

Abstract
Introduction
Multi-trauma patients require a multidisciplinary team, especially in the presence of various body systems injuries. The evaluation focuses on the decision regarding the DCO and ETC approaches.
Case presentation
A 24-year-old male patient with Glasgow Coma Score 8, arrived at the emergency room, followed by ATLS protocol. Orthopedic trauma included D8 vertebra unstable burst fracture, right open femur shaft fracture, left closed midshaft femur fracture, and right tibial plateau fracture of the knee.
Case summary
A hemodynamically stable patient with bilateral femur fractures is directed toward the DCO approach.
Discussion
An initial treatment for an external fixator across the knee on the right leg and a spine fusion and decompression of D5–10 surgery was made on the day of admission. Definitive fixation and conversion to internal fixators were done on day 9 after the accident. Postoperative drop-foot injury was seen in the right leg. A Masquelet technique was applied for the right femur segmental fracture due to gaps.
Conclusion
DCO may be employed to temporarily stabilize fractures, allowing the patient to recover from other life-threatening injuries before definitive fixation. Further secondary procedures, such as the Masquelet technique, should be considered to optimize the results. Long-term follow-up and rehabilitation are part of recovery, aiming to optimize functional recovery and improve the patient's quality of life.
Keywords: Multi trauma, Masquelet, Femur shaft fracture, Damage control, Early total care
Introduction
Around 1.19 million people die each year as a result of road traffic accidents. Road traffic accidents are the leading cause of death among children and young adults [1]. Multi-trauma injuries require a fast, thoughtful approach. Patients often suffer severe multi-organ injuries, most commonly in the musculoskeletal system. Treating these patients requires a multidisciplinary approach to the achievement of optimal outcomes. Managing orthopedic multi-trauma involves a coordinated effort between orthopedic surgeons, trauma specialists, anesthesiologists, radiologists, and rehabilitation experts [2,3].
The management of orthopedic multi-trauma has changed several times during the past decades, and some issues remain controversial. Damage Control Orthopedics (DCO), Early Total Care (ETC), Early Appropriate Care (EAC), and Definitive Orthopedic Surgery (SDS) are the most commonly used strategies [[4], [5], [6]]. The trauma team uses scoring systems, like Severity Index Score (ISS), New Injury Severity Score (NISS), and others, for a better understanding of possible predicted outcomes, survival rate, morbidity, mortality, and infection risk for each patient [[7], [8], [9]]. The most commonly injured organs are the head, neck, abdomen, pelvis/lower extremity, and spine [10].
Among road traffic accidents, femur shaft, and segmental fractures are the most common lower extremities fractures. For young patients, these injuries result from high-energy trauma. Femur fractures in high energy must be treated as fast as possible as the comorbidities from the late treatment of these fractures may be fatal, as long bone fractures increase the risk for ARDS (acute respiratory distress syndrome); on the other hand, unattended fractures, with massive bleeding increase the risk of low blood pressure may put the brain function in danger, especially in combination with head and spinal injuries [[11], [12], [13], [14], [15]].
The initial treatment is stabilization of the patient, followed by primary stabilization of the fracture. The overall physiological condition or soft tissue status may not be suitable for definitive fracture fixation. After the definitive fixation of the fracture, the healing process starts, with challenges such as malunion or nonunion of the long bones [16]. One currently used technique to treat these possible complications is the Masquelet technique. This technique is based on the temporary use of polymethyl methacrylate (PMMA) bone cement spacer and morselized bone graft. The procedure may be done in several stages [[17], [18], [19]].
This case report presents a multi-trauma patient managed successfully by a multidisciplinary approach at a tertiary hospital. Our work breaks down the decision-making process for orthopedic multi-trauma management, including initial assessment, surgical interventions, postoperative care, and rehabilitation.
Case presentation
A 24-year-old male patient was brought to the emergency department following a motorcycle traffic accident. On arrival, he was anxious and woke and presented with normal blood pressure (BP) tachycardia. He had a Glasgow Coma Scale score (GCS) of 13, which soon deteriorated to a GCS of 8. Following the ATLS protocol, he was resuscitated with blood products and IV fluids and given IV antibiotics, a tetanus toxoid vaccine, and tranexamic acid. eFAST was negative.
