Abstract
Clinical evidence is interpreted based on clinical studies and personal experience which can lead to different interpretations of data. This makes the opinions issued by panels of experts such as the Advanced Breast Cancer Panel which convened in November 2023 for the seventh time (ABC7) particularly important. At the conference, current issues around advanced breast cancer were evaluated by an international team of experts.
In 2023 the data on CDK4/6 inhibitors was so extensive that the answers to questions about the sequencing of therapy and the potential use of chemotherapy as an alternative therapy were relatively clear. Moreover, data on antibody drug conjugates which provides a good overview of their uses is available for all molecular subtypes.
Some therapeutic settings, including patients with brain metastases or leptomeningeal disease, older patients, locally advanced breast cancer and visceral crises, continue to be particularly important and were discussed in structured sessions. The scientific context of some of the topics discussed at ABC7 is presented and assessed here.
Keywords: breast cancer, metastatic, endocrine therapy, antibody drug conjugate, chemotherapy
Background
The Advanced Breast Cancer Conference in Lisbon (ABC7 held in 2023) focuses on the treatment of patients with advanced breast cancer. Following two days consisting mainly of overview presentations of the most important thematic areas, the third day consisted of a panel voting on key issues affecting the treatment of patients with advanced breast cancer. The majority of questions voted on during the conference and the relevant answers together with an assessment by the ABC7 panelists (ABC7 panelists; Supplement Table S1 , online) are presented here (Supplement Table S2 , online). In addition, a few selected topics have been placed in a scientific context to provide more differentiated background information about the questions.
Expansion of the Therapeutic Spectrum
After the human genome was decoded and with a growing understanding of intracellular signal transduction pathways, a number of studies were carried out in the last 20 years on patients with advanced breast cancer which lastingly changed clinical practice and treatment standards. Most of the innovations relate to signaling pathways, which have also been found to be connected to the pathogenesis and progression of breast cancer, e.g., inhibition of the PI3K/Akt-kinase pathway or utilization of the mechanisms of immune checkpoint inhibitors. Many of the discoveries were a direct consequence of systematically putting the newly obtained knowledge about the human genome to good use. Other developments have led to the development of new classes of drugs such as antibody drug conjugates (ADC), PROTACS (proteolysis-targeting chimeras) and radioligand therapeutics. While the use of PROTACS and radioligand therapeutics to treat breast cancer is still in clinical development, several ADCs have already been approved for the treatment of advanced breast cancer.
The introduction of antibody drug conjugates
The ADC trastuzumab emtansine was introduced more than 10 years ago to treat patients with advanced HER2-positive breast cancer after the EMILIA trial showed that it offered superior results over the tyrosine kinase inhibitor lapatinib in combination with capecitabine, both with regards to progression-free survival (PFS) and overall survival (OS) 1 , 2 . The introduction of new linker technology and other substances has led to the development of new ADCs such as trastuzumab deruxtecan (T-DXd). This new ADC did not just significantly improve the prognosis of HER2-positive disease 3 but also the prognosis of breast cancer in some patients with hormone receptor (HR)-positive/HER2-negative (HER2low population) and triple-negative (TNBC) breast cancer 4 . Moreover, the mechanism of action was also elucidated for sacituzumab govitecan, which targets Trop2 (trophoblast cell surface antigen 2) 5 , 6 . Sacituzumab govitecan improves both the PFS and the OS of patients with HR-positive/HER2-negative breast cancer and of TNBC patients. Accordingly, these therapies now hold a major position in the therapeutic landscape.
Immune therapies
Immune therapies differ from previous therapeutic approaches in that they change the tumorʼs micro-environment and mainly modify the interactions between the tumor cell and immune cells. The Keynote-355 trial was able to show that first-line therapy with pembrolizumab offered a benefit in terms of a better PFS and OS for patients with TNBC 7 , 8 . To assess the therapeutic effect, patients were investigated for PD-L1 expression (combined positive score; CPS). The effects of pembrolizumab were only significantly detectable if expression was confirmed with a score of more than 10. The Impassion130 trial showed similar results for atezolizumab, even though OS analysis did not achieve formal statistical significance 9 , 10 , 11 , and the results of the Impassion131 trial could not be confirmed 12 . It should be noted here that a different score must be used for the indication for treatment with atezolizumab (PD-L1 positive immune cells; IC score).
Overcoming endocrine resistance
The possibility of reducing the risk of progression or death for a certain period of time for a relevant percentage of HR+/HER2− patients is one of the big developments of recent years. The better understanding of the precise mechanisms of endocrine signaling pathways has translated into targeted therapies which modify these signaling pathways to achieve tumor control. Several drugs have been tested in clinical trials, including CDK4/6 inhibitors 13 , 14 , the Akt inhibitor capivasertib 15 and the PI3K inhibitor inavolisib 16 , and have been found to improve overall survival (ribociclib and abemaciclib) or have shown very promising trends with regards to overall survival (capivasertib and inavolisib).
State of knowledge on homologous recombination as an approach for therapy options
The introduction of PARP (poly [ADP-ribose] polymerase) inhibitors 17 , 18 , 19 , 20 , 21 , 22 represents a remarkable milestone in the treatment of patients with breast cancer. Following the discovery of the BRCA1 and BRCA2 genes, increased our understanding of the relevance of homologous recombination in the pathogenesis and progression of breast cancer. More recently, the importance of these genes is also being discussed in connection with possible endocrine resistance. An alternative explanation for reduced endocrine sensitivity in tumors with homologous recombination deficiency (HRD) could be that HR-positive tumors should be classified as a basal subtype and therefore endocrine therapy will not have the desired effect.
The voting in Lisbon at ABC7 took account of these more recent developments. Some of the facts are presented in more detail below.
Treatment of Patients with Advanced HR-positive, HER2-negative (HR+/HER2−) breast cancer
Now that treatment with CDK4/6 inhibitors has become the therapy standard for first-line treatment 23 , 24 , questions now mainly focus on the best therapy sequence.
Which exceptional patients should not receive a CDK4/6 inhibitor as first-line therapy? The focus was on the specific issue of how patients in visceral crisis who require urgent treatment should be treated.
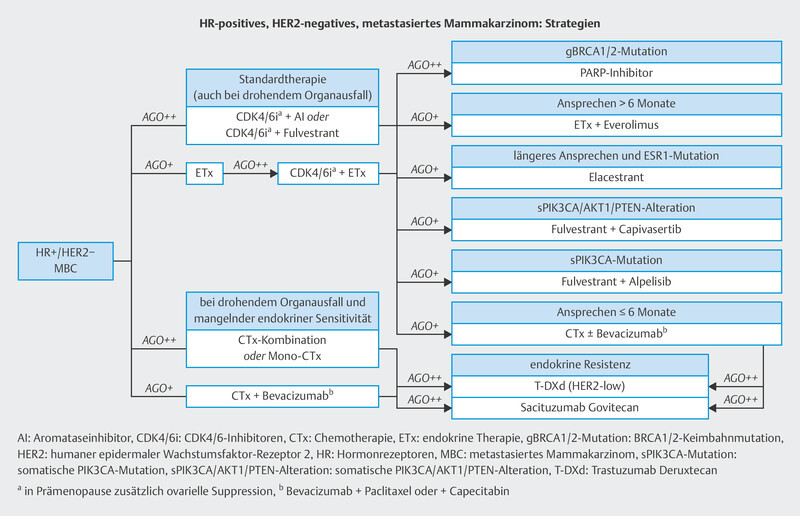
Which therapy sequence is best if a CDK4/6 inhibitor is administered as part of first-line therapy? With effective follow-up therapies (elacestrant, everolimus, alpelisib, PARP inhibitors, trastuzumab deruxtecan, sacituzumab govitecan) the question is what is the most effective therapy sequence. At the moment, the majority of patients undergoing second-line therapy still receive chemotherapy 24 . Could the new endocrine therapies change this approach and what is the significance of ADCs? Fig. 1 shows possible therapy sequences as assessed in national therapy recommendations ( https://www.ago-online.de/leitlinien-empfehlungen/leitlinien-empfehlungen/kommission-mamma , 25 ).
Fig. 1.
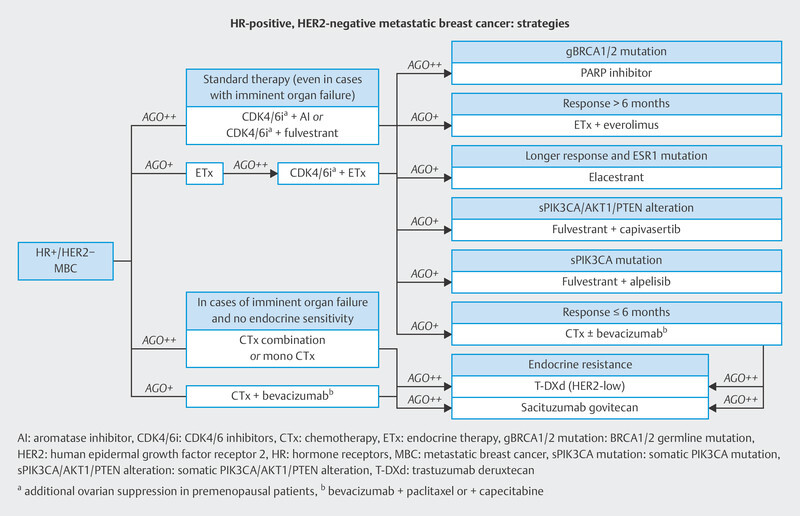
Treatment algorithm for patients with advanced HR+/HER2− disease 25 .
