

Abstract
BACKGROUND:
COVID-19 screening testing (ST) can detect asymptomatic or pre-symptomatic cases, allowing for prompt identification of cases and close contacts. This study examined parents’ and school staffs’ knowledge and attitudes toward to a pilot school-based ST program in a school district in southern Arizona.
METHODS:
In May 2021, online surveys to parents and school staff were administered to examine attitudes toward ST and impacts of the COVID-19 pandemic. Unweighted percent estimates were calculated, and bivariate differences were examined by demographics. Associations were assessed using chi-square tests and logistic regression.
RESULTS:
The survey had response rates of 10% (606/6085) and 22% (187/849) among parents and staff, respectively. Approximately one-third of responding parents (35%) would or already allow their child to participate in school-based ST, 37% would not participate; 28% were unsure. Among responding staff, 46% would or already participate in ST, 33% would not; 21% were unsure. The top concern (38%) among responding staff was taking job-related leave if testing positive.
CONCLUSION:
Schools work to balance the needs of students, families, and staff by implementing supportive and flexible policies and practices founded on buy-in and acceptance from their communities
Keywords: screening testing, COVID-19, K-12 schools, teacher concerns, parent concerns, SARS-CoV-2 transmission
The impact of the COVID-19 pandemic on school communities has been staggering, marked by unprecedented levels of closures and the need for hybrid or virtual learning to prevent and reduce transmission of SARS-CoV-2 in school settings.1 To keep students, teachers, and staff safe during the 2020–2021 academic year, school communities sought to prioritize in-person learning while adopting multiple layered COVID-19 mitigation strategies.
Testing became a key strategy for identifying individuals who may spread SARS-CoV-2 in school settings with test options (post exposure testing, screening testing [ST]), test type (antigen detection verses viral detection), and cadence. ST is used to identify pre-symptomatic or asymptomatic cases of COVID-19 who have no known or suspected exposure to SARS-CoV-2.2 Cadence for ST may vary with schools offering it to students and staff once a week, twice a week or every other week depending on the program.3
Implementing ST in schools can present a variety of challenges. Access can be particularly problematic, especially when COVID-19 community levels are high and testing efforts are prioritized to symptomatic individuals. Unlike in institutions of higher education that can utilize their own laboratory spaces for testing, K-12 schools often rely on public health or private laboratories for testing.4 Additionally, some K-12 schools may lack necessary resources (eg, human, financial) to implement and sustain school-based programs. Long lag time from specimen collection to test result can exacerbate socioeconomic and health inequities, particularly when delayed results may equate to longer quarantine periods for close contacts of those who test positive, reduction in in-person learning, or delayed access to health care as a result of COVID-19.4 Other social factors may also play an important role in implementing school-based ST, namely, lack of willingness to participate, social stigma, and fear of learning about a positive test result.5 Despite these challenges, implementing and evaluating ST programs is needed to continue understanding the impacts of COVID-19 on student and staff health and school operations. Limited evidence from school ST programs currently exists; this study contributes findings from the first pilot site for a national district-wide school-based ST program.
From April 19 to May 21, 2021, a school district in Pima County, Arizona (AZ) served as the pilot site for the ST program. The criteria for selection as a pilot site was a school district being located in a county with a high social vulnerability index (SVI) score (based on socioeconomic status, racial/ethnic minority status, household characteristics, and housing type/transportation),6 pandemic vulnerability, and high prevalence childhood poverty. Additionally, the pilot school district site must have demonstrated readiness and willingness to accept, support, and initiate the ST program within a month’s time. The US Centers for Disease Control and Prevention (CDC) and Pima County Health Department collaborated to conduct a formative pilot evaluation of the AZ school district’s ST program to assess feasibility and acceptability prior to and during implementation. To assess acceptability of ST among the school community, this study examines data from online surveys administered to parents and school staff aimed at understanding their knowledge, attitudes and beliefs, and concerns regarding ST as a COVID-19 prevention strategy in schools.
METHODS
Participants
The pilot school district had 10 schools, including a digital-only school, serving over 5800 students, and employing approximately 850 staff (including administrative, teaching, and support staff). During the 2020–2021 academic year, the pilot school district offered both virtual and in-person learning options. Optional ST was offered to all students in any grades kindergarten through 12 and all staff at no cost (free) beginning on April 19, 2021, except for students and staff participating in in-school athletic programs who were required to be screened for COVID-19 for participation per district requirements. ST was conducted at each school site once a week during school hours by a contracted external testing vendor. Sample collection was via self or clinician collected nasal swab and was processed for reverse transcription-polymerase chain reaction (RT-PCR) testing for detection of SARS-CoV-2 virus.
Instrumentation
Two online SurveyMonkey surveys were created by our project team and distributed using secure links, one for parents/guardians (hereafter called parents) of enrolled students (in any grades kindergarten-12) and one for school district staff. The surveys included items about the impact of the COVID-19 pandemic on children and families; attitudes and concerns toward school-based ST; and demographic characteristics of respondents. In addition, school district staff were asked about impacts of the COVID-19 pandemic on their workload. Dichotomized responses (yes/no) were used to measure parent and staff concerns about ST (see Data S1). Paper-based surveys for parents and school staff were also made available at each school and in English and Spanish languages.
