

Abstract
Background:
Pickleball is one of the fastest-growing sports in the United States, with more than an 11-fold increase in injuries from 2010 to 2019.
Purpose:
To (1) determine the prevalence and demographic variables associated with pickleball-related fractures among patients evaluated at emergency departments in the United States between 2002 and 2022 and (2) identify variables influencing patient disposition status.
Study Design:
Descriptive epidemiology study.
Methods:
The US Consumer Product Safety and Commission's publicly available database, the National Electronic Injury Surveillance System (NEISS), was used in this study. Analyses consisted of descriptive statistics for fracture prevalence and demographic variables as well as univariate analysis for disposition status (discharged home vs hospital admission).
Results:
A total of 397 pickleball-related fractures were recorded between 2002 and 2022, which indicated a 90-fold increase in our study period. Based on weighted national average of NEISS sampling, this equated to approximately 5400 fractures annually. Players who sustained pickleball fractures were primarily aged >60 years (n = 344 [87%]; P < .001) and female (n = 273 [69%]; P < .001). Most fractures involved the upper extremity (n = 262 [66%]; P < .001), with the most common ones involving the radius (n = 79 [30%]), humerus (n = 22 [8%]), and ulna (n = 8 [3%]). Fractures were due most commonly to falls (n = 365 [92%]; P < .001) and occurred in the winter months (n = 142 [36%]; P < .001). There was a significant difference in disposition status, with most patients discharged (n = 320 [81%] vs n = 77 [19%] for hospital admission; P < .001). Univariate analysis revealed that age >60 years, male sex, and fractures to the trunk and lower extremity all led to significantly increased odds of being admitted (odds ratios: 2.27, 2.31, 2.89, and 13.8, respectively).
Conclusion:
Between 2002 and 2022, there was a 90-fold increase in pickleball-related fractures. Most fractures were of the upper extremity after a fall in women aged >60 years. Despite female fracture predominance, men were 2.3 times more likely to be admitted after sustaining a fracture.
Keywords: epidemiologic study, fractures, geriatric, pickleball
Before 2020, pickleball and its associated injuries had no representation in the sports literature. Presently, pickleball encompasses a body of almost 9 million “core” players in 2022 in the United States and is experiencing a surge of attention both in the public sphere and orthopaedic community, most likely due to its low barrier to entry including affordability and ease of play.10,15,17,22,24,26 Pickleball is now the fastest-growing sport in the United States for the second year in a row. 27 Between 2019 and 2021, it has grown nearly 40%, with a mean growth rate of 11.5% over the past 5 years. 28
Moreover, the sport is seeing a greater diversity in player age. Traditionally considered a “senior” sport, as greater than half of “core” players are older than 55 years of age, USA Pickleball has recently observed a surge of younger players. Between 2020 and 2021, the growth rate was fastest in players aged 24 years and younger, with a reported increase of 21%. 28 This surge in growth and increased diversity in player age raises clinical attention for injury awareness. Notably, there has been a reported 11-fold increase of pickleball injuries between 2010 and 2019 in the senior population, supporting this as a growing source of orthopaedic trauma. 30 Several studies have described injuries in other racket sports, such as tennis, racquetball, and badminton; however, there is a paucity of literature regarding pickleball.9,13,23 A literature search currently yields fewer than 15 results, with only 2 articles investigating pickleball injuries at large. The first study, pioneered by Forrester, 11 outlines player demographics and injury prevalence. The second study, by Weiss et al, 30 is a more comprehensive examination comparing pickleball and tennis injuries, especially in players aged 60 years and older. However, no studies have yet conducted a detailed analysis of pickleball-related fractures.
The purpose of the current study was to (1) determine the prevalence of and demographic variables associated with pickleball-related fractures among patients evaluated in emergency departments (EDs) captured with a national database in the United States between 2002 and 2022 and (2) identify risk factors influencing patient's disposition status. We hypothesized that due to the rising popularity of pickleball that there would be an increase in pickleball-related fractures.