Chemotherapy – now the exception for first-line therapy of HR+/HER2+ ABC (advanced breast cancer) patients?
One therapeutic situation which comes up regularly when discussing whether chemotherapy is necessary is visceral crisis and/or constellations where remission is urgently needed (Question 43 to Question 46) . Up to now, the guidelines considered chemotherapy to be one of the standard options in this setting 26 . However, the presentation of the results from the phase II RIGHT Choice trial has changed the data by showing that endocrine-based therapy can also be a valid option as a first-line therapy for patients in urgent need of remission (Question 3) .
In the RIGHT Choice trial, the first-line therapy group also included patients with advanced HR+/HER2− breast cancer who had symptomatic visceral metastasis, were in visceral crisis, showed rapid disease progression, or had strong symptoms of non-visceral disease 27 . The patients were randomized either to therapy with ribociclib + letrozole (± goserelin) or to combination chemotherapy consisting of one of the following chemotherapies: docetaxel + capecitabine, paclitaxel + gemcitabine or capecitabine + vinorelbine. The primary study endpoint was PFS. Median PFS in the ribociclib arm was 24.0 months and therefore better than in the chemotherapy arm (12.3 months; HR = 0.54; 95% CI: 0.36 – 0.79; p = 0.007) 27 .
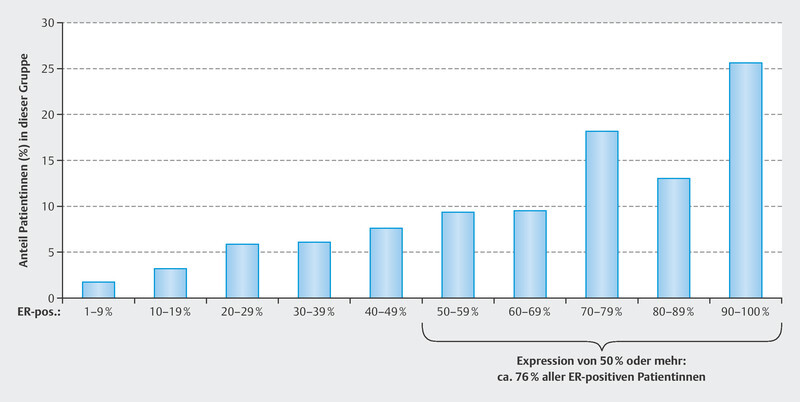
A recently updated analysis of the study noted that the percentage of patients with high ER (estrogen receptor) expression was relatively high. In the study, 79 – 91% of patients had an ER expression of 50% or more. It is possible that this reflects the normal distribution of ER expression. In a cohort from the USA, immunohistochemistry showed that 76% of ER-positive patients had an expression of 50% or more ( Fig. 2 ) 28 . Another anomaly of the RIGHT Choice trial was the young age of the patients. The median patient age in the study was 43 to 45 years 29 , whereas usually the mean age of HR+/HER2− patients with metastatic disease is 57 – 58 years when patients receive chemotherapy as their first-line treatment and about 61.5 years when they are treated with a CDK4/6 inhibitor 23 , 30 , 31 , 32 . The question that arises here is to what extent can the data of the RIGHT Choice trial be transferred to older patient populations. However, because of the clinical benefit of not carrying out chemotherapy, more than 95% of the ABC7 panelists voted to transpose the results also to postmenopausal patients and men (Question 3) .
Fig. 2.
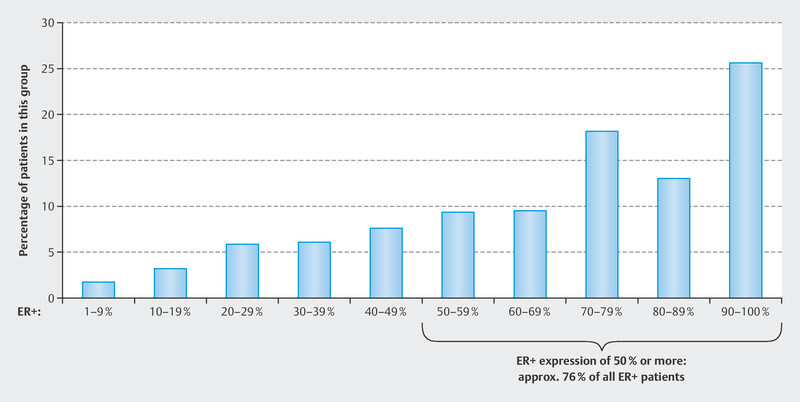
Distribution of ER expression in a cohort of breast cancer patients (Fig. is based on data from: Ma et al. 2013 28 ).
Optimization of CDK4/6 inhibitor use in different therapy lines
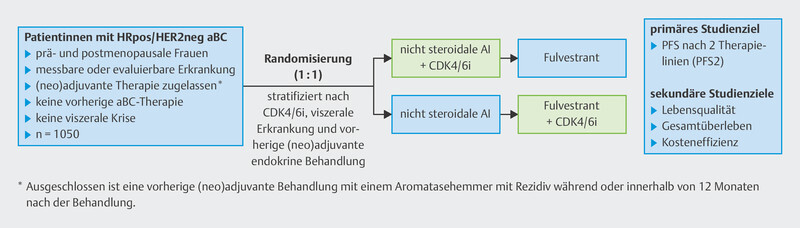
Even though the therapeutic standard now includes the use of CDK4/6 inhibitors as part of first-line therapy, some studies have focussed on later therapy lines and cohorts with higher levels of endocrine resistance (e.g., Monaleesa-3, Monarch-2 and Paloma 3 studies). In these therapeutic settings the addition of CDK4/6 inhibitors was found to be associated with good tumor control. Many treating physicians are of the opinion that it is important to have a therapy that is still effective for advanced lines of therapy. This is the context of the SONIA trial 33 . The SONIA trial was a randomized study which compared use of the CDK4/6 inhibitor palbociclib in the first and the second line of therapy ( Fig. 3 ). No differences were found with regards to OS.
Fig. 3.
Study design of SONIA trial (data from 33 ). PFS: progression-free survival; aBC: advanced breast cancer.
Since the vast majority of the participants in the SONIA study were treated with palbociclib and the Paloma-2 trial also found no difference in OS when it compared letrozole with palbociclib + letrozole 34 , the interpretation of the data is difficult and transferring the results of the SONIA trial is problematic. This was also reflected by the voting results of the ABC7 panelists. More than 93% viewed the inclusion of a CDK4/6 inhibitor into first-line therapy as the standard but were of the opinion that endocrine monotherapy was useful in exceptional situations (e.g., low tumor burden and problems with the availability of CDK4/6 inhibitors) (Question 4) .
Limited data on treatment beyond progression with CDK4/6 inhibitors
With combination therapies, the question always arises whether continuation of the therapy could be useful once disease has progressed if slight changes are then made to the therapy. Two phase II studies have been carried out for CDK4/6 inhibitors and data are available: the MAINTAIN trial 35 randomized patients with disease progression despite CDK4/6 inhibitor therapy 1 : 1 (n = 119) either into a therapy arm with ribociclib and an amended endocrine therapy (ET; continuation of CDK4/6 inhibitor therapy under ribociclib or switch to ribociclib) or a therapy arm consisting of monotherapy with ET alone. Continuation of the CDK4/6 inhibitor therapy was associated with longer median PFS (HR = 0.57; 95% CI: 0.39 – 0.95). The PACE trial addressed a similar question 36 . The PACE trial also included patients with disease progression under CDK4/6 inhibitor therapy. The patients were randomized into therapy with a) fulvestrant, b) fulvestrant + palbociclib, or c) fulvestrant + palbociclib + avelumab. When the 55 fulvestrant patients were compared with the 111 fulvestrant + palbociclib patients, no difference was found with regards to median PFS. The median PFS was similarly short for both arms with 4.8 and 4.6 months, respectively.
Given these data, more than 90% of ABC7 panelists considered therapy “beyond progression” to be unsuitable for clinical practice and recommended that such therapies should only be carried out in the context of clinical trials (Question 7) .
Elacestrant on the way to standard clinical practice?
With the new oral selective estrogen receptor degraders (SERDs), a number of new substances (elacestrant, giredestrant, imlunestrant, camizestrant, vepdegestrant) are currently undergoing clinical testing. Elacestrant has already been approved by the EMA (European Medicines Agency) and the FDA (U. S. Food and Drug Administration) for the treatment of patients with previously treated metastatic disease whose tumors have a missense mutation in the ESR1 gene, which codes for the estrogen receptor α. The approval of elacestrant is based on the EMERALD trial 37 . The improval in the median PFS in the EMERALD trial was only marginally significant for the total trial population. The median PFS was extended from 1.9 months to 2.8 months in the total population (HR = 0.70; 95% CI: 0.55 – 0.88) 37 . A bigger difference between the randomization arms was seen in the subgroup of patients with a tumor with ESR1 mutation (HR = 0.55; 95% CI: 0.39 – 0.77), while in the group of patients without ESR1 mutation the HR was 0.86 (95% CI: 0.63 – 1.19) 37 . The analysis found no OS benefit. Given these data, the vote by the ABC7 panel on whether elacestrant should be recommended for routine clinical use was divided. 51% of panelists were unable to make this recommendation whereas 44% were in favor (Question 10) ; nevertheless, the use of elacestrant was supported by more than 81% of panelists as a therapeutic option to treat tumors with ESR1 mutations as a second or third line of treatment (Question 11) .
