

Abstract
Dry scooping, a rather risky act of consuming undiluted pre-workout protein powder hoping for a more pronounced energy surge, is increasingly becoming a fitness trend worldwide. A previously healthy 25-year-old man of African origin presented with acute onset of crushing mid-sternal chest pain for 4 h. His symptoms began about an hour following completion of his 2-h exercise regimen at the gym. He had an unremarkable past medical history except for an 8-month consumption of a pre-workout supplement as part of his gym routine. He claimed to have adhered to the manufacturer’s recommended method of using the supplement, except for 3 days prior to presentation when he started “dry scooping” following the viewing of a video advocating such practice from his fitness WhatsApp group. Cardiac evaluation revealed features in keeping with diagnosis of anterolateral ST-elevation myocardial infarction. Emergency coronary angiography revealed a thrombotic lesion completely occluding the proximal left anterior descending coronary artery with TIMI 0 flow distally. After successful balloon angioplasty, a drug-eluting stent was implanted successfully, restoring TIMI 3 flow to the proximal left anterior descending coronary artery. This case report aims to raise awareness among both clinicians and the general public regarding the pervasiveness of pre-workout supplements, improper methods of consumption, and the potential life-threatening repercussions of misuse.
Keywords: Acute myocardial infarction, acute coronary syndrome, coronary artery thrombosis, STEMI, pre-workout supplement, fitness supplements
Introduction
There is compelling and unequivocal epidemiologic evidence regarding the pivotal role of regular physical activity in preventing several chronic diseases, as well as in reducing the risk of premature death.1–4 Despite such overwhelming evidence, over a third of individuals globally do not meet the World Health Organization recommended levels of physical activity.5,6 Nevertheless, exercise-related medical and physiological complications, particularly sudden death, arguably remain a concern regarding the safety of physical activity. 7 For instance, sudden cardiac death is the most frequent cause of death among athletes across all ages, occurring almost threefold compared to nonathletes.8–10 However, it is postulated that regular physical activity can reduce mortality by up to 50% in the general population. 4
Owing to its synergistic potential in improving mental focus, exercise capacity (i.e., delaying fatigue and increasing performance), and augmenting training adaptations,11,12 pre-workout supplementation is estimated to be used by a considerable proportion of young adults globally.13,14 However, consumption of these supplements has been linked with numerous negative health effects, including psychosis, 15 extensive esophageal ulcerations, 16 aplastic anemia, 17 hemorrhagic stroke, 18 ischemic colitis, 19 pancreatitis, 20 hepatic failure, 21 aortic dissection, 22 myocardial infarction, 23 cardiac arrest, 24 and death. 25 Moreover, despite their widespread popularity and increasing use, the exact composition of such products is often unknown, making their safety and efficacy profiles paradoxical.12,26 We present a case of acute myocardial infarction following the practice of “dry scooping” a pre-workout supplement in a healthy young male of African origin.
Case description
A previously healthy 25-year-old man of African origin presented to the Jakaya Kikwete Cardiac Institute with an acute onset of crushing mid-sternal chest pain for 4 h. His symptoms had begun about an hour following completion of his regular (2 h/day, 5 times a week) exercise regimen (weightlifting and aerobics) at the gym. He had an unremarkable medical history, denied any history of recreational drug use or relevant occupational exposure, and did not experience symptoms associated with atherosclerosis at a younger age. Additionally, there was no family history of familial hypercholesterolemia, premature coronary artery disease, or sudden death. However, as part of his gym routine, he has been taking a pre-workout supplement (containing caffeine, theophylline, glucuronolactone, L-glycine, methylcobalamin, beta-alanine, CreNitrate, ArgNitrate, choline bitartrate, L-glutamine nitrate, L-tyrosine, guarana extract, and taurine) roughly 30 min before exercise for the past 8 months. He denied the use of alcohol, tobacco, or energy drink consumption. He claimed to have adhered to the manufacturer’s recommended method of using the pre-workout supplement (i.e., mixing the protein powder with water or plant-based milk) all the way except for the past 3 days when he started “dry scooping” following the viewing of a video advocating such practice from his fitness WhatsApp group. Nevertheless, he claims that he has been adhering to an off-label recommendation of two single-serving scoops per day despite consuming it dry.