Methods
As deidentified data were used in this study, institutional review board approval was not needed. This was a descriptive study using the National Electronic Injury Surveillance System (NEISS), the publicly available government-funded database operated by the US Consumer Product Safety and Commission (CPSC). The NEISS database is based on a nationally representative probability sample of hospitals (about 100) in the United States and its territories. All participating hospitals have an NEISS hospital coordinator who abstracts pertinent patient information daily for every ED visit associated with a consumer product or the poisoning of a child younger than 5 years. These coordinators receive standardized training, computers, software, and compensation from the CPSC. 25 Further details regarding NEISS data collection and sampling procedures, changes over time, and statistical handling aspects have been reported by the CPSC. 16 With the NEISS, national estimates can be inferred through the total number of product-related injuries treated in US hospital EDs. Each case that is reported at an NEISS hospital ED is given a weight for which national estimates can be calculated. 25
There have been over 100 publications using the NEISS database since 2010. Strengths of the NEISS database include its randomized selection, systematic data acquisition, and data security. Weaknesses include possible infringement on randomization if hospitals elect to not participate; have a lack of longitudinal data; and have demographic data limited to age, sex, race, and weight.
The protocol for capturing pickleball-related fractures from the NEISS database was adapted from Forrester, 11 whereby cases from 2002 to 2022 (N = 7,676,533) were downloaded from NEISS and imported into Excel (Version 16.85; Microsoft) for query, review, filtering, formatting, and recoding. Variables examined included treatment date, age, sex, body region affected, primary diagnosis, disposition status from the ED, and location type.
Each NEISS record also contains a narrative text field containing descriptive comments from the ED record about the patient, involved product(s)/activity, sequence of events, associated diagnoses, affected body regions, and other information as directly reported by the ED physician. The narrative text field was used to find pickleball cases (since there is no specific NEISS product/activity code for pickleball), refine case selection, assign the mechanism of fracture, determine specified bones (ie, humerus, fibula, ulna, radius if noted), and determine the laterality (right/left) of the fracture.
Identifying Pickleball-Related Fractures
Potential cases were selected with a computer-assisted search of the narrative text field for the case-insensitive strings “pickleball” or “pickle ball” (n = 1318) and the common misspellings “pickelball” or “pickel ball” (n = 19). This is in accordance with Weiss et al. 30 A primary or secondary diagnosis of fracture (NEISS Diagnosis Code 57) was used to exclude all persons with nonfracture injuries (n = 960). Ultimately, 397 pickleball-related fractures in 377 patients were included (Figure 1). If a patient had multiple fractures, separate instances were created for each fracture diagnosis.
Figure 1.
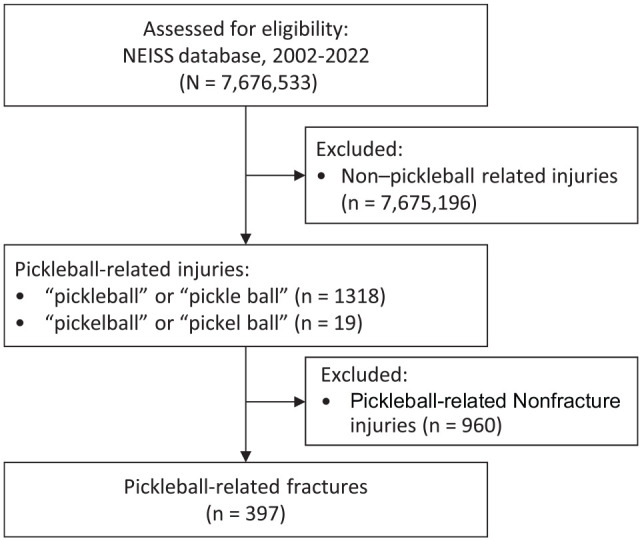
Selection process of 2002-2022 pickleball-related fractures from the NEISS database. NEISS, National Electronic Injury Surveillance System.