Capivasertib and other endocrine therapies as linkers between early and late therapy lines
The AKT kinase inhibitor capivasertib has already been approved in the USA for patients with disease progression after prior endocrine therapy to treat tumors with a mutation in PIK3CA, AKT1 or PTEN . In the CAPITELLO-291 trial, capivasertib in combination with fulvestrant improved the median PFS of patients with a mutation in these genes from 3.1 months to 7.3 months (HR = 0.50; 95% CI: 0.38 – 0.65, p < 0.0001). The OS analysis also showed a promising improvement with a hazard ratio of 0.74 (95% CI: 0.56 – 0.98) 15 . The majority of patients had previously been treated with a CDK4/6 inhibitor. This approach could therefore become the standard therapy for this therapeutic setting. Other therapies which can be administered in this setting are chemotherapies, alpelisib, everolimus with endocrine therapy or the above-mentioned elacestrant in the presence of an ESR1 mutation.
Establishing effective endocrine or endocrine-based therapies after CDK4/6 inhibitor therapy which could then be used in clinical practice would constitute significant progress in the treatment of HR+/HER2− patients, as traditional chemotherapies are currently still the most commonly used therapies in this setting 24 . The current indication still requires the administration of chemotherapy before one of the effective ADCs trastuzumab deruxtecan or sacituzumab govitecan can be administered. The Destiny-Breast06 trial could change this situation 38 . The data of this study have not yet been published but their publication is expected in the near future. In the study trastuzumab deruxtecan are administered after two previous endocrine therapies. If this change is implemented, the most common therapy sequence would be CDK4/6i (CDK4/6inhibitor) → other endocrine-based therapy → ADC.
Antibody drug conjugates have arrived in clinical practice
With sacituzumab govitecan for patients with HR+/HER2− breast cancer or TNBC and trastuzumab deruxtecan for patients with HER2-positive and HER2-low-expressing tumors, two very effective ADCs are available to treat patients with advanced breast cancer. The administration of T-DXd is currently tied to the presence of HER2 expression (expression should be at least in the HER2-low range). In this context, 97.6% of participating ABC7 panelists proposed (Question 2) that pathologists should provide a detailed assessment of the patientʼs HER2 status using the following categories:
HER2-zero/null
HER2-low: 1+ or 2+/ISH (in situ hybridization) not-amplified
HER2-positive (ISH amplified or HER2 3+)
Although ADCs are associated with a higher incidence of side effects (hematological toxicity, nausea and vomiting, alopecia) and cases with interstitial lung disease (ILD) and fatal outcomes have been reported for T-DXd, the benefits with regards to OS were considered so significant that almost all of the panelists described sacituzumab govitecan and T-DXd as the preferred therapy option in the respective therapeutic setting (Question 12 and Question 13) . The panel was also of the opinion that the administration of trastuzumab deruxtecan in HR-pos/HER2-low disease before initiating treatment with sacituzumab govitecan was the better therapy sequence even though the data on sequencing is limited (Question 14) . The Destiny-Breast04 trial with T-DXd investigated patients in earlier therapy lines (after endocrine therapy and one to two chemotherapies) 39 , and the Tropics-02 trial 5 investigated the effect of sacituzumab govitecan in patients who had received at least two chemotherapies. Therapeutic monitoring is particularly important with regards to T-DXd. The ABC7 panelists were agreed that patients being treated with T-DXd should have a high-resolution CT scan for early detection of interstitial lung disease every six to eight weeks (Question 13) . If the CT scan detects asymptomatic ILD, treatment with T-DXd must be paused until this side effect has been fully resolved.
Other ADCs are already in the pipeline, for example, datopotamab deruxtecan (Dato-DXd) which targets Trop-2 in a similar fashion to sacituzumab govitecan and has the same payload as T-DXd. In a randomized study, HR+/HER2− patients with advanced breast cancer who had previously undergone one or two chemotherapies were analyzed to see whether Dato-DXd or chemotherapy was more effective 40 . The median PFS in this population with significant prior treatment was extended from 4.9 months to 6.9 months (HR = 0.63; 95% CI: 0.52 – 0.76), OS data are still pending 40 . The drug has not yet been approved and therefore currently does not play a role in the planning of therapy sequences.
Outlook for patients with HR+/HER2− advanced breast cancer
As the understanding of the resistance mechanisms in patients with advanced breast cancer has increased, more and more substances are being tested which are either being added to existing therapies or administered sequentially and offer additional benefits to patients. One example of this is the PI3K inhibitor inavolisib. The INAVO120 trial compared a combination of palbociclib, fulvestrant and inavolisib with a combination of palbociclib and fulvestrant. The combination with inavolisib showed a PFS benefit (HR = 0.43; 95% CI: 0.32 – 0.59). Even though the change in OS was not formally statisticially significant, the HR for the comparison was very promising (HR = 0.64; 95% CI: 0.43 – 0.97), the substance also appears to have a comparatively favorable side effect profile 16 . This agent is also not yet available for use in routine clinical practice.
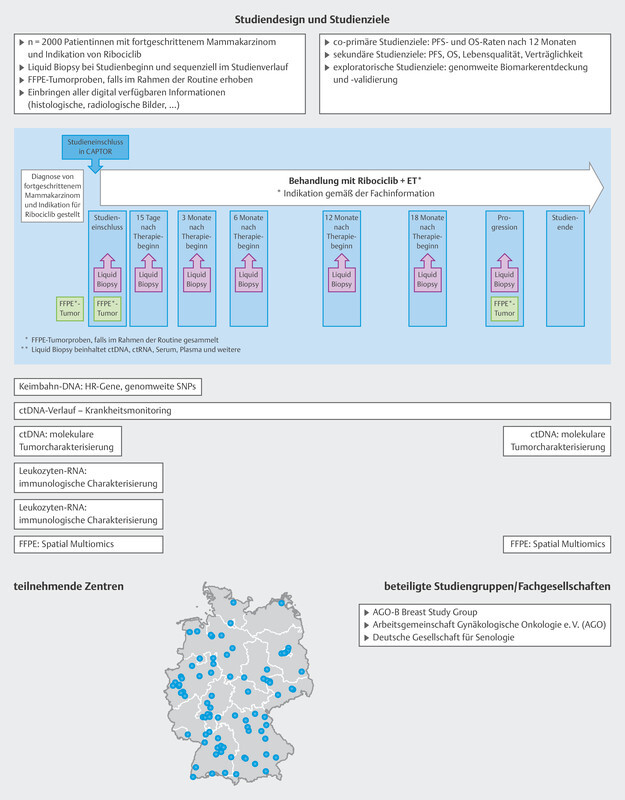
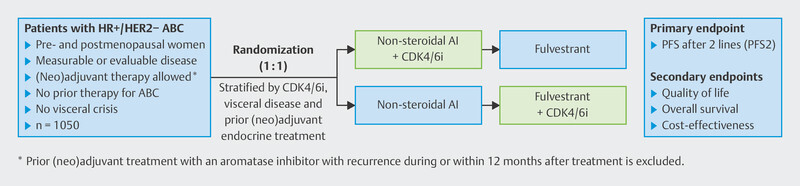
Some study programs are actively looking to understand endocrine resistance better during or after standard first-line therapy. The largest such program in Germany is the CAPTOR-BC trial 13 . More than 100 study centers across Germany have enrolled patients in the study who receive standard treatment with ribociclib and endocrine therapy as their first line of therapy. The effectivity and resistance mechanisms are being analyzed as part of an extensive translational study program ( Fig. 4 ).
Fig. 4.
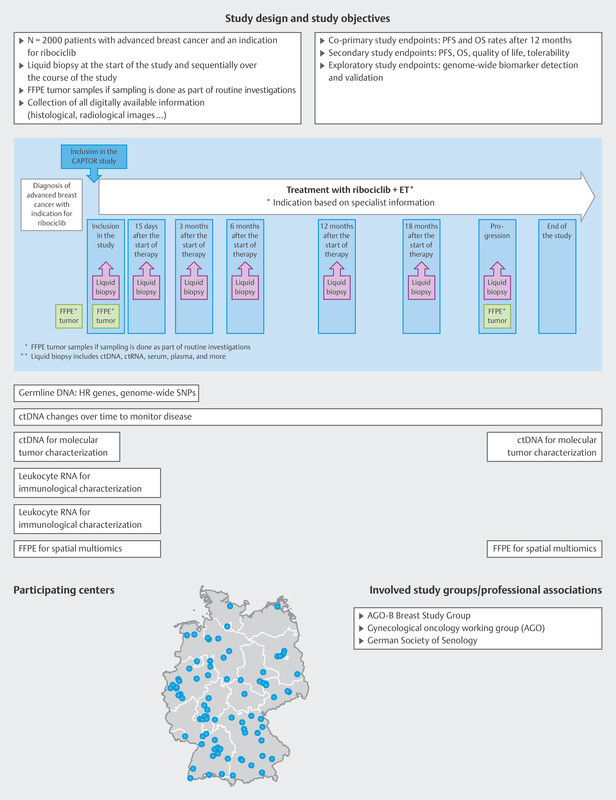
Study design of the CAPTOR-BC trial (from 13 ).
Treatment of Patients with Advanced HER2-positive Breast Cancer
Since the introduction of T-DXd 3 and tucatinib 41 , there have been no new therapies which have changed routine clinical treatment of patients with HER2-positive breast cancer. As these drugs are increasingly being administered in clinical practice, interest has focused on special therapeutic situations such as the treatment of brain metastases, a common occurrence with HER2-positive disease.