Physical examination - multiple head bruises, light bruise on the right chest, tender abdomen with no contusions, upper limbs without laceration or significant deformities (Fig. 1). Lower limbs: right open femoral shaft fracture with actively oozing bleeding, warm feet, dorsalis pedis pulse - weak, and a left closed femoral shaft fracture. A weak anal sphincter and priapism. A gastric tube and a Foley catheter were inserted, and no hematuria was observed. The patient was hemodynamically stable during the primary and secondary surveys, with a systolic BP of around 145 mmHg.
Fig. 1.

A case of damage control after polytrauma and bilateral femur fracture.
Basic debridement and lavage were performed on the right open femur fracture, followed by Thomas splints on both legs. The pelvis was stable on physical exam. Chest and pelvis X-rays were taken as part of the ATLS protocol.
A total body CT scan demonstrated a D8 vertebra burst fracture involving the posterior elements with over 50 % compression of the vertebral body, dorsal fragment breaching into the spinal canal, and bilateral lamina and pedicles fractures (Fig. 2); right open femur shaft fracture with a wide gap (AO 32B3) and left midshaft femur fracture (AO 32B3) (Fig. 3); tibial plateau fracture Schatzker 4 on the right knee (AO 41C1) (Fig. 4); normal blood flow on angiographic phase in lower limbs. The patient was taken to the ICU.
Fig. 2.
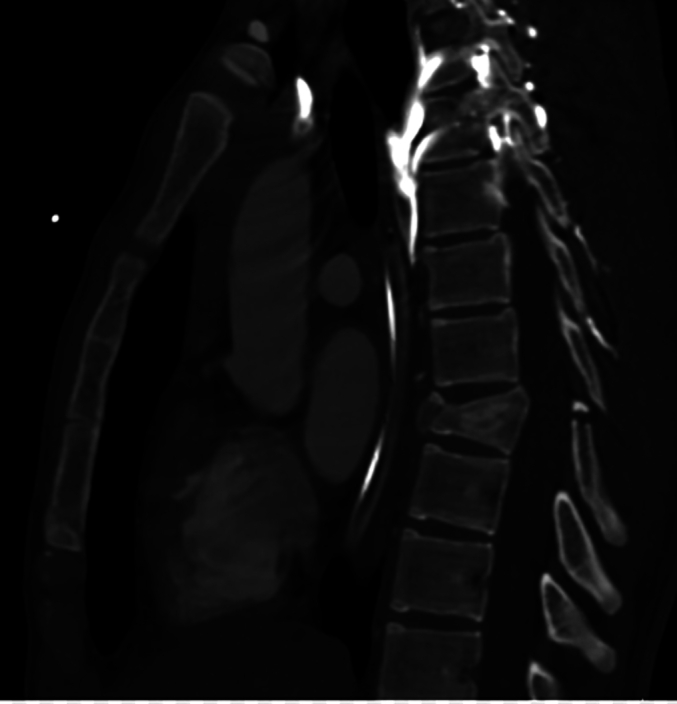
Sagittal plane CT scan of the patient's thoracic spine showing 3-column fracture of D8 vertebra.
Fig. 3.

3D CT scan of the patient's lower limbs.
Fig. 4.

Tibial plateau X-ray taken during the cross-knee Ex-Fix application.
Case presentation summary
Two distinct methods have mainly been used for orthopedic trauma - DCO, ETC. DCO, a staged approach. The goal is to minimize the systemic impact of severe trauma through temporary stabilization and rapid resuscitation. DCO involves initial external fixation or temporary fracture stabilization, followed by delayed definitive fixation after the patient's optimized physiologic status [20]. Temporary stabilization minimizes further soft tissue damage, reduces the risk of infection, and avoids the “second hit” phenomenon by preventing the additional stress on already compromised physiology, reducing the risk of multiple organ dysfunction syndrome (MODS) [[21], [22], [23]]. The main limitations are the need for additional surgeries for definitive fixation, potentially leading to prolonged hospital stays and increased healthcare costs, and delayed functional recovery, which may result in more prolonged immobilization, leading to joint stiffness, muscle atrophy, and delayed rehabilitation [24].