Anatomic Body Region Assignment
The body region fractured was grouped into (1) upper extremity (including the categories of shoulder girdle, upper arm, forearm, hand, and unknown); (2) head/neck (including head, neck/cervical spine, and face); (3) lower extremity (including upper leg, lower leg, foot, and unknown); and (4) trunk (including pelvis, rib, and spine), consistent with previous work. 12
Primary Fracture Mechanism Assignment
Each pickleball-related case narrative text was used to assign a fracture mechanism based on a modification of the coding scheme used by Gaw et al 12 to describe how the fracture took place. The primary fracture mechanism for all pickleball records was assigned independently by 2 authors (Y.S.G. and P.Z.); if disagreements arose, a third author (K.P.S.)—an orthopaedic sports medicine expert—was consulted for adjudication. The case narrative text review resulted in assigning each case to a primary mechanism (or to an exclusion category) as follows: fall, contact with an external object, athletic movement (diving, pushing off, etc), and unknown.
Disposition Status
Disposition from the ED was regrouped into 2 categories: (1) discharged to home and (2) hospitalization (including NEISS variables of treated and transferred, treated, and admitted, and held for <24 hours for observation).
Statistical Analysis
Descriptive analysis was performed for all variables related to fracture prevalence and patient characteristics. Contingency table comparisons of categorical variables (stratified age groups, mechanism of fracture, fracture location, and sex) were analyzed using either chi-square or Fisher exact test. Subgroup analysis of fractures based on patient sex was performed. Comparisons of continuous variables (patient age) were performed using 1-way analysis of variance. Bonferroni correction was applied when calculating differences in proportion with multiple comparisons, and Tukey post hoc analysis was performed when calculating analysis of variance tests.
Univariate analysis was performed to examine the odds of hospital admission for pickleball fractures across age, sex, and fracture location.
All statistical analyses were conducted using R Version 4.1.1 (R Foundation). For all analyses, a P value of <.05 was considered statistically significant.
Results
Characteristics of Pickleball-Related Fractures
A total of 377 persons with 397 pickleball-related fractures were identified between 2002 and 2022, resulting in a national estimate of fractures of 23,839 using weighted estimates. There was a 200% increase in pickleball-related fractures between 2020 and 2021. Based on data from the most recent years of approximately 90 fractures per year, this equates to approximately 5400 fractures annually. Results also indicated a 349% increase in pickleball fractures in the most recent 5 years (2017-2022) compared with the previous 5 years (2012-2017) (Figure 2). No pickleball-related fractures were reported before 2005.
Figure 2.

Prevalence of pickleball-related fractures by year, 2002-2022.
The mean age of fracture patients was 66.4 years (median age, 68 years; range, 9-93 years). There were more female (n = 273; 68.8%) than male (n = 124, 31.2%) players who sustained a fracture, and female players were significantly older than male players (67.4 ± 8.8 vs 64.4 ± 16.6 years; P = .02). Fractures were the most likely to occur in players aged 60-69 years (n = 181, 45.6%) and ≥70 years (n = 163, 41.1%). Further information regarding fractures stratified by age group and sex can be found in Figure 3. Of the fracture cases in which race was reported, the largest proportion of fractures came from White players (n = 154, 95.1%). Regarding laterality, 27% (n = 107) of fractures were right-sided and 33.2% (n = 132) were left-sided, with side unknown in the remaining 39.8% (n = 158).
Figure 3.