In the HER2CLIMB study, analysis of treatment of brain metastases was already planned in advance. A total of 291 patients with brain metastases were enrolled in the 2 : 1 randomized study, and were randomized either to the arm receiving tucatinib, capecitabine and trastuzumab or the arm treated with trastuzumab and capecitabine 42 . Median CNS (central nervous system)-related PFS improved with a hazard ratio of 0.32 (95% CI: 0.22 – 0.48) and OS improved with a hazard ratio of 0.58 (95% CI: 0.40 – 0.85). There was also a significant difference with regards to response to treatment between the two arms. In the tucatinib arm, 47.3% of patients achieved remission (41.8% had partial remission [PR] and 5.5% had complete remission [CR]), while this was only the case for 20% of patients in the arm without tucatinib (15% PR and 5% CR).
Recently, the results of patients with CNS involvement who were included in the DESTINY-Breast01–03 studies were presented 43 . As part of these trials, a total of 231 patients with brain metastases were treated with either T-DXd or chemotherapy. The rate of remission for both active and stable brain metastases was about 45% 43 (about 29% of cases had partial remission and 16% had complete remission).
Based on this data the overwhelming majority of ABC7 panelists considered T-DXd to be a therapeutic option for patients with brain metastases (Question 29) .
Treatment of Patients with Advanced Triple-negative Breast Cancer (TNBC)
What is the right therapy sequence for patients with triple-negative disease
Prior to the introduction of immune checkpoint inhibitors (cases with PD-L1 positivity in the first line of therapy), PARP inhibitors (cases with germline mutation in BRCA1/2 ) and the ADCs T-DXd and sacituzumab govitecan, the therapy landscape for patients with advanced triple-negative disease consisted of a sequence of chemotherapies. The fact that specialists are now discussing the optimal therapy sequence is the result of a number of positive studies carried out in recent years. Based on the currently available evidence, the introduction of ADCs in particular has raised a number of questions.
The ASCENT trial demonstrated a benefit from sacituzumab govitecan for patients who had a median of three previous chemotherapies. The benefit was evident not just for PFS but also for OS 6 . With 468 triple-negative disease patients in the trial, the randomized ASCENT trial is creating the basis for a high level of evidence. The Destiny-Breast04 trial also included a cohort of TNBC patients with HER2-low expression 39 . These patients had had a median of three previous therapies. A benefit with regards to PFS and OS was also evident for this small subpopulation of 68 patients 39 .
This raises the question of what the most beneficial sequence is. Most of the ABC7 panelists were of the opinion that the data showed that sacituzumab govitecan should be administered first when treating TNBC patients with HER2-low expression (Question 15) .
Special Therapy Situations
Oligometastasized disease
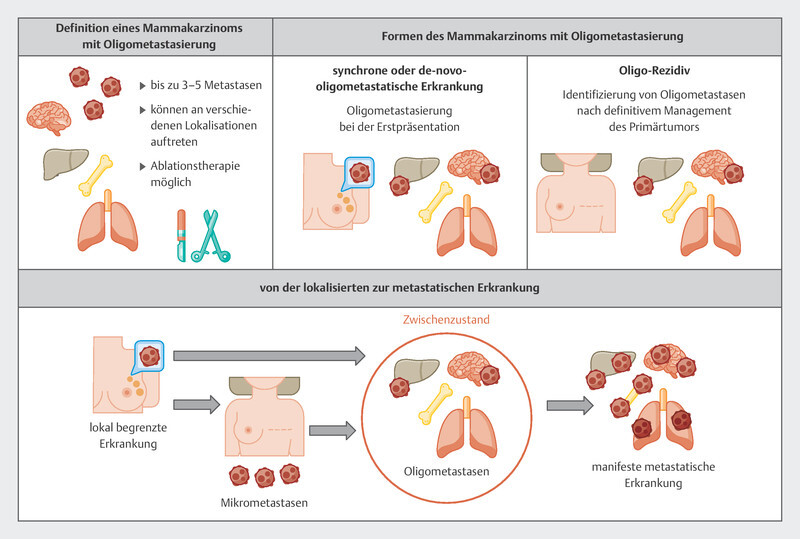
One issue which has preoccupied patients and treating physicians for decades is oligometastatic disease. The hypothesis that oligometastatic disease should be treated differently from manifest metastatic disease is based on the idea that if the number of metastases and the localizations of disease are limited, treatment in addition to standard systemic therapies could consist of local therapeutic procedures to treat the metastases. The background to this is the still speculative assumption that oligometastatic patients could be candidates for long-term remission or even cure. It is important to ensure that systemic therapies are not replaced by localized procedures. Most studies consider between three and five localized metastases as the maximum number to be still be termed oligometastatic disease. Fig. 5 provides an overview of the term and the concept of oligometastasis 44 . The evidence for local ablative procedures in this patient group is not high. There are two randomized studies, the NRG-BR002 and the SABR-COMET study, which have looked at this issue in recent years.
Fig. 5.
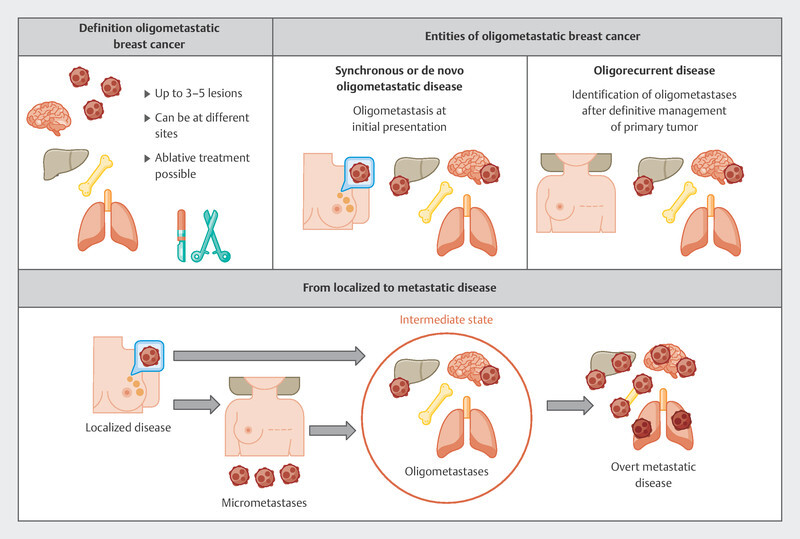
Summary of oligometastatic disease (data from 44 ).
The SABR-COMET study included cancer patients with between one and up to five metastases 45 . All of the metastases had to be treatable with stereotactic radiotherapy. A total of 99 patients were included in the study and randomized 2 : 1 to receive either stereotactic intervention or conventional palliative radiotherapy. A standard systemic therapy was administered in parallel. Eighteen patients with breast cancer participated in the study, of whom four in the stereotactic treatment arm survived for more than five years 45 .
The NRG-BR002 trial is a study which specifically focused on breast cancer patients 46 . This study enrolled patients with between one and four metastases who had controlled disease under first-line therapy. The 125 breast cancer patients were randomized 1 : 1 to stereotactic radiotherapy and/or surgical resection with continuation of systemic therapy or systemic therapy alone according to standard. This study was unable to show a benefit for local therapies with regards to PFS or OS 46 .
Given these limited data, the overwhelming majority of the ABC7 panelists rejected localized treatment of metastases as a standard therapy (Question 17) .
Removal of the primary tumor
A similar question arose in connection with resection of a primary tumor when disease has already metastasized. Of all the patients who present with metastasis, this situation (de-novo metastatic setting) occurs in about 50% of HER2-positive patients, 22% of triple-negative and 36% of HR+/HER2− patients 47 . It is well established with a high level of evidence that surgery of a primary tumor does not improve prognosis 54 . However, the use of this approach may be guided by patient preference and nursing aspects, meaning that, although prognosis will not improve, surgery may still be considered. Most of the panelists agreed (Question 18) .
Other special therapeutic situations
Other special therapeutic situations discussed at the conference were locally advanced inoperable breast cancer (Question 36 to Question 42) , visceral crisis (Question 43 to Question 46) and therapy of patients with HIV infection (Question 22 to Question 24) .
Other Topics
In addition to therapeutic situations, the internal and external circumstances which affect treatment and/or can affect the well-being of patients are also important. Some of these situations were also raised and discussed.
In recent years, wars have broken out in various crisis regions across the world which significantly negatively affect general medical care. This does not just apply to acute disease but also to chronic diseases such as advanced breast cancer 48 . All panelists were agreed that therapies can be adjusted to specific special situations and that colleagues in the respective crisis regions need to be supported (Question 19) .
Severe psychiatric disorders pose a particular challenge when treating patients. Some therapies have to be adapted accordingly. It is especially important to be aware of drug interactions 49 . Management of the therapies of patients with advanced breast cancer and additional comorbidities such as mental disorders should be planned proactively and carried out by an interdisciplinary team (Question 21) .
Pregnant women with advanced breast cancer continue to present very specific challenges. Some questions focused on this issue (Question 30 to Question 35) . While pregnancy during ongoing breast cancer therapy should be avoided with the appropriate contraception, the most common constellation for this group of patients is a new diagnosis of breast cancer in women who are already pregnant. Breast cancer tends to be in a more advanced stage of disease in these women compared to non-pregnant women 50 , 51 , 52 , 53 and is an interdisciplinary challege. The Expert Consensus Statements of the ESMO (European Society for Medical Oncology) 55 and the International Advisory Board of Cancer in Pregnancy ( www.ab-cip.org ) are relevant in this context.