Procedure
District administrative staff sent online survey links to 849 school staff and 8065 parent email accounts from a listserv. The period for voluntary and anonymous survey participation was from May 10–21, 2021, and consent was required. The estimated time to complete the surveys was about 8–10 minutes. Of note, 1 day after the survey’s launch, a local radio show host obtained access to the parent survey link and distributed it to listeners, potentially compromising the pool of individuals with access to the questionnaire. Consequently, the original parent survey link was closed May 11, 2021, and a new link was generated and launched again via parent email listserv on May 14, 2021. Parent survey responses submitted post radio show air date and before the new survey link was provided were removed from analysis (n = 39). Additionally, respondents who did not answer the screener question related to participation in school-based ST were removed from analysis (n = 85). This activity was reviewed by CDC and was conducted consistent with applicable federal law and CDC policy (see 45 C.F.R. part 46.102(l) (2), 21 C.F.R. part 56; 42 U.S.C. §241(d); 5 U.S.C. §552a; 44 U.S.C. §3501 et seq.).
Data Analysis
All analyses were conducted in SAS (v 9.4, Cary N.C.) and were unweighted. Stratified analyses by sex, age, race/ethnicity, education, household income, school athletics participation, and COVID-19 information source were conducted to assess differences in acceptance, knowledge, concerns, and beliefs about ST. Statistical associations were determined using the chi-square test for comparisons with multiple outcomes, specifically ST participation and primary information source (Figure 1). Unadjusted logistic regression analyses were conducted for comparisons with bivariate outcomes, including concerns with ST participation by demographics (Table 2). Odds ratios (ORs) with 95% confidence intervals (CIs) were calculated to compare concerns with ST by parent and school staff respondents’ willingness to participate (Table 3).
Figure 1.
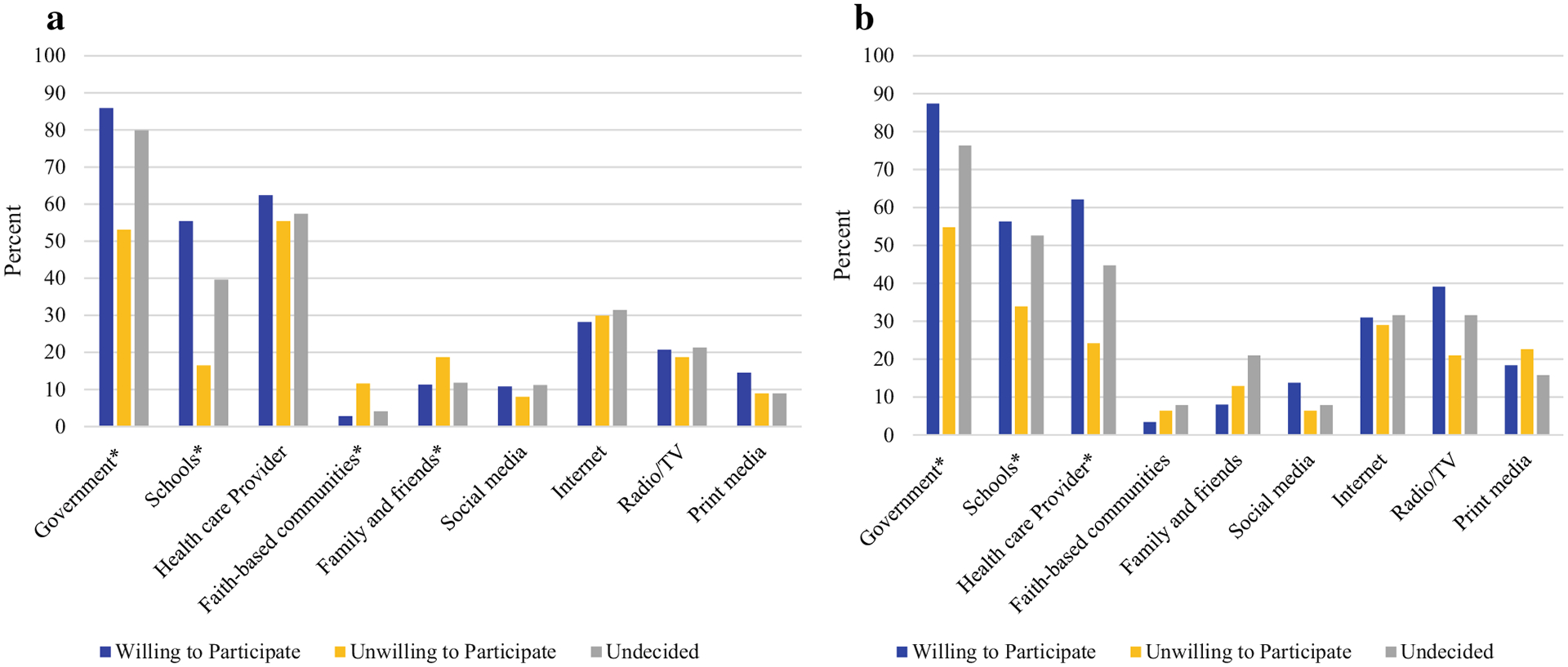
(a) Parent Respondents’ Willingness and (b) School District Staff Respondents’ Willingness to Participate in Screening Testing, by Reported COVID-19 Information Sources, Pima County Arizona—May 2021
*Significant differences between information source determined using chi-square test, confidence level set at p < .05.
Table 2.