ETC emphasizes definitive fracture fixation as early as possible, often within the first 24–72 h after injury. The concept aims to restore the biomechanical stability of the injured limb promptly, enabling early mobilization and reducing the risk of complications associated with prolonged immobilization [25]. The primary outcome of early stability is prompt initiation of weight-bearing and early mobilization, reducing the risk of joint stiffness and muscle wasting. This strategy aims for single-stage procedures, potentially leading to shorter hospital stays and improved patient satisfaction. Nevertheless, this approach may increase physiological stress, potentially leading to anesthesia-related complications, bleeding, or infection. The main pitfalls are the requirement for efficiency and coordination between the trauma teams, operating room availability, and resources, which may not always be feasible [26].
The “golden hour” in this setting refers to the critical 60-minute window following a severe injury. During this time, swift and decisive medical intervention is crucial to stabilize the patient, address life-threatening injuries, and initiate appropriate treatment. Prompt identification and management of fractures, dislocations, and soft tissue injuries within this timeframe can significantly improve outcomes, minimize complications, and optimize long-term functional recovery [27].
Our patient was hemodynamically stable at this point of treatment and completed surgical clearance for head-chest-abdomen injuries. His injuries were pure orthopedic: bilateral femur shaft fracture, tibial plateau fracture, and a vertebral fracture with clinical neurologic injury. ISS score was used to decide which approach should have been applied (DCO, ETC); it assesses the injuries' severity and magnitude. [28]. A patient with bilateral femur fractures is directed toward the DCO approach as it has a high risk for respiratory complications; if the team chooses to follow the ETC strategy, the patient would have a higher risk for developing ARDS (Fig. 6).
Fig. 6.

Intraoperative imaging of the left femur after Ex-Fix application.
Discussion
Due to this patient presentation, the decision was to proceed with DCO, an external fixator across the knee on the right leg (Fig. 5), and a spine fusion and decompression of D5–10 surgery followed the lower limbs surgery through the same surgery (Fig. 7). The patient received 6 packed cell units, 6 Fresh frozen plasma, and 4 platelet packages. After the surgery, the patient was admitted intubated to the ICU with hemoglobin of 7.8 g/dl without cardiac support. The intraoperative vascular examination was satisfactory for both legs. On postoperative day (POD) 2, the patient successfully extubated. On POD 9 days, he was transferred to the orthopedic department. On this occasion, a physical exam showed weakness in the tibialis anterior and extensor hallucis longus (0/5) and drop-foot, most likely resulting from the tibial plateau fracture. In addition, the patient presented with pain in his wrist and clavicle and demonstrated non-displaced midshaft clavicular and scaphoid fractures, which were treated non-operatively.
Fig. 5.

Intraoperative imaging of the right femur after cross-knee Ex-Fix application demonstrating the gap defect in the right femur.
Fig. 7.

intraoperative imaging of the spinal posterior fixation D5-D10 (A-AP; B-lateral views).
Planning the definitive treatment was challenging, as the right femur had a bone gap. The option of using bone graft was declined due to the high risk of absorption of the graft by the body. Therefore, the team used the Masquelet procedure, the induced membrane technique, or staged bone grafting. The procedure involves two stages. In the first stage, a temporary cement spacer is inserted into the bone defect or nonunion. This spacer helps stimulate and form a biological membrane around it - A masquelet membrane. The membrane is rich in growth factors and promotes the recruitment of progenitor cells. The surgeon fills the induced membrane with a bone graft during the second stage, typically several weeks after the first stage. This bone graft can be an autograft, allograft, or synthetic graft material. The induced membrane provides a rich blood supply to the graft, promoting its incorporation and subsequent bone healing. The induced membrane serves as a biological chamber, facilitating the incorporation of the graft and providing a favorable environment for bone healing [29,30].
The Masquelet procedure offers several advantages for bone defect reconstruction. It allows for reconstructing significant bone defects that would otherwise be difficult to manage. The induced membrane serves as a biological scaffold, promoting the formation of new blood vessels and supporting bone regeneration. The two-stage approach reduces the risk of infection and provides an opportunity for thorough debridement of infected tissues. It is essential to note that the Masquelet procedure is a complex and demanding surgical technique. It requires careful patient selection, meticulous surgical technique, and postoperative monitoring. Complications can occur, such as infection, graft resorption, or joint stiffness. Therefore, thorough evaluation and planning are crucial for successful outcomes [31].