Outlook
In recent years, therapies have been developed for all breast cancer subtypes (TNBC, HER2+, HR+/HER2−) which have led to an OS benefit for patients. Some of these therapies are accompanied by higher clinically relevant toxicity. As the longer survival times are accompanied by relevant toxicity profiles, the issue of maintaining patientsʼ quality of life has become particularly important. Some of the questions on this issue were also discussed (Question 27 and Question 28) . For example, it was proposed that measuring quality of life using patient-reported outcome tools could become part of routine clinical practice. This can be done using both classic paper-based methods and digital forms of data collection. It could help to move this important aspect more center stage during interactions between medical staff and patients. The conference participants also raised issues which require more research. These include treatment holidays and the therapeutic management of patients in long-term remission. Although there is not a lot of evidence from studies, pausing treatment is considered appropriate in certain cases although the situation requires a case-by-case decision. How long such treatment holidays can be and in which situations they are appropriate still needs to be defined and investigated further (Question 25 and Question 26) .
Irrespective of this, it can be stated that some of the therapies introduced in recent years are very effective and have contributed to an improvement in palliative treatment. To what extent the OS benefits will lead to lower overall mortality as a consequence of the therapeutic improvements for this group of patients still remains to be seen.
Acknowledgements
This work was partly the result of funding from the companies Gilead, Stemline Therapeutics, a part of the Menarini Group und onkowissen.de. None of the companies were involved in the compilation of the manuscript or contributed to any recommendations in the manuscript. The authors are solely responsible for the contents of the manuscript.
Danksagung
Diese Arbeit entstand teilweise in Folge von Förderungen der Firmen Gilead, Stemline Therapeutics, a part of the Menarini Group, und onkowissen.de. Keine der Firmen hatte einen Anteil an der Erstellung und den Empfehlungen dieses Manuskriptes. Für den Inhalt des Manuskriptes sind ausschließlich die Autoren verantwortlich.
Footnotes
Conflict of Interest/Interessenkonflikt B. A. received honoria and travel grants from AstraZeneca, Gilead, Genomic Health, Roche, Novartis, GSK, Stemline, Lilly, MSD, Eisai, Tesaro, Daiichi Sankyo and Pfizer. M. B.-P. received honoraria for lectures and advisory role from Roche, Novartis, Pfizer, pfm, Eli Lilly, Onkowissen, Seagen, Eisai, AstraZeneca, Amgen, Samsung, MSD, GSK, Daiichi Sankyo, Gilead, Sirius Pintuition, Pierre Fabre, and study support from Mammotome, Endomag and Merit Medical. E. B. received honoraria from Gilead, Ipsen, Sanofi, Sandoz, SunPharma, AstraZeneca, Novartis, Hexal, BMS, Lilly, Pfizer, Roche, MSD, BBraun and onkowissen.de for clinical research management and/or medical education activities. N. D. has received honoraria from MSD, Roche, AstraZeneca, Teva, Pfizer, Novartis, Seagen,Gilead, MCI Healthcare. P. A. F. received honoraria from Novartis, Pfizer, Roche, Amgen, Celgene, onkowissen.de, Daiichi Sankyo, AstraZeneca, Merck-Sharp & Dohme, Eisai, Puma and Teva. His institution conducts research with funding from Novartis and Biontech. T. N. F. has participated on advisory boards for Amgen, Daiichi Sankyo, Novartis, Pfizer, and Roche and has received honoraria for lectures from Amgen, Celgene, Daiichi Sankyo, Roche, Novartis and Pfizer. A. D. H. received speaker and consultancy honoraria from AstraZeneca, Genomic Health, Roche, Novartis, Celgene, Lilly, MSD, Eisai, Teva, Tesaro, Daiichi Sankyo, Hexal and Pfizer. M. H. has no conflict of interest. N. H. received honoraria for lectures and/or consulting from AstraZeneca, Daiichi Sankyo, Gilead, Lilly, MSD, Novartis, Pierre-Fabre, Pfizer, Roche, Sandoz, Seagen. W. J. has received research Grants and/or honoraria from Sanofi-Aventis, Daiichi Sankyo, Novartis, Roche, Pfizer, Lilly, AstraZeneca, Chugai, GSK, Eisai, Cellgene and Johnson & Johnson. A. K. has no conflict of interest. H.-C. K. has received honoraria from Pfizer, Seagen, Novartis, Roche, Genomic Health/Exact Sciences, Amgen, AstraZeneca, Riemser, Carl Zeiss Meditec, Teva, Theraclion, Janssen-Cilag, GSK, LIV Pharma, Lilly, SurgVision, Onkowissen, Gilead, Daiichi Sankyo, Zuellgen Pharma and MSD, travel support from Carl Zeiss Meditec, LIV Pharma, Novartis, Amgen, Pfizer, Daiichi Sankyo, Tesaro and owns stock of Theraclion SA. D. L. received honoraria from Amgen, AstraZeneca, Daiichi Sankyo, Eli Lilly, Exact Sciences, High5md, Gilead, GSK, Loreal, MSD, Novartis, Onkowissen, Pierre Fabre, Pfizer, Roche, Seagen, Teva. M. P. L. has participated on advisory boards for AstraZeneca, Lilly, MSD, Novartis, Pfizer, Eisai, Gilead, Exact Sciences, Grünenthal, Daiichi Sankyo and Roche and has received honoraria for lectures from MSD, Lilly, Roche, Novartis, Pfizer, Exact Sciences, Daiichi Sankyo, Grünenthal, Gilead, AstraZeneca, and Eisai. He received travel expenses from Pfizer, AstraZeneca and Daiichi-Sankyo. V. M. received speaker honoraria from Amgen, AstraZeneca, Daiichi Sankyo, Eisai, GSK, Pfizer, MSD, Medac, Novartis, Roche, Teva, Seagen, Onkowissen, high5 Oncology, Medscape, Gilead. Consultancy honoraria from Hexal, Roche, Pierre Fabre, Amgen, ClinSol, Novartis, MSD, Daiichi Sankyo, Eisai, Lilly, Sanofi, Seagen, Gilead. Institutional research support from Novartis, Roche, Seagen, Genentech. Travel grants: Roche, Pfizer, Daiichi Sankyo. E. S. received honoraria from Roche, Celgene, AstraZeneca, Novartis, Pfizer, Tesaro, Aurikamed GmbH, Pfizer, Seagen, Pierre Fabre, MCI Deutschland GmbH, bsh medical communications GmbH, Onkowissen TV. A. S. received research grants from Celgene, Roche, honoraria from Amgen, AstraZeneca, Aurikamed, Bayer, Celgene, Clinsol, Connectmedica, Gilead, GSK, I-MED, Lilly, MCI Deutschland, Metaplan, MSD, Nanostring, Novartis, Onkowissen.de, Promedicis, Pfizer, Pierre Fabre, Roche, Seagen, Streamedup, Teva, Tesaro, Thieme and travel support from Celgene, Pfizer, Roche. F. S. participated on advisory boards for Novartis, Lilly, Amgen and Roche and received honoraria for lectures from Roche, AstraZeneca, MSD, Novartis and Pfizer. H. T. received honoraria from Novartis, Roche, Celgene, Teva, Pfizer, AstraZeneca and travel support from Roche, Celgene and Pfizer. C. T. received honoraria for advisory boards and lectures from Amgen, AstraZeneca, Celgene, Daiichi Sankyo, Eisai, Gilead, Lilly, MSD, Mylan, Nanostring, Novartis, Pfizer, Pierre Fabre, Puma, Roche, Seagen, Vifor. M. T. has participated on advisory boards for AstraZeneca, Clovis, Daiichi Sankyo, Eisai, Gilead Science, GSK, Lilly, MSD, Novartis, Organon, Pfizer, Pierre-Fabre, Seagen and Roche and has received honoraria for lectures from Amgen, Clovis, Daiichi Sankyo, Eisai, GSK, Lilly, MSD, Roche, Novartis, Organon, Pfizer, Seagen, Exact Sciences, Viatris, Vifor and AstraZeneca and has received trial funding by Exact Sciences and Endomag Manuscript support was done by Amgen, ClearCut, pfm medical, Roche, Servier, Vifor. M. U. all honoraria went to the institution/employer: Abbvie, Amgen, AstraZeneca, Daiichi Sankyo, Eisai, Lilly, MSD, Myriad Genetics, Pfizer, Roche, Sanofi Aventis, Novartis, Pierre Fabre, Seagen; Gilead. M. W. has participated on advisory boards for