

Abstract
Background
The mental health of university students during the COVID-19 pandemic has attracted the attention of researchers. For the present study researchers constructed a mediation model to explore the relationship between psychological resilience and post-traumatic growth, the mediating role of negative emotions and the moderating role of deliberate rumination in students.
Methods
The Psychological Resilience Scale, Posttraumatic Growth Inventory, Depression-Anxiety-Stress Scale (DASS-21) and Event Related Rumination Inventory were used in a survey of 881 college students. The data were analyzed using SPSS 26.0 and the PROCESS plugin (version 3.3).
Results
(1) Psychological resilience is positively related with post-traumatic growth. Deliberate rumination is positively related to psychological resilience, posttraumatic growth, and negative emotions. Psychological resilience, post-traumatic growth and negative emotions are negatively related. (2) Negative emotions mediated the relationship between psychological resilience and post-traumatic growth. (3) Deliberate rumination plays a moderating role in psychological resilience affecting negative emotions. Deliberate rumination plays a moderating role in the extent to which psychological resilience influences PTG through negative emotions.
Conclusions
Psychological resilience affects post-traumatic growth directly and also indirectly through negative emotions. With the increase of mental resilience, the level of negative emotion tended to decrease. When individuals are experiencing negative emotions, high levels of active rumination are more likely to promote post-traumatic growth. This study helps to explore the factors affecting the mental health of college students during the epidemic, thus providing guidance for appropriate mental health interventions.
Keywords: Psychological resilience, Post-traumatic growth, Negative emotions, Deliberate rumination, Moderated mediation model, COVID-19
Background
The novel coronavirus pneumonia (COVID-19) is a global health threat, and its spread has had a huge impact on the mental health of people around the world. Its rapid development, the speed of spread and the number of people infected has so far taken on unprecedented proportions in more than 150 countries [1]. Global public health and social systems are collapsing under the strain of the coronavirus, and governments have taken extreme public health measures [2] that have caused widespread disruption to social structures and economic activity [3]. Restrictive measures such as quarantines can affect mental health and emotional responses to the pandemic itself [4–6].
Recently published studies have shown that psychological problems such as anxiety and depression are common during epidemics. For example, at the beginning of the COVID-19 outbreak in China, more than half of the population rated its psychological impact as moderate to severe, and about a third of participants reported moderate to severe anxiety [7]. Similarly, prevalence rates of depression and anxiety in North America ranged from 44.1% to 47.2% respectively in Canada [8] to 24.4% and 28.2% in the United States [9]. Similar negative effects on mental health were reported in other countries [10–13].
University students are among the groups whose mental health has been most severely affected by the pandemic [14–16]. Relevant studies have found that the overall prevalence of depression among these students was 23.8% [17], and the proportion of anxiety 24.9%, of which 0.9% was considered severe [18]. A reasonable explanation for this state of affairs is that students were under pressure from both the pandemic and their studies, making them susceptible to a mental disease [19–21].
Social media is one of the main channels for receiving up-to-date information about COVID-19 [22], and while students enjoy its convenience, they may also suffer from information overload, which can cause mental health problems [23]. Due to the pandemic, Chinese educational institutions turn to online instruction, and the lack of learning self-discipline at home has a negative impact on academic achievement, which may have increased depression, anxiety and stress [7]. A number of studies have also shown differences between male and female students with regard to resilience, perception, recovery and growth in the face of trauma [16]. For these reasons, during the COVID-19 outbreak it was important to increase awareness of mental health issues among university students and to adopt positive strategies to address these.
Research has shown that psychological resilience can be a strategy for addressing the mental health challenges posed by the COVID-19 pandemic [24]. This personality trait, explained more comprehensively below, can help individuals cope with the negative psychological effects of traumatic events, including the COVID-19 pandemic [25].
In the last 20 years, with the rise and development of positive psychology, researchers have found that, in addition to exhibiting symptoms of stress, individuals experiencing trauma can derive benefit and experience growth [26]. Research results that link psychological resilience and post-traumatic growth (PTG) have been available for some time; however, the relationship between these two phenomena is contested. It has been suggested that individuals with high psychological resilience scores have low levels of PTG [27] because, although they may experience emotional pain and behavioral or health changes, these are temporary in nature. Their high level of resilience makes them less reactive to traumatic events, and the events are not sufficiently shocking to their existing cognitive schemas, so PTG is less likely to occur [28]. However, other research has shown that high levels of psychological resilience can enhance PTG [29].
The existing literature suggests that negative emotions may be an important mediating variable between psychological resilience and PTG. Such emotions have often been found to be associated with both variables [30, 31]; however, few studies have focused on the possible mediating role of negative emotions between psychological resilience and PTG. In addition, the process of deliberate rumination may contribute to the process of psychological recovery when individuals make sense of their emotions and explore the meaning of the causes and consequences of negative events [32]. Therefore, when individuals experience negative emotions after a traumatic event, their level of psychological resilience and the interaction between PTG, ruminative thinking and future mental health merit further study.
The aim of this study was to investigate the relationship between psychological resilience and PTG, and the mediating role of negative emotions between them, with deliberate rumination included as a moderating factor in the model. As well, gender, a factor that may significantly influence psychological resilience and negative emotions, was added as a covariate and was controlled for in the process.
Theories and hypotheses
Psychological resilience
Individual responses to stress and trauma vary greatly, and so people may react differently to the emotional distress caused by a traumatic event such as the COVID-19 pandemic [33]. Psychological resilience, as defined by the American Psychological Association in 2016, is “the process of adapting well in the face of adversity, trauma, tragedy, threats, and even major stressors” [34] (p. 2). This personality trait enables individuals to cope better with stressful or traumatic events and plays an important role in overcoming the adverse effects of stressful environments [35]. In sport, for example, where athletes must overcome difficult challenges in order to succeed, psychological resilience enables individuals to adapt to unfavorable conditions [36]. Although psychological resilience is difficult to measure, previous research has shown that people with higher levels of psychological resilience tend to achieve better mental-health outcomes (e.g., with depression, anxiety and post-traumatic stress disorder) following natural and human-made disasters [37]. Preliminary evidence of the general psychological resilience of adults can be found in studies such as those on people’s bereavement [38, 39] and the terrorist attacks on the World Trade Center in New York City, USA, in 2001 [40]. Therefore, during the novel coronavirus pneumonia, increasing psychological resilience should be a primary public-health priority.
Post-traumatic growth
A growing number of studies have shown that PTG may be a positive outcome following traumatic events. The definition of trauma in the Diagnostic and Statistical Manual of Mental Disorders considers that “the person has been exposed to a traumatic event in which both of the following were present: (1) the person experienced, witnessed, or was confronted with an event or events that involved actual or threatened death or serious injury, or a threat to the physical integrity of self or others and (2) the person’s response involved intense fear, helplessness, or horror.” [41] People facing a major life crisis (either direct or indirect) often experience distressing emotions, and post-traumatic growth is accompanied by attempts to adapt to highly negative circumstances [42]. Tedeschi and Calhoun [26] suggested that PTG has the following four characteristics: (a) the traumatic event is shocking; (b) the psychological aspect of the struggle with the traumatic event is experienced as positive; (c) the individual’s level of functioning in at least one area is higher than it was before the traumatic event; and (d) growth and psychological distress co-exist [27]. The introduction of the concept of PTG has gradually led to a new perspective on stress and trauma research—a positive growth orientation with a focus on PTG [43]. The COVID-19 pandemic has created an environment in which survival can be in doubt. A more vulnerable environment leads to fear or increased fear of non-survival [44]. Based on the definition of trauma, the COVID-19 pandemic is similar to a profound existential crisis or traumatic experience. How university students coped with and adjusted to this experience, and whether they were able to carry on and grow as a result, is a key research question. Studies have pointed out that there are significant gender differences in the prevalence of post-traumatic stress symptoms (PTSS) [45].
Other existing research shows that psychological resilience is positively correlated with PTG. High levels of psychological resilience can contribute to PTG [29]. Optimism, one dimension of psychological resilience, has been shown to be moderately correlated with PTG [26]. Most people are likely to be exposed to traumatic experiences such as interpersonal violence, death of a loved one, natural disasters, serious industrial or other accidents, war and terrorism to some extent [46–50]. Although these experiences may affect mental health and lead to conditions such as post-traumatic stress disorder [51], the vast majority of individuals exposed to violent or life-threatening events do not develop this disorder. An individual’s level of psychological resilience is a major reason for this outcome. The relationship between psychological resilience and PTG among college students during the COVID-19 outbreak merits attention. Therefore, we propose the following hypothesis:
H1: The psychological resilience of college students has a positive correlation with PTG.