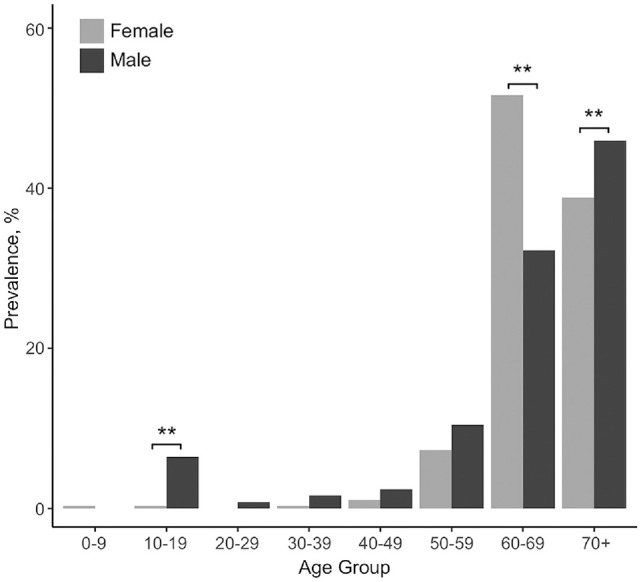
Prevalence of pickleball-related fractures by age group and sex. **Statistically significant difference (P < .05) between the sexes.
There was a significant increase in fractures in the winter months (December-February) (n = 142, 35.8%) compared with summer (n = 65, 16.4%) and fall (n = 87, 21.9%) (P < .001). There was also a statistically significant difference based on day of fracture, with players most likely visiting the ED on Thursdays (n = 74, 18.6%) followed by Fridays (n = 65, 16.4%), Wednesdays (n = 62, 15.6%), Mondays (n = 56, 14.1%), Tuesdays (n = 56, 14.1%), Sundays (n = 42,10.6%), and Saturdays (n = 42,10.6%) (P = .02).
Fracture Location and Mechanism
A comprehensive list of fracture locations and associated bones can be found in Tables 1 and 2. Notably, fractures occurred most commonly in the upper extremity (n = 262, 66.0%; P < .001). Of upper extremity fractures, the most reported bone fractured was the radius (n = 79, 19.9%). The female-to-male upper extremity fracture ratio was 3:1; however, the lower extremity-to-trunk fracture ratio was about 1:1.
Table 1.
Fracture Characteristics by Body Region a
| Body Region | Fractures | Female Patients | Male Patients | Patient Age, y |
|---|---|---|---|---|
| Upper extremity | 262 (66) | 204 (77.9) | 58 (22.1) | 66.9 ± 10.4 |
| Head/neck | 15 (3.8) | 10 (66.7) | 5 (33.3) | 62 ± 17.2 |
| Lower extremity | 77 (19.4) | 37 (48.1) | 40 (51.9) | 64.2 ± 16.4 |
| Trunk | 43 (10.8) | 22 (51.2) | 21 (48.8) | 68.2 ± 7.23 |
| Total | 397 (100) | 273 (68.8) | 124 (31.2) | 66.4 ± 11.87 |
Data are presented as n (%) or mean ± SD.
Table 2.
Number of Fractures With Associated Bones by Body Region
| Body Region | Associated Bones | No. of Fractures |
|---|---|---|
| Upper extremity (n = 262) | ||
| Shoulder girdle | Clavicle, 4; unknown, 14 | 18 |
| Upper arm | Humerus, 23 | 23 |
| Forearm | Radius, 85; ulna, 9; unknown, 89 | 183 |
| Hand | Unknown, 25 | 25 |
| Unknown upper extremity | - | 13 |
| Head/neck (n = 15) | ||
| Head | Skull, 1 | 1 |
| Neck | Cervical spine, 1 | 1 |
| Face | Orbit, 2; nasal bone, 6; mandible, 1; unknown, 4 | 13 |
| Lower extremity (n = 77) | ||
| Upper leg | Femur, 6; unknown, 32 | 38 |
| Lower leg | Fibula, 5; tibia, 2; unknown, 14 | 21 |
| Foot | Calcaneus, 1; unknown, 13 | 14 |
| Unknown lower extremity | - | 4 |
| Trunk (n = 43) | ||
| Pelvis | Pubic ramus, 1; acetabulum, 2; unknown, 3 | 6 |
| Rib | - | 21 |
| Spine | - | 16 |
There was a significant difference in the mechanism of fracture, with the most common mechanism being falls (n = 367, 92.4.%) followed by athletic movement (n = 8, 2%) and contact with an external object (n = 7, 1.76%) (P < .001). The mean age of players with fractures due to falls (67.4 years) was significantly older than those with fractures due to contact with an external object (45.6 years) and due to athletic movement (58 years) (p < .001).