During the physical examination, it was observed that the young man appeared healthy but displayed facial expressions indicative of pain. His vitals were stable (blood pressure 114/71 mmHg, pulse of 58 beats/min, respiratory rate of 18 breaths/min, and a body mass index of 21.8 kg/m²). Systemic examination was unremarkable except for an S4 gallop during cardiac auscultation. His lipid profile was within acceptable range (low-density lipoprotein 1.02 mmol/L, high-density lipoprotein 1.53 mmol/L, triglycerides 0.77 mmol/L and total cholesterol 2.96 mmol/L). The electrocardiogram (ECG) showed sinus bradycardia with ST-segment elevation in the anterolateral leads (V2–V5, I, aVL) (Figure 1), and the transthoracic echocardiogram (ECHO) showed anterior wall hypokinesia with preserved global left ventricular systolic function (ejection fraction (EF) 68%). Laboratory evaluation (i.e., Prothrombin time, Partial thromboplastin time, D-dimer, Protein C, Protein S, Antithrombin III activity, and Factor VIII activity) did not indicate a hypercoagulable state or a systemic thromboembolic disease; however, cardiac enzymes were elevated, with a peak troponin I of 5.14 ng/mL and CK-MB of 78.1 ng/mL. Considering the above history and symptomatology, we entertained a diagnosis of anterolateral ST-elevation myocardial infarction. A loading dose of aspirin (300 mg), clopidogrel (600 mg), and atorvastatin (80 mg) were initiated, and the patient was taken for emergency coronary angiography.
Figure 1.

Electrocardiogram displaying sinus rhythm with marked ST elevation on the anterolateral leads (V2–V5, I, aVL) and reciprocal changes in the inferior leads (III and aVF).
Coronary angiography revealed a thrombotic lesion completely occluding the proximal left anterior descending coronary artery (LAD) with TIMI 0 flow distally (Figure 2). There was no evidence of atherosclerosis, dissection, or coronary malformations, and the right coronary system was intact. After successful balloon angioplasty, a drug-eluting stent (DES) was implanted successfully, restoring TIMI 3 flow to the proximal LAD (Figure 3). He remained free of chest pain during a 2-day observation in the coronary care unit, and a follow-up ECG showed resolution of ST-elevation. Following extensive counseling, he was discharged from the hospital with statin and dual antiplatelet therapy. Upon review 4 weeks later, he reported normal functional capacity, with neither chest pain nor ischemic changes on ECG (Figure 4). His follow-up ECHO revealed preserved EF with limited residual hypokinesia on the anterior wall.
Figure 2.
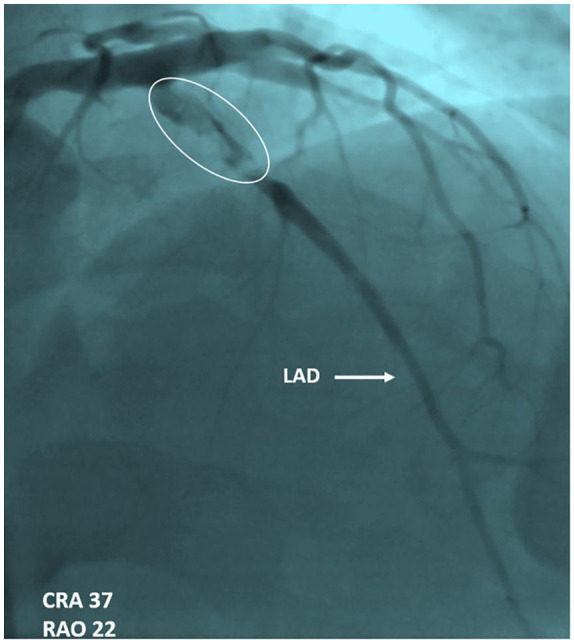
Coronary angiography-1 displaying a filling defect consistent with thrombosis, 100% occlusion of the proximal left anterior descending coronary artery artery, and distal tapering with TIMI 0 flow.
Figure 3.
