

Swellings
It is not unknown for people to discover and worry about oral lumps, but they usually first notice a lump because it becomes sore. Pathological causes include a range of different lesions, but neoplasms are most important (see earlier article).
Causes of salivary gland swelling
| • Inflammatory (mumps, ascending sialadenitis, recurrent juvenile parotitis, HIV sialadenitis, other infections such as tuberculosis, Sjogren's syndrome, sarcoidosis) | • Neoplasms |
| • Cystic fibrosis | • Duct obstruction |
| • Sialosis | |
| • Drugs (such as protease inhibitors) | |
| • Deposits (such as amyloid) | |
Most salivary swellings are caused by mucoceles in minor glands in the lower lip. These are best removed surgically. In the major glands salivary duct obstruction is more common, but sialadenitis, Sjogren's syndrome, and neoplasms are important causes to be excluded. It can be difficult to establish whether a salivary gland is genuinely swollen, especially in obese patients. A useful guide to whether a patient has parotid enlargement is to look for outward deflection of the ear lobe, which is seen in true parotid swelling.
Management—Diagnosis is mainly clinical, but investigations such as serology for autoantibodies or HIV antibodies, liver function tests, and needle or open biopsy may be indicated. Treatment is of the underlying cause.
Lesions which may present as lumps or swellings in the mouth
| Normal | Inflammatory | Cystic | Drugs |
| • Pterygoid hamulus | • Abscess | • Eruption cysts | • Phenytoin |
| • Parotid papillae | • Pyogenic granuloma | • Developmental cysts | • Cyclosporin |
| • Lingual papillae | • Crohn's disease | • Cysts of infective origin | • Calcium channel blockers |
| • Unerupted teeth | • Orofacial granulomatosis | Fibro-osseous | Blood dyscrasias |
| Developmental | • Sarcoidosis | • Fibrous dysplasia | • Leukaemia and lymphoma |
| • Haemangioma | • Wegener's granulomatosis | • Paget's disease | Neoplasms |
| • Lymphangioma | • Others | Hormonal | • Benign and malignant |
| • Maxillary and mandibular tori | Traumatic | • Pregnancy epulis or gingivitis | Others |
| • Hereditary gingival fibromatosis | • Epulis | • Oral contraceptive pill gingivitis | • Angio-oedema |
| • Von Recklinghausen's | • Fibroepithelial polyp | • Amyloidosis | |
| neurofibromatosis | • Denture granulomas | ||
Red oral lesions
Most red oral lesions are inflammatory in nature, but some are potentially malignant, especially erythroplasia.
Causes of red lesions
| Widespread redness | Localised red patches |
| • Candidiasis | • Candidiasis |
| • Iron deficiency | • Erythroplasia |
| • Avitaminosis B | • Purpura |
| • Irradiation mucositis | • Telangiectases |
| • Lichen planus | • Angiomas |
| • Mucosal atrophy | • Kaposi's sarcoma |
| • Polycythaemia | • Burns |
| • Lichen planus | |
| • Lupus erythematosus | |
| • Avitaminosis | |
Erythroplasia (erythroplakia)
Erythroplasia is a rare, isolated, red, velvety lesion that affects patients mainly in their 60s and 70s. It usually involves the floor of the mouth, the ventrum of the tongue, or the soft palate. This is one of the most important oral lesions because 75-90% of lesions prove to be carcinoma or carcinoma in situ or are severely dysplastic. The incidence of malignant change is 17 times higher in erythroplasia than in leucoplakia. Erythroplasia should be excised and sent for histological examination.
• Erythroplasia is an isolated red lesion that typically occurs in elderly people• It is usually dysplastic or malignant and is bestremoved
Erythematous candidiasis
Erythematous candidiasis may complicate treatment with corticosteroids or antimicrobials and cause widespread erythema and soreness of the oral mucosa, sometimes with thrush. It may also occasionally be seen in HIV infection, xerostomia, diabetes, and in people who smoke.
Red persistent lesions are especially noticeable on the palate and tongue. Median rhomboid glossitis (central papillary atrophy) is a red depapillated rhomboidal area in the centre of the tongue dorsum, now believed to be associated with candidiasis. Biopsy may show pseudoepitheliomatous hyperplasia, but the condition is not potentially malignant.
Management—Erythematous candidiasis may respond to stopping smoking and antifungal agents (usually fluconazole).
Denture induced stomatitis (denture sore mouth)
This is a common form of mild chronic erythematous candidiasis, usually seen after middle age as erythema limited to the area beneath an upper denture. The fitting surface of the denture is infested mainly with Candida albicans. Despite its name, this condition is rarely sore, though angular stomatitis may be associated. Patients are usually otherwise healthy.
Factors that predispose to denture induced stomatitis include wearing dentures (especially through the night), poor oral and denture hygiene, xerostomia, and carbohydrate-rich diets. It is not caused by allergy to the denture material.
