

Abstract
Objective:
Prenatal exposure to neighborhood crime has been associated with weaker neonatal frontolimbic connectivity; however, associations with early childhood behavior remain unclear. We hypothesized that living in a high crime neighborhood would be related to higher externalizing symptoms at 1 and 2 years, over and above other adversities, and that neonatal frontolimbic connectivity and observed parenting behaviors at 1 year would mediate this relationship.
Method:
Participants included 399 pregnant women, recruited as part of the eLABE study. Geocoded neighborhood crime data was obtained from Applied Geographic Solution. A total of 319 healthy, non-sedated neonates were scanned using resting-state fMRI on a Prisma 3T scanner and had ≥10 minutes of high-quality data. Infant-Toddler Socioemotional Assessment Externalizing T-scores were available for 274 mothers of 1-year-olds and 257 mothers of 2-year-olds. Observed parenting behaviors were available for 202 parent-infant dyads at 1 year. Multilevel and mediation models tested longitudinal associations.
Results:
Living in a neighborhood with high violent (β=.15, CI=.05–.27, p=.004) and property (β=.10, CI=.01–.20, p=.039) crime was related to more externalizing symptoms at 1 and 2 years, controlling for other adversities. Weaker frontolimbic connectivity was also associated with higher externalizing symptoms at 1 and 2 years. After controlling for other adversities, parenting behaviors mediated the specific association between crime and externalizing symptoms, but frontolimbic connectivity did not.
Conclusion:
These findings provide evidence that early exposure to neighborhood crime and weaker neonatal frontolimbic connectivity may influence later externalizing symptoms and suggest that parenting may be an early intervention target for families in high crime areas.
Keywords: externalizing behaviors, early life adversity, neighborhood crime, fMRI, early childhood
INTRODUCTION
Rapid and significant behavioral development occurs in the first two years of life, including in socioemotional domains that may rely on frontolimbic brain connectivity.1,2 While typically-developing toddlers often test boundaries and act impulsively or aggressively while developing socioemotional skills, toddlers who display severe behavior problems are more likely to develop externalizing disorders in childhood/adolescence.3 Importantly, this behavioral development, as well as underlying brain function, may be sensitive to adversity in general and neighborhood crime in particular, with theoretical models suggesting that community violence is an important environmental threat.4 Prenatal exposure to neighborhood crime has previously been associated with weaker frontolimbic connectivity in the newborn brain;5 however, it remains unclear whether neighborhood crime exposure and alterations in neonatal frontolimbic connectivity are also related to externalizing symptoms in toddlerhood.
Previous studies suggest that neighborhood crime may be a particularly salient environmental factor that relates to externalizing symptoms in older children. Meta-analytic evidence indicates that high levels of community violence are associated with greater psychiatric symptomatology, including externalizing symptoms.6 More specifically, community violence exposure has been related to aggression7 and conduct problems8 in both healthy adolescents and those with conduct disorder.9 This association between crime and externalizing symptomatology also persists when simply hearing about community violence, as opposed to being a victim or a witness of violence.6,10 Living in a high crime area during pregnancy, infancy, and toddlerhood may have different effects on behavior than later neighborhood crime exposure; however, only two previous studies have examined the relationship between crime and externalizing symptoms in early childhood.11,12 Ma et al. (2020) found that mother’s exposure to community violence was related to higher levels of externalizing symptoms in preschoolers at ages 3 and 5 years.11 Ramey and Harrington (2019) found that living in an area with high burglary at birth related to increased externalizing symptoms in girls at three years of age.12 These studies point to an association between neighborhood crime exposure and externalizing symptoms; however, it remains unclear whether these relationships occur in toddlerhood and what mechanisms might mediate these relationships.
Neonatal functional connectivity may be a mediating factor as weaker neonatal functional connectivity has been previously associated with greater externalizing problems in toddlers.13 Externalizing symptoms have also been associated with changes in brain function measured by resting-state and task-based fMRI in older children. A meta-analysis demonstrated increased limbic activity, including in the amygdala and hippocampus, during anger- or aggression-eliciting tasks in participants with a history of aggression;14 another meta-analysis found structural and functional abnormalities in the amygdala, insula, striatum, and frontal gyrus in individuals with conduct problems.15 Multiple studies have also shown that youth with conduct problems have altered amygdala activity and amygdala-ventromedial prefrontal cortex connectivity during empathy, emotional processing, and moral judgment tasks.16 Together with a prior study linking prenatal neighborhood crime exposure to weaker neonatal thalamus-anterior default mode connectivity,5 this literature suggests that neonatal functional connectivity could be a potential mediator between neighborhood crime exposure and externalizing symptoms. The prior literature also suggests that frontolimbic regions [amygdala, hippocampus, thalamus, anterior default mode, anterior frontoparietal network] may good candidates for hypothesis driven analyses, as these regions have been consistently associated with both neighborhood crime exposure and externalizing behaviors.5,13–16 Examining neonatal frontolimbic connectivity as a mediator is important, as it could indicate a need for prenatal interventions.
Another potential mediator between neighborhood crime exposure and toddler’s externalizing symptoms is parenting behaviors. Prior work has shown that exposure to community violence is associated with more parental harshness and less emotion expressivity. Specifically, higher exposure to community violence has been associated with more psychologically and physically aggressive parenting.17 Mother’s fear of crime has also been associated with less frequent expressions of positive emotions with their children.18 These parenting behaviors can inadvertently contribute to children’s externalizing symptoms as low warmth and high negativity have been associated with higher externalizing symptoms.19,20 In older children, mediation analyses show that low maternal warmth can exacerbate the effects of community violence on externalizing symptoms, especially for children living in high crime areas.19,21,22 In light of these findings, it is important to examine early parenting behaviors as a potential mediator because parenting interventions may be particularly impactful in toddlerhood.
Overall, this study utilizes a racially- and socioeconomically-diverse longitudinal cohort to investigate whether neighborhood crime is related to externalizing symptoms in toddlerhood and explores two potential factors that may mediate this relationship: neonatal functional connectivity and observed parenting behaviors. We tested whether longitudinal exposure to objectively measured neighborhood crime was related to parent-report externalizing symptoms at 1 and 2 years of age using within-person, multi-level modeling and controlled for other forms of adversity. In addition, we tested whether neonatal frontolimbic connectivity was related to parent-report externalizing symptoms at 1 and 2 years of age, over and above other adversities, and whether neonatal frontolimbic connectivity mediated the specific relationship between neighborhood crime exposure at birth and externalizing symptoms at age 2. We also explored whether multiple observed parenting practices were mediators of this relationship. We hypothesized that both higher neighborhood crime exposure and weaker neonatal frontolimbic connectivity would be related to greater externalizing symptoms at 1 and 2 years, and that weaker neonatal frontolimbic connectivity and weaker positive/greater negative parenting would mediate the relationship between higher neighborhood crime exposure and greater externalizing symptoms. This study extends prior work by using a broad range of objective crime data and observed parenting behaviors, incorporating residential moving data, examining these relationships at an earlier developmental period, and investigating two potential mediating mechanisms.
