

Greten TF, Abou-Alfa GK, Cheng A, et al. Society for Immunotherapy of Cancer (SITC) clinical practice guideline on immunotherapy for the treatment of hepatocellular carcinoma. J Immunother Cancer 2021;9:e002794. doi: 10.1136/jitc-2021-002794
On October 21, 2022, the United States (US) Food and Drug Administration (FDA) approved tremelimumab in combination with durvalumab for adult patients with unresectable HCC. Approval was based on statistically significant and clinically meaningful improvement in overall survival for tremelimumab plus durvalumab compared to sorafenib in the phase III HIMALAYA trial (NCT03298451), which enrolled patients with confirmed unresectable HCC who had not received prior systemic treatment.
In light of the approval, the ‘Society for Immunotherapy of Cancer (SITC) clinical practice guideline on immunotherapy for the treatment of hepatocellular carcinoma’ has been updated. The following changes have been made to the manuscript. Amendments to the original text are shown in italics and described below in order of the sections in which they appear in the order of the original publication.
Introduction
A sentence has been added to include acknowledgment of the tremelimumab and durvalumab approval:
The updated text now reads: ‘In 2022, the ICI combination of durvalumab (anti-PD-L1) with tremelimumab (anti-CTLA-4) was also approved for the treatment of unresectable HCC. Additional trials are ongoing and the therapeutic landscape continues to evolve and expand.’
Recommended immunotherapies for HCC
The following sentences have been modified to include information on the approval of tremelimumab and durvalumab: ‘For more than 10 years, sorafenib was the only systemic therapy approved by the FDA for the treatment of HCC. Since 2017, four ICI regimens have entered the clinic after having received full or accelerated approval by the FDA for the treatment of advanced HCC. Only one combination, atezolizumab with bevacizumab, had full FDA approval at the time of guideline preparation, the remaining regimens (nivolumab and pembrolizumab monotherapy and nivolumab with ipilimumab) received accelerated approvals, and FDA review of confirmatory trials is ongoing.’
The updated text now reads: ‘For more than 10 years, sorafenib was the only systemic therapy approved by the FDA for the treatment of HCC. In recent years, ICI-based regimens have become standard of care in the first-line setting as well as for the treatment of disease that has progressed on prior sorafenib treatment. As of 2022, two ICI-based combinations, atezolizumab with bevacizumab and tremelimumab with durvalumab, had full FDA approval for first-line treatment of HCC, and pembrolizumab monotherapy as well as nivolumab in combination with ipilimumab had accelerated approvals as second line options.’
The following paragraphs have been inserted immediately prior to the Panel recommendations header to include supporting data for the FDA approval of tremelimumab and durvalumab:
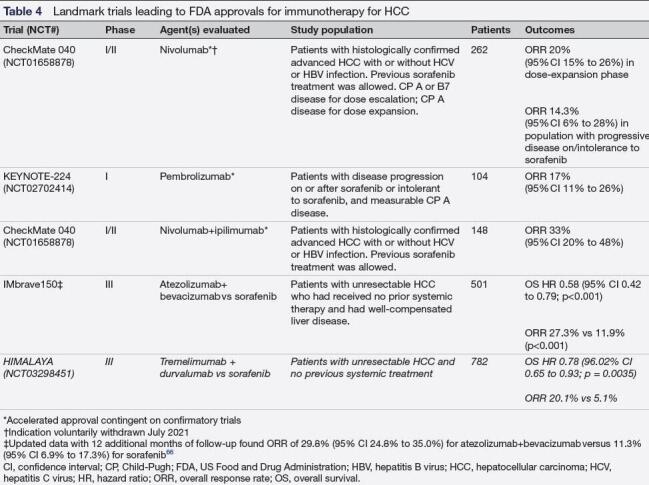
‘The second ICI regimen to receive full approval for the treatment of HCC is tremelimumab in combination with durvalumab for patients with unresectable HCC, which was approved in 2022. Approval was based on the open-label, phase III HIMALAYA trial, in which 1,171 patients were randomly assigned (1:1:1) to receive tremelimumab in combination with durvalumab (n=393), durvalumab (n=389), or sorafenib (n=389). 1 The primary endpoint for this trial was OS. In HIMALAYA, tremelimumab was administered as a one-time single dose plus durvalumab every 4 weeks (single tremelimumab regular interval durvalumab, or STRIDE regimen). Median OS for the tremelimumab in combination with durvalumab arm was 16.43 months (95% CI 14.16 to 19.58), compared with 16.56 months (95% CI 14.06 to 19.12) in the durvalumab arm and 13.77 months (95% CI 12.25 to 16.13) in the sorafenib arm. Superiority was demonstrated for tremelimumab plus durvalumab compared with sorafenib, with an OS HR of 0.78 (96.02% CI 0.65 to 0.93; p=0.0035). Delayed separation of Kaplan-Meier survival curves was observed, and in an analysis of the piece-wise constant treatment effects of tremelimumab in combination with durvalumab versus sorafenib, the HRs before and after the 9 month time points were 0.87 (95% CI 0.68 to 1.11) and 0.70 (95% CI 0.56 to 0.89), respectively. Secondary endpoints included investigator-assessed ORR (table 4) and PFS, which was not significantly different among the three groups.
The study was not powered to assess for efficacy of the durvalumab plus tremelimumab combination compared with durvalumab alone. OS with durvalumab monotherapy was found to be noninferior to sorafenib (HR 0.86 [95.67% CI 0.73 to 1.03]; noninferiority margin 1.08). As of 2023, anti-PD-(L)1 monotherapy in the first-line setting is being used in some cases for patients with advanced HCC considered to be at high risk for complications with dual-ICI therapy. Although evidence of survival benefit for anti-PD-(L)1 monotherapy over sorafenib or lenvatinib in phase III studies is lacking, this monotherapy approach could be an alternative treatment option for these patients.