Management includes
• Denture stomatitis occurs mainly when Candida spp proliferate beneath and infest the denture• It may be asymptomatic but may be associated with angular stomatitis• Denture wearing should be minimised and the infection eradicated
Eradicating infection by soaking dentures overnight in chlorhexidine or 1% (v/v) hypochlorite solution then using miconazole denture lacquer. Metal dentures should not be soaked in hypochlorite as they may discolour
Using miconazole gel (5 ml), nystatin pastilles (100 000 units), or amphotericin lozenges (10 mg) in the mouth four times daily for up to one month
Using systemic fluconazole 50 mg daily for resistant cases
Adjustment of the dentures.
Other red lesions
Petechiae are usually caused by trauma or suction but may also be seen in thrombocytopenia, amyloidosis, localised oral purpura, or scurvy. Telangiectasia may be a feature of hereditary haemorrhagic telangiectasia or systemic sclerosis.
White oral lesions
White lesions were formerly called leucoplakia and believed
often to be potentially malignant. The term leucoplakia is now restricted to white lesions of unknown cause. Most white lesions are innocuous keratoses caused by cheek biting, friction, or tobacco use, but other conditions must be excluded, usually by biopsy. These include infections (such as candidiasis, syphilis, and hairy leucoplakia), dermatoses (usually lichen planus), and neoplastic disorders (such as leucoplakias and carcinomas). Chronic candidiasis may produce tough, adherent white patches (chronic hyperplastic candidiasis or candidal leucoplakias), which can have a malignant potential and may clinically be indistinguishable from other leucoplakias, though they may be speckled.
Main causes of white oral lesions
| • Idiopathic keratosis | • Infections |
| • Carcinoma | Candidiasis |
| • Skin grafts | Hairy leucoplakia |
| • Physical or chemical | Syphilitic keratosis |
| Friction | Papillomas (some) |
| Burns | • Mucocutaneous disease |
| Chemicals | Lichen planus |
| Tobacco | Lupus erythematosus |
| Snuff | Inherited lesions (such as white sponge naevus) |
| Sanguinarine | |
Keratosis (leucoplakia)
This is a persistent adherent white patch. Keratoses are most commonly uniformly white plaques (homogenous leucoplakia), prevalent in the buccal mucosae, and are usually of low malignant potential. More serious are non-homogenous keratoses (nodular and, especially, speckled leucoplakias), which consist of white patches or nodules often in a red, commonly eroded, area of mucosa. The presence of severe epithelial dysplasia indicates a considerable risk of malignant development. The overall prevalence of malignant change is 3-33% over 10 years, but a proportion of such malignancies (about 15%) regress spontaneously.
• The aetiology of leucoplakia is unclear• Less than a third of lesions turn malignant in 10 years• It is good practice to exclude dysplasia by biopsy• Leucoplakia is best removed
It can be difficult to be certain of the precise diagnosis of a white patch, as even carcinoma can present as a white lesion. Biopsy is indicated, and indurated, red, erosive, or ulcerated areas should be sampled rather than the more obvious whiter hyperkeratinised areas; staining with toluidine blue may help highlight the most appropriate area. An oral brush biopsy may be helpful, but incisional biopsy is needed if carcinoma is strongly suspected.
Management can be difficult, especially in extensive lesions of leucoplakia and those with areas of erythroplasia. Obvious predisposing factors must be reduced or eliminated. Some studies have shown regression of leucoplakia in over half of patients who stopped smoking for a year. Others have shown vitamin A and various retinoids to have beneficial effects, but these are teratogenic and may have other adverse effects such as hyperlipidaemia, and often produce only temporary benefit. Dysplastic lesions should be excised (laser is useful), and patients should then be followed up regularly at intervals of 3-6 months. Unfortunately, excised lesions sometimes recur.
Lichen planus
Oral lichen planus is common, mainly occurs after middle age, and typically presents as bilateral white lesions (papules, plaques, or reticular areas) in the buccal and lingual mucosae. Lesions may be symptomless. The less common but painful erosive lichen planus typically affects the tongue or buccal mucosae on both sides.
Biopsy is usually necessary to exclude dysplasia, keratosis, lupus erythematosus, chronic ulcerative stomatitis associated with autoantibodies to nuclear proteins (CUSP), and other disorders. Some lichenoid lesions may be drug induced (such as by non-steroidal anti-inflammatory drugs) or occasionally related to factors such as materials used in dental work, hepatitis C infection, or graft versus host disease.