According to DCO, definitive treatment should be delayed for 7–10 days. The external fixators were converted to internal fixation devices using retrograde intra-medullary nails (IMN) for both femurs and left tibial plateau plating 10 days after admission to the hospital. As part of the first stage of Masquelet, the proper femur fixation included polymethyl methacrylate (PMMA) bone cement placement around the nail (Fig. 8) in the gap areas. For our patient, the Masquelet 1st stage took place during the conversion of the external fixator conversion to internal fixation (Fig. 9). The second stage took place two months later. During the time between the stages, the patient moved to a rehabilitation center and was discharged.
Fig. 8.

Postoperative image of the right femur 1 month after masquelet procedure stage 1 (A-both legs images; B-zoom in of the right femur).
Fig. 9.

Routine follow-up 6 months after the accident.
The patient was satisfied and had a minimal disability, mainly due to his drop foot. During the first follow-up, our patient's X-ray films showed a new forming gap as the surrounding tissues absorbed some of the bone graft. During the following weeks, the patient underwent daily physiotherapy and occupational therapy, and although his right femur gap did not bridge completely, the patient returned home without significant disabilities. He walks without aids, has knee flexion of over 90 degrees, and uses a dictus brace for his right ankle.
Conclusion
Multi-trauma management in orthopedic surgery is complex and challenging. Orthopedic surgeons must prioritize their interventions to address life-threatening conditions and stabilize them before proceeding with definitive treatment. Surgeons must perform a systematic examination to identify fractures, dislocations, and soft tissue injuries. Imaging studies, such as X-rays, CT scans, and sometimes MRIs, play a crucial role in the diagnostic process. Open fractures and fractures associated with vascular compromise should be managed promptly.
The timing of surgical interventions in multi-trauma patients must be carefully considered. The surgeon must weigh the benefits of each strategy to facilitate early mobilization and reduce complication rates against the risks associated with the patient's overall condition, including potential hemodynamic instability or respiratory compromise. In some cases, DCO may be employed to temporarily stabilize fractures, allowing the patient to recover from other life-threatening injuries before definitive fixation. Postoperative care involves close monitoring of the patient's vital signs, pain control, wound management, and early initiation of physical therapy. Early mobilization is encouraged to prevent complications such as deep vein thrombosis, pneumonia, and pressure ulcers. Long-term follow-up and rehabilitation are integral components of multi-trauma management, aiming to optimize functional recovery and improve the patient's quality of life.
CRediT authorship contribution statement
Dana Avraham: Writing – review & editing, Writing – original draft, Conceptualization. Amir Herman: Project administration, Methodology. Maria Oulianski: Writing – review & editing, Supervision.
Declaration of competing interest
The authors declare that they have no known competing financial interests or personal relationships that could have appeared to influence the work reported in this paper.