METHOD
Participants
Participants included 399 mother-infant dyads recruited as part of the Early Life Adversity, Biological Embedding, and Risk for Developmental Precursors of Mental Disorders (eLABE) study from two outpatient obstetrics clinics in St. Louis, Missouri. Written informed consent was obtained from mothers prior to participation in the study. All study procedures were approved by Washington University in St. Louis Institutional Review Board. Addresses and income-to-needs ratios were collected every 4 months from birth to two years of age via survey. Neonatal imaging was performed shortly after birth (mean postmenstrual age [PMA]=41 weeks, range=37–45). Mothers of participants filled out surveys including the Infant and Toddler Socioemotional Assessment (ITSEA) at 1 year (mean=13 months, range = 10.9–20.6) and 2 years (mean=25 months, range=22.9–31.7). Participants also returned in-person at 1 year (mean=13.2 months, range=10.9–21.1) and completed a number of assessments including a parent-child interaction task. Inclusion criteria for the present study included speaking English, maternal age 18 years or older, and singleton birth. Excluded were women with self-reported alcohol or illicit substance use during pregnancy other than marijuana (see Supplement 1 for analysis excluding marijuana as those participants were included in the main analyses for generalizability and to preserve statistical power, available online), known maternal congenital infections, or fetal abnormalities including intrauterine growth restriction. Neonates were excluded if they had any parenchymal abnormality detected on neonatal MRI during an anatomic MR review by a neuroradiologist (J.S.S.) and pediatric neurologist (C.D.S.). Of the 399 neonates who were recruited, 382 participants were healthy with no evidence of brain injury. The demographics of this sample are listed in Table 1.
Table 1.
Sample Demographics (n = 382)
| % | n | ||
|---|---|---|---|
|
| |||
| Infant Characteristics | |||
| Sex assigned at birth | |||
| Female | 44.5 | 170 | |
| Male | 55.5 | 212 | |
| Race | |||
| African American | 62.83 | 240 | |
| Asian | 1.31 | 5 | |
| Pacific Islander | 0.26 | 1 | |
| White | 33.51 | 128 | |
| Othera | 1.05 | 8 | |
| Ethnicity | |||
| Hispanic or Latina/o | 2.62 | 10 | |
| Not Hispanic or Latina/o | 96.86 | 370 | |
| Unspecified | 0.52 | 2 | |
| Maternal Background | |||
| Educationb | |||
| Less than High school | 7.33 | 28 | |
| High school graduate | 54.45 | 208 | |
| College graduate | 10.47 | 40 | |
| Post-graduate degree | 21.99 | 84 | |
| Unspecified | 5.76 | 22 | |
| Race | |||
| African American | 63.09 | 241 | |
| Asian | 1.31 | 5 | |
| Pacific Islander | 0 | 0 | |
| White | 33.25 | 127 | |
| Other (Not defined) | 2.36 | 9 | |
| Ethnicity | |||
| Hispanic or Latina | 2.62 | 10 | |
| Not Hispanic or Latina | 96.86 | 370 | |
| Unspecified | 0.52 | 2 | |
|
| |||
| Mean | SD | Range | |
|
| |||
| Infant Characteristics | |||
| 1yo. ITSEA Domain Scores | |||
| Externalizing T-scores (n=274) | 52.7 | 11.4 | 32–96 |
| Internalizing T-scores (n=280) | 47.5 | 10.8 | 26–80 |
| 2yo. ITSEA Subdomain Scores | |||
| Externalizing T-scores (n=257) | 54.0 | 10.4 | 33–99 |
| Internalizing T-scores (n=258) | 47.9 | 10.7 | 27–77 |
| Maternal Background | |||
| Age at delivery, years | 29.1 | 5.3 | 18–41 |
Note: ITSEA = Infant and Toddler Socioemotional Assessment
Two children were Non-Hispanic White and African American. Two children were Non-Hispanic White and Asian. Four participants were missing data.
Maternal education category represents the highest level of education that a mother achieved from birth to age 2 years.
Of these 382 participants, 316 participants (83% retention) had address and survey data and thus were included in the analyses relating crime to externalizing symptoms. Usable fMRI scans with ≥10 minutes of data was available for 319 participants (84% usable scans). After accounting for the missing fMRI and survey data, the final sample size for the analyses with fMRI and externalizing symptoms was n=276 and n=265 when crime, racial discrimination, and income-to-needs variables were included in the model. Parenting data at age 1 year was obtained and coded from in-person assessments for 202 participants. Detailed reasons for missing data are described in the Supplement 1, available online. Parent-child dyads with missing data did not differ from parent-child dyads without missing data on any demographic characteristics including child sex, maternal education, race, experiences of discrimination, gestational age at birth, neighborhood crime at birth, or income to needs at birth.
Measures
Geocoding and Crime Rates.
Maternal addresses were collected up to seven times from birth to age 2 years at the following time-points: birth, 4 months, 8 months, 12 months, 16 months, 20 months, and 24 months. The addresses were geocoded and categorized into their respective block groups based on the “Block API” from the Federal Communications Commission, as well as from the ‘censusxy’ package in RStudio using the 2010 Decennial Census.23 Supplemental analyses examined moving patterns, though at the group-level crime rates did not change over time (see Supplement 1; Figure S1; available online). The number of mothers with data at each timepoint and at multiple timepoints is listed in Table S1, available online.
Crime data at the block group level were obtained from Applied Geographic Solution’s (AGS) CrimeRisk Database from 2020, a commercial dataset that combines data from over 16,000 law enforcement agencies.24 AGS Crime data is indexed in comparison to the national average, which is set at a value of 100. The two variables of interest in these analyses are “Crimes Against Persons” (hereafter referred to as “Violent Crime”), which combines data on murder, rape, robbery, and aggravated assault, and “Property Crimes,” which combines data on burglary, larceny, and motor vehicle theft. Crime rates relative to the national average at the block-group level in St. Louis City are displayed in Figure 1 and rates and trajectories of the exposure to violent crime over time is described in Figure 2 and Figure S2, available online. Multi-level models were conducted by averaging the birth through 12-month timepoints and the 16-month through 24-month timepoints to leverage all of our collected data given that the outcome measures were collected at 1 and 2 years. The analyzed crime rates do not assess personal exposure to crime.
Figure 1: Map of Violent and Property Crime in St. Louis City.

Maps display the 2020 violent (left) and property (right) crime rates relative to the national average (set as 100) in St. Louis city. The borders on the maps represent block group boundaries established in the 2010 census.
Figure 2: Household Moving Patterns from Birth to 2 Years.