Concerns Among (a) Parent Respondents About Their Child’s Participation and (b) School District Staff* Respondents About Participation in School-Based COVID-19 Screening Testing, Pima County Arizona,May 2021
| (a) | My Child’s Privacy | Do Not Want My Child to be Tested for COVID-19 if They Do Not Feel Sick | Believe Test is Uncomfortable or Harmful (May Cause Injury) to My Child | Screening Testing Will be Disruptive and Take Away Learning Time From My Child | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| N (%) | OR (95% Cl) | p-value | N (%) | OR (95% Cl) | p-value | N (%) | OR (95% Cl) | p-value | N (%) | OR (95% Cl) | p-value | |
| Total (n = 606) | 188 (31.0) | 259 (42.7) | 138 (22.8) | 189 (31.2) | ||||||||
| Sex | ||||||||||||
| Male | 56 (31.1) | 2.2 (1.5–3.3) | 0.0001 | 68 (27.4) | 1.9 (1.3–2.8) | 0.002 | 31 (23.7) | 1.2 (0.75–1.9) | 0.447 | 54 (30.2) | 2.1 (1.4–3.1) | 0.0005 |
| Female | 124 (68.9) | Ref | Ref | 180 (72.6) | Ref | Ref | 100 (76.3) | Ref | Ref | 125 (69.8) | Ref | Ref |
| Race/Ethnicity | ||||||||||||
| Non-white, non-Hispanic† | 22 (12.1) | 1.5 (0.85–2.8) | 0.16 | 27 (10.8) | 1.2 (0.70–2.2) | 0.42 | 13 (9.8) | 1.1 (0.57–2.2) | 1.0 | 17 (9.5) | 0.82 (0.44–1.5) | 0.94 |
| Hispanic | 70 (38.7) | 1.04 (0.71–1.5) | 0.4 | 96 (38.2) | 0.96 (0.68–1.4) | 0.463 | 57 (42.9) | 1.2 (0.82–1.9) | 0.5 | 58 (32.4) | 0.64 (0.43–0.93) | 0.11 |
| Non-Hispanic white | 89 (49.2) | Ref | Ref | 128 (51.0) | Ref | Ref | 63 (47.4) | Ref | Ref | 104 (58.1) | Ref | Ref |
| Child grade level | ||||||||||||
| K-5 | 84 (44.9) | 1.3 (0.89–2.0) | 0.557 | 123 (47.7) | 1.4 (1.0–2.1) | 0.033 | 82 (60.3) | 2.8 (1.7–4.5) | <0.0001 | 85 (45.4) | 1.2 (0.8–1.7) | 0.343 |
| 6–8 | 47 (25.1) | 1.4 (0.90–2.3) | 0.3 | 54 (20.9) | 1.0 (0.66–1.6) | 0.43 | 24 (17.6) | 1.3 (0.70–2.3) | 0.28 | 40 (21.4) | 0.98 (0.61–1.6) | 0.63 |
| 9–12 | 56 (30.0) | Ref | Ref | 81 (31.4) | Ref | Ref | 30 (22.1) | Ref | Ref | 62 (33.2) | Ref | Ref |
| (b) | My Privacy | Do Not Want to be Tested for COVID-19 ifl Do Not Feel Sick | Believe Test Is Uncomfortable or Harmful (May Cause Injury) | Screening Testing Will be Disruptive and Take Away Learning Time | ||||||||
| N (%) | OR (95% Cl) | p-value | N (%) | OR (95% Cl) | p-value | N (%) | OR (95% Cl) | p-value | N (%) | OR (95% Cl) | p-value | |
| Total (n = 187) | 40 (21.4) | 50 (26.7) | 14 (7.5) | 35 (18.7) | ||||||||
| Sex | ||||||||||||
| Male | 7 (17.5) | 1.1 (0.43–2.8) | 0.836 | 11 (22.4) | 1.9 (0.81–4.3) | 0.786 | 3 (21.4) | — | — | 9 (25.7) | 2.1 (0.87–5.1) | 0.355 |
| Female | 32 (80.0) | Ref | Ref | 35 (71.4) | Ref | Ref | 11 (78.6) | Ref | Ref | 25 (71.4) | Ref | Ref |
| Race/Ethnicity | ||||||||||||
| Non-white, non-Elispanict | 4 (10.3) | — | — | 5 (10.6) | 1.3 (0.41–4.0) | 0.607 | 0 (0) | N/A | N/A | 3 (8.8) | — | — |
| Hispanic | 10 (25.6) | 0.92 (0.4–2.1) | 0.716 | 12 (25.5) | 0.92 (0.42–2.0) | 0.632 | 2 (14.3) | — | — | 5 (14.7) | 0.4 (0.14–1.1) | 0.16 |
| Non-Elispanic white | 25 (64.1) | Ref | Ref | 30 (63.8) | Ref | Ref | 12 (85.7) | Ref | Ref | 26 (76.5) | Ref | Ref |
| Grade level taught | ||||||||||||
| K-5 | 18 (45.0) | 1.6 (0.54–4.8) | 0.476 | 16 (32.0) | 0.55 (0.22–1.41) | 0.21 | 3 (21.4) | — | — | 13 (37.1) | 0.59 (0.21–1.6) | 0.71 |
| 6–8 | 10 (25.0) | 2.4 (0.70–8.1) | 0.08 | 8 (16.0) | 0.7 (0.23–2.1) | 0.765 | 3 (21.4) | — | — | 5 (14.3) | 0.53 (0.15–1.8) | 0.595 |
| 9–12 | 5 (12.5) | Ref | Ref | 10 (20.0) | Ref | Ref | 6 (42.9) | Ref | Ref | 8 (22.9) | Ref | Ref |
| Non-teaching staff | 7 (17.5) | 0.8 (0.23–2.8) | 0.146 | 16 (32.0) | 0.91 (0.35–2.4) | 0.533 | 2 (14.3) | — | — | 9 (25.7) | 0.59 (0.2–1.7) | 0.751 |
N, unweighted; OR, odds ratio; CI, confidence interval; ref, referent. Odds ratios suppressed due to insufficient sample size (—).
