

Abstract
Key Clinical Message
A whirl sign on contrast‐enhanced abdominal CT scan is indicative of intestine twisted around the mesenteric vessels, and is observed in cases of strangulated obstruction, signaling compromised intestinal circulation. In cases of intestinal volvulus, surgery is necessary to untwist the affected bowel, and resection is necessary if necrosis is present.
Abstract
A 31‐year‐old Japanese man presented with acute lower abdominal pain and vomiting. Contrast‐enhanced abdominal computed tomography (CT) revealed a 1440‐degree clockwise torsion of superior mesenteric artery and a whirl sign. Intestinal volvulus in adulthood with a background of malrotation is extremely rare. Contrast‐enhanced CT is effective for diagnosis.
Keywords: abdominal contrast‐enhanced computed tomography, intestinal volvulus, malrotation, whirl sign
A 31‐year‐old Japanese man presented with acute lower abdominal pain and vomiting. Contrast‐enhanced abdominal computed tomography revealed a 1440‐degree clockwise torsion of superior mesenteric artery and a whirl sign. Intestinal volvulus in adulthood with a background of malrotation is extremely rare. Contrast‐enhanced computed tomography is effective for diagnosis.

A 31‐year‐old Japanese man presented with acute lower abdominal pain and postprandial vomiting. He had experienced similar episodes monthly since the age of 5 years. His medical history was unremarkable. His vital signs were normal. Physical examination revealed a flat, soft abdomen with normal peristalsis and tenderness of the lower abdomen and peri‐umbilical area. Laboratory tests revealed no abnormalities. Contrast‐enhanced abdominal computed tomography (CT) revealed a 1440‐degree clockwise torsion of the superior mesenteric artery, with surrounding soft tissue involvement, and a whirl sign (Figure 1). The duodenojejunal junction was displaced rightward, with a subhepatic cecum, and the transverse colon was dorsal to the superior mesenteric artery (Figure 2). When the abdomen was opened, the end of the ileum and proximal jejunum were twisted and clumped together in the pelvis. The ileum was twisted four times in a clockwise direction. The twisted intestine was mildly congested, but there was no evidence of necrosis. The intestinal stasis was quickly corrected by manual reshaping. These findings led to a diagnosis of intestinal volvulus secondary to malrotation. Although no arterial perfusion defects were present, mesenteric edema and ascites secondary to venous congestion necessitated emergency detorsion, Ladd's procedure, and prophylactic appendectomy. He was discharged on postoperative Day 13 without complications and has subsequently remained symptom‐free.
FIGURE 1.
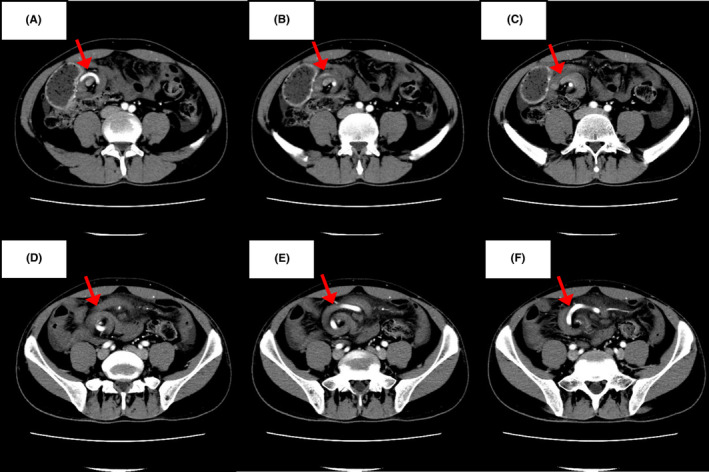
(A–F) Contrast‐enhanced abdominal computed tomography (CT) revealed a 1440‐degree clockwise torsion of the superior mesenteric artery, with surrounding soft tissue involvement, and a whirl sign.
FIGURE 2.

The duodenojejunal junction was displaced rightward, with a subhepatic cecum, and the transverse colon was dorsal to the superior mesenteric artery.
Malrotation is a congenital anomaly arising from atypical intestinal rotation during fetal development. It commonly manifests as intestinal obstruction in neonates and infants, and presentation in adulthood is extremely rare. 1 , 2 Volvulus is categorized as neonatal, primarily due to abnormal bowel rotation or mesenteric fixation defects; primary, without any underlying disease or anatomical defect; and secondary to adhesions, diverticulitis, or band‐like structures. In neonates, intestinal volvulus is typically a primary condition caused by anomalous bowel rotation or mesenteric fixation defects, without associated diseases or other anatomical irregularities, and surgery generally has a favorable outcome. A whirl sign on contrast‐enhanced abdominal CT scan is indicative of intestine twisted around the mesenteric vessels, and is also observed in cases of strangulated obstruction, signaling compromised intestinal circulation. 3 In cases of intestinal volvulus, surgery is necessary to untwist the affected bowel, and resection is necessary if necrosis is present. Notably our patient had no intestinal necrosis, despite the 1440‐degree torsion, making this case an extremely rare presentation of intestinal volvulus.
AUTHOR CONTRIBUTIONS
Jun Kakisako: Conceptualization; data curation; resources; writing – original draft. Takuya Otsuki: Conceptualization; supervision; writing – review and editing. Takeshi Asakura: Conceptualization; supervision; writing – review and editing. Daisuke Sasaki: Conceptualization; supervision; writing – review and editing. Kenya Ie: Conceptualization; supervision; writing – review and editing. Kosuke Ishizuka: Conceptualization; supervision; writing – review and editing.
FUNDING INFORMATION
No specific grant was received for this work from any funding agency.
CONFLICT OF INTEREST STATEMENT
The authors state that they have no conflict of interest.
ETHICS APPROVAL
This manuscript conforms to the provisions of the Declaration of Helsinki in 1995 (as revised in Brazil 2013).
CONSENT
Written informed consent was obtained from the patient to publish this report in accordance with the journal's patient consent policy.
ACKNOWLEDGMENTS
We thank Editage (www.editage.jp) for English language editing.
Kakisako J, Otsuki T, Asakura T, Sasaki D, Ie K, Ishizuka K. Quadruple (1440 degrees) intestinal volvulus. Clin Case Rep. 2024;12:e9022. doi: 10.1002/ccr3.9022
All authors meet the ICMJE authorship criteria.
DATA AVAILABILITY STATEMENT
The data that support the findings of this study are available from the corresponding author upon reasonable request.
REFERENCES
- 1. Perez AA, Pickhardt PJ. Intestinal malrotation in adults: prevalence and findings based on CT colonography. Abdom Radiol. 2021;46:3002‐3010. [DOI] [PubMed] [Google Scholar]
- 2. Vaez‐Zadeh K, Dutz W, Nowrooz‐Zadeh M. Volvulus of the small intestine in adults: a study of predisposing factors. Ann Surg. 1969;169:265‐271. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3. Fisher JK. Computed tomographic diagnosis of volvulus in intestinal malrotation. Radiology. 1981;140:145‐146. [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Data Availability Statement
The data that support the findings of this study are available from the corresponding author upon reasonable request.