Disposition Status
Of the 397 patients with pickleball-related fractures, 77 (19.4%) required hospital admission, while 320 (80.6%) were discharged (P < .001). In the univariate analysis, age >60 years, male sex, and fracture location trunk or lower extremity were significantly more associated with hospital admission (odds ratios: 2.27, 2.31, 2.89, and 13.8, respectively) (Table 3).
Table 3.
Univariate Analysis of Factors Associated With Hospital Admission for Pickleball-Related Fracture a
| Variable | Odds Ratio (95% CI) | P |
|---|---|---|
| Age, y | ||
| <60 | Reference | - |
| >60 | 2.27 (1.37-3.73) | .001 |
| Sex | ||
| Female | Reference | - |
| Male | 2.31 (1.4-3.9) | .002 |
| Fracture location | ||
| Upper extremity | Reference | - |
| Head/neck | 2.72 (0.72-10.4) | .14 |
| Trunk | 2.89 (1.2-6.8) | .02 |
| Lower extremity | 13.8 (7.37-25.8) | <.001 |
Dashes indicate areas not applicable. Boldface P values indicate statistical significance (P < .05).
The mean age of patients admitted to the hospital was significantly older than those discharged and treated on an outpatient basis (70.0 vs 65.6 years; P = .0028). Of those admitted, female and male patients were of similar ages (69.5 vs 70.7 years, P = .54). Of discharged patients, women were significantly older than men (67 vs 61.8 years, P = .0007). Admitted and discharged women were of similar ages (P = .0901), while admitted men were significantly older than discharged men (P = .0061).
There were 18 pickleball players with multiple fractures: 16 had 2 concurrent fractures and 2 had 3 concurrent fractures. Five players had associated pneumothoraces with rib fractures; 4 (80%) of these patients were admitted to the hospital. Of the 12 players who had concurrent closed head injuries (ie, concussions), 2 were admitted to hospital.
Discussion
The data from this epidemiological study revealed that the number of pickleball-related fractures doubled from 47 to 94 between 2020 and 2021. This doubling in fractures occurred in the setting of a 14% growth in total players, no growth in “core” players, and a 22% growth in the number of “casual” players during that span. 9 While the total increase in players did not double, the larger growth in casual players may have been attributed to 2 times increased fracture risk, as in previous studies, novice athletes were noted to be at higher risk for fracture. This finding may also be due to a lack of pickleball awareness among the ED as well as NEISS data entrants, who could have falsely diluted fracture incidence reporting. Further incidence data and prospective data are needed to elucidate this association.
There was an observed increase in participation of 21% among players aged ≤24 years between 2020 and 2021. 27 Despite this growing younger pickleball player population, most fractures occurred in players who were ≥60 years old, with 86% of fractures involving this demographic, concordant with previously published works. 27 We noted a 90-fold increase in fracture rates since 2005, a 45.5-fold increase since 2010, a 5-fold increase since 2015, and a 1.9-fold increase since 2020.
In our study, sex was observed to play a role in fracture rates, as women accounted for 69% of the fractures during the period studied, despite pickleball having a male predominance (60% male players vs 40% female players). 9 Other racket and paddle sport-related fractures have shown similar distributions of fractures by sex, with women always affected more frequently.3,12 This is likely exacerbated by postmenopausal bone loss for women as they age. Two longitudinal population-based prospective studies have reported that annual loss in bone mineral density was significantly greater in women compared with men ≥60 years old.8,29 This can be attributed to the fact that, although estradiol levels decrease in both men and women as they age, women have from much greater bone loss after menopause due to the loss of production of endogenous ovarian estrogens. 2
Fractures occurred significantly more during the winter months relative to any other season. Given the limitations of this study and the current literature of pickleball, we are unable to ascertain whether this fracture increase was due to increased participation frequency or other reasons. Further prospective studies are needed to elucidate the etiology of this finding. Moreover, the most common mechanism of fracture was via fall for both sexes, with the radius implicated the most often. A ground-level fall is a commonly observed mechanism for sports-related fractures.18,30 Women accounted for 86% of radius fractures, which corroborates work from Weiss et al 30 and epidemiologic injury trends at large.4-6,21 The previously mentioned 2 longitudinal populated-based prospective studies also noted the greatest loss in bone mineral density in the distal radius in women relative to men, which may contribute to this being the most frequently fractured bone during pickleball play.8,29 These findings reflect the relatively high proportion of fractures affecting the distal radius populations as noted above.