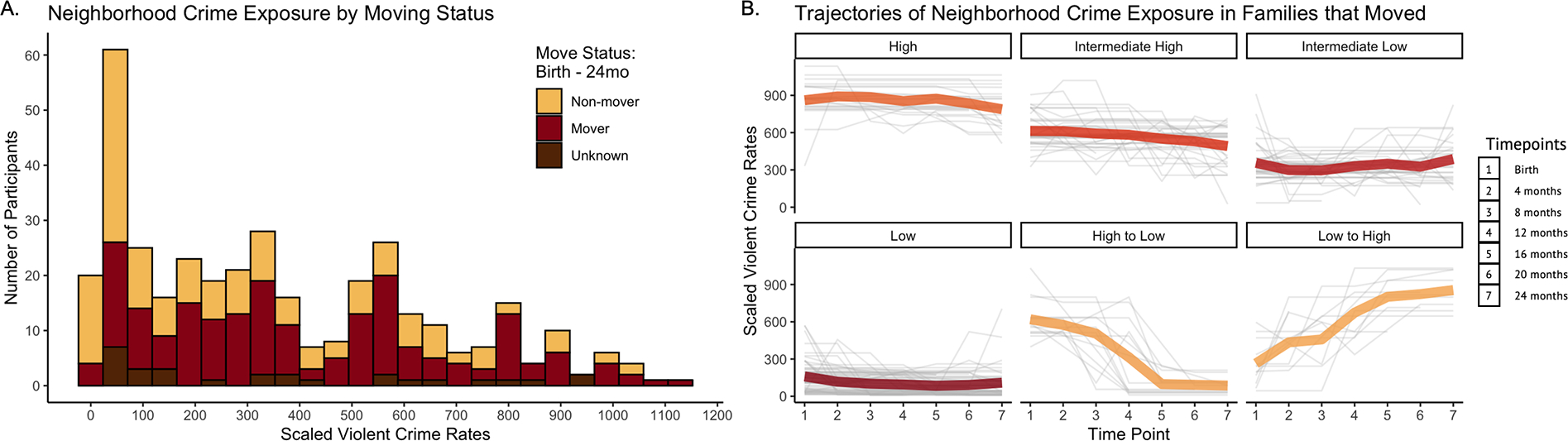
Panel A displays the number of participants who are exposed to a particular level of violent crime (i.e. crime rate compared to the national average of 100) at birth, grouped by whether or not the family moved from birth until age 2 years, in a stacked histogram. The yellow bar represents mother-child dyads that never reported moving (n=155) whereas the red bar represents mother-child dyads that reported moving at least once during the 2-year period (n=192). The brown bar represents mothers who only had address data at one time point, so it was unknown if they moved (n=35). Panel B examines the various trajectories of neighborhood crime exposure in families that moved to show how neighborhood crime exposure changed over time. Latent classes are depicted for display purposes only as they allow for better visualization of moving patterns across various participants (for more details on this analysis see Supplement 1, available online). The red-to-orange lines represent the average violent neighborhood crime exposure over time within a particular latent class, with each color representing an individual class. Darker/red lines represent more participants in a class whereas lighter/orange lines represent fewer participants in a class.
Functional MRI.
Imaging was performed in sleeping, non-sedated infants using a Siemens (Munich, Germany) 3T PRISMA scanner and 64-channel head coil. T2-weighted images (208 slices, 0.8mm isotropic resolution, TE=563ms, tissue T2=160ms, TR=3200ms or 4500ms) were collected. Resting-state functional imaging data were collected using a blood-oxygen-level dependent (BOLD) gradient-recalled echo-planar multiband sequence (72 slices, 2.0mm isotropic resolution, TE=37 ms, TR=800 ms, MB factor=8). FIRMM was used during scanning to monitor real-time participant movement.25 MRI data underwent standard BOLD pre-preprocessing followed by functional connectivity processing (see Supplement 1, available online) done in surface space for cortical areas and volume space for subcortical areas. A minimum of 10 minutes of low-motion (framewise displacement <0.25mm) data were required for inclusion. Resting-state functional connectivity measures were computed as the Fisher z-transformed Pearson correlation between time courses from pairs of surface vertices or surface parcels. Values were arranged into a connectivity matrix based upon age-specific resting state network assignments that were determined and validated using previously published methods.26,27 A total of 11 networks were identified and are displayed in Figure S3, available online. In the neonatal networks, the default mode network (DMN) and frontal parietal network (FPN) were split into anterior and posterior portions as that was the best fit for the data based on community segregation algorithms.28 Figure 3 demonstrates the frontolimbic regions of interest that were examined in hypothesis-driven analyses. Frontolimbic regions were chosen based on prior research [limbic structures: amygdala, hippocampus, thalamus; frontal regions: anterior DMN (aDMN) and anterior FPN (aFPN)].5,13–16 Two negative control regions (motor-motor and motor-aDMN) were also examined.
Figure 3: Neonatal Brain Regions/Networks of Interest.

The brain regions and networks of interest (Teal=Amygdala; Pink=Hippocampus; Green=Thalamus; Red=Anterior Default Mode Network; Blue=Anterior Frontal Parietal Network) are displayed on the neonatal brain. The neonatal brain was constructed using an atlas with n=8 participants mapped to a single participant. Blender was used to edit transparency for visualization of deeper brain structures.
Infant and Toddler Socio Emotional Assessment (ITSEA).
The ITSEA is a parent-reported questionnaire that measures socioemotional problems and behavioral competencies in 12- to 36-month-old children.29 The ITSEA was collected prospectively at both 1 year and 2 years in our study. Analyses focused on externalizing symptoms, which have demonstrated good test-retest reliability, and construct validity.29 The externalizing domain of the ITSEA includes three subdomains: activity/impulsivity, aggression/defiance, and peer aggression. The internalizing domain of the ITSEA was used as a control to further examine behavioral domain specificity. Analyses of externalizing and internalizing behaviors used the domain T-scores. Domain T-scores were normed for sex, age, and adjusted for prematurity, so these variables are controlled for within the analyses by virtue of using the T-score.30 T-scores have a mean of 50 with a standard deviation of 10. Externalizing subdomain analyses used raw scores, as T-scores are unavailable, so sex and age were included in the models as covariates. For both T-scores and raw scores, higher scores represent more of that behavior. All surveys were completed by mothers.
Parenting Behaviors.