Negative emotions
Depression, anxiety and stress are risk factors that affect mental health. Previous studies have also found that 28.6% of Chinese students have symptoms of depression [52], and 59.2% have academic stress [53]. In addition, 7.6% of Chinese people suffer from life-long anxiety disorders [54]. There is a close relationship between depression, anxiety and stress [55], and Henry & Crawford believe that the three phenomena can be combined into a higher-order psychological variable called negative emotions [56]. These negative emotions are strongly associated with negative outcomes such as suicidal behavior [57, 58]. and they are negatively correlated with quality of life [59, 60].
Psychological resilience is strongly associated with negative emotions. Research has shown that negative emotions such as anxiety and depression have a negative impact on the development of psychological resilience [61, 62], but some researchers have linked psychological resilience to better mental health outcomes, suggesting that higher psychological resilience predicts lower levels of depression, anxiety and stress [63, 64] and that psychological resilience reduces the likelihood of developing depression [31]. Other researchers consider resilience to be a facilitator of well-being [65] and an indicator of adolescent development [66]. College students are in a period of rapid physical and psychological development, and only a resilient psyche can cope with the negative emotions of depression, anxiety and stress in everyday life. The role of psychological resilience in regulating and associating negative emotions among college students is particularly important in situations where COVID-19 has triggered a variety of lifestyle changes that also lead to a high incidence of negative emotions. Therefore, we propose the following hypothesis:
H2a: Psychological resilience among college students is negatively associated with negative emotions.
A moderately positive relationship between negative emotions and PTG has been reported [67]. The model of PTG proposed by Tedeschi and Calhoun [42] suggests that events leading to psychological stress stimulate cognitive processing, and that when such thinking is constructive individuals think positively about their post-traumatic self, others and the world, contributing to PTG. This means that the individual experiencing negative emotions may also experience PTG. Negative life events such as the COVID-19 outbreak, inevitably lead to negative emotions among college students, but whether this results in PTG has been less studied and reported on. Therefore, the following hypotheses is proposed:
H2b: Negative emotions of college students have a positive correlation with PTG.
On the basis of the literature and the three hypotheses mentioned above, we further propose the following hypothesis:
H2c: Negative emotions of university students act as a mediator between psychological resilience and PTG.
Deliberate rumination
After a traumatic event, and especially after a global traumatic event like COVID-19, individuals may revisit or reconsider their beliefs. This cognitive process is referred to as rumination [68]. There are many different classifications of ruminant, and the classification method of Tedeschi et al. [42] will be adopted in this paper. He categorized ruminant into intrusive rumination and deliberate rumination. Intrusive rumination is a non-constructive cognition process whereby a traumatic event passively intrudes into an individual’s cognition, and they ponder negative states and emotions in an evaluative manner. Conversely, deliberate rumination is a constructive cognition process whereby the individual consciously thinks positively about the cues related to the traumatic event, tending to face the dilemma openly and solve the problem. The following is a list of some of the most important features.
Researchers have also begun to explore the relationship between rumination and psychological resilience, suggesting that deliberate rumination, which involves making sense of one’s emotions and exploring the causes and consequences of negative events, may contribute to the process of psychological recovery [69]. Those with high levels of psychological resilience are more likely to focus on and process positive information and the positive aspects of their personal experiences [70] and therefore have higher levels of deliberate rumination. As well, psychological resilience and rumination were included when factors that influence recovery from post-traumatic stress were explored [71], with psychological resilience considered as facilitating recovery and rumination as hindering it. However, the relationship between these two variables has been the subject of little discussion. Therefore, we propose the following hypothesis:
H3a: The psychological resilience of college students has a positive correlation with deliberate rumination.
Research has consistently found that stress, anxiety, depressive symptoms and other negative emotions are associated with rumination. For example, cross-sectional studies have shown that people who are more prone to negative emotions have stronger negative rumination and weaker positive rumination than normal people [72]. More important, longitudinal studies have found that negative emotions are associated with increased rumination [73, 74]. In one study, the relationship between rumination and anxiety was significant, with a correlation coefficient of 0.32 [75]. However, deliberate rumination, which represents a constructive form of deep thinking, may relate differently with negative emotions than in previous studies. Therefore, the following hypothesis is proposed for this study.
H3b: Negative emotions in college students has a negative correlation with deliberate rumination.
On the basis of the literature and the above two hypotheses, we further propose the following hypothesis:
H3c: The interaction of psychological resilience and deliberate rumination has a negative correlation with negative emotions.
Researchers have argued in the literature that deliberate rumination can promote PTG [68, 76, 77]. PTG is the positive result of struggling with and coping with a traumatic event, and cognitive processing plays a key role in its development [42]. Deliberate rumination enables a person to actively reflect on and reevaluate their cognitive processes and ways of thinking after trauma and to shift their personal attention to its positive aspects [78]. Therefore, we propose the following hypothesis:
H4a: Deliberate rumination by college students has a correlation with PTG.
On the basis of the literature and the two hypotheses presented above, we further propose the following hypothesis:
H4b: The interaction of negative emotions and deliberate rumination has a positive correlation with PTG.
In summary, based on the relationship between psychological resilience and PTG, we propose a moderator-mediator model (see Fig. 1). Our aim is to provide insight into how (in the mediating role of negative emotions) and under what circumstances (the mediating role of deliberate rumination) psychological resilience leads to higher levels of PTG.
Fig. 1.
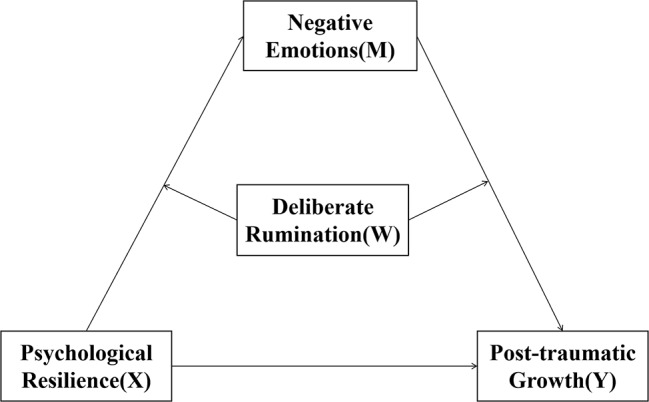
Moderated mediation model of the present research
Materials and methods
Participants and procedure
The study was carried out at an independent college in Guangdong Province, China. The college has more than 20,000 undergraduate and specialist students in 44 disciplines. Here is the formula to determine the sample size:
 |
n is the sample size, Z is the standard error, p is the variance of the population estimate, and e is the permissible error.
When the 95% confidence interval, Z is 1.96. p is taken to be 0.5 for prudent estimation. The formula calculation shows that at least 385 participants are needed for this study. A total of 918 students completed a questionnaire. Questionnaires for non-Guangdong students were removed from the data, reducing the sample size to 881. Sample size is higher than 385.This method of data selection is to better understand the relevant situation of students in epidemic areas and make this study more targeted. The respondents comprised 317males (35.982%) and 564 females (64.018%), all from a single year. To generate research ideas and hypotheses, exploratory focus-group interviews were conducted at the college before the research design was finalized. Interviews were convened by the course teacher and conducted online. The majority of the interviewees indicated that they had experienced negative emotions for a variety of reasons during COVID-19. Some students also said that they could better regulate their emotions when they had negative emotions because of their high ability to resist pressure. Other students said that thinking about positive things can help them recover and even gain something.
Data were collected for this study between April 10 and June 15, 2020 using an online questionnaire survey. The QR code for the questionnaire was presented to students enrolled in same-level English classes during a break. (In China, QR codes are widely used for such tasks as information retrieval, mobile payments and internet links, and they are informative, easy to identify and cost-effective.) The study received an ethical review from the School of Geographic Sciences, South China Normal University. Before students filled out the questionnaire, we asked “Do you agree to participate in this survey?” online to investigate the willingness of the students to participate in the survey, with students ticking “1” if they agreed and “2” otherwise. The study was explained to them after obtaining their consent to participate in the survey and the students completed the questionnaire on a voluntary basis.
Measures
The questionnaire used in this study consisted of five sections: (a) demographic data, (b) Psychological Resilience Scale, (c) Post-Traumatic Growth Inventory, (d) Depression, Anxiety and Stress Scale –DASS-21, and (e) Event Related Rumination Inventory. The demographic information section included gender and current place of residence. To check the accuracy of the existing Chinese version, the English versions of the scales were translated into Chinese using a back-translation method [79]. One researcher translated the English versions into Chinese, then another researcher translated the Chinese versions back into English, and finally a third researcher compared the original, translated and back-translated versions to check for equivalence between the original English versions and the translated Chinese versions. Any non-equivalence was resolved prior to data collection. All scales selected for this study had been used in other studies in the Chinese context and had good reliability and validity [80–83].