To our knowledge, this is the first study reporting the prevalence of pickleball fractures over 2 decades. We believe this was also the first study to examine variables influencing ED disposition status for pickleball-related fractures. In this study, 19.4% (77/397) of all pickleball-related fractures reported at NEISS EDs required hospital admission. Interestingly, despite a female preponderance of fractures, men were 2.3 times more likely than women to be admitted after a pickleball-related fracture. This may be explained by the anatomic region and consequent severity of fractures sustained by men compared with women. In our study, men were more likely to have fractures located in the trunk (male players, 21/124 [16.9%] vs female players, 22/273 [8.1%]) and lower extremity (male players, 40/124 [32.2%] vs female players, 37/273 [13.6%]) relative to women. Fractures of the trunk and lower extremity had 2.89 and 13.8 times the odds of being admitted relative to upper extremity fractures, respectively.
Fractures of the trunk, including those of the pelvis, rib, and spine, may be more severe and complicated due to the proximity to internal organs, which may be damaged by a trunk fracture compared with the extremities. Five pneumothoraces, all in male participants, were reported, and 80% of these patients were admitted. Fractures of the lower extremity, particularly the femur and hip, are known to be more severe, with higher morbidity and mortality rates than fractures of the upper extremity.7,19 Mortality due to hip and femur fractures has also been noted to be significantly higher in men compared with women.1,14,20 Higher admission rates for lower extremity fractures reflect the severity of these fractures and the likely necessity of surgery.
Age may also have played a more substantial role in the disposition status of pickleball-related fractures in men. On further analysis, there was no significant age disparity between sexes in patients who were admitted (69.5 vs 70.7 years; P = .54). However, male patients who were discharged were significantly younger than those who were admitted (P = .0061). This same trend was not true of female patients, suggesting that age more strongly influences disposition status in men. Further studies should investigate the association between sex-based aging and the severity of fracture.
Limitations
This study has several limitations. First, pickleball was not well recognized in the early years of the study period, and during our study period, the sport did not have a product code. Consequently, providers may have been less likely to include this in the patient's injury narrative. In addition, only 46.9% (186/397) of fractured bones were identified in the NEISS database, limiting our data analysis and conclusions. Data from NEISS are limited to patients who presented to EDs in the US, which may restrict the population and be selective for more severe fractures. Patients who were fractured and sought care at urgent care or physician offices were therefore not included in the study. Although the NEISS database provided data with regard to admission status giving us insight into potential severity, surgical status which could also be seen as a marker of injury severity was unable to be assessed as prospective treatment data were not available. The NEISS database was also representative of about only 1.7% of national pickleball-related fractures based on weighted estimates, which can limit the generalizability of our results. In addition, the level of detail provided by NEISS case narratives is limited by the amount of information included by the NEISS coders and heterogeneity of detail reported by ED providers. Therefore, further details surrounding desired information such as the type of fracture, mechanism of fracture, or athlete experience may not be included in this study. Despite these limitations, the strength of this study lies in its large nationally representative sample and the study period, which spans 21 years.
Conclusion
Between 2002 and 2022, there was a 90-fold increase in pickleball-related fracture presenting to the ED, estimated at 5400 fractures annually. Most fractures were of the upper extremity and occurred after a fall in women >60 years old. Despite female fracture predominance, men were 2.3 times more likely to be admitted after sustaining a fracture. Interestingly, there were significant age differences based on disposition status in male patients that were not found in female patients. Further prospective studies are needed to ascertain incidence rates and patient outcomes for pickleball-related fractures. A better understanding of the mechanisms of fracture and their outcomes can lead to prevention strategies to prevent fractures.