AstraZeneca, Lilly, MSD, Novartis, Pfizer and Roche. I. W. has participated on advisory boards for Novartis, Daiichi Sankyo, Lilly, Pfizer and received speaker honoraria from AstraZeneca, Daiichi Sankyo, MSD, Novartis, Pfizer, Roche. A. W. participated on advisory boards for Novartis, Lilly, Amgen, Pfizer, Roche, Tesaro, Eisai and received honoraria for lectures from Novartis, Pfizer, Aurikamed, Roche, Celgene. R. B. has received honoraria from Astra-Zeneca, Daiichi, Eisai, Eli-Lilly, Gilead, Gruenenthal, MSD, Novartis, Pfizer, Pierre-Fabre, Puma, Roche, Seagen, Stemline, travel support from Astra Zeneca, Daiichi, MSD, Lilly, Novartis, and grants from Daiichi and MSD. R. W. has received honoraria, travel support from Agendia, Amgen, Aristo, AstraZeneca, Boeringer Ingelheim, Carl Zeiss, Celgene, Daiichi Sankyo, Eisai, Exact Sciences, Genomic Health, Gilead, GlaxoSmithKline, Hexal, Lilly, Medstrom Medical, MSD, Mundipharma, Mylan, Nanostring, Novartis, Odonate, Paxman, Palleos, Pfizer, Pierre Fabre, Puma Biotechnology, Riemser, Roche, Sandoz/Hexal, Sanofi Genzyme, Seattle Genetics/Seagen, Tesaro Bio, Teva, Veracyte, Viatris. The other authors have no conflict of interest to declare for this specific work./ B. A. erhielt Honorare und und Reisekosten von AstraZeneca, Gilead, Genomic Health, Roche, Novartis, GSK, Stemline, Lilly, MSD, Eisai, Tesaro, Daiichi Sankyo und Pfizer. M. B.-P. erhielt Vortragshonorare und Beraterhonorare von Roche, Novartis, Pfizer, pfm, Eli Lilly, Onkowissen, Seagen, Eisai, AstraZeneca, Amgen, Samsung, MSD, GSK, Daiichi Sankyo, Gilead, Sirius Pintuition, Pierre Fabre, und Forschungsförderung von Mammotome, Endomag und Merit Medical. E. B. erhielt Honorare von Gilead, Ipsen, Sanofi, Sandoz, SunPharma, AstraZeneca, Novartis, Hexal, BMS, Lilly, Pfizer, Roche, MSD, B. Braun und onkowissen.de für klinisches Forschungsmanagement und/oder medizinische Fortbildungsaktivitäten. N. D. erhielt Honorare von MSD, Roche, AstraZeneca, Teva, Pfizer, Novartis, Seagen, Gilead, MCI Healthcare. P. A. F. erhielt Honorare von Novartis, Pfizer, Roche, Amgen, Celgene, onkowissen.de, Daiichi Sankyo, AstraZeneca, Merck Sharp & Dohme, Eisai, Puma und Teva. Seine Institution betreibt Forschung mit Unterstützung von Novartis und BioNtech. T. N. F. hat in Beiräten mitgewirkt für Amgen, Daiichi Sankyo, Novartis, Pfizer und Roche und erhielt Vortragshonorare von Amgen, Celgene, Daiichi Sankyo, Roche, Novartis und Pfizer. A. D. H. erhielt Sprecher- und Beraterhonorare von AstraZeneca, Genomic Health, Roche, Novartis, Celgene, Lilly, MSD, Eisai, Teva, Tesaro, Daiichi Sankyo, Hexal und Pfizer. M. H. hat keine Interessenkonflikte zu melden. N. H. erhielt Vortragshonorare und/oder Honorare für Beratertätigkeiten von AstraZeneca, Daiichi Sankyo, Gilead, Lilly, MSD, Novartis, Pierre-Fabre, Pfizer, Roche, Sandoz, Seagen. W. J. erhielt Forschungsstipendien und/oder Honorare von Sanofi Aventis, Daiichi Sankyo, Novartis, Roche, Pfizer, Lilly, AstraZeneca, Chugai, GSK, Eisai, Cellgene und Johnson & Johnson. A. K. hat keine Interessenkonflikte zu melden. H.-C. K. erhielt Honorare von Pfizer, Seagen, Novartis, Roche, Genomic Health/Exact Sciences, Amgen, AstraZeneca, Riemser, Carl Zeiss Meditec, Teva, Theraclion, Janssen-Cilag, GSK, LIV Pharma, Lilly, SurgVision, Onkowissen, Gilead, Daiichi Sankyo, Zuellgen Pharma und MSD; Reisekostenzuschüsse von Carl Zeiss Meditec, LIV Pharma, Novartis, Amgen, Pfizer, Daiichi Sankyo, Tesaro; und besitzt Aktien von Theraclion SA. D. L. erhielt Honorare von Amgen, AstraZeneca, Daiichi Sankyo, Eli Lilly, Exact Sciences, High5md, Gilead, GSK, Loreal, MSD, Novartis, Onkowissen, Pierre Fabre, Pfizer, Roche, Seagen, Teva. M. P. L. hat in Beiräten mitgewirkt für AstraZeneca, Lilly, MSD, Novartis, Pfizer, Eisai, Gilead, Exact Sciences, Grünenthal, Daiichi Sankyo und Roche und erhielt Vortragshonorare von MSD, Lilly, Roche, Novartis, Pfizer, Exact Sciences, Daiichi Sankyo, Grünenthal, Gilead, AstraZeneca und Eisai; Reisekostenzuschüsse von Pfizer, AstraZeneca und Daiichi-Sankyo. V. M. erhielt Sprecherhonorare von Amgen, AstraZeneca, Daiichi Sankyo, Eisai, GSK, Pfizer, MSD, Medac, Novartis, Roche, Teva, Seagen, Onkowissen, high5 Oncology, Medscape, Gilead; Beraterhonorare von Hexal, Roche, Pierre Fabre, Amgen, ClinSol, Novartis, MSD, Daiichi Sankyo, Eisai, Lilly, Sanofi, Seagen, Gilead; institutionelle Forschungsförderung von Novartis, Roche, Seagen, Genentech; Reisekostenzuschüsse von Roche, Pfizer, Daiichi Sankyo. E. S. erhielt Honorare von Roche, Celgene, AstraZeneca, Novartis, Pfizer, Tesaro, Aurikamed GmbH, Pfizer, Seagen, Pierre Fabre, MCI Deutschland GmbH, bsh medical communications GmbH, Onkowissen TV. A. S. erhielt Forschungsstipendien von Celgene, Roche, Honorare von Amgen, AstraZeneca, Aurikamed, Bayer, Celgene, Clinsol, Connectmedica, Gilead, GSK, I-MED, Lilly, MCI Deutschland, Metaplan, MSD, Nanostring, Novartis, Onkowissen.de, Promedicis, Pfizer, Pierre Fabre, Roche, Seagen, Streamedup, Teva, Tesaro, Thieme und Reisekostenzuschüsse von Celgene, Pfizer, Roche. F. S. hat in Beiräten mitgewirkt für Novartis, Lilly, Amgen and Roche und erhielt Vortragshonorare von Roche, AstraZeneca, MSD, Novartis und Pfizer. H. T. erhielt Honorare von Novartis, Roche, Celgene, Teva, Pfizer, AstraZeneca und Reisekostenzuschüsse von Roche, Celgene and Pfizer. C. T. erhielt Honorare für die Teilnahme an Beiräten und für Vorträge von Amgen, AstraZeneca, Celgene, Daiichi Sankyo, Eisai, Gilead, Lilly, MSD, Mylan, Nanostring, Novartis, Pfizer, Pierre Fabre, Puma, Roche, Seagen, Vifor. M. T. hat in Beiräten mitgewirkt für AstraZeneca, Clovis, Daiichi Sankyo, Eisai, Gilead Science, GSK, Lilly, MSD, Novartis, Organon, Pfizer, Pierre-Fabre, Seagen und Roche; erhielt Vortragshonorare von Amgen, Clovis, Daiichi Sankyo, Eisai, GSK, Lilly, MSD, Roche, Novartis, Organon, Pfizer, Seagen, Exact Sciences, Viatris, Vifor und AstraZeneca; erhielt Studienfinanzierung von Exact Sciences and Endomag; Unterstützung für das Manuskript kam von Amgen, ClearCut, pfm medical, Roche, Servier, Vifor. M. U. Alle Honorare wurden an die Institution/den Arbeitergeber abgeführt: Abbvie, Amgen, AstraZeneca, Daiichi Sankyo, Eisai, Lilly, MSD, Myriad Genetics, Pfizer, Roche, Sanofi Aventis, Novartis, Pierre Fabre, Seagen, Gilead. M. W. hat in Beiräten mitgewirkt für AstraZeneca, Lilly, MSD, Novartis, Pfizer und Roche. I. W. hat in Beiräten mitgewirkt für Novartis, Daiichi Sankyo, Lilly, Pfizer und erhielt Sprecherhonorare von AstraZeneca, Daiichi Sankyo, MSD, Novartis, Pfizer, Roche. A. W. hat in Beiräten mitgewirkt für Novartis, Lilly, Amgen, Pfizer, Roche, Tesaro, Eisai und erhielt Vortragshonorare von Novartis, Pfizer, Aurikamed, Roche, Celgene. R. B. erhielt Honorare von Astra-Zeneca, Daiichi, Eisai, Eli-Lilly, Gilead, Gruenenthal, MSD, Novartis, Pfizer, Pierre-Fabre, Puma, Roche, Seagen, Stemline; Reisekostenzuschüsse von Astra Zeneca, Daiichi, MSD, Lilly, Novartis und Forschungszuschüsse von Daiichi und MSD. R. W. erhielt Honorare und Reisekostenzuschüsse von Agendia, Amgen, Aristo, AstraZeneca, Boeringer Ingelheim, Carl Zeiss, Celgene, Daiichi Sankyo, Eisai, Exact Sciences, Genomic Health, Gilead, GlaxoSmithKline, Hexal, Lilly, Medstrom Medical, MSD, Mundipharma, Mylan, Nanostring, Novartis, Odonate, Paxman, Palleos, Pfizer, Pierre Fabre, Puma Biotechnology, Riemser, Roche, Sandoz/Hexal, Sanofi Genzyme, Seattle Genetics/Seagen, Tesaro Bio, Teva, Veracyte, Viatris. Die anderen Autoren und Autorinnen haben keine Interessenkonflikte zu melden.
Supplement
• Supplement Tab. S1: Panelists of ABC7 conference.