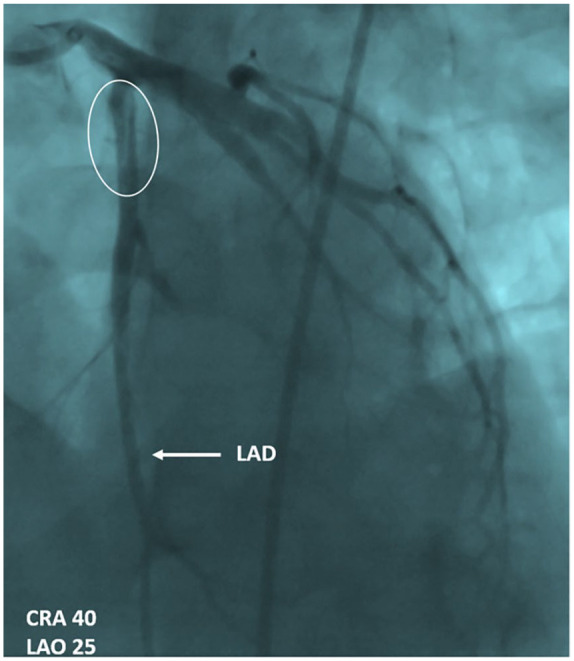
Coronary angiography-2 displaying a patent left anterior descending coronary artery vessel post revascularization with drug-eluting stent.
Figure 4.

Electrocardiogram at follow-up displaying normal findings.
Discussion
In this era of noncommunicable disease preponderance, individuals are increasingly becoming more health-conscious than before, with a vivid inclination toward fitness-oriented lifestyles. Parallel to this, there is a surging demand for pre-workout supplements (predominantly protein powder) from athletes and fitness enthusiasts, and the rapidly growing global sports nutrition market (valued at USD 45.24 billion in 2023) is projected to reach USD 77.95 billion by 2030. 27 Recent studies have revealed considerably high rates of pre-workout supplement consumption in fitness centers, ranging from 68.7% among Saudi women to 96% among gymnasium trainees in Lesotho.28–35
Designed to boost energy and augment athletic performance, protein formulas—largely containing a blend of performance-enhancing ingredients including caffeine, nitric oxide precursors (e.g., L-arginine, L-citrulline), creatine, beta-alanine, and branched-chain amino acids—are the most widely used formulations.12,36 Typically sold in powder form, pre-workout supplements are recommended to be ingested with a liquid accompaniment (water or plant-based milk). Nevertheless, dry scooping, a rather risky act of consuming undiluted pre-workout powder hoping for a more pronounced energy surge, is increasingly becoming a fitness trend worldwide. Although it investigated an unorthodox platform (i.e., TikTok), a study by Lin et al. revealed that 86% of individuals portrayed improper use (including dry scooping) of pre-workout supplements. 37 Moreover, despite the purported benefits of dry scooping, ingestion of the highly concentrated powder could potentially lead to catastrophic symptoms ranging from choking to death. 37
Similar to our earlier case on energy drinks and acute coronary syndrome, 38 this case report demonstrates a similarly life-threatening presentation in a young, healthy man with no obvious cardiovascular risk factors. Although the cause of coronary thrombus in our case remains uncertain, it is conceivable that the thrombus developed as a result of pre-workout-induced coronary spasm. As reiterated by previous articles,23,39–43 some ingredients in pre-workout supplements (potentially synergistically) coupled with a catecholamine surge during exercise could potentially lead to spasm-induced thrombosis.44,45 Furthermore, the current body of knowledge supports the notion of misinformed decisions and subsequently a wide variation in practice among pre-workout supplement users and prescribers.46,47 Therefore, it is fundamental that athletes and fitness enthusiasts are aware of the potential risks linked to pre-workouts, particularly their improper use. Moreover, given the documented adverse health consequences following their improper use,48–51 it is pivotal that pre-workout supplements are consumed as recommended.
Conclusion
Dry scooping, a practice not endorsed by health professionals or supplement manufacturers, carries life-threatening consequences. Given the potential risks associated with this improper method of consumption, it is pivotal for fitness enthusiasts to consume pre-workout supplements as directed to avoid the health repercussions of misuse. Additionally, ongoing research and monitoring are imperative to better understand the potential health consequences of pre-workout supplement use and to inform evidence-based recommendations for safe practices.