School district staff included, instructional (ie, teaching), and non-teaching staff (ie, any administrative or support personnel) at the district or school-level.
Non-white non-Hispanic includes all respondents who did not select Hispanic as their ethnicity and selected at least one race category other than white.
Table 3.
Concerns Related to COVID-19 Screening Testing by Participation Status Among Parents of School-Aged Children and School District Staff Respondents, Pima County Arizona, May 2021
| Willing to Participate* | Unwilling to Participate | Undecided† | |||||
|---|---|---|---|---|---|---|---|
| N (%) | N (%) | OR (95% CI) | p-value | N (%) | OR (95% CI) | p-value | |
| Parents | |||||||
| Total | 213 (35.2) | 224 (37.0) | — | — | 169 (27.9) | — | — |
| What will happen if my child tests positive | 29 (13.6) | 36 (16.1) | 1.2 (0.7–2.1) | 0.53 | 25 (14.8) | 1.1 (0.62–2.0) | 0.997 |
| My child’s privacy | 25 (11.7) | 117 (52.2) | 8.2 (5.0–13.5) | <0.0001 | 46 (27.2) | 2.8 (1.6–4.8) | 0.930 |
| Do notwantmychildto betestedfor COVID-19 if they do notfeel sick | 21 (9.9) | 163 (72.8) | 24.4 (14.3–41.8) | <0.0001 | 75 (44.4) | 7.3 (4.2–12.6) | 0.059 |
| Believe test is uncomfortable or harmful (may cause injury) to my child | 18 (8.5) | 77 (34.4) | 5.7 (3.2–9.9) | <0.0001 | 43 (25.4) | 3.7 (2.0–6.7) | 0.052 |
| Screening testing will be disruptive and take away learning time from my child | 16 (7.5) | 121 (54.0) | 14.5 (8.1–25.7) | <0.0001 | 52 (30.8) | 5.5 (3.0–10.0) | 0.100 |
| Childcare needed if my child tests positive for COVID-19 | 11 (5.2) | 10 (4.5) | 0.86 (0.36–2.1) | 0.92 | 6 (3.5) | 0.68 (0.24–1.9) | 0.505 |
| Costs of COVID-19 screening testing | 12 (5.6) | 15 (6.7) | 1.2 (0.55–2.6) | 0.45 | 21 (12.4) | 2.4 (1.1–5.0) | 0.012 |
| School District Staff‡ | |||||||
| Total | 87 (46.5) | 62 (33.2) | — | — | 38 (20.3) | — | — |
| What will happen if I test positive | 33 (37.9) | 11 (17.7) | 0.35 (0.16–0.77) | 0.033 | 11 (28.9) | 0.67 (0.29–1.5) | 0.778 |
| My privacy | 16 (18.4) | 16 (25.8) | 1.5 (0.7–3.4) | 0.355 | 8 (21.0) | 1.2 (0.46–3.1) | 0.913 |
| Do not want tobe tested for COVID-19 if I do not feel sick | 4 (4.6) | 30 (48.4) | — | — | 16 (42.1) | — | — |
| Believe test is uncomfortable or harmful (may cause injury) | 1 (1.1) | 9 (14.5) | — | — | 4 (10.5) | — | — |
| Screening testing will be disruptive and take away learning time | 5 (5.7) | 23 (37.1) | 9.7 (3.4–27.3) | <0.0001 | 7 (18.4) | 3.7 (1.1–12.5) | 0.724 |
| Costs of COVID-19 screening testing | 2 (2.3) | 4 (6.4) | — | — | 1 (2.6) | — | — |
| Do not think screening testing is needed because I am vaccinated | 13 (14.9) | 21 (33.9) | 2.9 (1.3–6.4) | 0.0969 | 12 (31.6) | 2.6 (1.1–6.5) | 0.285 |
N, unweighted; OR, odds ratio; CI, confidence interval. Odds ratios suppressed due to insufficient sample size (—).
Reference group.
Undecided includes respondents who selected either: “I am unsure if I would allow my child to participate in screening testing at school” or “I am interested but need more information.”
School district staff included, instructional (ie, teaching), and non-teaching staff (ie, any administrative or support personnel) at the district or school-level.
RESULTS
Sample
The survey response rates were 10% for parents (606/6085) and 22% (187/849) for staff. In our sample, parent respondents were majority female (78.7%), aged 40 years and older (61.8%), White non-Hispanic (51.2%), with an annual household income over $100,000 (50.6%). School staff respondents were predominantly female (79.1%), aged 40 years and older, (63.5%), White non-Hispanic (63.9%), and had an annual household income between $50,000 and $99,999 (43.5%). Respondents’ demographics varied from individuals living in Pima County, AZ between 2017 and 2021, which included female (50.5%), White non-Hispanic (50.1%), median household income ($59,215), and those having at least a bachelor’s degree (34.4%) (see Data S3).7
Of the parents that completed the survey, 42.6% had at least one child enrolled in grades kindergarten through 5, grades 6–8 (22.7%), and grades 9–12 (34.7%). A large proportion of parent respondents reported they received COVID-19 information from governmental sources (72.1%), their health care providers (58.4%), and the school district (36.6%). A large proportion of staff respondents reported they received COVID-19 information from governmental sources (74.3%), the school district (48.1%), and their health care providers (46.0%) (Table 1). Most school staff respondents reported being instructional (ie, teaching) (72.6%), while fewer (27.4%) were non-instructional.