The Parent Child Interaction Rating Scales, a validated observational coding system used extensively in studies of racially, ethnically and socioeconomically diverse studies of families and young children,31,32 was used to code observationally measured parent-child interactions (PCI) at 1 year of age across standardized videotaped tasks. Parenting behaviors were scored on a 7-point scale where higher scores represent more of a given behavior. Five parenting behaviors were examined in this study: positive regard (e.g., verbal or non-verbal expressions of warmth, love, and praise), sensitivity (e.g., noticing and responding to a child’s cues), negative regard (e.g., verbal or nonverbal expressions of anger, disapproval, or rejection of the child), intrusiveness (e.g., directive, controlling, or adult-centered interactions), and detachment (e.g., lack of attention to and engagement with the child). These behaviors were assessed and averaged across the three tasks: a feeding task in which parent feeds child a snack, a teaching task in which parent teaches child to find a ball under two cups, and a free play task in which parent and child freely play with a bin of toys. Cronbach’s alpha was .65 to .82 for all measures. Reliability was established by coders reaching a “gold standard” with the master coder of 92% exact or within 1 point on the coding scale before coding interactions independently, and 20% of tapes were double coded for ongoing reliability. Ratings were also examined for racial bias (see Supplement 1; Figure S4, available online) Intraclass correlation coefficients (ICCs) computed at the conclusion of the study all indicated good reliability (.78 to .87). 200 mothers and 2 fathers completed the PCI task; results were unchanged when fathers were excluded from analyses.
Adversity Measures.
We assessed self-reported family income and household size compared to the federal poverty level birth, hereby referred to as the income-to-needs ratio (INR), every four months for two years. Multi-level models were conducted by averaging prenatal INR through 12-month INR and 16-month INR through 24-month INR to leverage all of our collected data. We also collected and averaged a measure of neighborhood poverty, the Area Deprivation Index (ADI), in the same way (see Supplement 1; Table S2, Table S3, available online). Finally, we assessed mother’s self-reported experiences of racism using the Everyday Discrimination Survey,33 which was collected at the neonatal MRI scan. We averaged participants’ experienced discrimination that was attributed to “race” or “skin color.” Experiences of racial discrimination were included in our analyses instead of race because race is not biologically meaningful and is instead a proxy for racism and cultural differences.
Data Analysis
All analyses were conducted using R and RStudio.34 Distributions of crime levels, adversity, frontolimbic functional connectivity, and parenting were examined. Within-participant, longitudinal, multi-level models relating neighborhood crime exposure to ITSEA Externalizing T-scores at ages 1 and 2 years were conducted using the ‘lme4’ package. Violent and property crime were examined in separate models using a forward model selection process with time, crime, and an interaction (crime-by-time) to find the best model fit based on AIC and chi-square values. Specificity analyses controlled for INR and participant’s self-reported experience of racism. Additional control analyses were conducted using neighborhood poverty, as measured by the ADI, instead of INR (see Supplement 1; Table S2, available online) and individual trauma history (see Supplement 1, available online). Relationships with internalizing symptoms were examined as a behavioral control (see Table S4, available online). Each table contains the final predictors for the specified model. In an ad-hoc analysis, multi-level models with the ITSEA subdomain scores as the outcome variables were conducted to determine which type of externalizing symptoms were related to crime.
To examine the relationship between fMRI and externalizing symptoms, bivariate correlations between hypothesized frontolimbic connections and ITSEA Externalizing T-scores were computed and corrected for multiple comparisons using the Benjamini-Hochberg procedure for false discovery rate (21 corrections). For a complete bivariate correlation table with corrected p-values, see Table S5, available online. Significant bivariate associations were then further related to externalizing symptoms using multi-level models corrected for gestational age at birth and postmenstrual age at scan. Ad-hoc analyses also examined relationships with the subdomains of externalizing behavior (see Supplement 1, available online). Additional analyses controlled for violent crime, racial discrimination, and INR to determine connections that might mediate the relationship between crime and externalizing symptoms (see Supplement 1 for analysis using ADI; Table S3, available online).
To examine mediation, the indirect path from neighborhood violent crime exposure at birth to externalizing T-scores at ages 1 and 2 years through neonatal functional connectivity was tested in a structural model and non-parametrically bootstrapped using 1000 simulations with the ‘laavan’ package in R, correcting for INR and racial discrimination (see Supplement 1 for ADI analysis, available online). For the parenting mediation, bivariate associations between parenting practices (positive regard, sensitivity, negative regard, intrusiveness, and detachment) and violent crime/ITSEA externalizing T-scores were computed and corrected for multiple comparisons using the Benjamini-Hochberg procedure for false discovery rate (5 corrections per analysis). All associations passed multiple comparisons testing and were used in subsequent mediations, see Table S6, available online. The structural modelling method described above was used to test whether parenting practices at 1 year of age were mediators of the relationship between neighborhood crime exposure at birth and externalizing symptoms at age 2 years.
RESULTS
Neighborhood Crime and Externalizing Symptoms at 1 and 2 years
Multi-level models demonstrated that high levels of violent crime were positively related to externalizing symptoms, meaning that children living in areas with higher crime levels displayed more externalizing behavior at 1 and 2 years (β=0.19, CI=.10–.29, p=.001; Table S7, available online). Similarly, high levels of property crime were positively related to externalizing symptoms (β=.14, CI=.04–.23, p=.01; Table S8, available online). When controlling for INR and racism, the relationships between violent crime (β=.15, CI=.05–.27, p=.004; Table S7, available online) and property crime (β=.10, CI=.01–.20, p=.039: Table S8, available online) with externalizing symptoms remained significant. The interaction between crime and time improved model fit but was non-significant (Figure S5, available online). Within the externalizing domain, aggressive/defiant behaviors were related to both violent crime (β=.08, CI=.02–.19, p<.001) and property crime (β=.05, CI=.04–.15, p=.004) controlling for INR and racism; however, neither activity/impulsivity nor peer aggression were related to neighborhood crime (all p>.05). Replacing INR with the ADI yielded similar results (see Supplement 1; Table S2, available online) and no change in significant results was observed when accounting for individual trauma history (see Supplement 1, available online). Neither violent nor property crime was associated with internalizing symptoms in specificity analyses (all p>.05; Table S4, available online).
Neonatal fMRI and Externalizing Symptoms at 1 and 2 years
In multi-level models controlling for GA at birth and PMA at scan, weaker amygdala-thalamus (β=−.13, CI=−.24–−.02, p=.02), thalamus-aFPN (β=−.14, CI=−.25–−.03, p=.01), amygdala-aDMN (β=−.13, CI=−.24–−.02, p=.03), and thalamus-thalamus (β=−.12, CI=−.24–−.01, p=.04) connectivity were all associated with higher externalizing symptoms at 1 and 2 years. In specificity analyses, amygdala-thalamus connectivity (β=−.14, CI=−.25–−.03, p=.01; Table 2) remained significant when controlling for crime, racism, and INR. However, amygdala-thalamus connectivity did not mediate the specific relationship between neighborhood crime at birth and externalizing symptoms at 1 year (indirect path: Std Est.=.003; p=.82) or 2 years (indirect path: Std Est.=.002; p=.85), after controlling for prenatal INR and racial discrimination. This indirect path was non-significant because neighborhood crime did not predict amygdala-thalamus connectivity over and above INR and racial discrimination (Std. Est. −0.02; p=0.80 for year 1; std. Est. −0.02; p=0.83 for year 2). There was no change in significant results when INR was replaced by ADI (see Supplement 1; Table S3, available online). Additionally, motor-motor (β=−.05, p=.43) and motor-DMN (β=−.02, p=.74) connectivity were not related to externalizing symptoms at ages 1 and 2 years, suggesting frontolimbic specificity.