Acknowledgments
The authors are grateful to the patient for giving us the opportunity to learn and to pass on the lessons learnt to others.
Footnotes
Author contributions: P.P. and S.V.B. took the history and performed the physical examination. S.V.B. performed the cardiac imaging, and E.S.M. processed the laboratory investigations. Y.G. and P.R.K. performed the coronary angiography. S.V.B., P.P., J.M., P.R.K., M.K., and Z.S.M. participated in clinical management and counseling of the patient during hospitalization and follow-up. P.P. wrote the initial draft of the manuscript. All authors reviewed and contributed to the final version of this case report.
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding: The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethics approval: Our institution does not require ethical approval for reporting individual cases or case series.
Informed consent: Written informed consent was obtained from the patients for their anonymized information to be published in this article.
ORCID iD: Pedro Pallangyo  https://orcid.org/0000-0002-6720-5110
https://orcid.org/0000-0002-6720-5110
References
- 1. Anderson E, Durstine JL. Physical activity, exercise, and chronic diseases: a brief review. Sports Med Health Sci 2019; 1(1): 3–10. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2. Usmani D, Ganapathy K, Patel D, et al. The role of exercise in preventing chronic diseases: current evidence and recommendations. Georgian Med News 2023; 339: 137–142. [PubMed] [Google Scholar]
- 3. Saint-Maurice PF, Graubard BI, Troiano RP, et al. Estimated number of deaths prevented through increased physical activity among US adults. JAMA Intern Med 2022; 182(3): 349–352. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4. Aune D, Schlesinger S, Hamer M, et al. Physical activity and the risk of sudden cardiac death: a systematic review and meta-analysis of prospective studies. BMC Cardiovasc Disord 2020; 20: 318. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5. Guthold R, Stevens GA, Riley LM, et al. Worldwide trends in insufficient physical activity from 2001 to 2016: a pooled analysis of 358 population-based surveys with 1·9 million participants. Lancet Glob Health 2018; 6(10): e1077–e1086. [DOI] [PubMed] [Google Scholar]
- 6. Varela AR, Cruz GIN, Hallal P, et al. Global, regional, and national trends and patterns in physical activity research since 1950: a systematic review. Int J Behav Nutr Phys Act 2021; 18: 5. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7. Fanous Y, Dorian P. The prevention and management of sudden cardiac arrest in athletes. CMAJ 2019; 191(28): E787–E791. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8. Corrado D, Basso C, Rizzoli G, et al. Does sports activity enhance the risk of sudden death in adolescents and young adults?. J Am Coll Cardiol 2003; 42: 1959–1963. [DOI] [PubMed] [Google Scholar]
- 9. Corrado D, Basso C, Schiavon M, et al. Pre-participation screening of young competitive athletes for prevention of sudden cardiac death. J Am Coll Cardiol 2008; 52: 1981–1989. [DOI] [PubMed] [Google Scholar]
- 10. Prakash K, Swarnakari K, Bai M, et al. Sudden cardiac arrest in athletes: a primary level of prevention. Cureus 2022; 14(10): e30517. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11. Wardenaar F, van den Dool R, Ceelen I, et al. Self-reported use and reasons among the general population for using sports nutrition products and dietary supplements. Sports 2016; 4(2): 33. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12. Harty PS, Zabriskie HA, Erickson JL, et al. Multi-ingredient pre-workout supplements, safety implications, and performance outcomes: a brief review. J Int Soc Sports Nutr 2018; 15(1): 41. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13. Hoffman JR, Faigenbaum AD, Ratamess NA, et al. Nutritional supplementation and anabolic steroid use in adolescents. Med Sci Sports Exerc 2008; 40: 15–24. [DOI] [PubMed] [Google Scholar]