Management—Topical corticosteroids are useful in controlling symptoms. In view of the slight risk (about 1%) of oral carcinoma in non-reticular lichen planus, patients should be regularly reviewed.
• Lichen planus is common• There is no single cause, but it is often idiopathic and may be related to drug use or dental materials.• Diagnosis from leucoplakia and lupus erythematosus can be difficult• It is often treated with topical corticosteroids
Candidiasis (candidosis, moniliasis, thrush)
Oral carriage of Candida albicans is more common in people who smoke and those who are ill. C albicans is the most common cause of candidiasis, which can arise in patients after recent use of antibiotics or corticosteroids, immunosuppressive drugs, cytotoxic chemotherapy, or irradiation; in those with xerostomia, immunodeficiencies such as leukaemia or AIDS, malnutrition, or diabetes; and in neonates, who have little immunity to Candida spp. The soft, creamy patches of thrush can be wiped off the mucosa, leaving erythema.
• Candidiasis may be seen in healthy neonates• It otherwise indicates local immunosuppressive treatment, xerostomia, or an immune defect
Management—Avoid smoking, treat predisposing causes (such as xerostomia), and improve oral hygiene. Chlorhexidine has some anti-candidal activity, and antifungal drugs can be used, the choice depending on the severity and extent of disease, medical contraindications, and other complications of an immunocompromising condition.
Hairy leucoplakia
This is an asymptomatic white lesion not removable by wiping that is typically seen on the lateral margins of the tongue in immunocompromised patients, usually those with HIV infection or AIDS. It is associated with Epstein-Barr virus and has no known malignant potential, but it is a predictor of poor prognosis and, in HIV infection, is an AIDS-defining condition.
Treatment is usually not required, but it resolves with aciclovir or anti-retroviral agents.
Pigmented oral lesions
Furred, brown, and black hairy tongue
The tongue in healthy children is seldom furred, but healthy adults sometimes have a coating of epithelial, food, and microbial debris, particularly if they are edentulous, have a soft non-abrasive diet, have poor oral hygiene, smoke, are fasting or ill, or are using antimicrobials or chlorhexidine. Black hairy tongue is an extreme example that affects mainly the posterior dorsum of tongue. The filiform papillae are long and stained by accumulated debris.
Management—The condition is improved by increasing oral hygiene, brushing the tongue, using a tongue scraper, increasing dietary fruit and roughage (pineapple may help), and using sodium bicarbonate mouthwashes.
Localised hyperpigmented lesions
Haemangiomas, purpura, and Kaposi's sarcoma give rise to localised red and purple lesions. Brown or black lesions are usually amalgam tattoos or naevi, but melanomas must be excluded.
Generalised mucosal hyperpigmentation
This is usually racial in origin or caused by smoking or betel use and only occasionally has a systemic cause such as drugs, Addison's disease, or ectopic production of adrenocorticotrophic hormone (such as by bronchogenic carcinoma).
Further reading
| • Lee LA, Walsh P, Prater CA, Su LJ, Marchbank A, Egbert TB, et al. Characterization of an autoantigen associated with chronic ulcerative stomatitis: the CUSP autoantigen is a member of the p53 family. J Invest Dermatol 1999;113:146-51 | • Scully C, Beyli M, Feirrero M, Ficarra G, Gill Y, Griffiths M, et al. Update on oral lichen planus: aetiopathogenesis and management. Crit Rev Oral Biol Med 1998;9:86-122 |
| • Mashberg A. Early diagnosis of asymptomatic oral and oropharyngeal squamous cancers. CA Cancer J Clin 1995;45:328-51 | • Scully C, Cawson RA. Potentially malignant oral lesions. J Epidemiol Biostatistics 1996;1:3-12 |
| • Schoelch ML, Sekandari N, Regezi JA, Silverman S. Laser management of oral leukoplakias: a follow-up study of 70 patients. Laryngoscope 1999;109:949-53 | • Scully C, Flint S, Porter SR. Oral diseases. London: Martin Dunitz, 1996 |
| • Sciubba JJ. Improving detection of precancerous and cancerous oral lesions: computer-assisted analysis of the oral brush biopsy. J Am Dent Assoc 1999;130:1445-57 | • Triantos D, Porter SR, Scully C, Teo CG. Oral hairy leukoplakia; clinicopathological features, pathogenesis, diagnosis and clinical significance. Clin Infect Dis 1997;25:1392-6 |
• Hyperpigmentation in the buccal cavity may be due to racial origin or caused by dental amalgam, drugs, using tobacco or betel, naevi, or, rarely, melanoma• Brown tongue is usually caused by poor diet or oral hygiene
Causes of brown or black pigmented mucosal lesions
| • Ephelis (freckle) | • Drugs (such as phenothiazines, zidovudine, minocycline) |
| • Racial | • Smoking |
| • Naevus | • Heavy metals |
| • Malignant melanoma | • Addison's disease (and related disorders) |
| • Kaposi's sarcoma | • Other rare causes |
| • Peutz-Jegher's syndrome | |
| • Amalgam or graphite tattoo | |
Figure.