References
- 1.World Health Organization . World Heal Organ; 2023. Global Status Report on Road Safety 2023; p. 81. [Google Scholar]
- 2.Anon. The trauma call. BMJ. 2018:361. doi: 10.1136/bmj.k2272. [DOI] [PubMed] [Google Scholar]
- 3.Cole E., Crichton N. The culture of a trauma team in relation to human factors. J. Clin. Nurs. 2006;15(10):1257–1266. doi: 10.1111/j.1365-2702.2006.01566.x. [DOI] [PubMed] [Google Scholar]
- 4.Pape H.-C., Halvachizadeh S., Leenen L., Velmahos G.D., Buckley R., Giannoudis P.V. Timing of major fracture care in polytrauma patients - an update on principles, parameters and strategies for 2020. Injury. 2019;50(10):1656–1670. doi: 10.1016/j.injury.2019.09.021. [DOI] [PubMed] [Google Scholar]
- 5.Devendra A., Nishith P.G., Dilip Chand Raja S., Dheenadhayalan J., Rajasekaran S. Current updates in management of extremity injuries in polytrauma. J. Clin. Orthop. Trauma. 2021;12(1):113–122. doi: 10.1016/j.jcot.2020.09.031. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Nauth A., Hildebrand F., Vallier H., et al. Polytrauma: update on basic science and clinical evidence. OTA Int. Open Access J. Orthop. Trauma. 2021;4(1) doi: 10.1097/OI9.0000000000000116. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Harwood P.J., Giannoudis P.V., Probst C., Krettek C., Pape H.-C. The risk of local infective complications after damage control procedures for femoral shaft fracture. J. Orthop. Trauma. 2006;20(3):181–189. doi: 10.1097/00005131-200603000-00004. [DOI] [PubMed] [Google Scholar]
- 8.Balogh Z.J., Varga E., Tomka J., Süveges G., Tóth L., Simonka J.A. The new injury severity score is a better predictor of extended hospitalization and intensive care unit admission than the injury severity score in patients with multiple orthopaedic injuries. J. Orthop. Trauma. 2003;17(7):508–512. doi: 10.1097/00005131-200308000-00006. [DOI] [PubMed] [Google Scholar]
- 9.Osler T., Baker S.P., Long W. A modification of the injury severity score that both improves accuracy and simplifies scoring. J. Trauma. 1997;43(6):922–926. doi: 10.1097/00005373-199712000-00009. [DOI] [PubMed] [Google Scholar]
- 10.Nakao S., Katayama Y., Kitamura T., et al. Trends and characteristics of severe road traffic injuries in children: a nationwide cohort study in Japan. Eur. J. Trauma Emerg. Surg. Off. Publ. Eur. Trauma Soc. 2023 doi: 10.1007/s00068-023-02372-z. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Guerado E., Bertrand M.L., Cano J.R., Cerván A.M., Galán A. Damage control orthopaedics: state of the art. World J. Orthop. 2019;10(1):1–13. doi: 10.5312/wjo.v10.i1.1. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Harwood P.J., Giannoudis P.V., van Griensven M., Krettek C., Pape H.-C. Alterations in the systemic inflammatory response after early total care and damage control procedures for femoral shaft fracture in severely injured patients. J. Trauma. 2005;58(3):444–446. doi: 10.1097/01.ta.0000153942.28015.77. [DOI] [PubMed] [Google Scholar]
- 13.Tuttle M.S., Smith W.R., Williams A.E., et al. Safety and efficacy of damage control external fixation versus early definitive stabilization for femoral shaft fractures in the multiple-injured patient. J. Trauma. 2009;67(3):602–605. doi: 10.1097/TA.0b013e3181aa21c0. [DOI] [PubMed] [Google Scholar]
- 14.Mugesh Kanna R., Prasad Shetty A., Rajasekaran S. Timing of intervention for spinal injury in patients with polytrauma. J. Clin. Orthop. Trauma. 2021;12(1):96–100. doi: 10.1016/j.jcot.2020.10.003. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Pape H.-C., Hildebrand F., Pertschy S., et al. Changes in the management of femoral shaft fractures in polytrauma patients: from early total care to damage control orthopedic surgery. J. Trauma. 2002;53(3):452. doi: 10.1097/00005373-200209000-00010. [DOI] [PubMed] [Google Scholar]
- 16.Roberts C.S., Pape H.-C., Jones A.L., Malkani A.L., Rodriguez J.L., Giannoudis P.V. Damage control orthopaedics: evolving concepts in the treatment of patients who have sustained orthopaedic trauma. Instr. Course Lect. 2005;54:447–462. [PubMed] [Google Scholar]