In HIMALAYA, the median time to deterioration of patient-reported QOL was 7.5 months for tremelimumab in combination with durvalumab, 7.4 months for durvalumab monotherapy, and 5.7 months for sorafenib. Grade 3–4 AEs occurred in 50.5% of patients in the tremelimumab with durvalumab arm, 37.1% in the durvalumab monotherapy arm, and 52.4% in the sorafenib arm. IrAEs requiring high-dose glucocorticoid treatment occurred in 20.1%, 9.5%, and 1.9% across the three treatment arms, respectively. The frequency of hepatic/hemorrhage AEs was similar across all treatment arms. Anti-durvalumab ADAs (positive post-baseline only) were detected in 3.1% and 2.5% of patients receiving tremelimumab plus durvalumab or durvalumab, respectively, and anti-tremelimumab ADAs were detected in 11% of patients in the dual therapy arm.’
The following expert panel recommendation was modified to include information on the approval of tremelimumab and durvalumab: ‘For first-line treatment of patients with advanced Child-Pugh A HCC, atezolizumab plus bevacizumab is recommended, unless either medication is contraindicated (LE: 2).’
The updated recommendation now reads: ‘For first-line treatment of patients with advanced Child-Pugh A HCC, atezolizumab plus bevacizumab (LE:2) or tremelimumab plus durvalumab (LE:2) are recommended, unless any medications are contraindicated.’
The following expert panel recommendation was modified to include information on the approval of tremelimumab and durvalumab: ‘For patients with contraindications to atezolizumab plus bevacizumab treatment, lenvatinib or sorafenib should be considered as standard first-line therapy (LE: 2).’
The updated recommendation now reads: ‘For patients with contraindications to an ICI-containing combination therapy (ie, atezolizumab plus bevacizumab or tremelimumab plus durvalumab), lenvatinib or sorafenib should be considered as standard first-line therapy (LE:2).’
Table 4 has been edited to include information on the HIMALAYA trial and efficacy data for tremelimumab and durvalumab:
Immunotherapies in development for HCC
The following sentence has been modified: ‘Tremelimumab, an anti-CTLA-4 ICI, has been evaluated in a pilot trial of patients with HCC with chronic HCV infection.’
The updated text now reads: ‘Tremelimumab monotherapy has been evaluated in a pilot trial of patients with HCC with chronic HCV infection.
The following sentences have been removed to reflect the approval of tremelimumab in combination with durvalumab. Details on the data supporting the FDA approval of tremelimumab plus durvalumab were added to the First-line therapy section.
Removed text: ‘Combination ICI regimens are also under investigation. The FDA has approved nivolumab at 1 mg/kg with ipilimumab at 3 mg/kg regimen as a second-line treatment option for patients with prior sorafenib exposure. Recently, another combination regimen, durvalumab in combination with tremelimumab, reported an ORR of up to 22.7% and a median OS of up to 18.7 months in the advanced HCC population using one single dose of tremelimumab at 300 mg, with further enhancement of response among patients with CD8+Ki67+ proliferative T cells. The phase III HIMALAYA trial investigating one single dose of tremelimumab with durvalumab as first-line treatment in patients with unresectable HCC is ongoing and this combination regimen has been granted orphan drug designation by the FDA.’
Patient selection and management
The following sentences have been modified to include information on the approval of tremelimumab and durvalumab: ‘For the combination of atezolizumab with bevacizumab in IMbrave150, the most common adverse reactions were hypertension (n=98, 29.8%), fatigue (n=67, 20.4%), and proteinuria (n=66, 20.1%), and no serious AEs with a difference in incidence of >2% were noted between the atezolizumab with bevacizumab and sorafenib treatment groups.’
The updated text now reads: ‘For the combination of atezolizumab with bevacizumab in IMbrave150, the most common adverse reactions were hypertension (n=98, 29.8%), fatigue (n=67, 20.4%), and proteinuria (n=66, 20.1%), and no serious AEs with a difference in incidence of >2% were noted between the atezolizumab with bevacizumab and sorafenib treatment groups. For the combination of tremelimumab plus durvalumab, the most common any grade treatment-related AEs were diarrhea (26.5%), pruritus (22.9%), and rash (22.4%).’ 1
Patient support and QOL
The following sentences have been modified to include information on QOL outcomes in HIMALAYA: ‘Additionally, IMbrave150 provided a large and rich data set on patient-reported QOL outcomes, which complemented the efficacy data, with a reporting rate of greater than 90%. The study found that fewer patients treated with the combination of atezolizumab with bevacizumab experienced QOL deterioration compared with those receiving sorafenib. Furthermore, for the patients who did experience QOL deterioration on immunotherapy, the onset was later.’
The updated text now reads: ‘Additionally, IMbrave150 provided a large and rich data set on patient-reported QOL outcomes, which complemented the efficacy data, with a reporting rate of greater than 90%. The study found that fewer patients treated with the combination of atezolizumab with bevacizumab experienced QOL deterioration compared with those receiving sorafenib. Furthermore, for the patients who did experience QOL deterioration on immunotherapy, the onset was later. In HIMALAYA, durvalumab in combination with tremelimumab treatment was also associated with delayed worsening of disease-related symptoms, physical functioning, and global QOL compared to sorafenib.’ 1
Reference
- 1. Abou-Alfa GK, Lau G, Kudo M, et al. Tremelimumab plus Durvalumab in Unresectable hepatocellular carcinoma. NEJM Evidence 2022;1. 10.1056/EVIDoa2100070 [DOI] [PubMed] [Google Scholar]