Psychological resilience scale
The Psychological Resilience Scale used in this study was proposed by Hu and Gan [80] after reviewing conceptualizations of psychological resilience proposed by Chinese and foreign scholars [84]. The scale’s 27 items are divided into five dimensions: (a) goal focus (5 items), (b) emotional control (6 items), (c) positive perception (4 items), (d) family support (6 items) and (e) interpersonal assistance (6 items). A 5-point Likert rating is used:0.1 = completely disagree, 2 = somewhat disagree, 3 = unsure, 4 = somewhat agree, and 5 = completely agree. The theoretical score ranges from 27 to 135. The higher the score, the greater the psychological resilience of the participant. The Cronbach α coefficient for this scale was 0.860 and its 95% confidence intervals were [0.836,0.879].
Posttraumatic growth inventory
This study used the Post-Traumatic Growth Inventory, originally proposed by Tedeschi and Calhoun [26, 30] and translated into Chinese by Geng et al. [81] to suit the Chinese context. The 21-item scale is divided into five dimensions: (a) interpersonal relationships (7 items), (b) new possibilities (5 items), (c) personal strengths (4 items), (d) spiritual change (2 items) and (e) appreciation of life (3 items). A 6-point Likert scale is used: 1 = never; 2 = few; 3 = a few; 4 = medium; 5 = more; 6 = most. The theoretical score ranges from 21 to 126. The higher the score, the higher the degree of post-traumatic growth. The Cronbach α coefficient for this scale was 0.958 and its 95% confidence intervals were [0. 955,0.961].
Depression-anxiety-stress scale 21 – DASS-21
The Depression-Anxiety-Stress Scale 21 – DASS-21 used in this study was revised by Lovibond, which has 21 items divided into three dimensions: depression, anxiety and stress [85]. Each dimension has 7 items. The Likert scale used has 4 points: 1 = not conforming, 2 = somewhat conforming, 3 = often conforming, 4 = always conforming. The theoretical score ranges from 21 to 84. The higher the score, the higher the frequency of the depression, anxiety and stress conditions. The Cronbach α coefficient for this scale was 0.960 and its 95% confidence intervals were [0.956,0.963].
Event related rumination inventory
The study used the “Deliberate Rumination” section of the Event-Related Rumination Scale proposed by Cann et al. in 2011 [68], which consists of 10 items. A 4-point Likert rating is used: 1 = not at all, 2 = sometimes, 3 = often, and 4 = always. The theoretical score ranges from 10 to 40. The higher the score, the higher the frequency of deliberative rumination. The Cronbach α coefficient of this scale was 0.913 and its 95% confidence intervals were [0.903,0.920].
Data analysis
In this study, statistical analysis of the data was mainly carried out using SPSS 26.0 statistical software. Firstly, Harman’s single-factor test was used to test for common method bias [86]. Secondly, a series of descriptive analyses were carried out to test for trends in concentration and dispersion of the data. Pearson product moment correlation coefficients were then calculated to test the relationships between the independent, mediator, moderator and dependent variables. Finally, moderator-mediator models of psychological resilience and PTG were tested using the PROCESS plugin (version 3.3) in SPSS, developed by Hayes specifically for path analysis-based moderator and mediator analyses and their combinations [87]. Bias-corrected 95% confidence intervals for conditional direct and indirect effects were estimated from 5,000 data resamples, and the effects were significant when the confidence intervals did not include zero [75, 88]. In addition, gender was used as a control variable in this study.
Results
Testing for common method bias
In order to ensure the validity of the data analysis, the common method bias (CMB) was first investigated by the Harman single factor test. CMB refers to the fact that the use of the same type of data source, the same measurements or the same data collection environment may result in artificial covariances between association and criterion variables and impose an unrealistic relationship between them [86, 89]. As all data in this study were collected using self-report questionnaires, in the same environment and over the same time period, this source of bias needed to be controlled and tested.
The Harman single-factor test was used to carry out principal component analysis of all 79 items in the questionnaire (except demographic variables). The results showed that 15 components had eigenvalues greater than 1. The contribution of the 15 components to the total variance was 64.735%. As can be seen from the Scree plot (Fig. 2), the curve tends to be stable after the eighth component, and the contribution rate of the eight components to the total variance is 60.252%. The first component accounting for only 20.868%, well below 40%, which is the cut-off value for classifying the magnitude of common method deviations [90]. Therefore, it can be stated that there was no significant common method bias in this study. In other words, the covariance between the dependent and independent variables in this study is largely attributable to their nature rather than to the measurement methods used in the data-collection process.
Fig. 2.

Scree plot
Descriptive and correlation analysis
Table 1 summarizes the results of the descriptive and correlational analyses of the four variables in this study. The study showed that the psychological resilience of college students was significantly and positively correlated with PTG, deliberate rumination (r = 0.414, p < 0.01; r = 0.077, p < 0.05) and negatively correlated with negative emotions (r=-0.469, p < 0.01). PTG was significantly positively correlated with deliberate rumination (r = 0.353, p < 0.01) and negatively correlated with negative emotions (r = -0.081, p < 0.05). Deliberate rumination was also significantly and positively correlated with negative emotions (r = 0.158, p < 0.01).
Table 1.
Mean, standard deviation and correlations between variables
| Variables | M | SD | 1 | 2 | 3 | 4 |
|---|---|---|---|---|---|---|
| 1. Psychological Resilience | 3.417 | 0.443 | 1 | |||
| 2. Post-Traumatic Growth | 3.302 | 1.002 | 0.414** | 1 | ||
| 3. Negative Emotions | 1.626 | 0.562 | -0.496** | -0.081* | 1 | |
| 4. Deliberate Rumination | 2.012 | 0.520 | 0.077* | 0.353** | 0.158** | 1 |
Note. N = 881
*p<0.05, **p<0.01 (2-tailed)
Testing the mediation model
The mediation analysis was conducted using psychological resilience as the independent variable, PTG as the dependent variable and negative emotions as the mediating variable (model 4) in PROCESS (version 3.3). The results, summarized in Table 2, showed that gender had a certain impact on students’ psychological resilience and negative emotions(β=-0.073, p < 0.05). Psychological resilience positively associated PTG (β = 1.127, p < 0.001), after controlling for gender. Psychological resilience negatively associated negative emotions (β=-0.623, p < 0.001), whereas negative emotions positively associated PTG (β = 0.289, p < 0.001). The total effect of psychological resilience on PTG was 0.946 (95% CI = [0.810, 1.083]) as tested by the bias-corrected percentile bootstrap method, with direct (95% CI = [0.972, 1.282]) and indirect (95% CI = [-0.270, -0.093]) effects. These results mean that psychological resilience can have a direct impact on PTG or an indirect impact on PTG through negative emotions.
Table 2.
Analysis of the mediation effect
| Independent Variable | STEP1 | STEP2 | STEP3 | ||||||
|---|---|---|---|---|---|---|---|---|---|
| Post-Traumatic Growth | Negative Emotions | Post-Traumatic Growth | |||||||
| β | SE | t | β | SE | t | β | SE | t | |
| Gender | -0.110 | 0.064 | -1.715 | -0.073 | 0.034 | -2.126* | -0.089 | 0.064 | -1.399 |
| Psychological Resilience | 0.946 | 0.070 | 13.607*** | -0.623 | 0.037 | -16.763*** | 1.127 | 0.079 | 14.262*** |
| Negative emotions | 0.289 | 0.062 | 4.632*** | ||||||
| R2 | 0.175 | 0.250 | 0.194 | ||||||
| F | 92.807*** | 146.320*** | 70.466*** | ||||||
Note. N = 881
*p<0.05, **p<0.01, ***p<0.001 (2-tailed)
Testing the moderated mediation model
After adding moderator (deliberate rumination) to the first and second halves of the mediation model, Model 58 was used to analyze the moderated mediation model. The results showed (see Table 3) that gender differences exist between the variables in this model (β=-0.091, p < 0.05; β=-0.153, p < 0.05). The correlation of psychological resilience and deliberate rumination was statistically significant in affecting negative emotions (β = -0.155, t = -2.546, p < 0.001). This suggests that deliberate rumination can play a moderating role in psychological resilience affecting negative emotions. Similarly, the correlation of negative emotions and deliberate rumination was also statistically significant in affecting PTG (β = -0.297, t = -3.822, p < 0.001), suggesting that deliberate rumination also plays a moderating role in the extent to which psychological resilience influences PTG through negative emotions.
Table 3.