- 17.Klein C., Monet M., Barbier V., et al. The Masquelet technique: current concepts, animal models, and perspectives. J. Tissue Eng. Regen. Med. 2020;14(9):1349–1359. doi: 10.1002/term.3097. [DOI] [PubMed] [Google Scholar]
- 18.Wong T.M., Lau T.W., Li X., Fang C., Yeung K., Leung F. Masquelet technique for treatment of posttraumatic bone defects. Sci. World J. 2014;2014 doi: 10.1155/2014/710302. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Alford A.I., Nicolaou D., Hake M., McBride-Gagyi S. Masquelet’s induced membrane technique: review of current concepts and future directions. J. Orthop. Res. Off. Publ. Orthop. Res. Soc. 2021;39(4):707–718. doi: 10.1002/jor.24978. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Pape H.-C., Tornetta P., 3rd, Tarkin I., Tzioupis C., Sabeson V., Olson S.A. Timing of fracture fixation in multitrauma patients: the role of early total care and damage control surgery. J. Am. Acad. Orthop. Surg. 2009;17(9):541–549. doi: 10.5435/00124635-200909000-00001. [DOI] [PubMed] [Google Scholar]
- 21.Weinberg D.S., Narayanan A.S., Moore T.A., Vallier H.A. Assessment of resuscitation as measured by markers of metabolic acidosis and features of injury. Bone Joint J. 2017;99-B(1):122–127. doi: 10.1302/0301-620X.99B1.BJJ-2016-0418.R2. [DOI] [PubMed] [Google Scholar]
- 22.Scalea T.M., Boswell S.A., Scott J.D., Mitchell K.A., Kramer M.E., Pollak A.N. External fixation as a bridge to intramedullary nailing for patients with multiple injuries and with femur fractures: damage control orthopedics. J. Trauma. 2000;48(4):613. doi: 10.1097/00005373-200004000-00006. [DOI] [PubMed] [Google Scholar]
- 23.Morshed S., Miclau T., 3rd, Bembom O., Cohen M., Knudson M.M., Colford J.M.J. Delayed internal fixation of femoral shaft fracture reduces mortality among patients with multisystem trauma. J. Bone Joint Surg. Am. 2009;91(1):3–13. doi: 10.2106/JBJS.H.00338. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.Bates P., Parker P., McFadyen I., Pallister I. Demystifying damage control in musculoskeletal trauma. Ann. R. Coll. Surg. Engl. 2016;98(5):291–294. doi: 10.1308/rcsann.2016.0111. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.Nahm N.J., Como J.J., Wilber J.H., Vallier H.A. Early appropriate care: definitive stabilization of femoral fractures within 24 hours of injury is safe in most patients with multiple injuries. J. Trauma. 2011;71(1):175–185. doi: 10.1097/TA.0b013e3181fc93a2. [DOI] [PubMed] [Google Scholar]
- 26.Enocson A., Lundin N. Early versus late surgical treatment of pelvic and acetabular fractures a five-year follow-up of 419 patients. BMC Musculoskelet. Disord. 2023;24(1):848. doi: 10.1186/s12891-023-06977-8. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27.van Olden G.D.J., Meeuwis J.D., Bolhuis H.W., Boxma H., Goris R.J.A. Clinical impact of advanced trauma life support. Am. J. Emerg. Med. 2004;22(7):522–525. doi: 10.1016/j.ajem.2004.08.013. [DOI] [PubMed] [Google Scholar]
- 28.Pape H.-C., Giannoudis P.V., Krettek C., Trentz O. Timing of fixation of major fractures in blunt polytrauma: role of conventional indicators in clinical decision making. J. Orthop. Trauma. 2005;19(8):551–562. doi: 10.1097/01.bot.0000161712.87129.80. [DOI] [PubMed] [Google Scholar]
- 29.Masquelet A.C., Begue T. The concept of induced membrane for reconstruction of long bone defects. Orthop. Clin. North Am. 2010;41(1):27–37. doi: 10.1016/j.ocl.2009.07.011. (table of contents) [DOI] [PubMed] [Google Scholar]
- 30.Shen J., Wei Z., Wang S., et al. Treatment of infected bone defects with the induced membrane technique. Bone Joint Res. 2023;12(9):546–558. doi: 10.1302/2046-3758.129.BJR-2022-0439.R2. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 31.Piacentini F., Ceglia M.J., Bettini L., Bianco S., Buzzi R., Campanacci D.A. Induced membrane technique using enriched bone grafts for treatment of posttraumatic segmental long bone defects. J. Orthop. Traumatol. Off. J. Ital. Soc. Orthop. Traumatol. 2019;20(1):13. doi: 10.1186/s10195-019-0522-6. [DOI] [PMC free article] [PubMed] [Google Scholar]