Mucocele in a typical site
Figure.
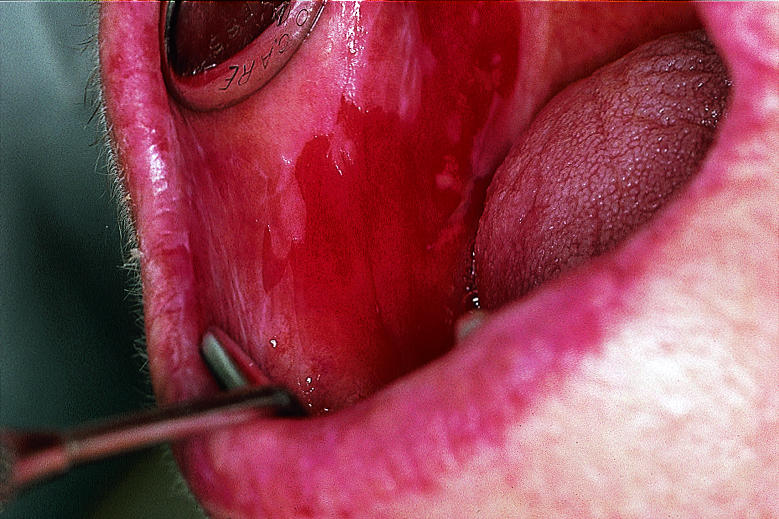
Erythroplasia has high malignant potential
Figure.

Chronic atrophic candidiasis beneath an upper denture
Figure.

Leucoplakia of lower gingivae—a typical site for this type of lesion
Figure.

Lichen planus of dorsum of tongue
Figure.

Acute pseudomembranous candidiasis in patient with drug induced immunosuppression
Figure.

Hairy leucoplakia on lateral margin of tongue of patient with AIDS
Figure.

Black hairy tongue in patient who, by chance, also has erythema migrans (see previous article)
Figure.

Haemangioma of left buccal mucosa. Unlike Kaposi's sarcoma, this lesion blanches on pressure
Acknowledgments
Crispian Scully is grateful for the advice of Rosemary Toy, general practitioner, Rickmansworth, Hertfordshire.
Footnotes
Crispian Scully is dean and Stephen Porter is professor of oral medicine at the Eastman Dental Institute for Oral Health Care Sciences, University College London, University of London (www.eastman.ucl.ac.uk).
The ABC of oral health is edited by Crispian Scully and will be published as a book in autumn 2000.