might be the dependence of older patients on their younger family members to seek health advice and services from healthcare providers. This could limit the direct communication between older patients with NCDs and health care providers.
The majority of the respondents in our study had limited HLL for ‘Navigating the healthcare system’, which is consistent with the study conducted in Australia among individuals with chronic health conditions [30]. This reflects the complex healthcare system, poorer user-friendly information, and poorer skills of the patients to interact and negotiate with health organisations and health professionals in shared decision-making [31, 32]. Mobilising the patient navigators to support patients in finding their way through the health and social care system could be the strategy to address this problem [33]. Our study revealed that respondents with no comorbidity had higher odds of HLL than those with comorbidity for ‘Navigating the healthcare system’. This indicates people facing multiple health issues struggle with healthcare access due to communication problems, complex needs, and system issues [32]. Comorbid patients, often more dependent than non-comorbid individuals, face logistical and financial burdens that impede the caregiver and patient’s ability to interact appropriately with the healthcare system [34]. These obstacles could make it harder for them to comprehend and utilise health-related information, leading to a lower HL [35]. These further necessitate a more accessible system that supports patients in making health decisions.
The respondents who were not involved in regular physical activities were 55% less likely to have a higher HLL than those engaged in regular physical activities for the domain ‘Feeling understood and supported by healthcare provider’. This is in line with the findings from a similar study, which indicated that the respondents with regular physical activity had higher HLL [36]. The respondents involved in regular physical activities understand disease prevention and the health system [37]. They adopt healthy behaviours that could improve cognitive functioning and decrease the rate of cognitive decline [29], enabling them to understand and explore health-related information.
In our study, the respondents who had not attended health-related seminars were less likely to have higher HLL than those who had participated in health seminars. Those respondents who had not attended health seminars were 64% less likely to have a higher HLL for the domain ‘Having sufficient information to manage my health’, 57% less likely to have a higher HLL for the domain ‘Actively managing own health’ and 65% less likely to have higher HLL for domain ’Ability to find good health information’, respectively. This implies that the individuals participating in health seminars and conferences share new scientific information with doctors, talk about their experiences, and become more involved in their care [38]. This helps to improve their HL and leads to better health results. Such activities should be promoted to uplift the HL of patients with NCDs.
The individuals without social connection were 65% less likely to have a high HLL for the domain ‘Actively managing own health’ and 63% less likely to have a high HLL for the domain ‘Appraisal of health information’. This indicates that limited social connections correlate with reduced information sharing and community engagement, negatively impacting HL, which is concordant with studies conducted in the USA and China [39, 40]. The respondents with high social life and connections frequently interacted with other people and health organisations; they exchanged their thoughts and experiences, which could expand the HLL [41]. A cross-sectional study conducted by Joy Agner et al. indicates that individuals who name more staff for health assistance tend to rely less on external help for understanding medical information [42]. It shows the mutual benefit of the doctor-patient relationship. The results also offer important knowledge on HLL that healthcare professionals and patients can utilise to improve their ability to understand and work together in healthcare management.
Strength and limitation
To our knowledge, this study is the first among patients with NCDs in Nepal using HLQ. Additionally, this study was conducted among follow-up patients with NCDs visiting a health facility, making it difficult to generalise for general people. However, it was broadly representative nationwide as it was conducted in a pioneering government hospital and higher referral centre. As the purposive sampling technique and face-to-face interview through structured questionnaire were applied, respondent and selection bias were possible. We tried to reduce this by using standard and validated tools and techniques.
Implication of study
Several key implications emerged based on our study on HL among Nepalese patients with NCDs. Given the significant influence of educational attainment, targeted interventions should enhance educational experiences to bolster HL. Addressing the notably lower scores in ‘Navigating the healthcare system’ suggests the introduction of patient navigators or similar roles to guide patients effectively. Additionally, age-specific interventions are crucial, given the challenges older individuals face in healthcare interactions. Integrated care models for patients with multiple comorbidities can improve their HL and outcomes, which can be tested in future studies. Promoting physical activity and advancing social connections through community engagement initiatives are vital to enhancing HLLs. Overall, collaborative efforts among healthcare providers, policymakers, and educators are essential to develop evidence-based strategies, ensuring improved HL and outcomes for patients with NCDs in Nepal.