Table 2.
Crime and Neonatal fMRI Predict Externalizing Symptoms at 1 and 2 years
| ITSEA Externalizing T-score | |||
|---|---|---|---|
| Predictors | Statistic std. Beta | p | |
|
| |||
| Intercept | 1.45 | 0.00 | 0.149 |
| Time | 2.28 | 0.06 | 0.023 |
| GA at Birth | −0.36 | −0.02 | 0.719 |
| PMA at Scan | 1.46 | 0.09 | 0.146 |
| Amygdala-Thalamus | −2.53 | −0.14 | 0.012 |
| Income-to-Needs | −1.22 | −0.07 | 0.222 |
| Violent Crime | 2.64 | 0.17 | 0.009 |
| Racial Discrimination | 2.63 | 0.15 | 0.009 |
| Violent Crime-by-Time | −1.42 | −0.05 | 0.156 |
| Random Effects | |||
| σ2 | 50.10 | ||
| τ00 participant | 51.82 | ||
| ICC | 0.51 | ||
| n participants | 265 | ||
|
| |||
| Observations | 434 | ||
| Marginal R2 / Conditional R2 | 0.106 / 0.560 | ||
Note: ICC = Intraclass correlation coefficient; ITSEA = Infant and Toddler Socioemotional Assessment.
Parenting Behaviors as Mediators
Higher levels of violent crime at birth were related to decreased parental positive regard (indirect path: Std Est.=.06; p=.038) and decreased parental sensitivity (indirect path: Std Est.=.09; p=.006) at 1 year controlling for INR and racial discrimination, which were in turn related to more externalizing symptoms at age 2 years. Increased parental negative regard also mediated the relationship between high levels of violent crime and greater externalizing symptoms, controlling for INR and racial discrimination (indirect path: Std Est.=.09; p=.01). In contrast, neither parental intrusiveness (indirect path: Std Est.=.04; p=.09) nor parental detachment (indirect path: Std Est.=.06 p=.07) mediated the specific relationship between crime and externalizing symptoms. All models demonstrated a good fit for the data with a CFI > .95, RMSEA < .07 (all but one model <.05), and SRMR < .05. There was no change in significant results when INR was replaced by ADI (see Supplement 1, available online).
DISCUSSION
Exposure to high rates of neighborhood violent or property crime during the first two years of life is related to toddler’s externalizing symptoms at ages 1 and 2 years, even when controlling for other forms of adversity. Specifically, living in an area with high crime is related to toddler’s aggression and defiance, but not their attention, impulsivity, or peer aggression. Weaker neonatal frontolimbic connectivity in the amygdala-thalamus, thalamus-aFPN, amygdala-aDMN, and thalamus-thalamus were also related to externalizing symptoms in toddlers, although only the amygdala-thalamus connectivity contributed additional variance over and above INR, racism, and exposure to neighborhood crime. However, amygdala-thalamus connectivity at birth did not mediate the specific relationship between neighborhood crime exposure and externalizing symptoms. Instead, less parental positive regard, less parental sensitivity, and more parental negative regard in observed parenting tasks at age 1 year mediated the relationship between neighborhood crime exposure at birth and externalizing symptoms at age 2 years.
Similar to the existing literature linking community violence exposure to children’s externalizing symptoms in general and aggressive behaviors in particular,6–10 this study demonstrated that exposure to neighborhood crime is related to externalizing symptoms, especially aggression and defiance, in toddlers. Two other studies conducted in early childhood also demonstrate a similar link between neighborhood crime and early externalizing symptoms,11,12 though these studies did not examine the subdomains of externalizing psychopathology. The current study also expanded upon prior findings by showing that violent crimes, in addition to burglaries,12 were related to increased externalizing symptoms and aggression. There is increasing evidence that living in an area with high crime may be detrimental in early childhood. This is important as many public policies aim to reduce externalizing symptoms in school-aged children and adolescents by reducing the time spent in high-crime neighborhoods after school, but these policies do not address the mechanisms by which crime might be influencing toddlers prior to school entry. Additional public policy and public health interventions, such as providing more resources to families in high crime areas, may be necessary to ameliorate the effects of neighborhood crime exposure on externalizing symptoms in early childhood.
This study also demonstrated that weaker neonatal functional connectivity between the amygdala-thalamus, thalamus-aFPN, amygdala-aDMN, and thalamus-thalamus at birth were related to externalizing symptoms at ages 1 and 2 years. These findings align with the prior literature showing changes in amygdala activation,14,16 as well as resting state changes in amygdala connectivity in children with conduct problems.15,16 Reductions in ventromedial prefrontal cortex and DMN connectivity have also been implicated in conduct problems.16 However, the thalamus’ potential role in externalizing disorders has previously been under-appreciated, as most studies do not include the thalamus as an area of interest. The thalamus is classically thought of as a “relay station” or “gatekeeper” for sensory information,35,36 but the paraventricular thalamic nucleus projects limbic signals from the amygdala and other subcortical regions to the anterior cingulate, orbitofrontal, and prefrontal cortices.37 Preclinical models have shown that the paraventricular nuclei determines reactions to threats38 and controls fear circuits in the amygdala,39 indicating a potential reason for thalamic associations with externalizing behavior.
Even though amygdala-thalamus connectivity was a significant predictor of externalizing symptoms over and above crime, racial discrimination, and INR, this connection did not mediate the specific relationship between crime and externalizing symptoms. This is perhaps not surprising because neonatal amygdala-thalamus connectivity was previously associated with general adversity as opposed to crime-specific adversity in the same cohort.5 Additionally, violent crime remained a significant predictor of externalizing symptoms when neonatal amygdala-thalamus connectivity was added to the model, which suggests a lack of mediation. It is important to note that neonatal frontolimbic connectivity may play a role in the development of externalizing symptoms even though it is not mediator between crime and externalizing symptoms in toddlerhood. For one, neonatal frontolimbic connectivity could mediate the relationship between other forms of adversity and externalizing symptoms. Secondly, crime and adversity may affect behavior through multiple mechanisms; even if functional connectivity changes were one of those mechanisms, one would not necessarily expect it to account for more variance than adversity (i.e., significant over and above adversity) given the multiple mechanisms at play. Future studies will be needed to further define the role of neonatal, infant, and toddler frontolimbic connectivity as a neurobiological mechanism.