Moderated mediation test
| Independent Variable | STEP1 | STEP2 | ||||
|---|---|---|---|---|---|---|
| Negative Emotions | Post-Traumatic Growth | |||||
| β | SE | t | β | SE | t | |
| Gender | -0.091 | 0.033 | -2.734* | -0.153 | 0.060 | -2.564* |
| Psychological Resilience | -0.637 | 0.036 | -17.594*** | 0.961 | 0.075 | 12.756*** |
| Deliberate Rumination | 0.217 | 0.031 | 7.037*** | 0.639 | 0.057 | 11.131*** |
|
Psychological Resilience* Deliberate Rumination |
-0.155 | 0.061 | -2.546* | |||
| Negative Emotions | 0.145 | 0.060 | 2.411* | |||
|
Negative Emotions* Deliberate Rumination |
-0.297 | 0.078 | -3.822*** | |||
| R2 | 0.296 | 0.297 | ||||
| F | 92.080*** | 73.840*** | ||||
Note. Analyses conducted using PROCESS model 14. N = 881
*p<0.05, **p<0.01, ***p<0.001
We further analyzed the regulatory role of deliberate rumination using a simple slope test. The adjustment variables were grouped according to the mean score of deliberate rumination plus or minus one standard deviation. The mean plus one standard deviation was designated as the high deliberate rumination group, while the mean minus one standard deviation was designated as the low deliberate rumination group. The analysis leads to the following conclusions:
When the level of deliberate rumination was low, as the level of psychological resilience increased, the level of negative emotion showed a tendency to decrease (Effect=-0.555, t=-11.238, p < 0.001).
When the level of deliberate rumination was high, as the level of psychological resilience increased, the level of negative emotion showed a more significant tendency to decrease than the low level. (Effect=-0.717, t=-15.300, p < 0.001).
When the level of deliberate rumination was low, as the level of negative emotions increased, the level of post-traumatic growth significantly increased (Effect = 0.300, t = 4.099, p < 0.001).
When the level of deliberate rumination was high, as the level of negative emotions increased, there was no significant change in the level of post-traumatic growth (Effect=-0.009, t=-0.129, p>0.5).
The above results suggest that after controlling for gender variables, deliberate rumination played a significant moderating role in the relationship between psychological resilience and negative emotion, and negative emotion and post-traumatic growth.
Table 4.
Conditional indirect effect at specific levels of deliberate rumination when mediated by psychological resilience
| Moderator Variable | Effect | se | t | 95%CI | |
|---|---|---|---|---|---|
| LLCI | ULCI | ||||
| M-1SD | -0.555 | 0.049 | -11.238 | -0.653 | -0.459 |
| M | -0.634 | 0.036 | -17.594 | -0. 708 | -0.566 |
| M + 1SD | -0.717 | 0.047 | -15.300 | -0.810 | -0.626 |
Table 5.
Conditional indirect effect at specific levels of deliberate rumination when mediated by negative emotion
| Moderator Variable | Effect | se | t | 95%CI | |
|---|---|---|---|---|---|
| LLCI | ULCI | ||||
| M-1SD | 0.299 | 0.073 | 4.094 | 0.156 | 0.443 |
| M | 0.145 | 0.06 | 2.411 | 0.027 | 0.263 |
| M + 1SD | -0.01 | 0.072 | -0.134 | -0.150 | 0.131 |
Fig. 3.

The relationship between psychological resilience and negative emotion for high and low levels of deliberate rumination
Fig. 4.

The relationship between negative emotion and post-traumatic growth for high and low levels of deliberate rumination
Fig. 5.

The standardized estimate values of the final model
Discussion
Discussion of the results
The results are generally consistent with the hypotheses offered in the present study and the conclusions of previous studies, although the hypotheses related to deliberate rumination were not confirmed. According to the literature, exposure to public-health emergencies (such as the Ebola epidemic [91], earthquakes [92] and SARS [93]) has caused mental-health problems. The COVID-19 pandemic and its preventive measures have also greatly affected mental health. Early studies of the COVID-19 outbreak reported significant psychological effects from both the outbreak and the response, suggesting that study participants exhibited high levels of psychopathological symptoms [7]. Furthermore, gender is a consistent factor affecting psychological outcomes: women are relatively more vulnerable to psychological distress than men, exhibiting moderate levels of anxiety [7, 14]. It has also been noted that there are significant gender differences in the prevalence of post-traumatic stress symptoms (PTSS) [45]. The results of the present study suggest that females are associated with increased anxiety, depression and stress. This finding is consistent with previous research findings [94].
Another possible explanation for poorer mental health during the COVID-19 outbreak is related to information overload [95]. A recent study in mainland China found that the higher the frequency of social media exposure, the higher the likelihood of anxiety [23].
First, these results are consistent with H1 and also with the results of other studies that confirmed the existence of a relationship between psychological resilience and PTG [96, 97]. College with greater psychological resilience reported higher levels of PTG [29, 30]. According to relevant studies, resilience has been widely studied in other populations including patients, political refugees and survivors of natural disasters, which previously highlighted strong psychological resilience can help person better endure trauma during the event, recover and maintain more positive mental health state after the event [98–100]. Psychological resilience is associated with numerous desired health outcomes [101, 102]. Colleges with higher psychological resilience have a greater sense of self-control, are more optimistic in their outlook, are stronger and more optimistic in the face of trauma, are more positive about their traumatic experiences, and mobilize their own personal and environmental resources to help them move beyond the trauma. It also depends on individual qualities or skill in coping with adversity navigating and negotiating to resources [103]. In addition, individuals who demonstrate psychological resilience or PTG are significantly more resistant to possible future traumatic events [104].
Second, the findings are consistent with H2a, H2b and those of other studies. In this study, psychological resilience negatively affected negative emotions, similarly to conclusions of Ren and Cai [105]. In our undergraduate participants, we observed that the psychological resilience of college students was a negative association of negative emotions. This is consistent with the findings of Way K. W. Lua, who used cross hysteresis to study the relationship between mental resilience of college students and symptoms of depression and anxiety, and this research showed that psychological resilience of college students negatively affected depressive symptoms in a certain period of time [106]. Psychological resilience has been extensively studied in diverse groups such as adult refugees, patients with depression, and college students without mental illness, but few studies have focused on the mediating effect of negative emotions on mental resilience. However, our findings are consistent with previous emphasis on the potential protective effects of mental resilience on mental health in different populations. Poudel Tandukar K et al. showed in their study that adult refugees with the highest mental resilience had the lowest risk of above-threshold anxiety and depression [99]. Chen, N. et al. believe that anxiety and depression can be alleviated by improving the psychological resilience of patients with depression [107]. These findings suggest that the negative association of mental resilience and negative emotions apply to different groups. Furthermore, negative emotions negatively affect PTG. This is consistent with the findings of narrative analysis by Zieba et al., students in the high PTG group mentioned more positive emotions than negative emotions in the narrative [108]. The degree of negative emotions caused by various traumatic events was relatively high in college students, but negative emotions did not significantly affect PTG [109, 110]. Negative emotions can give individuals negative psychological feelings and hinder their recovery from traumatic experiences, thus affecting the formation of PTG [111]. The findings of other studies have demonstrated that the expression of negative emotions through venting can facilitate the development of PTG at higher levels [112]. Emotional expression and emotional processing can affect PTG in traumatized individuals [113, 114].
Third, the results of this study are consistent with H2c and the results of other studies. These studies suggest that negative emotions play a mediating and buffering role in psychological resilience and PTG. Psychological resilience is positively correlated with mental health [115]. When faced with stressful or adverse situations, those with higher levels of psychological resilience tend to experience lower levels of depression or anxiety and have the ability to recover more quickly to the pre-crisis stage and reach a pre-stress baseline more quickly [116]. However, those with lower levels of psychological resilience have more difficulty coping with the emotional challenges of a pandemic crisis [34]. A study of U.S. adults found that psychological resilience was negatively correlated with the level of concern about COVID-19: individuals with higher levels of psychological resilience were less affected by future anxiety and the perceived threat of COVID-19, and thus experienced less impact on their subjective well-being, than those with lower levels of psychological resilience [117]. Such negative emotional reactions during a disaster can predict the occurrence of mental health problems after the disaster [118]. Therefore, people with higher levels of psychological resilience are able to grow more in response to COVID-19 induced emotional distress [116].
Fourth, the findings contradict hypotheses H3a, H3b, H3c, H4a and H4b. Previous research has shown that for many people coping with a variety of negative emotions in their lives, deliberate rumination on an event involves a process of examination of the event and its meaning [119]. Therefore, students with higher psychological resilience are better able to reduce their negative emotions through deliberate rumination. This is due to the fact that deliberate rumination is a variety of recurrent, event-related thinking that includes understanding the meaning of the event, problem solving, recollection of the event, and anticipation of the future [120]. At the same time, when trauma occurs, individuals with higher levels of deliberate rumination are able to evaluate and interpret the traumatic event rationally, try to discover the meaning embedded in the traumatic event, reconstruct their perceptions of the traumatic event and the world, i.e. they engage in deliberate rumination about the traumatic event, and thus gain post-traumatic growth [121]. The students in this study were still studying at home online during the study period and had been exposed to the traumatic experiences of the epidemic. Therefore, their psychological health problems should be actively intervened to promote the moderating effect of deliberate rumination. And the related mechanisms are yet to be studied in depth in follow-up.