Conclusions
This study reveals that patients with NCDs exhibit varying HLL across different domains of the HLQ. Factors such as higher education, physical activity, attendance at health-related seminars, and social connectedness correlate positively with HLL, while comorbidity is negatively associated. Despite limitations due to its cross-sectional and exploratory nature, the findings emphasise the need for exploring a comprehensive approach to addressing health literacy, particularly in high-risk populations. Transforming health institutions into health literacy-friendly environments by implementing the feedback system of patients towards the healthcare provider and health system is crucial, and this approach needs to be tested in future studies.
Supporting information
(ZIP)
Acknowledgments
We thank Global Health & Equity, Swinburne University of Technology, for providing access to the HLQ. We would like to acknowledge all the enumerators, patients and staff of TUTH for their cooperation during the data collection process.
Abbreviations
- COVID-19
Corona Virus Disease of 2019
- CVD
Cardiovascular Disease
- HL
Health Literacy
- HLL
Health Literacy Level
- HLQ
Health Literacy Questionnaire
- LMIC
Low-and Middle-Income Countries
- NCDs
Non-communicable diseases
- SDG
Sustainable Development Goal
- TUTH
Tribhuvan University Teaching Hospital
Data Availability
All relevant data are within the manuscript and its Supporting information files. Data set are provided in supplementary files.
Funding Statement
The author(s) received no specific funding for this work.
References
- 1.The Global Health Observatory [Internet]. https://www.who.int/data/gho/data/themes/noncommunicable-diseases
- 2.World Health Organization. COVID-19 and NCDs. World Heal Organ [Internet]. 2020;5. https://www.who.int/docs/default-source/ncds/ncd-covid-19/for-web—rapid-assessment—29-may-2020-(cleared).pdf?sfvrsn=6296324c_14&download=true
- 3.World Health Organization. The impact of the COVID-19 pandemic on noncommunicable disease resources and services: results of a rapid assessment. World Health Organization. 2020. 1–32 p. [Google Scholar]
- 4.Nutbeam D, Kickbusch I. Health promotion glossary. Health Promot Int. 1998;13(4):349–64. [Google Scholar]
- 5.Amoah PA, Phillips DR. Health literacy and health: rethinking the strategies for universal health coverage in Ghana. Public Health [Internet]. 2018;159:40–9. doi: 10.1016/j.puhe.2018.03.002 [DOI] [PubMed] [Google Scholar]
- 6.Assessment N. The Health Literacy of America’s Adults Results From the 2003 National Assessment. 2006;
- 7.Geneva: World Health Organization. WHO Global Coordination Mechanism on the Prevention and Control of NonCommunicable Diseases. WHO Publ [Internet]. 2018;1–120. http://creativecomons.org/licenses/by-nc-sa/3.0/igo [Google Scholar]
- 8.Rheault H, Coyer F, Jones L, Bonner A. Health literacy in Indigenous people with chronic disease living in remote Australia. BMC Health Serv Res. 2019;19(1):1–10. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Cabellos-García AC, Castro-Sánchez E, Martínez-Sabater A, Díaz-Herrera MÁ, Ocaña-Ortiz A, Juárez-Vela R, et al. Relationship between determinants of health, equity, and dimensions of health literacy in patients with cardiovascular disease. Int J Environ Res Public Health. 2020;17(6). doi: 10.3390/ijerph17062082 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Berkman ND, Sheridan SL, Donahue KE, Halpern DJ, Crotty K. Low health literacy and health outcomes: An updated systematic review. Ann Intern Med. 2011;155(2):97–107. doi: 10.7326/0003-4819-155-2-201107190-00005 [DOI] [PubMed] [Google Scholar]
- 11.Mitchell SE, Sadikova E, Jack BW, Paasche-Orlow MK. Health literacy and 30-day postdischarge hospital utilization. J Health Commun. 2012;17(SUPPL. 3):325–38. doi: 10.1080/10810730.2012.715233 [DOI] [PubMed] [Google Scholar]