Finally, this study demonstrated that parenting behaviors mediated the relationship between exposure to neighborhood crime and toddler’s externalizing symptoms. Parents in high crime areas may employ less positive/sensitive and more negative parenting behaviors as an adaptive mechanism to keep their children safe, even though it has the unintended consequence of elevating externalizing symptoms. Given that some parents in high crime areas feel the need to use strict parental control,40 early negative regard may be used to establish a hierarchy of command that allows parents to enforce discipline later on in childhood and adolescence. However, unfortunately, more negative and less positive/sensitive parenting behaviors may also have the effect of elevating externalizing problems.20 High crime areas could also normalize psychological and physical aggression and make harsher parenting styles more common41 and seemingly more acceptable. Alternatively, mothers who are constantly vigilant due to the threat of living in a high crime area may have emotional burnout. A prior study has shown that social vigilance leads to more hostile reactivity and negative emotional contagion.42 Furthermore, the amygdala is responsible for attention to threat and emotional processing,43 so it is possible that emotional processing suffers when constantly paying attention to potential threats in the environment. As such, parents suffering the stress of living in high crime areas may be less able to practice supportive parenting behaviors, which in turn leads to higher externalizing symptoms.19,20 Future studies will be needed to tease apart these various hypotheses and to develop effective interventions.
While the strengths of this study include a diverse, prospective, longitudinal sample of over 300 mother-infant dyads, objective crime metrics, neonatal fMRI, multiple observed measures of parenting, and follow-up at two timepoints, there are also some limitations. First, we were unable to control for direct exposure to crime that occurred over the first two years of life. Future work will be necessary to distinguish between the effects of living in a high crime area and being a victim or a witness of criminal behavior. Additionally, there was low social mobility in our sample given the two-year timeframe. A limited number of mothers moved between neighborhoods with significantly different crime rates, which resulted in sample sizes that were too small to examine moving trajectories in-depth (see Supplement 1, available online). Cross-lagged models would be helpful in more precisely specifying the directionality of the associations in future studies. We were also unable to control for participant’s household composition; however, prior studies have shown that living in a two-parent households did not moderate the relationship between violence exposure and children’s aggressive behaviors21 and that there was no effect of living in a single family household after accounting for socioeconomic status.44 Finally, it is possible that cultural factors, such as perceived parenting norms and rarity of specific parenting practices, may moderate the effects of parenting on externalizing symptoms.45–48 Future work will be necessary to determine how culture might alter the associations described in the manuscript and determine whether they generalize outside of an urban city in America.
Overall, this study provides evidence that living in a high crime neighborhood is associated with higher externalizing symptoms in toddlerhood. One way that neighborhood crime may alter behavior is through altered parental behaviors. Parents living in high crime areas at birth display fewer positive and sensitive behaviors and more negative behaviors when their child is 1 year old, which are in turn associated with higher externalizing symptoms in the child at age 2 years. As such, parenting may be an important target for interventions aimed at preventing elevated aggression in toddlers living in high crime areas. Future studies are needed to design appropriate parenting interventions for families with high neighborhood crime exposure. Other future directions of this work include examining whether specific types of crime (i.e., murder) or proximity to the crimes influence outcomes and exploring other biological mechanisms that might mediate the relationship between crime and externalizing psychopathology. Overall, this study aims to inspire future work that helps understand and prevent adverse effects of neighborhood crime exposure on externalizing symptoms.
Supplementary Material
Acknowledgments
Research reported in this publication was supported by the National Institutes of Health (R01 MH113883; F30 HD104313), the March of Dimes Prematurity Research Center at Washington University, the Intellectual and Developmental Disabilities Research Center at Washington University (P50 HD103525), the Washington University in St. Louis Center for the Study of Race, Ethnicity, and Equity Small Grant, Children’s Discovery Institute, the McDonnell Center for Systems Neuroscience, and the Washington University Medical Scientist Training Program. The views are those of the authors.
The authors would like to thank Michael J. Strube, PhD, of Washington University in St. Louis, for his help with the statistical analyses. The authors would also like to thank the Washington University Neonatal Developmental Research Group and eLABE staff for their support and for collecting a truly impressive amount of data. Finally, this study would not have been possible without the families involved with the study and the authors truly appreciate their generosity.
Diversity & Inclusion Statement:
We worked to ensure race, ethnic, and/or other types of diversity in the recruitment of human participants. We worked to ensure that the study questionnaires were prepared in an inclusive way. One or more of the authors of this paper self-identifies as a member of one or more historically underrepresented racial and/or ethnic groups in science. One or more of the authors of this paper self-identifies as a member of one or more historically underrepresented sexual and/or gender groups in science. We actively worked to promote sex and gender balance in our author group. We actively worked to promote inclusion of historically underrepresented racial and/or ethnic groups in science in our author group. While citing references scientifically relevant for this work, we also actively worked to promote sex and gender balance in our reference list. While citing references scientifically relevant for this work, we also actively worked to promote inclusion of historically underrepresented racial and/or ethnic groups in science in our reference list. The author list of this paper includes contributors from the location and/or community where the research was conducted who participated in the data collection, design, analysis, and/or interpretation of the work.
Footnotes
Disclosure: Drs. Gerstein, Warner, Barch, Luby, Rogers, and Smyser, Mss. Brady, Leverett, Mueller, and Ruscitti, Mr. Latham, and Ms. Smyser have reported no biomedical financial interests or potential conflicts of interest.
Publisher's Disclaimer: This is a PDF file of an unedited manuscript that has been accepted for publication. As a service to our customers we are providing this early version of the manuscript. The manuscript will undergo copyediting, typesetting, and review of the resulting proof before it is published in its final form. Please note that during the production process errors may be discovered which could affect the content, and all legal disclaimers that apply to the journal pertain.
Contributor Information
Rebecca G. Brady, Washington University School of Medicine in St. Louis, St. Louis, Missouri.
Shelby D. Leverett, Washington University School of Medicine in St. Louis, St. Louis, Missouri.
Liliana Mueller, Washington University School of Medicine in St. Louis, St. Louis, Missouri.
Michayla Ruscitti, Washington University School of Medicine in St. Louis, St. Louis, Missouri.
Aidan R. Latham, Washington University School of Medicine in St. Louis, St. Louis, Missouri.
Tara A. Smyser, Washington University School of Medicine in St. Louis, St. Louis, Missouri.
Emily D. Gerstein, Department of Psychological Sciences, University of Missouri-St. Louis.
Barbara B. Warner, Washington University School of Medicine in St. Louis, St. Louis, Missouri.
Deanna M. Barch, Washington University School of Medicine in St. Louis, St. Louis, Missouri; Washington University in St. Louis, St. Louis, Missouri.
Joan L. Luby, Washington University School of Medicine in St. Louis, St. Louis, Missouri.
Cynthia E. Rogers, Washington University School of Medicine in St. Louis, St. Louis, Missouri.