Implications
The main theoretical implication of this study is the confirmation of the link between psychological resilience and PTG, which deepens the focus on these two phenomena and their interaction in a highly traumatic situation like a pandemic. By analyzing mediating and moderating effects, it was found that higher psychological resilience among college students may lead to a reduction in negative emotions, and then to PTG. Furthermore, deliberate rumination negatively regulates this mediation model, a finding that is inconsistent with previous research findings.
In practical terms, the relationship between the four variables proposed in this study may help to mitigate the occurrence of negative emotions among college students, and subsequently promote their physical and psychological well-being, growth and success during the pandemic.
Limitations and future directions
There are also some limitations to this study. First, this study used a cross-sectional design. Although cross-sectional studies combined with data analysis can analyze relationships between variables, causality cannot be determined reliably. Future researchers could use a longitudinal survey design to collect data over time. Second, the data were all collected using self-report methods, and although the Harman single-factor test results suggested the absence of common-method bias, future studies could profitably use a combination of parent reports and teacher evaluations to collect data. Moreover, data collection began on April 10, 2020, when PTG was not evident enough. This could be followed up further in future studies. Finally, all participants were from one university, which may undermine the generalizability of the findings. In the future, recruiting participants from different institutions could strengthen generalizability.
Conclusion
COVID-19 is considered to be among those recent epidemics with the most serious psychosocial impact, and interventions are needed to assist people improve their mental health. This study explored the relationship between psychological resilience and PTG among college students during the COVID-19 pandemic, as well as the mediating role of negative emotions between the two and the moderating role of deliberate rumination in the pre- and post-pathway. The results showed that psychological resilience was positively associated with PTG and that negative emotions partially mediated between psychological resilience and PTG. Furthermore, deliberate rumination affected both the front and back half of PTG by regulating psychological resilience through negative emotions. The mental health and well-being of college students is a major concern for education authorities and universities, and attention to, research on and interventions with the psychological outcomes of university students who have experienced traumatic events are of paramount importance. The results of this study may help us understand the factors that influenced the mental health of college students during the COVID-19 pandemic and thus lead to appropriate mental-health interventions that enable positive change after their traumatic experiences.
Acknowledgements
We would like to thank the students who completed the questionnaire for their contributions to our research study. We would also like to thank those who made assisted with language revision.
Abbreviations
- DASS
21 Depression-Anxiety-Stress Scale
- COVID
19 Novel coronavirus pneumonia
- PTG
Post Traumatic growth
- PTSS
Post traumatic stress symptoms
- CMB
Common method bias
Author contributions
Conceptualization: YX and WZ; methodology: YX and WZ; formal analysis: YN, JY, JW, WZ and YX; writing—original draft preparation: YX, YN, JY, JW, YL, JL, WZ, YZ, DH, XW, JS, ZZ and QL; writing—review and editing: YX and WZ. All authors have read and agreed to the published version of the manuscript.
Funding
This research was funded by the Guangdong Planning Office of Philosophy and Social Science, grant number GD20CJY19.
Data availability
The datasets used and/or analyzed during the current study are not publicly available. Permissions could be obtained/required from the corresponding author on a reasonable request.
Declarations
Ethics approval and consent to participate
The ethical approval was obtained from the Ethics Committee of South China Normal University and based on the Declaration of Helsinki. All participants in the study gave informed consent.
Consent for publication
Not applicable.
Competing interests
The authors declare no competing interests.
Footnotes
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
References
- 1.Liu Y, Gayle AA, Wilder-Smith A, Rocklöv J. The reproductive number of COVID-19 is higher compared to SARS coronavirus. J Travel Med. 2020;27:taaa021. doi: 10.1093/jtm/taaa021. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Xiao H, Shu W, Li M, Li Z, Tao F, Wu X, et al. Social distancing among medical students during the 2019 Coronavirus Disease pandemic in China: Disease awareness, anxiety disorder, Depression, and behavioral activities. IJERPH. 2020;17:5047. doi: 10.3390/ijerph17145047. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Nicola M, Alsafi Z, Sohrabi C, Kerwan A, Al-Jabir A, Iosifidis C, et al. The socio-economic implications of the Coronavirus Pandemic (COVID-19): a review. Int J Surg. 2020;78:185–93. doi: 10.1016/j.ijsu.2020.04.018. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Pietrabissa G, Simpson SG. Psychological consequences of social isolation during COVID-19 outbreak. Front Psychol. 2020;11:2201. doi: 10.3389/fpsyg.2020.02201. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Rossi R, Socci V, Talevi D, Mensi S, Niolu C, Pacitti F, et al. COVID-19 pandemic and lockdown measures impact on mental health among the general population in Italy. Front Psychiatry. 2020;11:790. doi: 10.3389/fpsyt.2020.00790. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.López-Bueno R, Calatayud J, Ezzatvar Y, Casajús JA, Smith L, Andersen LL, et al. Association between current physical activity and current perceived anxiety and mood in the initial phase of COVID-19 confinement. Front Psychiatry. 2020;11:729. doi: 10.3389/fpsyt.2020.00729. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Wang C, Pan R, Wan X, Tan Y, Xu L, Ho CS, et al. Immediate psychological responses and associated factors during the initial stage of the 2019 Coronavirus Disease (COVID-19) epidemic among the general population in China. IJERPH. 2020;17:1729. doi: 10.3390/ijerph17051729. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Nwachukwu I, Nkire N, Shalaby R, Hrabok M, Vuong W, Gusnowski A, et al. COVID-19 pandemic: age-related differences in measures of stress, anxiety and depression in Canada. IJERPH. 2020;17:6366. doi: 10.3390/ijerph17176366. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Twenge JM, Joiner TE. Mental distress among U.S. adults during the COVID-19 pandemic. J Clin Psychol. 2020;76:2170–82. doi: 10.1002/jclp.23064. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.El-Zoghby SM, Soltan EM, Salama HM. Impact of the COVID-19 pandemic on mental health and social support among adult egyptians. J Community Health. 2020;45:689–95. doi: 10.1007/s10900-020-00853-5. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Mazza C, Ricci E, Biondi S, Colasanti M, Ferracuti S, Napoli C, et al. A nationwide survey of psychological distress among Italian people during the COVID-19 pandemic: Immediate psychological responses and associated factors. IJERPH. 2020;17:3165. doi: 10.3390/ijerph17093165. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Roy D, Tripathy S, Kar SK, Sharma N, Verma SK, Kaushal V. Study of knowledge, attitude, anxiety & perceived mental healthcare need in Indian population during COVID-19 pandemic. Asian J Psychiatry. 2020;51:102083. doi: 10.1016/j.ajp.2020.102083. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Stanton R, To QG, Khalesi S, Williams SL, Alley SJ, Thwaite TL, et al. Depression, anxiety and stress during COVID-19: associations with changes in physical activity, sleep, tobacco and alcohol use in Australian adults. IJERPH. 2020;17:4065. doi: 10.3390/ijerph17114065. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Qiu J, Shen B, Zhao M, Wang Z, Xie B, Xu Y. A nationwide survey of psychological distress among Chinese people in the COVID-19 epidemic: implications and policy recommendations. Gen Psych. 2020;33:e100213. doi: 10.1136/gpsych-2020-100213. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Zhou Y, MacGeorge EL, Myrick JG. Mental health and its predictors during the early months of the COVID-19 pandemic experience in the United States. IJERPH. 2020;17:6315. doi: 10.3390/ijerph17176315. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Solomou I, Constantinidou F. Prevalence and predictors of anxiety and depression symptoms during the COVID-19 pandemic and compliance with precautionary measures: age and sex matter. IJERPH. 2020;17:4924. doi: 10.3390/ijerph17144924. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Chi X, Becker B, Yu Q, Willeit P, Jiao C, Huang L, et al. Prevalence and Psychosocial Correlates of Mental Health Outcomes among Chinese College Students during the Coronavirus Disease (COVID-19) pandemic. Front Psychiatry. 2020;11:803. doi: 10.3389/fpsyt.2020.00803. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Talevi D, Socci V, Carai M, Carnaghi G, Faleri S, Edoardo Trebbi, et al. Mental health outcomes of the CoViD-19 pandemic. Rivista Di Psichiatria. 2020 doi: 10.1708/3382.33569. [DOI] [PubMed] [Google Scholar]