- 12.Shrestha A, Singh SB, Khanal VK, Bhattarai S, Maskey R, Pokharel PK. Health Literacy and Knowledge of Chronic Diseases in Nepal. HLRP Heal Lit Res Pract. 2018;2(4):221–30. doi: 10.3928/24748307-20181025-01 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Bhusal S, Paudel R, Gaihre M, Paudel K, Adhikari TB, Pradhan PMS. Health literacy and associated factors among undergraduates: A university-based cross-sectional study in Nepal. PLOS Glob Public Heal [Internet]. 2021;1(11):e0000016. doi: 10.1371/journal.pgph.0000016 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.LA Fauci V, Trimarchi G, Ceccio C, Mazzitelli F, Pappalardo R, Alessi V. Health literacy in Mediterranean general population. J Prev Med Hyg. 2022;63(4):E527–32. doi: 10.15167/2421-4248/jpmh2022.63.4.2485 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Sørensen K, Pelikan JM, Röthlin F, Ganahl K, Slonska Z, Doyle G, et al. Health literacy in Europe: Comparative results of the European health literacy survey (HLS-EU). Eur J Public Health. 2015;25(6):1053–8. doi: 10.1093/eurpub/ckv043 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Rathnakar UP, Belman M, Kamath A, Unnikrishnan B, K AS, Udupa AL. Evaluation of Health Literacy Status Among Patients in a Tertiary Care Hospital in Coastal Karnataka, India. 2013;2551–4. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Osborne RH, Batterham RW, Elsworth GR, Hawkins M, Buchbinder R. The grounded psychometric development and initial validation of the Health Literacy Questionnaire (HLQ). BMC Public Health [Internet]. 2013;13(1):1. BMC Public Health doi: 10.1186/1471-2458-13-658 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Budhathoki SS, Hawkins M, Elsworth G, Fahey MT, Thapa J, Karki S, et al. Use of the English Health Literacy Questionnaire (HLQ) with Health Science University Students in Nepal: A Validity Testing Study. Int J Environ Res Public Health. 2022;19(6):1–14. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Tilahun D, Abera A, Nemera G. Communicative health literacy in patients with non-communicable diseases in Ethiopia: a cross-sectional study. Trop Med Health. 2021;49(1). doi: 10.1186/s41182-021-00345-9 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Batterham RW, Hawkins M, Collins PA, Buchbinder R, Osborne RH. Health literacy: Applying current concepts to improve health services and reduce health inequalities. Public Health [Internet]. 2016;132(2016):3–12. 10.1016/j.puhe.2016.01.001 [DOI] [PubMed] [Google Scholar]
- 21.Tiller D, Herzog B, Kluttig A, Haerting J. Health literacy in an urban elderly East-German population—Results from the population-based CARLA study. BMC Public Health. 2015;15(1):1–9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Levin-Zamir D, Baron-Epel OB, Cohen V, Elhayany A. The Association of Health Literacy with Health Behavior, Socioeconomic Indicators, and Self-Assessed Health From a National Adult Survey in Israel. J Health Commun [Internet]. 2016;21(00):61–8. 10.1080/10810730.2016.1207115 [DOI] [PubMed] [Google Scholar]
- 23.Liu L, Qian X, Chen Z, He T. Health literacy and its effect on chronic disease prevention: Evidence from China’s data. BMC Public Health. 2020;20(1):1–14. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.Haghdoost AA, Karamouzian M, Jamshidi E, Sharifi H, Rakhshani F, Mashayekhi N, et al. Health literacy among Iranian adults: Findings from a nationwide population-based survey in 2015. East Mediterr Heal J. 2019;25(11):828–36. doi: 10.26719/emhj.19.017 [DOI] [PubMed] [Google Scholar]
- 25.Friis K, Lasgaard M, Osborne RH, Maindal HT. Gaps in understanding health and engagement with healthcare providers across common long-term conditions: A population survey of health literacy in 29 473 Danish citizens. BMJ Open. 2016;6(1):1–10. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26.Zimmerman E, Woolf SH. Understanding the Relationship Between Education and Health. NAM Perspect. 2014;4(6). [Google Scholar]