Footnotes
Final revision submitted January 3, 2024; accepted February 2, 2024.
One or more of the authors has declared the following potential conflict of interest or source of funding: K.P.S. has received research support from DJO; education payments from Summit Surgical; consulting fees from NovoPedics, Flexion Therapeutics, Emory DSM, and the National Football League; royalties from Obers; and honoraria from NovoPedics. L.K.C. has received hospitality payments from Smith+Nephew. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval was not sought for the present study.
ORCID iD: Kurt P. Spindler  https://orcid.org/0000-0002-0185-6922
https://orcid.org/0000-0002-0185-6922
References
- 1. Abrahamsen B, van Staa T, Ariely R, Olson M, Cooper C. Excess mortality following hip fracture: a systematic epidemiological review. Osteoporos Int. 2009;20(10):1633-1650. [DOI] [PubMed] [Google Scholar]
- 2. Cauley JA. Estrogen and bone health in men and women. Steroids. 2015;99(Pt A):11-15. [DOI] [PubMed] [Google Scholar]
- 3. Changstrom B, McBride A, Khodaee M. Epidemiology of racket and paddle sports-related injuries treated in the United States emergency departments, 2007-2016. Phys Sportsmed. 2022;50(3):197-204. [DOI] [PubMed] [Google Scholar]
- 4. Court-Brown CM, Caesar B. Epidemiology of adult fractures: a review. Injury. 2006;37(8):691-697. [DOI] [PubMed] [Google Scholar]
- 5. Court-Brown CM, Clement ND, Duckworth AD, Aitken S, Biant LC, McQueen MM. The spectrum of fractures in the elderly. Bone Joint J. 2014;96-B(3):366-372. [DOI] [PubMed] [Google Scholar]
- 6. Court-Brown CM, Duckworth AD, Clement ND, McQueen MM. Fractures in older adults. A view of the future? Injury. 2018;49(12):2161-2166. [DOI] [PubMed] [Google Scholar]
- 7. Cummings SR, Melton LJ. Epidemiology and outcomes of osteoporotic fractures. Lancet. 2002;359(9319):1761-1767. [DOI] [PubMed] [Google Scholar]
- 8. Daly RM, Rosengren BE, Alwis G, Ahlborg HG, Sernbo I, Karlsson MK. Gender specific age-related changes in bone density, muscle strength and functional performance in the elderly: a 10-year prospective population-based study. BMC Geriatr. 2013;13:71. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9. Dines JS, Bedi A, Williams PN, et al. Tennis injuries: epidemiology, pathophysiology, and treatment. J Am Acad Orthop Surg. 2015;23(3):181-189. [DOI] [PubMed] [Google Scholar]
- 10.Feldman J.What is pickleball, and how did it become so popular? Published online March 13, 2023. Accessed May 15, 2023. https://www.sportico.com/business/sports/2023/history-of-pickleball-1234712282/
- 11. Forrester MB. Pickleball-related injuries treated in emergency departments. J Emerg Med. 2020;58(2):275-279. [DOI] [PubMed] [Google Scholar]
- 12. Gaw CE, Chounthirath T, Smith GA. Tennis-related injuries treated in United States emergency departments, 1990 to 2011. Clin J Sport Med. 2014;24(3):226-232. [DOI] [PubMed] [Google Scholar]
- 13. Guermont H, Le Van P, Marcelli C, Reboursière E, Drigny J. Epidemiology of injuries in elite badminton players: a prospective study. Clin J Sport Med. 2021;31(6):e473-e475. [DOI] [PubMed] [Google Scholar]
- 14. Haentjens P, Magaziner J, Colón-Emeric CS, et al. Meta-analysis: excess mortality after hip fracture among older women and men. Ann Intern Med. 2010;152(6):380-390. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15. Harrell A. How pickleball became America's fastest growing sport. National Geographic. Published online October 17, 2022. Accessed May 15, 2023. https://www.nationalgeographic.com/history/article/pickleball-is-for-everyone-inside-americas-fastest-growing-sport