Christopher D. Smyser, Washington University School of Medicine in St. Louis, St. Louis, Missouri.
REFERENCES
- 1.Crowell JA. Development of Emotion Regulation in Typically Developing Children. Child Adolesc Psychiatr Clin N Am. 2021;30(3):467–474. doi: 10.1016/j.chc.2021.04.001 [DOI] [PubMed] [Google Scholar]
- 2.Köster M, Kärtner J. Why do infants help? A simple action reveals a complex phenomenon. Dev Rev. 2019;51:175–187. doi: 10.1016/j.dr.2018.11.004 [DOI] [Google Scholar]
- 3.Campbell SB, Shaw DS, Gilliom M. Early externalizing behavior problems: Toddlers and preschoolers at risk forlater maladjustment. Dev Psychopathol. 2000;12(3):467–488. doi: 10.1017/S0954579400003114 [DOI] [PubMed] [Google Scholar]
- 4.Ellis BJ, Sheridan MA, Belsky J, McLaughlin KA. Why and how does early adversity influence development? Toward an integrated model of dimensions of environmental experience. Dev Psychopathol. 2022;34(2):447–471. doi: 10.1017/S0954579421001838 [DOI] [PubMed] [Google Scholar]
- 5.Brady RG, Rogers CE, Prochaska T, et al. The Effects of Prenatal Exposure to Neighborhood Crime on Neonatal Functional Connectivity. Biol Psychiatry. 2022;92(2):139–148. doi: 10.1016/j.biopsych.2022.01.020 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Fowler PJ, Tompsett CJ, Braciszewski JM, Jacques-Tiura AJ, Baltes BB. Community violence: A meta-analysis on the effect of exposure and mental health outcomes of children and adolescents. Dev Psychopathol. 2009;21(1):227–259. doi: 10.1017/S0954579409000145 [DOI] [PubMed] [Google Scholar]
- 7.Jakubovic RJ, Drabick DAG. Community Violence Exposure and Youth Aggression: The Moderating Role of Working Memory. J Abnorm Child Psychol. 2020;48(11):1471–1484. doi: 10.1007/s10802-020-00683-y [DOI] [PubMed] [Google Scholar]
- 8.Edwards B, Bromfield LM. Neighborhood influences on young children’s conduct problems and pro-social behavior: Evidence from an Australian national sample. Child Youth Serv Rev. 2009;31(3):317–324. doi: 10.1016/j.childyouth.2008.08.005 [DOI] [Google Scholar]
- 9.Kersten L, Vriends N, Steppan M, et al. Community Violence Exposure and Conduct Problems in Children and Adolescents with Conduct Disorder and Healthy Controls. Front Behav Neurosci. 2017;11:219. doi: 10.3389/fnbeh.2017.00219 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Zimmerman GM, Posick C. Risk Factors for and Behavioral Consequences of Direct Versus Indirect Exposure to Violence. Am J Public Health. 2016;106(1):178–188. doi: 10.2105/AJPH.2015.302920 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Ma J, Grogan-Kaylor A, Lee SJ. Does community violence exposure moderate the associations between maternal spanking and early child behavior problems? Aggress Behav. 2020;46(3):210–219. doi: 10.1002/ab.21882 [DOI] [PubMed] [Google Scholar]
- 12.Ramey DM, Harrington N. Early exposure to neighborhood crime and child internalizing and externalizing behaviors. Health Place. 2019;57:228–237. doi: 10.1016/j.healthplace.2019.04.010 [DOI] [PubMed] [Google Scholar]
- 13.Ramphal B, Whalen DJ, Kenley JK, et al. Brain connectivity and socioeconomic status at birth and externalizing symptoms at age 2 years. Dev Cogn Neurosci. 2020;45:100811. doi: 10.1016/j.dcn.2020.100811 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Nikolic M, Pezzoli P, Jaworska N, Seto MC. Brain responses in aggression-prone individuals: A systematic review and meta-analysis of functional magnetic resonance imaging (fMRI) studies of anger- and aggression-eliciting tasks. Prog Neuropsychopharmacol Biol Psychiatry. 2022;119:110596. doi: 10.1016/j.pnpbp.2022.110596 [DOI] [PubMed] [Google Scholar]
- 15.Noordermeer SDS, Luman M, Oosterlaan J. A Systematic Review and Meta-analysis of Neuroimaging in Oppositional Defiant Disorder (ODD) and Conduct Disorder (CD) Taking Attention-Deficit Hyperactivity Disorder (ADHD) Into Account. Neuropsychol Rev. 2016;26(1):44–72. doi: 10.1007/s11065-015-9315-8 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Blair RJR, Veroude K, Buitelaar JK. Neuro-cognitive system dysfunction and symptom sets: A review of fMRI studies in youth with conduct problems. Neurosci Biobehav Rev. 2018;91:69–90. doi: 10.1016/j.neubiorev.2016.10.022 [DOI] [PubMed] [Google Scholar]
- 17.Zhang S, Anderson SG. Low-income single mothers’ community violence exposure and aggressive parenting practices. Child Youth Serv Rev. 2010;32(6):889–895. doi: 10.1016/j.childyouth.2010.02.010 [DOI] [Google Scholar]
- 18.Shareefah N. Al’Uqdah, Sycarah Grant, Celeste M. Malone, Tyne McGee, Ivory A. Toldson. Impact of Community Violence on Parenting Behaviors and Children’s Outcomes. J Negro Educ. 2015;84(3):428. doi: 10.7709/jnegroeducation.84.3.0428 [DOI] [Google Scholar]
- 19.Labella MH, Masten AS. Family influences on the development of aggression and violence. Curr Opin Psychol. 2018;19:11–16. doi: 10.1016/j.copsyc.2017.03.028 [DOI] [PubMed] [Google Scholar]
- 20.Wiggins JL, Mitchell C, Hyde LW, Monk CS. Identifying early pathways of risk and resilience: The codevelopment of internalizing and externalizing symptoms and the role of harsh parenting. Dev Psychopathol. 2015;27(4pt1):1295–1312. doi: 10.1017/S0954579414001412 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Spano R, Vazsonyi AT, Bolland J. Does parenting mediate the effects of exposure to violence on violent behavior? An ecological–transactional model of community violence. J Adolesc. 2009;32(5):1321–1341. doi: 10.1016/j.adolescence.2008.12.003 [DOI] [PubMed] [Google Scholar]
- 22.Ozer EJ, Lavi I, Douglas L, Wolf JP. Protective Factors for Youth Exposed to Violence in Their Communities: A Review of Family, School, and Community Moderators. J Clin Child Adolesc Psychol. 2015;46(3):353–378. doi: 10.1080/15374416.2015.1046178 [DOI] [PubMed] [Google Scholar]
- 23.Prener C, Fox B. Censusxy: Access the U.S. Census Bureau’s Geocoding A.P.I. System; 2021. https://CRAN.R-project.org/package=censusxy