- 19.Huang Y, Zhao N. Generalized anxiety disorder, depressive symptoms and sleep quality during COVID-19 outbreak in China: a web-based cross-sectional survey. Psychiatry Res. 2020;288:112954. doi: 10.1016/j.psychres.2020.112954. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Ahmed MZ, Ahmed O, Aibao Z, Hanbin S, Siyu L, Ahmad A. Epidemic of COVID-19 in China and associated psychological problems. Asian J Psychiatry. 2020;51:102092. doi: 10.1016/j.ajp.2020.102092. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Kumar B, Shah MAA, Kumari R, Kumar A, Kumar J, Tahir A. Depression, anxiety, and stress among final-year medical students. Cureus. 2019 doi: 10.7759/cureus.4257. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Bao Y, Sun Y, Meng S, Shi J, Lu L. 2019-nCoV epidemic: address mental health care to empower society. Lancet. 2020;395:e37–8. doi: 10.1016/S0140-6736(20)30309-3. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.Gao J, Zheng P, Jia Y, Chen H, Mao Y, Chen S, et al. Mental health problems and social media exposure during COVID-19 outbreak. PLoS ONE. 2020;15:e0231924. doi: 10.1371/journal.pone.0231924. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.Prime H, Wade M, Browne DT. Risk and resilience in family well-being during the COVID-19 pandemic. Am Psychol. 2020;75:631–43. doi: 10.1037/amp0000660. [DOI] [PubMed] [Google Scholar]
- 25.Liu CH, Zhang E, Wong GTF, Hyun S, Hahm H. Chris. Factors associated with depression, anxiety, and PTSD symptomatology during the COVID-19 pandemic: clinical implications for U.S. young adult mental health. Psychiatry Res. 2020;290:113172. doi: 10.1016/j.psychres.2020.113172. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26.Tedeschi RG, Calhoun LG. The posttraumatic growth inventory: measuring the positive legacy of trauma. J Traum Stress. 1996;9:455–71. doi: 10.1002/jts.2490090305. [DOI] [PubMed] [Google Scholar]
- 27.Levine SZ, Laufer A, Stein E, Hamama-Raz Y, Solomon Z. Examining the relationship between resilience and posttraumatic growth: resilience and growth. J Traum Stress. 2009;22:282–6. doi: 10.1002/jts.20409. [DOI] [PubMed] [Google Scholar]
- 28.Bonanno GA. Loss, trauma, and human resilience: have we underestimated the human capacity to thrive after extremely aversive events? Am Psychol. 2004;59:20–8. doi: 10.1037/0003-066X.59.1.20. [DOI] [PubMed] [Google Scholar]
- 29.Hooper LM, Marotta SA, Lanthier RP. Predictors of growth and distress following childhood parentification: a retrospective exploratory study. J Child Fam Stud. 2008;17:693–705. doi: 10.1007/s10826-007-9184-8. [DOI] [Google Scholar]
- 30.Blackmon BJ, Lee J, Cochran DM, Kar B, Rehner TA, Baker AM. Adapting to life after Hurricane Katrina and the deepwater horizon oil spill: an examination of psychological resilience and depression on the Mississippi Gulf Coast. Social Work Public Health. 2017;32:65–76. doi: 10.1080/19371918.2016.1188746. [DOI] [PubMed] [Google Scholar]
- 31.Salo JA, Qouta S, Punamäki R-L. Adult attachment, posttraumatic growth and negative emotions among former political prisoners. Anxiety Stress Coping. 2005;18:361–78. doi: 10.1080/10615800500289524. [DOI] [Google Scholar]
- 32.Dunn J, Occhipinti S, Campbell A, Ferguson M, Chambers SK. Benefit finding after cancer: the role of optimism, intrusive thinking and social environment. J Health Psychol. 2011;16:169–77. doi: 10.1177/1359105310371555. [DOI] [PubMed] [Google Scholar]
- 33.Killgore WDS, Taylor EC, Cloonan SA, Dailey NS. Psychological resilience during the COVID-19 lockdown. Psychiatry Res. 2020;291:113216. doi: 10.1016/j.psychres.2020.113216. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 34.Association AP. The road to resilience. Washington, DC; 2016.
- 35.Southwick SM, Bonanno GA, Masten AS, Panter-Brick C, Yehuda R. Resilience definitions, theory, and challenges: interdisciplinary perspectives. Eur J Psychotraumatology. 2014;5:25338. doi: 10.3402/ejpt.v5.25338. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 36.Hill Y, Den Hartigh RJR, Meijer RR, De Jonge P, Van Yperen NW. Resilience in sports from a dynamical perspective. Sport Exerc Perform Psychol. 2018;7:333–41. [Google Scholar]
- 37.Osofsky HJ, Osofsky JD, Hansel TC. Deepwater horizon oil spill: Mental health effects on residents in heavily affected areas. Disaster med Public Health prep. 2011;5:280–6. doi: 10.1001/dmp.2011.85. [DOI] [PubMed] [Google Scholar]
- 38.Bonanno GA, Wortman CB, Lehman DR, Tweed RG, Haring M, Sonnega J, et al. Resilience to loss and chronic grief: a prospective study from preloss to 18-months postloss. J Personal Soc Psychol. 2002;83:1150–64. doi: 10.1037/0022-3514.83.5.1150. [DOI] [PubMed] [Google Scholar]
- 39.Bonanno GA, Moskowitz JT, Papa A, Folkman S. Resilience to loss in bereaved spouses, bereaved parents, and bereaved gay men. J Personal Soc Psychol. 2005;88:827–43. doi: 10.1037/0022-3514.88.5.827. [DOI] [PubMed] [Google Scholar]
- 40.Bonanno GA, Rennicke C, Dekel S. Self-enhancement among high-exposure survivors of the September 11th Terrorist Attack: resilience or social maladjustment? J Personal Soc Psychol. 2005;88:984–98. doi: 10.1037/0022-3514.88.6.984. [DOI] [PubMed] [Google Scholar]
- 41.American Psychiatric Association. Diagnostic and statistical manual of mental disorders (4th ed.). Washington, DC.
- 42.Tedeschi RG, Calhoun LG, TARGET ARTICLE Posttraumatic growth: conceptual foundations and empirical evidence. Psychol Inq. 2004;15:1–18. doi: 10.1207/s15327965pli1501_01. [DOI] [Google Scholar]
- 43.Joseph S, Linley PA. Growth following adversity: theoretical perspectives and implications for clinical practice. Clin Psychol Rev. 2006;26:1041–53. doi: 10.1016/j.cpr.2005.12.006. [DOI] [PubMed] [Google Scholar]
- 44.Emanuel L, Solomon S, Fitchett G, Chochinov H, Handzo G, Schoppee T, et al. Fostering existential maturity to manage terror in a pandemic. J Palliat Med. 2021;24:211–7. doi: 10.1089/jpm.2020.0263. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 45.Liu N, Zhang F, Wei C, Jia Y, Shang Z, Sun L, et al. Prevalence and predictors of PTSS during COVID-19 outbreak in China hardest-hit areas: gender differences matter. Psychiatry Res. 2020;287:112921. doi: 10.1016/j.psychres.2020.112921. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 46.Dimitry L. A systematic review on the mental health of children and adolescents in areas of armed conflict in the Middle East: The impact of war on children living in the Middle East. Child: Care, Health and Development. 2012;38:153–61. [DOI] [PubMed]
- 47.Eisenberg N, Silver RC. Growing up in the shadow of terrorism: youth in America after 9/11. Am Psychol. 2011;66:468–81. doi: 10.1037/a0024619. [DOI] [PubMed] [Google Scholar]
- 48.Furr JM, Comer JS, Edmunds JM, Kendall PC. Supplemental material for disasters and youth: a meta-analytic examination of posttraumatic stress. J Consult Clin Psychol. 2010;:a0021482.supp. [DOI] [PubMed]
- 49.Masten AS, Narayan AJ. Child development in the context of disaster, war, and terrorism: pathways of risk and resilience. Annu Rev Psychol. 2012;63:227–57. doi: 10.1146/annurev-psych-120710-100356. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 50.Osofsky HJ, Osofsky JD. Hurricane Katrina and the gulf oil spill. Psychiatr Clin North Am. 2013;36:371–83. doi: 10.1016/j.psc.2013.05.009. [DOI] [PubMed] [Google Scholar]
- 51.Karam EG, Friedman MJ, Hill ED, Kessler RC, McLaughlin KA, Petukhova M, et al. Cumulative traumas and risk thresholds: 12-month PTSD in the World Mental Health (WMH) surveys: cumulative trauma and PTSD. Depress Anxiety. 2014;31:130–42. doi: 10.1002/da.22169. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 52.Li J, Chen X, Zhao C, Xu Y. Relationship between adaptability and depressive symptoms among adolescent students [in Chinese] Chin JPublic Health. 2017;33:806–9. [Google Scholar]
- 53.Choi IJ, Lee GB, Lee HN. Korean Youth Indicator Survey v. International comparative survey of youth health status (Korea, United States of America, Japan, and China). National Youth Policy Institute: Seoul, Korea;; 2010.