• Supplement Tab. S2: Questions voted on by the ABC7 panelists. Because voting was done live, the list does not claim to be complete. The questions have been numbered to match the text of this article. The numbering was not specified during the ABC7 conference.
Supplement
• Supplement Tab. S1: Panelisten der ABC7-Konferenz.
• Supplement Tab. S2: Fragen der Abstimmung unter den ABC7-Panelisten. Wegen des Live-Charakters der Abstimmungen besteht kein Anspruch auf Vollständigkeit. Die Fragen sind nummeriert zum Text dieses Artikels. Die Nummerierung war keine Vorgabe der ABC7-Konferenz.
References/Literatur
- 1.Diéras V, Miles D, Verma S et al. Trastuzumab emtansine versus capecitabine plus lapatinib in patients with previously treated HER2-positive advanced breast cancer (EMILIA): a descriptive analysis of final overall survival results from a randomised, open-label, phase 3 trial. Lancet Oncol. 2017;18:732–742. doi: 10.1016/S1470-2045(17)30312-1. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Verma S, Miles D, Gianni L et al. Trastuzumab emtansine for HER2-positive advanced breast cancer. N Engl J Med. 2012;367:1783–1791. doi: 10.1056/NEJMoa1209124. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Cortés J, Kim S-B, Chung W-P et al. Trastuzumab deruxtecan versus trastuzumab emtansine for breast cancer. N Engl J Med. 2022;386:1143–1154. doi: 10.1056/NEJMoa2115022. [DOI] [PubMed] [Google Scholar]
- 4.Modi S, Saura C, Yamashita T et al. Trastuzumab deruxtecan in previously treated HER2-positive breast cancer. N Engl J Med. 2020;382:610–621. doi: 10.1056/NEJMoa1914510. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Rugo H S, Bardia A, Marmé F et al. Overall survival with sacituzumab govitecan in hormone receptor-positive and human epidermal growth factor receptor 2-negative metastatic breast cancer (TROPiCS-02): a randomised, open-label, multicentre, phase 3 trial. Lancet. 2023;402:1423–1433. doi: 10.1016/S0140-6736(23)01245-X. [DOI] [PubMed] [Google Scholar]
- 6.Bardia A, Hurvitz S A, Tolaney S M et al. Sacituzumab govitecan in metastatic triple-negative breast cancer. N Engl J Med. 2021;384:1529–1541. doi: 10.1056/NEJMoa2028485. [DOI] [PubMed] [Google Scholar]
- 7.Cortes J, Cescon D W, Rugo H S et al. Pembrolizumab plus chemotherapy versus placebo plus chemotherapy for previously untreated locally recurrent inoperable or metastatic triple-negative breast cancer (KEYNOTE-355): a randomised, placebo-controlled, double-blind, phase 3 clinical trial. Lancet. 2020;396:1817–1828. doi: 10.1016/S0140-6736(20)32531-9. [DOI] [PubMed] [Google Scholar]
- 8.Cortes J, Rugo H S, Cescon D W et al. Pembrolizumab plus Chemotherapy in Advanced Triple-Negative Breast Cancer. N Engl J Med. 2022;387:217–226. doi: 10.1056/NEJMoa2202809. [DOI] [PubMed] [Google Scholar]
- 9.Rugo H S, Loi S, Adams S et al. Performance of PD-L1 immunohistochemistry (IHC) assays in unresectable locally advanced or metastatic triple-negative breast cancer (mTNBC): Post-hoc analysis of IMpassion130. Ann Oncol. 2019;30:v858–v859. [Google Scholar]
- 10.Schmid P, Adams S, Rugo H S et al. Atezolizumab and nab-paclitaxel in advanced triple-negative breast cancer. N Engl J Med. 2018;379:2108–2121. doi: 10.1056/NEJMoa1809615. [DOI] [PubMed] [Google Scholar]
- 11.Schmid P, Rugo H S, Adams S et al. Atezolizumab plus nab-paclitaxel as first-line treatment for unresectable, locally advanced or metastatic triple-negative breast cancer (IMpassion130): updated efficacy results from a randomised, double-blind, placebo-controlled, phase 3 trial. Lancet Oncol. 2020;21:44–59. doi: 10.1016/S1470-2045(19)30689-8. [DOI] [PubMed] [Google Scholar]
- 12.Miles D, Gligorov J, André F et al. Primary results from IMpassion131, a double-blind, placebo-controlled, randomised phase III trial of first-line paclitaxel with or without atezolizumab for unresectable locally advanced/metastatic triple-negative breast cancer. Ann Oncol. 2021;32:994–1004. doi: 10.1016/j.annonc.2021.05.801. [DOI] [PubMed] [Google Scholar]
- 13.Schneeweiss A, Brucker S Y, Hübner H C et al. CDK4/6 Inhibition – Therapy Sequences and the Quest for Finding the Best Biomarkers – an Overview of Current Programs. Geburtshilfe Frauenheilkd. 2024 doi: 10.1055/a-2286-6066. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Nabieva N, Fasching P A. CDK4/6 Inhibitors–Overcoming Endocrine Resistance Is the Standard in Patients with Hormone Receptor-Positive Breast Cancer. Cancers. 2023;15:1763. doi: 10.3390/cancers15061763. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Turner N C, Oliveira M, Howell S J et al. Capivasertib in hormone receptor–positive advanced breast cancer. N Engl J Med. 2023;388:2058–2070. doi: 10.1056/NEJMoa2214131. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Jhaveri K, Im S-A, Saura C et al. Inavolisib or placebo in combination with palbociclib and fulvestrant in patients with PIK3CA-mutated, hormone receptor-positive, HER2-negative locally advanced or metastatic breast cancer: Phase III, INAVO120 primary analysis. Proceedings of the 2023 San Antonio Breast Cancer Symposium, San Antonio, TX, USA. 2023;2023:5–9. [Google Scholar]
- 17.Litton J K, Rugo H S, Ettl J et al. Talazoparib in patients with advanced breast cancer and a germline BRCA mutation. N Engl J Med. 2018;379:753–763. doi: 10.1056/NEJMoa1802905. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Turner N C, Telli M L, Rugo H S et al. A phase II study of talazoparib after platinum or cytotoxic nonplatinum regimens in patients with advanced breast cancer and germline BRCA1/2 mutations (ABRAZO) Clin Cancer Res. 2019;25:2717–2724. doi: 10.1158/1078-0432.CCR-18-1891. [DOI] [PubMed] [Google Scholar]
- 19.Hurvitz S, Quek R, Turner N et al. Quality of life with talazoparib after platinum or multiple cytotoxic non-platinum regimens in patients with advanced breast cancer and germline BRCA1/2 mutations: patient-reported outcomes from the ABRAZO phase 2 trial. Eur J Cancer. 2018;104:160–168. doi: 10.1016/j.ejca.2018.09.003. [DOI] [PubMed] [Google Scholar]
- 20.Robson M, Im S-A, Senkus E et al. Olaparib for metastatic breast cancer in patients with a germline BRCA mutation. N Engl J Med. 2017;377:523–533. doi: 10.1056/NEJMoa1706450. [DOI] [PubMed] [Google Scholar]
- 21.Ettl J, Quek R, Lee K-H et al. Quality of life with talazoparib versus physicianʼs choice of chemotherapy in patients with advanced breast cancer and germline BRCA1/2 mutation: patient-reported outcomes from the EMBRACA phase III trial. Ann Oncol. 2018;29:1939–1947. doi: 10.1093/annonc/mdy257. [DOI] [PubMed] [Google Scholar]
- 22.Robson M, Ruddy K J, Seock-Ah I et al. Patient-reported outcomes in patients with a germline BRCA mutation and HER2-negative metastatic breast cancer receiving olaparib versus chemotherapy in the OlympiAD trial. Eur J Cancer. 2019;120:20–30. doi: 10.1016/j.ejca.2019.06.023. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.Engler T, Fasching P A, Lüftner D et al. Implementation of CDK4/6 Inhibitors and its Influence on the Treatment Landscape of Advanced Breast Cancer Patients–Data from the Real-World Registry PRAEGNANT. Geburtshilfe Frauenheilkd. 2022;82:1055–1067. doi: 10.1055/a-1880-0087. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.Braun M SO, Salat C et al. Current therapy landscape of advanced HER2 negative breast cancer in pateints in a network of office based internistic oncologists and gynecologic oncologists in Germany. Deutscher Krebskongress. 2022;2022:Abstr.. 306. [Google Scholar]
- 25.AGO Kommission Mamma Diagnostik und Therapie früher und fortgeschrittener Mammakarzinome: Therapiealgorithmen 2024. Online (Stand: 25.03.2024):https://www.ago-online.de/leitlinien-empfehlungen/leitlinien-empfehlungen/kommission-mamma
- 26.Cardoso F, Paluch-Shimon S, Senkus E et al. 5th ESO-ESMO international consensus guidelines for advanced breast cancer (ABC5) Ann Oncol. 2020;31:1623–1649. doi: 10.1016/j.annonc.2020.09.010. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27.Lu Y-S, Mahidin E IBM, Azim H Primary results from the randomized Phase II RIGHT Choice trial of premenopausal patients with aggressive HR+/HER2− advanced breast cancer treated with ribociclib + endocrine therapy vs physician’s choice combination chemotherapy. Presented at SABCS 2022. December 6–10, 2022. Abstract GS1-10