- 14. Froiland K, Koszewski W, Hingst J, et al. Nutritional supplement use among college athletes and their sources of information. Int J Sport Nutr Exerc Metab 2004; 14(1): 104–120. [DOI] [PubMed] [Google Scholar]
- 15. Gallop A, Marx Bhagat C, et al. Psychosis in an 18-year-old male. Contemp Pediatr 2022; 39: 10. [Google Scholar]
- 16. Caratenuto R, Karanfilian B, Navlani R, et al. Social media trends, dry scooping, and extensive esophageal ulcerations. J Gen Intern Med 2023; 38(16): 3633–3635. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17. Bastola S, Kc O, Khanal S, et al. Hepatitis-associated aplastic anemia from workout supplement: rare but potentially fatal entity. SAGE Open Med Case Rep 2020; 8: 2050313X20901937. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18. Harris BF, Winn C, Ableman TB. Hemorrhagic stroke in a young healthy male following use of pre-workout supplement animal rage XL. Mil Med 2017; 182(9): e2030–e2033. [DOI] [PubMed] [Google Scholar]
- 19. Magee CD, Moawad FJ, Moses F. NO-Xplode: a case of supplement-associated ischemic colitis. Mil Med 2010; 175(3): 202–205. [DOI] [PubMed] [Google Scholar]
- 20. Ridha M, Rivera Gonzalez G, Seenivasagam M. Pre-workout-induced pancreatitis. Cureus 2023; 15(9): e44609. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21. Romick J, Viswanathan L, Ramos B. S2600 pre-workout peril: drug-induced liver injury in a young deployed service member. Am J Gastroenterol 2020; 115: S1365–S1366. [Google Scholar]
- 22. Doctorian T, Do B. Ascending aortic dissection in a young patient using a synephrine-containing workout supplement. J Cardiol Cases 2017; 15(5): 150–152. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23. Bonim A, Duarte SBCP, Dos Santos RB, et al. Acute myocardial infarction induced by pre-workout supplement in a young patient. Open J Clin Med Case Rep 2017; 3(10): 1259. [Google Scholar]
- 24. Karnatovskaia LV, Leoni JC, Freeman ML. Cardiac arrest in a 21-year-old man after ingestion of 1,3-DMAA-containing workout supplement. Clin J Sport Med 2015; 25(1): e23–e25. [DOI] [PubMed] [Google Scholar]
- 25. Singer N, Lattman P. A workout booster, and a lawsuit. The New York Times, 13 February 2013, https://www.nytimes.com/2013/02/14/business/death-after-use-of-jack3d-shows-gap-in-regulation.html (accessed 12 March 2024).
- 26. Eudy AE, Gordon LL, Hockaday BC, et al. Efficacy and safety of ingredients found in pre workout supplements. Am J Health Syst Pharm 2013; 70: 577–588. [DOI] [PubMed] [Google Scholar]
- 27. Grand View Research. Sports Nutrition Market Size, Share & Trends Analysis Report By Product Type (Sports Supplements, Sports Drinks), By Formulation, By Consumer Group, By Sales Channel, By Region, And Segment Forecasts, 2024–2030. https://www.grandviewresearch.com/industry-analysis/sports-nutritionmarket#:~:text=The%20global%20sports%20nutrition%20market,are%20essential%20for%20maximum%20performance.
- 28. Mazzilli M, Macaluso F, Zambelli S, et al. The use of dietary supplements in fitness practitioners: a cross-sectional observation study. Int J Environ Res Public Health 2021; 18(9): 5005. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29. Senekal M, Meltzer S, Horne A, et al. Dietary supplement use in younger and older men exercising at gyms in Cape Town. S Afr J Clin Nutr 2019: 1–8. [Google Scholar]
- 30. Aljebeli S, Albuhairan R, Ababtain N, et al. The prevalence and awareness of dietary supplement use among saudi women visiting fitness centers in Riyadh, Saudi Arabia. Cureus 2023; 15(6): e41031. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 31. Solheim SA, Nordsborg NB, Ritz C, et al. Use of nutritional supplements by Danish elite athletes and fitness customers. Scand J Med Sci Sports 2017; 27: 801–808. [DOI] [PubMed] [Google Scholar]
- 32. Morrison LJ, Gizis F, Shorter B. Prevalent use of dietary supplements among people who exercise at a commercial gym. Int J Sport Nutr Exerc Metab 2004; 14: 481–492. [DOI] [PubMed] [Google Scholar]