- 54.Huang Y, Wang Y, Wang H, Liu Z, Yu X, Yan J, et al. Prevalence of mental disorders in China: a cross-sectional epidemiological study. Lancet Psychiatry. 2019;6:211–24. doi: 10.1016/S2215-0366(18)30511-X. [DOI] [PubMed] [Google Scholar]
- 55.Anyan F, Hjemdal O. Adolescent stress and symptoms of anxiety and depression: Resilience explains and differentiates the relationships. J Affect Disord. 2016;203:213–20. doi: 10.1016/j.jad.2016.05.031. [DOI] [PubMed] [Google Scholar]
- 56.Henry JD, Crawford JR. The short-form version of the Depression anxiety stress scales (DASS‐21): construct validity and normative data in a large non‐clinical sample. Br J Clin Psychol. 2005;44:227–39. doi: 10.1348/014466505X29657. [DOI] [PubMed] [Google Scholar]
- 57.Apter A, Bleich A, Plutchik R, Mendelsohn S, Tyano S. Suicidal behavior, depression, and conduct disorder in hospitalized adolescents. J Am Acad Child Adolesc Psychiatry. 1988;27:696–9. doi: 10.1097/00004583-198811000-00005. [DOI] [PubMed] [Google Scholar]
- 58.Frison E, Eggermont S. Exploring the relationships between different types of Facebook use, perceived online social support, and adolescents’ depressed mood. Social Sci Comput Rev. 2016;34:153–71. doi: 10.1177/0894439314567449. [DOI] [Google Scholar]
- 59.Geng Y, Gu J, Zhu X, Yang M, Shi D, Shang J, et al. Negative emotions and quality of life among adolescents: a moderated mediation model. Int J Clin Health Psychol. 2020;20:118–25. doi: 10.1016/j.ijchp.2020.02.001. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 60.Ingram J, Maciejewski G, Hand CJ. Changes in diet, sleep, and physical activity are associated with differences in negative mood during COVID-19 lockdown. Front Psychol. 2020;11:588604. doi: 10.3389/fpsyg.2020.588604. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 61.Galatzer-Levy IR, Brown AD, Henn-Haase C, Metzler TJ, Neylan TC, Marmar CR. Positive and negative emotion prospectively predict trajectories of resilience and distress among high-exposure police officers. Emotion. 2013;13:545–53. doi: 10.1037/a0031314. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 62.Yu Y, Peng L, Liu B, Liu Y, Li M, Chen L, et al. The effects of anxiety and depression on stress-related growth among Chinese army recruits: Resilience and coping as mediators. J Health Psychol. 2016;21:1884–95. doi: 10.1177/1359105314567769. [DOI] [PubMed] [Google Scholar]
- 63.Hjemdal O, Vogel PA, Solem S, Hagen K, Stiles TC. The relationship between resilience and levels of anxiety, depression, and obsessive-compulsive symptoms in adolescents. Clin Psychol Psychother. 2011;18:314–21. doi: 10.1002/cpp.719. [DOI] [PubMed] [Google Scholar]
- 64.Morote R, Hjemdal O, Martinez Uribe P, Corveleyn J. Psychometric properties of the resilience scale for adults (RSA) and its relationship with life-stress, anxiety and depression in a hispanic latin-american community sample. PLoS ONE. 2017;12:e0187954. doi: 10.1371/journal.pone.0187954. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 65.Toland J, Carrigan D. Educational psychology and resilience: New concept, new opportunities. School Psychol Int. 2011;32:95–106. doi: 10.1177/0143034310397284. [DOI] [Google Scholar]
- 66.Masten AS, Tellegen A. Resilience in developmental psychopathology: contributions of the project competence longitudinal study. Dev Psychopathol. 2012;24:345–61. doi: 10.1017/S095457941200003X. [DOI] [PubMed] [Google Scholar]
- 67.Taku K, Calhoun LG, Cann A, Tedeschi RG. The role of rumination in the coexistence of distress and posttraumatic growth among Bereaved Japanese University students. Death Stud. 2008;32:428–44. doi: 10.1080/07481180801974745. [DOI] [PubMed] [Google Scholar]
- 68.Cann A, Lawrence G, Calhoun RG, Tedeschi KN, Triplett T, Vishnevsky, Cassie M, Anxiety Stress Coping. 2011;24:137–56. doi: 10.1080/10615806.2010.529901. [DOI] [PubMed] [Google Scholar]
- 69.Prati G, Pietrantoni L. Optimism, social support, and coping strategies as factors contributing to posttraumatic growth: a Meta-analysis. J Loss Trauma. 2009;14:364–88. doi: 10.1080/15325020902724271. [DOI] [Google Scholar]
- 70.Hou WK, Ng SM. Emotion-focused positive rumination and relationship satisfaction as the underlying mechanisms between resilience and psychiatric symptoms. Pers Indiv Differ. 2014;71:159–64. doi: 10.1016/j.paid.2014.07.032. [DOI] [Google Scholar]
- 71.Blackburn L, Owens GP. Rumination, resilience, and posttraumatic stress disorder symptom severity among veterans of Iraq and Afghanistan. J Aggress Maltreatment Trauma. 2016;25:197–209. doi: 10.1080/10926771.2015.1107174. [DOI] [Google Scholar]
- 72.Vandevala T, Pavey L, Chelidoni O, Chang N-F, Creagh-Brown B, Cox A. Psychological rumination and recovery from work in intensive care professionals: associations with stress, burnout, depression and health. j Intensive care. 2017;5:16. doi: 10.1186/s40560-017-0209-0. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 73.Selby EA, Kranzler A, Panza E, Fehling KB. Bidirectional-compounding effects of rumination and negative emotion in predicting impulsive behavior: implications for emotional cascades. J Pers. 2016;84:139–53. doi: 10.1111/jopy.12147. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 74.Moberly NJ, Watkins ER. Ruminative self-focus and negative affect: an experience sampling study. J Abnorm Psychol. 2008;117:314–23. doi: 10.1037/0021-843X.117.2.314. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 75.Harrington JA, Blankenship V. Ruminative thoughts and their relation to depression and anxiety1. J Appl Social Pyschol. 2002;32:465–85. doi: 10.1111/j.1559-1816.2002.tb00225.x. [DOI] [Google Scholar]
- 76.Lindstrom CM, Cann A, Calhoun LG, Tedeschi RG. The relationship of core belief challenge, rumination, disclosure, and sociocultural elements to posttraumatic growth. Psychol Trauma: Theory Res Pract Policy. 2013;5:50–5. doi: 10.1037/a0022030. [DOI] [Google Scholar]
- 77.Wu X, Zhou X, Wu Y, An Y. The role of rumination in posttraumatic stress disorder and posttraumatic growth among adolescents after the Wenchuan earthquake. Front Psychol. 2015;6. [DOI] [PMC free article] [PubMed]
- 78.Zhang Y, Xu W, Yuan G, An Y. The relationship between posttraumatic cognitive change, posttraumatic stress disorder, and posttraumatic growth among Chinese adolescents after the Yancheng tornado: the mediating effect of rumination. Front Psychol. 2018;9:474. doi: 10.3389/fpsyg.2018.00474. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 79.Brislin RW. Back-translation for cross-cultural research. J Cross-Cult Psychol. 1970;1:185–216. doi: 10.1177/135910457000100301. [DOI] [Google Scholar]
- 80.Hu Y, Gan Y. Establishment and validity verification of adolescent mental toughness scale [in Chinese] J Psychol. 2008;40:902–12. [Google Scholar]
- 81.Geng Y, Xu Q, Liu H, Xu X. Reliability and validity analysis of the Chinese version of the post-traumatic growth scale in multiple trauma survivors [in Chinese] Chin J Nurs. 2011;46:1003–5. [Google Scholar]
- 82.Gong X, Xie X, Xu R, Luo Y. Psychometric properties of the Chinese versions of DASS-21 in Chinese college students [in Chinese] Chin J Clin Psychol. 2010;18:04. [Google Scholar]
- 83.Zhou X, Wu X, An Y, Chen J. The roles of rumination and social support in the associations between core belief challenge and post-traumatic growth among adolescent survivors after the Wenchuan earthquake [in Chinese] Acta Physiol Sinica. 2014;46:10. [Google Scholar]
- 84.Connor KM, Davidson JRT. Development of a new resilience scale: the Connor-Davidson Resilience Scale (CD-RISC) Depress Anxiety. 2003;18:76–82. doi: 10.1002/da.10113. [DOI] [PubMed] [Google Scholar]
- 85.Lovibond PF, Lovibond SH. The structure of negative emotional states: comparison of the Depression anxiety stress scales (DASS) with the Beck Depression and anxiety inventories. Behav Res Ther. 1995;33:335–43. doi: 10.1016/0005-7967(94)00075-U. [DOI] [PubMed] [Google Scholar]
- 86.Podsakoff PM, MacKenzie SB, Lee J-Y, Podsakoff NP. Common method biases in behavioral research: a critical review of the literature and recommended remedies. J Appl Psychol. 2003;88:879–903. doi: 10.1037/0021-9010.88.5.879. [DOI] [PubMed] [Google Scholar]