- 28.Ma H, Lu Y, Marchbanks P A et al. Quantitative measures of estrogen receptor expression in relation to breast cancer-specific mortality risk among white women and black women. Breast Cancer Res. 2013;15:1–12. doi: 10.1186/bcr3486. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29.Azim H, El Saghir N, Yap Y et al. 402P First-line ribociclib (RIB)+ endocrine therapy (ET) vs. combination chemotherapy (combo CT) in aggressive HR+/HER2− advanced breast cancer (ABC): A subgroup analysis of patients (pts) with or without visceral crisis from the phase II RIGHT choice study. Ann Oncol. 2023;34:S350–S351. [Google Scholar]
- 30.Schneeweiss A, Ettl J, Lüftner D et al. Initial experience with CDK4/6 inhibitor-based therapies compared to antihormone monotherapies in routine clinical use in patients with hormone receptor positive, HER2 negative breast cancer–Data from the PRAEGNANT research network for the first 2 years of drug availability in Germany. Breast. 2020;54:88–95. doi: 10.1016/j.breast.2020.08.011. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 31.Fasching P A, Yadav S, Hu C et al. Mutations in BRCA1/2 and other panel genes in patients with metastatic breast cancer–Association with patient and disease characteristics and effect on prognosis. J Clin Oncol. 2021;39:1619. doi: 10.1200/JCO.20.01200. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 32.Hartkopf A D, Huober J, Volz B et al. Treatment landscape of advanced breast cancer patients with hormone receptor positive HER2 negative tumors–Data from the German PRAEGNANT breast cancer registry. Breast. 2018;37:42–51. doi: 10.1016/j.breast.2017.10.002. [DOI] [PubMed] [Google Scholar]
- 33.Sonke G S, Van Ommen-Nijhof A, Wortelboer Net al. Primary outcome analysis of the phase 3 SONIA trial (BOOG 2017-03) on selecting the optimal position of cyclin-dependent kinases 4 and 6 (CDK4/6) inhibitors for patients with hormone receptor-positive (HR+), HER2-negative (HER2-) advanced breast cancer (ABC) JCO 202341(Suppl.)LBA1000. 10.1200/JCO.2023.41.17_suppl.LBA1000 [DOI] [Google Scholar]
- 34.Finn R S, Rugo H S, Dieras V Cet al. Overall survival (OS) with first-line palbociclib plus letrozole (PAL+LET) versus placebo plus letrozole (PBO+LET) in women with estrogen receptor–positive/human epidermal growth factor receptor 2–negative advanced breast cancer (ER+/HER2− ABC): Analyses from PALOMA-2 JCO 202240(Suppl.)LBA1003. 10.1200/JCO.2022.40.17_suppl.LBA1003 [DOI] [Google Scholar]
- 35.Kalinsky K, Accordino M K, Chiuzan C et al. Randomized phase II trial of endocrine therapy with or without ribociclib after progression on cyclin-dependent kinase 4/6 inhibition in hormone receptor–positive, human epidermal growth factor receptor 2–negative metastatic breast cancer: Maintain trial. J Clin Oncol. 2023;41:4004–4013. doi: 10.1200/JCO.22.02392. [DOI] [PubMed] [Google Scholar]
- 36.Mayer E L, Ren Y, Wagle N et al. Abstract Gs3-06: Gs3-06 Palbociclib after Cdk4/6I and endocrine therapy (PACE): A randomized phase II study of Fulvestrant, Palbociclib, and Avelumab for endocrine pre-treated ER+/Her2-metastatic breast cancer. Cancer Res. 2023;83(5_Supplement):GS3-06. [Google Scholar]
- 37.Bidard F-C, Kaklamani V G, Neven P et al. Elacestrant (oral selective estrogen receptor degrader) versus standard endocrine therapy for estrogen receptor–positive, human epidermal growth factor receptor 2–negative advanced breast cancer: results from the randomized phase III EMERALD trial. J Clin Oncol. 2022;40:3246. doi: 10.1200/JCO.22.00338. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 38.Clinicaltrials.gov Study of Trastuzumab Deruxtecan (T-DXd) vs. Investigatorʼs Choice Chemotherapy in HER2-low, Hormone Receptor Positive, Metastatic Breast Cancer (DB-06) 2024. Online (Stand: 24.01.2024):https://clinicaltrials.gov/study/NCT04494425
- 39.Modi S, Jacot W, Yamashita T et al. Trastuzumab deruxtecan in previously treated HER2-low advanced breast cancer. N Engl J Med. 2022;387:9–20. doi: 10.1056/NEJMoa2203690. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 40.Bardia A, Jhaveri K, Im S et al. LBA11 Datopotamab deruxtecan (Dato-DXd) vs. chemotherapy in previously-treated inoperable or metastatic hormone receptor-positive, HER2-negative (HR+/HER2–) breast cancer (BC): Primary results from the randomised phase III TROPION-Breast01 trial. Ann Oncol. 2023;34:S1264–S1265. [Google Scholar]
- 41.Murthy R K, Loi S, Okines A et al. Tucatinib, trastuzumab, and capecitabine for HER2-positive metastatic breast cancer. N Engl J Med. 2020;382:597–609. doi: 10.1056/NEJMoa1914609. [DOI] [PubMed] [Google Scholar]
- 42.Curigliano G, Mueller V, Borges V et al. Tucatinib versus placebo added to trastuzumab and capecitabine for patients with pretreated HER2+ metastatic breast cancer with and without brain metastases (HER2CLIMB): final overall survival analysis. Ann Oncol. 2022;33:321–329. doi: 10.1016/j.annonc.2021.12.005. [DOI] [PubMed] [Google Scholar]
- 43.Hurvitz S, Modi S, Li W et al. 377O A pooled analysis of trastuzumab deruxtecan (T-DXd) in patients (pts) with HER2-positive (HER2+) metastatic breast cancer (mBC) with brain metastases (BMs) from DESTINY-Breast (DB)-01,-02, and-03. Ann Oncol. 2023;34:S335–S336. [Google Scholar]
- 44.Miglietta F, Visani L, Marini S et al. Oligometastatic breast cancer: Dissecting the clinical and biological uniqueness of this emerging entity. Can we pursue curability? Cancer Treat Rev. 2022;110:102462. doi: 10.1016/j.ctrv.2022.102462. [DOI] [PubMed] [Google Scholar]
- 45.Palma D A, Olson R, Harrow S et al. Stereotactic ablative radiotherapy for the comprehensive treatment of oligometastatic cancers: long-term results of the SABR-COMET phase II randomized trial. J Clin Oncol. 2020;38:2830. doi: 10.1200/JCO.20.00818. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 46.Chmura S J, Winter K A, Woodward W Aet al. NRG-BR002: A phase IIR/III trial of standard of care systemic therapy with or without stereotactic body radiotherapy (SBRT) and/or surgical resection (SR) for newly oligometastatic breast cancer (NCT02364557) JCO 202240(Suppl.)1007. 10.1200/JCO.2022.40.16_suppl.1007 [DOI] [Google Scholar]
- 47.Müller V, Hein A, Hartkopf A D et al. Occurrence and characteristics of patients with de novo advanced breast cancer according to patient and tumor characteristics–A retrospective analysis of a real world registry. Eur J Cancer. 2022;172:13–21. doi: 10.1016/j.ejca.2022.05.015. [DOI] [PubMed] [Google Scholar]
- 48.Caglevic C, Rolfo C, Gil-Bazo I et al. The armed conflict and the impact on patients with cancer in Ukraine: Urgent considerations. JCO Glob Oncol. 2022;8:e2200123. doi: 10.1200/GO.22.00123. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 49.van Leeuwen R W, Jansman F G, van den Bemt P M et al. Drug–drug interactions in patients treated for cancer: a prospective study on clinical interventions. Ann Oncol. 2015;26:992–997. doi: 10.1093/annonc/mdv029. [DOI] [PubMed] [Google Scholar]
- 50.Poggio F, Tagliamento M, Pirrone C et al. Update on the management of breast cancer during pregnancy. Cancers. 2020;12:3616. doi: 10.3390/cancers12123616. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 51.Loibl S, Han S N, von Minckwitz G et al. Treatment of breast cancer during pregnancy: an observational study. Lancet Oncol. 2012;13:887–896. doi: 10.1016/S1470-2045(12)70261-9. [DOI] [PubMed] [Google Scholar]
- 52.Amant F, von Minckwitz G, Han S N et al. Prognosis of women with primary breast cancer diagnosed during pregnancy: results from an international collaborative study. J Clin Oncol. 2013;31:2532–2539. doi: 10.1200/JCO.2012.45.6335. [DOI] [PubMed] [Google Scholar]
- 53.Loibl S, Schmidt A, Gentilini O et al. Breast cancer diagnosed during pregnancy: adapting recent advances in breast cancer care for pregnant patients. JAMA Oncol. 2015;1:1145–1153. doi: 10.1001/jamaoncol.2015.2413. [DOI] [PubMed] [Google Scholar]
- 54.Khan S A, Zhao F, Solin L J et al. A randomized phase III trial of systemic therapy plus early local therapy versus systemic therapy alone in women with de novo stage IV breast cancer: A trial of the ECOG-ACRIN Research Group (E2108) J Clin Oncol. 2020;38(Suppl):LBA2. doi: 10.1200/JCO.2020.38.18_suppl.LBA2. [DOI] [Google Scholar]
- 55.Loibl S, Azim H A, jr., Bachelot T et al. ESMO Expert Consensus Statements on the management of breast cancer during pregnancy (PrBC) Ann Oncol. 2023;34:849–866. doi: 10.1016/j.annonc.2023.08.001. [DOI] [PubMed] [Google Scholar]