- 27.Pampel FC, Krueger PM, Denney JT. Socioeconomic disparities in health behaviors. Annu Rev Sociol. 2010;36:349–70. doi: 10.1146/annurev.soc.012809.102529 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28.Yadav UN, Lloyd J, Hosseinzadeh H, Baral KP, Bhatta N, Harris MF. Levels and determinants of health literacy and patient activation among multi-morbid COPD people in rural Nepal: Findings from a crosssectional study. PLoS One [Internet]. 2020;15(5):1–16. 10.1371/journal.pone.0233488 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29.Murman DL. The Impact of Age on Cognition. Semin Hear. 2015;36(3):111–21. doi: 10.1055/s-0035-1555115 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 30.Beauchamp A, Buchbinder R, Dodson S, Batterham RW, Elsworth GR, McPhee C, et al. Distribution of health literacy strengths and weaknesses across socio-demographic groups: A cross-sectional survey using the Health Literacy Questionnaire (HLQ). BMC Public Health [Internet]. 2015;15(1). 10.1186/s12889-015-2056-z [DOI] [PMC free article] [PubMed] [Google Scholar]
- 31.Griese L, Berens EM, Nowak P, Pelikan JM, Schaeffer D. Challenges in navigating the health care system: Development of an instrument measuring navigation health literacy. Int J Environ Res Public Health. 2020;17(16):1–17. doi: 10.3390/ijerph17165731 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 32.Osborne RH, Elsworth GR, Whitfield K. The Health Education Impact Questionnaire (heiQ): An outcomes and evaluation measure for patient education and self-management interventions for people with chronic conditions. Patient Educ Couns. 2007;66(2):192–201. doi: 10.1016/j.pec.2006.12.002 [DOI] [PubMed] [Google Scholar]
- 33.Manderson B, McMurray J, Piraino E, Stolee P. Navigation roles support chronically ill older adults through healthcare transitions: A systematic review of the literature. Heal Soc Care Community. 2012;20(2):113–27. doi: 10.1111/j.1365-2524.2011.01032.x [DOI] [PubMed] [Google Scholar]
- 34.Jones SMW, Chennupati S, Nguyen T, Fedorenko C, Ramsey SD. Comorbidity is associated with higher risk of financial burden in Medicare beneficiaries with cancer but not heart disease or diabetes. Med (United States). 2019;98(1):E14004. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 35.Garcia-Codina O, Juvinyà-Canal D, Amil-Bujan P, Bertran-Noguer C, González-Mestre MA, Masachs-Fatjo E, et al. Determinants of health literacy in the general population: Results of the Catalan health survey. BMC Public Health. 2019;19(1):1–12. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 36.Sharifirad G, Reisi M, Javadzade S, Heydarabadi A, Mostafavi F, Tavassoli E. The relationship between functional health literacy and health promoting behaviors among older adults. J Educ Health Promot. 2014;3(1):119. doi: 10.4103/2277-9531.145925 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 37.Olisarova V, Kaas J, Staskova V, Bartlova S, Papp K, Nagorska M, et al. Health literacy and behavioral health factors in adults. Public Health [Internet]. 2021;190:75–81. doi: 10.1016/j.puhe.2020.11.011 [DOI] [PubMed] [Google Scholar]
- 38.Greene J, Hibbard JH, Tusler M. How Much Do Health Literacy and Patient Activation Contribute to Older Adults’ Ability to Manage Their Health? AARP Public Policy Inst. 2005;(June). [Google Scholar]
- 39.Steinman L, Parrish A, Mayotte C, Bravo Acevedo P, Torres E, Markova M, et al. Increasing Social Connectedness for Underserved Older Adults Living With Depression: A Pre-Post Evaluation of PEARLS. Am J Geriatr Psychiatry. 2021;29(8):828–42. doi: 10.1016/j.jagp.2020.10.005 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 40.Chai X. How Has the Nationwide Public Health Emergency of the COVID-19 Pandemic Affected Older Chinese Adults’ Health Literacy, Health Behaviors and Practices, and Social Connectedness? Qualitative Evidence From Urban China. Front Public Heal. 2022;9(March):1–12. doi: 10.3389/fpubh.2021.774675 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 41.Van Hoa H, Giang HT, Vu PT, Van Tuyen D, Khue PM. Factors Associated with Health Literacy among the Elderly People in Vietnam. Biomed Res Int. 2020;2020. doi: 10.1155/2020/3490635 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 42.Agner J, Meyer M, Kaukau TM, Liu M, Nakamura L, Botero A, et al. Health Literacy, Social Networks, and Health Outcomes among Mental Health Clubhouse Members in Hawai‘i. Int J Environ Res Public Health. 2023;20(1):1–17. doi: 10.3390/ijerph20010837 [DOI] [PMC free article] [PubMed] [Google Scholar]