- 24.Nau C, Sidell M, Clift K, Koebnick C, Desai J, Rohm-Young D. A commercially available crime index may be a reliable alternative to actual census-tract crime in an urban area. Prev Med Rep. 2020;17:100996. doi: 10.1016/j.pmedr.2019.100996 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.Dosenbach NUF, Koller JM, Earl EA, et al. Real-time motion analytics during brain MRI improve data quality and reduce costs. NeuroImage. 2017;161:80–93. doi: 10.1016/j.neuroimage.2017.08.025 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26.Eggebrecht AT, Elison JT, Feczko E, et al. Joint Attention and Brain Functional Connectivity in Infants and Toddlers. Cereb Cortex. Published online January 6, 2017. doi: 10.1093/cercor/bhw403 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27.Wheelock MD, Hect JL, Hernandez-Andrade E, et al. Sex differences in functional connectivity during fetal brain development. Dev Cogn Neurosci. 2019;36:100632. doi: 10.1016/j.dcn.2019.100632 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28.Sylvester CM, Kaplan S, Myers MJ, et al. Network-specific selectivity of functional connections in the neonatal brain. Cereb Cortex. Published online May 21, 2022:bhac202. doi: 10.1093/cercor/bhac202 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29.Carter AS, Briggs-Gowan MJ, Jones SM, Little TD. The Infant – Toddler Social and Emotional Assessment (ITSEA): Factor structure, reliability, and validity. J Abnorm Child Psychol. 2003;31(5):495–514. doi: 10.1023/A:1025449031360 [DOI] [PubMed] [Google Scholar]
- 30.Carter AS, Briggs-Gowan MJ. Infant toddler social and emotional assessment (ITSEA) manual. N Hav Yale Univ Dep Psychol. Published online 2000. [Google Scholar]
- 31.Brady-Smith C, O’Brien C, Berlin L, Ware A, Brooks-Gunn J. EARLY HEAD START RESEARCH AND EVALUATION PROJECT. Published online 1999. [Google Scholar]
- 32.Vogel C, Caronongan P, Thomas J, et al. Toddlers in Early Head Start: A Portrait of 2-Year-Olds, Their Families, and the Programs Serving Them. OPRE Rep 2015–10 Wash DC Off Plan Res Eval Adm Child Fam US Dep Health Hum Serv. Published online 2015. [Google Scholar]
- 33.Williams DR, Yan Yu, Jackson JS, Anderson NB. Racial Differences in Physical and Mental Health: Socio-economic Status, Stress and Discrimination. J Health Psychol. 1997;2(3):335–351. doi: 10.1177/135910539700200305 [DOI] [PubMed] [Google Scholar]
- 34.R Core Team. R: A Language and Environment for Statistical Computing. R Foundation for Statistical Computing; 2020. https://www.R-project.org/ [Google Scholar]
- 35.Sherman SM, Guillery RW. The role of the thalamus in the flow of information to the cortex. Adams P, Guillery RW, Sherman SM, Sillito AM, eds. Philos Trans R Soc Lond B Biol Sci. 2002;357(1428):1695–1708. doi: 10.1098/rstb.2002.1161 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 36.Steriade M, Llinás RR. The functional states of the thalamus and the associated neuronal interplay. Physiol Rev. 1988;68(3):649–742. doi: 10.1152/physrev.1988.68.3.649 [DOI] [PubMed] [Google Scholar]
- 37.Taber KH. The Limbic Thalamus. J Neuropsychiatry. 2004;16(2):127–132.doi: 10.1176/appi.neuropsych.16.2.127 [DOI] [PubMed] [Google Scholar]
- 38.Salay LD, Ishiko N, Huberman AD. A midline thalamic circuit determines reactions to visual threat. Nature. 2018;557(7704):183–189. doi: 10.1038/s41586-018-0078-2 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 39.Penzo MA, Robert V, Tucciarone J, et al. The paraventricular thalamus controls a central amygdala fear circuit. Nature. 2015;519(7544):455–459. doi: 10.1038/nature13978 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 40.Ceballo R, Kennedy TM, Bregman A, Epstein-Ngo Q. Always aware (Siempre pendiente): Latina mothers’ parenting in high-risk neighborhoods. J Fam Psychol. 2012;26(5):805–815. doi: 10.1037/a0029584 [DOI] [PubMed] [Google Scholar]
- 41.Barajas-Gonzalez RG, Brooks-Gunn J. Income, neighborhood stressors, and harsh parenting: Test of moderation by ethnicity, age, and gender. J Fam Psychol. 2014;28(6):855–866. doi: 10.1037/a0038242 [DOI] [PubMed] [Google Scholar]
- 42.Kraus MW, Horberg EJ, Goetz JL, Keltner D. Social Class Rank, Threat Vigilance, and Hostile Reactivity. Pers Soc Psychol Bull. 2011;37(10):1376–1388. doi: 10.1177/0146167211410987 [DOI] [PubMed] [Google Scholar]
- 43.Davis M, Whalen PJ. The amygdala: vigilance and emotion. Mol Psychiatry. 2001;6(1):13–34. doi: 10.1038/sj.mp.4000812 [DOI] [PubMed] [Google Scholar]
- 44.Beyers JM, Bates JE, Pettit GS, Dodge KA. Neighborhood Structure, Parenting Processes, and the Development of Youths’ Externalizing Behaviors: A Multilevel Analysis. Am J Community Psychol. 2003;31(1–2):35–53. doi: 10.1023/A:1023018502759 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 45.Smetana JG. Current research on parenting styles, dimensions, and beliefs. Curr Opin Psychol. 2017;15:19–25. doi: 10.1016/j.copsyc.2017.02.012 [DOI] [PubMed] [Google Scholar]
- 46.Valentino K, Nuttall AK, Comas M, Borkowski JG, Akai CE. Intergenerational Continuity of Child Abuse Among Adolescent Mothers: Authoritarian Parenting, Community Violence, and Race. Child Maltreat. 2012;17(2):172–181. doi: 10.1177/1077559511434945 [DOI] [PubMed] [Google Scholar]
- 47.Simons RL, Lin KH, Gordon LC, Brody GH, Murry V, Conger RD. Community Differences in the Association Between Parenting Practices and Child Conduct Problems. J Marriage Fam. 2002;64(2):331–345. doi: 10.1111/j.1741-3737.2002.00331.x [DOI] [Google Scholar]
- 48.Gershoff ET, Grogan-Kaylor A, Lansford JE, et al. Parent Discipline Practices in an International Sample: Associations With Child Behaviors and Moderation by Perceived Normativeness. Child Dev. 2010;81(2):487–502. doi: 10.1111/j.1467-8624.2009.01409.x [DOI] [PMC free article] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.