- 16. Hazard and Injury Data Systems: NEISS: Background. US Consumer Product Safety Commission. Accessed May 15, 2023. https://www.cpsc.gov/epidemiology/cpsc_epi/NEISS_background.html
- 17. How to Prevent and Treat Pickleball Injuries. Atrium Health Wake Forest Baptist. Published online February 6, 2023. Accessed May 15, 2023. https://newsroom.wakehealth.edu/news-releases/2023/02/how-to-prevent-and-treat-pickleball-injuries
- 18. Kaiser P, Stock K, Benedikt S, et al. Acute tennis injuries in the recreational tennis player. Orthop J Sports Med. 2021;9(1):2325967120973672. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19. Kanis JA, Oden A, Johnell O, De Laet C, Jonsson B, Oglesby AK. The components of excess mortality after hip fracture. Bone. 2003;32(5):468-473. [DOI] [PubMed] [Google Scholar]
- 20. Kannegaard PN, van der Mark S, Eiken P, Abrahamsen B. Excess mortality in men compared with women following a hip fracture. National analysis of comedications, comorbidity and survival. Age Ageing. 2010;39(2):203-209. [DOI] [PubMed] [Google Scholar]
- 21. Lauritzen JB, Schwarz P, Lund B, McNair P, Transbøl I. Changing incidence and residual lifetime risk of common osteoporosis-related fractures. Osteoporos Int. 1993;3(3):127-132. [DOI] [PubMed] [Google Scholar]
- 22. Legget P. Pickleball: common injuries and best treatments in today's hottest sport. Published online November 7, 2022; updated September 15, 2023. Accessed May 15, 2023. https://www.novanthealth.org/healthy-headlines/pickleball-common-injures-and-best-treatments-in-todays-hottest-sport
- 23. Maylack FH. Epidemiology of tennis, squash, and racquetball injuries. Clin Sports Med. 1988;7(2):233-243. [PubMed] [Google Scholar]
- 24. Mullen S. America’s fastest-growing sport is a cross of tennis, pingpong and badminton. Published online February 19, 2022. Accessed April 21, 2023. https://www.npr.org/2022/02/19/1081257674/americas-fastest-growing-sport-pickleball
- 25. NEISS frequently asked questions. US Consumer Product Safety Commission. Accessed May 15, 2023. https://www.cpsc.gov/Research—Statistics/NEISS-Injury-Data/Neiss-Frequently-Asked-Questions.
- 26. Quirolgico KM. Stretches and exercises to prevent pickleball injuries. Hospital for Special Surgery website. Published online November 16, 2022. Accessed May 15, 2023. https://www.hss.edu/article_stretches-exercises-prevent-pickleball-injuries.asp [Google Scholar]
- 27. Robbins S. Pickleball is the fastest-growing sport for second year in a row, growing by 39.3%. USA Pickleball website. Published online February 16, 2022. Accessed May 15, 2023. https://usapickleball.org/news/fastest-growing-sport/ [Google Scholar]
- 28. USA Pickleball. 2023 USA Pickleball fact sheet. Accessed May 15, 2023. USA-Pickleball-Fact-Sheet-2023.pdf [Google Scholar]
- 29. Warming L, Hassager C, Christiansen C. Changes in bone mineral density with age in men and women: a longitudinal study. Osteoporos Int. 2002;13(2):105-112. [DOI] [PubMed] [Google Scholar]
- 30. Weiss H, Dougherty J, DiMaggio C. Non-fatal senior pickleball and tennis-related injuries treated in United States emergency departments, 2010-2019. Inj Epidemiol. 2021;8(1):34. [DOI] [PMC free article] [PubMed] [Google Scholar]