- 87.Hayes AF. Introduction to mediation, moderation, and conditional process analysis: a regression-based approach. New York: The Guilford; 2013. [Google Scholar]
- 88.Cero I, Sifers SK. Parenting behavior and the interpersonal-psychological theory of suicide: a mediated moderation analysis with adolescents. J Affect Disord. 2013;150:987–92. doi: 10.1016/j.jad.2013.05.025. [DOI] [PubMed] [Google Scholar]
- 89.Zhou H, Long L. Statistical remedies for common method biases [in Chinese] Adv Psychol Sci. 2004;12:942–50. [Google Scholar]
- 90.Li YZ. The impact of parental rearing style on learning engagement among senior high school students: a serial mediation effect model [in Chinese] Psychol Dev Educ. 2018;34:576–85. [Google Scholar]
- 91.Shultz JM, Baingana F, Neria Y. The 2014 Ebola outbreak and mental health: current status and recommended response. JAMA. 2015;313:567. doi: 10.1001/jama.2014.17934. [DOI] [PubMed] [Google Scholar]
- 92.Zhang Z, Shi Z, Wang L, Liu M. One year later: Mental health problems among survivors in hard-hit areas of the Wenchuan earthquake. Public Health. 2011;125:293–300. doi: 10.1016/j.puhe.2010.12.008. [DOI] [PubMed] [Google Scholar]
- 93.Mak IWC, Chu CM, Pan PC, Yiu MGC, Chan VL. Long-term psychiatric morbidities among SARS survivors. Gen Hosp Psychiatry. 2009;31:318–26. doi: 10.1016/j.genhosppsych.2009.03.001. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 94.Sareen J, Erickson J, Medved MI, Asmundson GJG, Enns MW, Stein M, et al. Risk factors for post-injury mental health problems: Review: post-injury mental health problems. Depress Anxiety. 2013;30:321–7. doi: 10.1002/da.22077. [DOI] [PubMed] [Google Scholar]
- 95.Fiorillo A, Gorwood P. The consequences of the COVID-19 pandemic on mental health and implications for clinical practice. Eur Psychiatr. 2020;63:e32. doi: 10.1192/j.eurpsy.2020.35. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 96.Affleck G, Tennen H. Construing benefits from adversity: adaptotional significance and disposltional underpinnings. J Personality. 1996;64:899–922. doi: 10.1111/j.1467-6494.1996.tb00948.x. [DOI] [PubMed] [Google Scholar]
- 97.Yun MR, Lim EJ, Yu B, Choi S. Effects of academic motivation on clinical practice-related post-traumatic growth among nursing students in South Korea: Mediating Effect of Resilience. IJERPH. 2020;17:4901. doi: 10.3390/ijerph17134901. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 98.Michalczyk J, Dmochowska J, Aftyka A, Milanowska J. Post-traumatic growth in women with breast Cancer: intensity and predictors. IJERPH. 2022;19:6509. doi: 10.3390/ijerph19116509. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 99.Poudel-Tandukar K, Chandler GE, Jacelon CS, Gautam B, Bertone-Johnson ER, Hollon SD. Resilience and anxiety or depression among resettled Bhutanese adults in the United States. Int J Soc Psychiatry. 2019;65:496–506. doi: 10.1177/0020764019862312. [DOI] [PubMed] [Google Scholar]
- 100.Kukihara H, Yamawaki N, Uchiyama K, Arai S, Horikawa E. Trauma, depression, and resilience of earthquake/tsunami/nuclear disaster survivors of Hirono, Fukushima, Japan. Psychiatry Clin Neurosci. 2014;68:524–33. doi: 10.1111/pcn.12159. [DOI] [PubMed] [Google Scholar]
- 101.Zeidner M, Kampler S. Memory traces of childhood exposure to terror attack and resilience and post-traumatic growth in adulthood. Pers Indiv Differ. 2020;155:109719. doi: 10.1016/j.paid.2019.109719. [DOI] [Google Scholar]
- 102.Philippe FL, Lecours S, Beaulieu-Pelletier G. Resilience and positive emotions: examining the role of emotional memories. J Pers. 2009;77:139–75. doi: 10.1111/j.1467-6494.2008.00541.x. [DOI] [PubMed] [Google Scholar]
- 103.Hooberman J, Rosenfeld B, Rasmussen A, Keller A. Resilience in trauma-exposed refugees: the moderating effect of coping style on resilience variables. Am J Orthopsychiatry. 2010;80:557–63. doi: 10.1111/j.1939-0025.2010.01060.x. [DOI] [PubMed] [Google Scholar]
- 104.Davis CG, Wohl MJA, Verberg N. Profiles of posttraumatic growth following an unjust loss. Death Stud. 2007;31:693–712. doi: 10.1080/07481180701490578. [DOI] [PubMed] [Google Scholar]
- 105.Cai SQ. A study on the relationship between college students’ negative emotions, psychological resilience and life satisfaction [in Chinese]. Capital Normal University; 2013.
- 106.Lau WKW. The role of resilience in depression and anxiety symptoms: a three-wave cross‐lagged study. Stress Health. 2022;38:804–12. doi: 10.1002/smi.3136. [DOI] [PubMed] [Google Scholar]
- 107.Chen N, Xi J, Fan X. Correlations among psychological resilience, Cognitive Fusion, and depressed emotions in patients with Depression. Behav Sci. 2023;13:100. doi: 10.3390/bs13020100. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 108.Zięba M, Wiecheć K, Biegańska-Banaś J, Mieleszczenko-Kowszewicz W. Coexistence of post-traumatic growth and post-traumatic depreciation in the Aftermath of Trauma: qualitative and quantitative narrative analysis. Front Psychol. 2019;10:687. doi: 10.3389/fpsyg.2019.00687. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 109.Mi Young K, Yujeong K. Factors affecting Posttraumatic Growth among College Students. TONURSJ. 2018;12:238–47. doi: 10.2174/1874434601812010238. [DOI] [Google Scholar]
- 110.Zeng W, Huang D, Li Q, Xu Y, Xu Z, Wu C, et al. Negative emotions and creativity among Chinese college students during the COVID-19 pandemic: the mediating role of psychological resilience and the moderating role of posttraumatic growth. Arch Public Health. 2022;80:194. doi: 10.1186/s13690-022-00954-8. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 111.Farnsworth JK, Sewell KW. Fear of emotion as a moderator between PTSD and firefighter social interactions. J Trauma Stress. 2011;24:444–50. doi: 10.1002/jts.20657. [DOI] [PubMed] [Google Scholar]
- 112.Henson C, Truchot D, Canevello A. What promotes post traumatic growth? A systematic review. Eur J Trauma Dissociation. 2021;5:100195. doi: 10.1016/j.ejtd.2020.100195. [DOI] [Google Scholar]
- 113.Manne S. Posttraumatic growth after breast Cancer: patient, Partner, and couple perspectives. Psychosom Med. 2004;66:442–54. doi: 10.1097/01.psy.0000127689.38525.7d. [DOI] [PubMed] [Google Scholar]
- 114.Norlander T, Schedvin HV, Archer T. Thriving as a function of affective personality: relation to personality factors, coping strategies and stress. Anxiety Stress Coping. 2005;18:105–16. doi: 10.1080/10615800500093777. [DOI] [Google Scholar]
- 115.Arslan G. Mediating role of the self–esteem and resilience in the association between social exclusion and life satisfaction among adolescents. Pers Indiv Differ. 2019;151:109514. doi: 10.1016/j.paid.2019.109514. [DOI] [Google Scholar]
- 116.Luthar SS, Cicchetti D, Becker B. The construct of resilience: a critical evaluation and guidelines for future work. Child Dev. 2000;71:543–62. doi: 10.1111/1467-8624.00164. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 117.Paredes MR, Apaolaza V, Fernandez-Robin C, Hartmann P, Yañez-Martinez D. The impact of the COVID-19 pandemic on subjective mental well-being: the interplay of perceived threat, future anxiety and resilience. Pers Indiv Differ. 2021;170:110455. doi: 10.1016/j.paid.2020.110455. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 118.Norris FH, Friedman MJ, Watson PJ, Byrne CM, Diaz E, Kaniasty K. 60,000 disaster victims speak: Part I. An empirical review of the empirical literature, 1981–2001. Psychiatry: Interpersonal and Biological Processes. 2002;65:207–39. [DOI] [PubMed]
- 119.Akinola M, Mendes WB. The dark side of creativity: biological vulnerability and negative emotions lead to greater artistic creativity. Pers Soc Psychol Bull. 2008;34:1677–86. doi: 10.1177/0146167208323933. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 120.Wyer RS. Ruminative thoughts. L Erlbaum Associate; 1996.
- 121.De Dreu CKW, Baas M, Nijstad BA. Hedonic tone and activation level in the mood-creativity link: toward a dual pathway to creativity model. J Personal Soc Psychol. 2008;94:739–56. doi: 10.1037/0022-3514.94.5.739. [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Data Availability Statement
The datasets used and/or analyzed during the current study are not publicly available. Permissions could be obtained/required from the corresponding author on a reasonable request.