Table 1.
Demographic Characteristics, COVID-19 Information Source, and Willingness to Participate in a Screening Testing Program Among Parents of School-Age Children and School District Staff Respondents, Pima County Arizona, May 2021
| Parents of School-Age Child, N (%) | School District Staff*, N (%) | |
|---|---|---|
| Total† | 606 | 187 |
| Sex | ||
| Female | 459 (78.7) | 148 (79.1) |
| Male | 124 (21.3) | 30 (16.0) |
| Age | ||
| <40 years | 228 (38.2) | 66 (36.5) |
| 40+ years | 369 (61.8) | 115 (63.5) |
| Race/Ethnicity | ||
| Non-white, non-Hispanic‡ | 56 (9.6) | 16 (8.9) |
| Hispanic | 229 (39.2) | 49 (27.2) |
| White, non-Hispanic | 299 (51.2) | 115 (63.9) |
| Education Level | ||
| High school or less | 49 (8.3) | 1 (0.6) |
| Some college and associate’s | 201 (34.2) | 43 (24.0) |
| Bachelor’s degree | 216 (36.7) | 58 (32.4) |
| Above bachelor’s degree | 122 (20.7) | 77 (43.0) |
| Annual household income | ||
| < $50,000 | 86 (15.4) | 48 (28.2) |
| ≥$50,000-$99,999 | 189 (33.9) | 74 (43.5) |
| ≥$100,000+ | 282 (50.6) | 48 (28.2) |
| Grade level | ||
| Grades K-5 | 257 (42.6) | 74 (39.6) |
| Grades 6–8 | 137 (22.7) | 31 (16.6) |
| Grades 9–12 | 209 (34.7) | 30 (16.0) |
| Non-teaching staff | N/A | 51 (27.4) |
| COVID-19 information source§ | ||
| Government | 437 (72.1) | 139 (74.3) |
| Schools/District | 222 (36.6) | 90 (48.1) |
| Healthcare provider | 354 (58.4) | 86 (46.0) |
| Faith communities | 39 (6.4) | 10 (5.3) |
| Family and friends | 86 (14.2) | 23 (12.3) |
| Social media | 60 (9.9) | 19 (10.2) |
| Internet | 180 (29.7) | 57 (30.5) |
| Radio/TV | 122 (20.1) | 59 (31.5) |
| Print media∥ | 66 (10.9) | 36 (19.2) |
| Screeningtesting participation | ||
| Willing to participate | 213 (35.2) | 87 (46.5) |
| Unwilling to participate | 224 (37.0) | 62 (33.2) |
| Undecided | 169 (27.9) | 38 (20.3) |
N, unweighted.
School district staff included, instructional (ie, teaching), and non-teaching staff (ie, administrative or support personnel) at the district or school-level.
Individual numbers may not add to total denominator if participants declined to respond to a given survey question.
Non-white non-Hispanic includes all respondents who did not select Hispanic as their ethnicity and selected at least one race category other than white.
Respondents were able to select more than one primary COVID-19 information source.
Print media includes newspapers and other physical informational products.
Acceptance of ST
Overall, 35.2% of responding parents reported they would allow their child to participate in school-based ST; whereas 37.0% reported they would not allow their child to participate, and 27.9% were undecided (Table 1). Differences in willingness to participate were also observed by parent respondents’ reported COVID-19 information source including from the government (85.9% of willing to participate compared to53.1% of unwilling, p ≤ .0001; 79.9% undecided to participate compared to53.1% of unwilling, p ≤.0001), and school/district (55.4% of willing to participate compared to 16.5% unwilling, p ≤ .0001; 39.6% undecided compared to16.5% unwilling, p ≤.0001) (see Figure 1a). A similar pattern was observed for faith-based (p = .0003) and family/friends (p = .048) information sources.
Among responding school staff, 46.5% reported they would participate in school-based ST; whereas 33.2% reported they would not, and 20.3% were undecided (Table 1). Responding staff willingness to participate in ST significantly varied by COVID-19 information source including government (87.4% willing to participate compared to 54.8% unwilling p ≤ .0001), school/district (56.3% willing to participate compared to 33.9% of unwilling, p = .021), and health care provider (62.1% willing to participate compared to 24.4% of unwilling, p ≤ .0001) (see Figure 1b).
Concerns About Participation in ST
Overall, primary concerns expressed by parent respondents included having their child tested if they did not feel sick (42.7%), testing causing disruption or taking away learning time (31.2%), child’s privacy (31.0%), uncomfortable/harmful testing (22.8%) (Table 2a), consequences if their child tests positive (14.9%), and cost (7.9%) (Data S2A). Concerns about ST varied significantly by select demographics (Table 2a). As compared to female parent respondents, male parent respondents were 1.9 times more likely to be concerned about their child being tested when they did not feel sick (95% CI 1.3–2.8, p = .002), had 2.1 greater odds of being concerned that testing would cause disruption or take away learning time (95% CI 1.4–3.1, p = .0005), and 2.2 greater odds of concern for their child’s privacy (95% CI 1.5–3.3, p = .0001). Compared to parent respondents of older children (grades 9–12), parent respondents of children in grades kindergarten-5 were more likely to be concerned about their child being tested when they did not feel sick (OR 1.4, 95% CI 1.0–2.1, p = .033) and that ST would be uncomfortable/harmful to their child (OR 2.8, 95% CI 1.7–4.5, p ≤ .0001) (Table 2a). Furthermore, parent respondents with children in grades kindergarten-5 were more likely to be concerned about cost than those of older children (OR 2.1, 95% CI 1.0–4.4, p = .041). Parent respondents with children in grades 6–8 had 2.3 greater odds of being concerned about testing positive than those with older children (grades 9–12) (95% CI 1.2–4.2, p = .026) (Data S2A).