- 33. da Silva WV, de Andrade Gomes Silva MI, Tavares Toscano L, et al. Supplementation prevalence and adverse effects in physical exercise practitioners. Nutr Hosp 2014; 29: 158–165. [DOI] [PubMed] [Google Scholar]
- 34. Mettler S, Bosshard JV, Häring D, et al. High prevalence of supplement intake with a concomitant low information quality among Swiss Fitness Center users. Nutrients 2020; 12(9): 2595. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 35. Sello MG, Letšoara M, Qhomoko M. The use of nutritional supplements among gymnasium trainees in Maseru, Lesotho. World J Nutr Health 2023; 11(1): 11–16. [Google Scholar]
- 36. Jagim AR, Harty PS, Camic CL. Common ingredient profiles of multi-ingredient pre-workout supplements. Nutrients 2019; 11(2): 254. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 37. Lin A, Chow N, O’Connor M, et al. Dry scooping and other dangerous pre-workout consumption methods: a quantitative analysis. Pediatrics 2022; 149: 204. [Google Scholar]
- 38. Pallangyo P, Bhalia SV, Komba M, et al. Acute myocardial infarction following the consumption of energy drink in a 28-year-old male: a case report. J Investig Med High Impact Case Rep 2023; 11: 23247096231168811. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 39. Suchard JR, Suchard MA, Steinfeldt JL. Physician knowledge of herbal toxicities and adverse herb-drug interactions. Eur J Emerg Med 2004; 11: 193–197. [DOI] [PubMed] [Google Scholar]
- 40. Thomas JE, Munir JA, McIntyre PZ, et al. STEMI in a 24-year-old man after use of a synephrine-containing dietary supplement: a case report and review of the literature. Tex Heart Inst J 2009; 36(6): 586–590. [PMC free article] [PubMed] [Google Scholar]
- 41. Smith TB, Staub BA, Natarajan GM, et al. Acute myocardial infarction associated with dietary supplements containing 1,3-dimethylamylamine and Citrus aurantium. Tex Heart Inst J 2014; 41(1): 70–72. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 42. Haller CA, Benowitz NL. Adverse cardiovascular and central nervous system events associated with dietary supplements containing ephedra alkaloids. N Engl J Med 2000; 343(25): 1833–1838. [DOI] [PubMed] [Google Scholar]
- 43. Samenuk D, Link MS, Homoud MK, et al. Adverse cardiovascular events temporally associated with ma huang, an herbal source of ephedrine. Mayo Clin Proc 2002; 77(1): 12–16. [DOI] [PubMed] [Google Scholar]
- 44. Unnikrishnan D, Annam R, Jacob A, et al. STEMI in a young male after use of synephrine-containing dietary supplement. Case Rep Cardiol 2018; 2018: 7074104. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 45. Johnson GJ, Griggs TR, Badimon L. The utility of animal models in the preclinical study of interventions to prevent human coronary artery restenosis: analysis and recommendations. Thrombosis Haemostasis 1999; 81(5): 835–843. [PubMed] [Google Scholar]
- 46. Jones G. Caffeine and other sympathomimetic stimulants: modes of action and effects on sports performance. Essays Biochem 2008; 44:109–123. [DOI] [PubMed] [Google Scholar]
- 47. Kemper KJ, Gardiner P, Gobble J, et al. Expertise about herbs and dietary supplements among diverse health professionals. BMC Complement Altern Med 2006; 6: 15. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 48. Schröder H, Navarro E, Mora J, et al. The type, amount, frequency and timing of dietary supplement use by elite players in the First Spanish Basketball League. J Sports Sci 2002; 20(4): 353–358. [DOI] [PubMed] [Google Scholar]
- 49. Dunn MS, Eddy JM, Wang MQ, et al. The influence of significant others on attitudes, subjective norms and intentions regarding dietary supplement use among adolescent athletes. Adolescence 2001; 36(143): 583–591. [PubMed] [Google Scholar]
- 50. Cisek-Woźniak A, Mruczyk K, Wójciak RW. Physical activity and dietary supplementation intake among postmenopausal women. Balt J Health Phys Act 2019; 11(3): 66–76. [Google Scholar]
- 51. Deldicque L, Francaux M. Potential harmful effects of dietary supplements in sports medicine. Curr Opin Clin Nutr Metab Care 2016; 19(6): 439–445. [DOI] [PubMed] [Google Scholar]