The most prevalent concerns related to ST among school staff respondents were consequences if they test positive (29.4%), testing when they did not feel sick (26.7%), privacy (21.4%), causing disruption or taking away learning time (18.7%), and uncomfortable/harmful (7.5%), and cost (3.7%), (Table 2b, Data S2B). No statistically significant demographic differences in concerns by school staff were observed.
Association Between ST Concerns and Participation
Specific concerns related to ST varied by respondent willingness to participate. Among responding parents, significantly more who were concerned about testing if their child did not feel sick were unwilling to allow participation (72.8%), than those willing to participate (9.9%) (OR 24.4, 95% CI 14.3–41.8, p ≤ .0001). Significantly more responding parents concerned about ST causing disruption or taking away learning time were unwilling to participate in ST (54.0%), compared to 7.5% who were willing to participate (OR 14.5, 95% CI 8.1–25.7, p ≤ .0001). Significantly more responding parents concerned about privacy were unwilling to allow their child to participate in ST, than those allowing participation (52.2% compared to 11.7%, OR 8.2, 95% CI 5.0–13.5, p ≤ .0001). Significantly more parents concerned about testing being uncomfortable/harmful were unwilling to participate in ST (34.4% compared to 8.5%), compared to those willing to participate (OR 5.7, 95% CI 3.2–9.9, p < .0001). Additionally, responding parents concerned about the cost (12.4%) were significantly more likely to be undecided about ST participation, than those who were willing (5.6%) (OR 2.4, 95% CI 1.1–5.0 p = .012) (Table 3).
The greatest concerns among responding staff unwilling to participate in ST were testing if they do not feel sick (48.4%), causing disruption or taking away learning time (37.1%), and privacy (25.8%). Similar patterns of concerns among responding staff undecided about participating in ST emerged, including testing if they do not feel sick (42.1%), consequences if they test positive (28.9%), privacy (21.0%) and causing disruption or taking away learning time (18.4%) (Table 3).
Significantly more staff respondents who were concerned about ST causing disruption or taking away learning time were unwilling to participate than those willing to participate (37.1% compared to 5.7%, OR 9.7, 95% CI 3.4–27.3, p ≤ .0001). Conversely, significantly fewer staff respondents who were concerned about what happens if they test positive were unwilling to participate than those willing to participate (17.7% compared to 37.9%, OR 0.35, 95% CI 0.16–0.77, p = .03) (Table 3).
DISCUSSION
This study presents data from a sample of parents and school staff who participated in a survey about their knowledge, attitudes, and beliefs toward school-based COVID-19 ST during a pilot study program in one Arizona school district. Results suggest more acceptance for ST among school district staff respondents compared to parent respondents in the sample. Almost half of school staff respondents reported they would or currently participate in ST, while only slightly over one-third of parent respondents said they would or currently allow their child to participate in ST. Notably, both parents and school staff respondents with or serving children in grades kindergarten-5 had greater concerns than adults with or those serving older children and teens. Results may suggest a greater challenge to participation or unique age-specific factors related to ST implementation with younger children in our sample. For example, parent and teacher respondent concerns about disruptions to child’s learning may contribute to attitudes and support for school-based ST.5
Though the risk of transmission of SARS-CoV-2 in schools has been low relative to community levels (especially when COVID-19 prevention strategies are in place),8 school staff respondents may feel their work environment is safer if regular testing is in place. A survey of former public-school teachers in December 2020 found roughly half of teachers who resigned due to COVID-19-related factors reported they would return to the profession if widespread testing were available.9
Participation concerns varied between parents and school staff respondents, with parent respondents most concerned about having their child tested if they did not feel sick, that ST was disruptive to learning time, and privacy. The epidemiology of the COVID-19 pandemic has continued to show asymptomatic infections, reduced susceptibility, and reduced infectivity in children compared to adults.10–13 Yet, there have been reports of children spreading COVID-19 to members of their household.13–15 Public health messaging to parents, from trusted information sources, can promote clarifying language communicating that reduced risk of transmission and disease severity in children does not equal no risk, and early detection of SARS-CoV-2 in all age groups can mitigate unwanted outcomes including loss of in-person learning due to quarantine, school closures, and disease spread.16 Staff training regarding disease transmission within school settings can be important to ensuring program integrity and effective implementation, specifically trainings covering consent, reporting systems, specimen collection protocols, and health data storage and management.13,17
Significant differences were found between respondents willing and unwilling to participate in ST among both parents and staff, especially, regarding asymptomatic testing, disruptive learning, privacy, and perceived test discomfort/harm. Concerns about ST being disruptive to learning time may be remedied by scheduling specimen collection during non-instructional work time. A potential strategy to mitigate concerns about the discomfort or harm caused by testing could be to utilize a less invasive approach such as saliva specimen collection which may be more acceptable compared to nasopharyngeal swabbing.18 Interestingly, parent respondents who were unsure about ST were significantly more likely to be concerned about testing cost. Though school ST has been offered at no-cost,17 parents in our sample, may worry about financial burdens if testing costs and information are not adequately communicated.
In response to public health data illustrating increased COVID-19 transmission among people engaged in close contact sports, many school districts, including the one in this pilot study, required ST of students and staff for participation in school-sponsored athletics when vaccines were not yet widely available.19–22 Due to the importance of testing in this population, buy-in from parents, athletes, and athletic staff is important to ST acceptance and participation.
IMPLICATIONS FOR SCHOOL HEALTH POLICY, PRACTICE, AND EQUITY
Study findings from this pilot may have implications for school district administrators, staff, and parents, public health researchers, and practitioners to consider. Understanding the knowledge and beliefs of the K-12 school community has been shown to be important to the success of school-based ST programs.23 A recent study found one of the biggest challenges to in-school COVID-19 testing was limited engagement with families, students, and staff.23 Many of the concerns among parents and staff who participated in our surveys highlight the importance of pre-implementation outreach and education. Using listening sessions, town halls meetings, and focus groups to address school community concerns and including them as part of decision-making processes remains vital, especially since schools were considered among the top three trusted sources for COVID-19 information among our survey respondents.17
Importantly, this study was conducted when the Alpha variant of SARS-CoV-2 was the dominant strain in circulation. Delta and Omicron variant surges fueled increased necessity for ST in schools given high levels of community transmission. With a shift in the ways schools respond to COVID-19 (ie, more focus on diagnostic testing at school and at-home testing), it is unclear how ST programs will look going forward.
To date, limited information is available on the knowledge and attitudes of the school community regarding COVID-19 school-based ST programs. Our findings contribute diverse perspectives from parent and school staff respondents in one Arizona school district, including child privacy, disruptions to learning, and job-related leave caused by the pandemic; all of which may be useful in decision-making, implementing, and communicating about school-based ST in the future. Key concerns voiced by parent and school staff respondents could be helpful to other school districts in considering how to broaden acceptance for this important COVID-19 prevention strategy while leveraging trust and existing relationships within and outside the school community.
This study has several limitations. Results reflect the self-reported knowledge, attitudes, and beliefs of parents and school staff respondents in one Pima County, AZ school district and are not generalizable beyond this specific population. Low survey response rates for parent (10%) and staff (22%) impacts interpretability of findings and contribute to non-response and self-selection bias. Due to small sub-populations for certain groups used in this analysis (eg, staff willing to participate), some estimates for the size of the associations were unable to be detected at a statistically significant level. Factors such as survey administration during end-of-year events (eg, final examinations, graduation), short data collection period (2 weeks), and the unauthorized distribution of the parent survey link by a local radio host could have impacted response rates.
Conclusions
Broad engagement of the school community while planning and implementing ST may increase acceptance and inform participation among parents and staff.16,22 The evolving health needs of students, staff, and their families and concerns about testing procedures and disruptions to learning may also influence ST participation. Findings supported the need for tailored messaging and education from trusted sources, specifically focused on the purpose and importance of ST in identifying asymptomatic cases that may go undetected. Furthermore, policies that increase support services for students and families and paid leave for staff may incentivize ST participation and acceptability.
Supplementary Material
Data S1. Survey items asked to parent and school district staff respondents and operationalized to assess willingness to participate and screening testing concerns.
Data S2. (A) Concerns among parent respondents about their child’s participation in school-based COVID-19 screening testing, Pima County Arizona, May 2021. (B) Concerns among school district staff1 respondents related to participation in school-based COVID-19 screening testing, Pima County Arizona, May 2021.
Data S3. U.S. Census data for adults in Pima County, Arizona, 2017–2021.
Acknowledgments
We appreciate Ken Komatsu for approving this investigation. Aspecial thanks to the following people for their contributions to this work: Amber Woods, Jeanine Sarnacki, John Neatherlin, Kristin King, Sabrina Madni, January Cornelius, and Increasing Community Access to Testing (ICATT) programpartners.
Footnotes
Human Subjects Approval Statement
This activity was reviewed by the CDC and was conducted consistent with applicable federal law and CDC policy (see, eg, 45 C.F.R. part 46.102(l)(2), 21 C.F.R. part 56; 42 U.S.C. §241(d); 5 U.S.C. §552a; 44 [AQ7] U.S.C. §3501 et seq.).
Disclaimer Statement
The findings and conclusions of this report are those of the authors and do not necessarily represent the official position of the Centers for Disease Control and Prevention.
Conflict of Interest
The authors have no conflicts of interest to disclose.
SUPPORTING INFORMATION
Additional supporting information may be found online in the Supporting Information section at the end of the article.
REFERENCES
- 1.Masonbrink AR, Hurley E. Advocating for children during the COVID-19 school closures. Pediatrics. 2020;146(3):1–4. [DOI] [PubMed] [Google Scholar]
- 2.Centers for Disease Control and Prevention. Testing strategies for SARS-CoV-2. 2021. Available at: https://www.cdc.gov/coronavirus/2019-ncov/lab/resources/sars-cov2-testing-strategies.html. Accessed September 08, 2023.
- 3.Centers for Disease Control and Prevention. What to know about COVID-19 testing in schools. 2022. Available at: https://www.cdc.gov/coronavirus/2019-ncov/community/schools-childcare/what-you-should-know.html. Accessed September 08, 2023.
- 4.Rafiei Y, Mello MM. The missing piece - SARS-CoV-2 testing and school reopening. N Engl J Med. 2020;383(23):e126. [DOI] [PubMed] [Google Scholar]
- 5.Unger JB, Soto D, Lee R, Deva S, Shanker K, Sood N. COVID-19 testing in schools: perspectives of school administrators, teachers, parents, and students in southern California. Health Promot Pract. 2021;24:350–359. 10.1177/15248399211066076. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Agency for Toxic Substances and Disease Registry. CDC/ATSDR’s Social Vulnerability Index (SVI). Available at: https://www.atsdr.cdc.gov/placeandhealth/svi/index.html. Accessed September 07, 2023.
- 7.United States Census Burearu. QuickFacts: Pima County, Arizona. 2021. Available at: https://www.census.gov/quickfacts/pimacountyarizona. Accessed September 08, 2023.
- 8.Doyle T, Kendrick K, Troelstrup T, et al. COVID-19 in primary and secondary school settings during the first semester of school reopening - Florida, August-December 2020. MMWR. 2021;70(12):437–441. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Diliberti MK, Schwartz HL, Grant D. Stress Topped the Reasons Why Public School Teachers Quit, Even Before COVID-19. Santa Monica, CA: RAND Corporation; 2021. Available at: https://www.rand.org/pubs/research&uscore;reports/RRA1121-2.html. Accessed September 08, 2023. [Google Scholar]
- 10.Lee B, Raszka WV Jr. COVID-19 in children: looking forward, not back. Pediatrics. 2021;147(1):1–4. [DOI] [PubMed] [Google Scholar]
- 11.Viner RM, Ward JL, Hudson LD, et al. Systematic review of reviews of symptoms and signs of COVID-19 in children and adolescents. Arch Dis Child. 2020;106:802–807. 10.1136/archdischild-2020-320972. [DOI] [PubMed] [Google Scholar]
- 12.Swanson M, Hast M, Burnett E, et al. Is symptom screening useful for identifying COVID-19 infection in school settings? Georgia, USA. J Sch Nurs. 2021;37(6):503–512. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Grijalva CG, Rolfes MA, Zhu Y, et al. Transmission of SARS-COV-2 infections in households - Tennessee and Wisconsin, April-September 2020. MMWR. 2020;69(44):1631–1634. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Laws RL, Chancey RJ, Rabold EM, et al. Symptoms and transmission of SARS-CoV-2 among children - Utah and Wisconsin, March-May 2020. Pediatrics. 2021;147(1):1–15. 10.1542/peds.2020-027268. [DOI] [PubMed] [Google Scholar]
- 15.Centers for Disease Control and Prevention. Operational guidance for K-12 schools and early care and education programs to support safe in-person learning. 2022. Available at: https://www.cdc.gov/coronavirus/2019-ncov/community/schools-childcare/k-12-guidance.html. Accessed October 04, 2022.
- 16.Faherty L, Master, Steiner E, et al. COVID-19 Testing in K-12 Schools: Insight from Early Adopters. Santa Monica, CA: RAND Corporation; 2021. Available at: https://www.rand.org/pubs/research&uscore;reports/RRA1103-1.html. Accessed October 04, 2022. [Google Scholar]
- 17.Al Suwaidi H, Senok A, Varghese R, et al. Saliva for molecular detection of SARS-CoV-2 in school-age children. Clin Microbiol Infect. 2021;27(9):1330–1335. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Lanier WA, Babitz KD, Collingwood A, et al. COVID-19 testing to sustain in-person instruction and extracurricular activities in high schools - Utah, November 2020-March 2021. MMWR. 2021;70(21):785–791. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Honein MA, Barrios LC, Brooks JT. Data and policy to guide opening schools safely to limit the spread of sars-cov-2 infection. JAMA. 2021;325(9):823–824. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Drogosz M, Pellegren J, Creegan E, et al. Implications of sports on covid-19 cases in Rhode Island school-aged athletes. R I Med J (2013). 2021;104(5):51–54. [PubMed] [Google Scholar]
- 21.Sasser P, McGuine T, Haraldsdottir K, et al. Reported COVID-19 incidence in Wisconsin high school athletes in fall 2020. J Athl Train. 2021;57(1):59–64. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Vohra D, Rowan P, Hotchkiss J, Lim K, Lansdale A, O’Neil S. Implementing COVID-19 Routine Testing in K-12 Schools: Lessons and Recommendations from Pilot Sites. Princeton, NJ: Mathematica; 2021. Available at: https://www.mathematica.org/publications/implementing-covid-19-routine-testing-in-k-12-schools-lessons-and-recommendations-from-pilot-sites. Accessed September 16, 2022. [Google Scholar]
- 23.Haroz EE, Kalb LG, Newland JG, et al. Implementation of school-based COVID-19 testing programs in underserved populations. Pediatrics. 2022;149(12 Suppl 2), S1–S14. [DOI] [PMC free article] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
Data S1. Survey items asked to parent and school district staff respondents and operationalized to assess willingness to participate and screening testing concerns.
Data S2. (A) Concerns among parent respondents about their child’s participation in school-based COVID-19 screening testing, Pima County Arizona, May 2021. (B) Concerns among school district staff1 respondents related to participation in school-based COVID-19 screening testing, Pima County Arizona, May 2021.
Data S3. U.S. Census data for adults in Pima County, Arizona, 2017–2021.