

Abstract
Background
Multiple mhealth (mobile health) interventions and mobile applications have been developed to support diabetes self-management. However, most of the apps are developed without the need for assessment and evaluation by experts in the field. This study aimed to design and develop a mobile application (app) supporting diabetes self-management for people with Type 2 Diabetes Mellitus (T2D) using a systematic approach.
Methods
In this study mixed method design was used to develop the mobile application. The mhealth intervention was designed and developed in five steps: i) Extensive literature search, ii) Needs assessment of patients with T2D with the help of healthcare providers and patients (Interviews with 15 healthcare providers like clinicians, dietitians, and diabetes educators, and 2 focus group discussions with patients) iii) Ideation and content development of app based on outcomes of needs assessment; iv) content validation (by 10 healthcare providers) and v) App development on a hybrid platform. Evaluation of the app by users i.e., type 2 diabetes patients was done using the users' Mobile App rating scale (uMARS). The app was evaluated by 40 patients and rated on the uMARS questionnaire.
Results
A patient-centric mobile app was developed for the nutritional management of diabetes with three modules: The patient module, the Evaluation module, and the Healthcare provider module. The patient module was the app that was provided to the patients with features like diet, physical activity, blood glucose log, education, etc., in addition to, a symptom checker, Stress meter blog, and FAQ. The evaluation module was integrated with the app it works when a user enters any log, it evaluates the entry against the standard cutoffs and flash prompts on the screen. The Healthcare provider module interacts with the server to provide them with patient data, comments, and feedback.
Conclusions
The users found the app to be satisfactory. Incorporating additional features to enhance the user interface and streamline navigation could potentially enhance user engagement, thereby aiding in the management of T2D.
Keywords: Type 2 Diabetes, Mobile app, uMARS, mHealth, Needs assessment, User interface, App usability
Background
Diabetes has become a significant health concern, reaching critical levels. Presently, over half a billion people are grappling with diabetes on a global scale. Diabetes is one of the largest health emergencies of the twenty-first century with a worldwide prevalence of 422 million [1]. It is predicted by International Diabetes Federation (IDF) that this number will reach 642 million by 2040, i.e. one in every ten adults. The largest increase is taking place in regions where economies are moving from low- to middle-income levels. About 75% of people with diabetes live in low- and middle-income countries (LMIC) [2]. In India, an estimated 8.7% of the population between 20–70 years of age are diabetic [3].
Mobile health technologies can provide a very important opportunity for alleviating the massive healthcare challenges and economic burden associated with diabetes and its long-term complications. Nowadays, a large number of people access the mobile phone. The number of mobile phone users is increased to over 3 billion (and rapidly rising) in recent times [4]. The individual patient plays the central participatory role in their diabetes self-management and care process. Through their smart mobile phone apps, the reach of healthcare services could be increased massively. Although mobile health (mHealth) may not be a substitute for professional health care, it could play a very significant role in diabetes management. mHealth services are empowering individuals with information related to primary, secondary, and tertiary prevention so that they might be able to make knowledgeable decisions about their lifestyle and behaviors [5].
Mobile applications have been effectively used to provide support for self-management by promoting healthy lifestyle changes and fostering medication adherence [6–8]. Nevertheless, limited user engagement with these apps could prevent users from fully experiencing their benefits [9, 10] Involving users in the design process may lead to increased empowerment and engagement, thereby aiding mobile health (mHealth) apps in effectively supporting patients with T2D [8, 11]. In a recent study, it was highlighted that when developing an app for diabetes, attention should be given to three primary areas of focus: application design (including architecture), UI design, and the assessment of trust factors in the application. These trust factors encompass functionality, ease of use, usefulness, security, privacy, and cost [12].
Novel apps stressed on increasing the usability of the app to increase its effectiveness [8, 13]. Therefore developing a mobile app which can enhace user engagement is the need of the hour.
The aim of this study was to employ a systematic approach in creating a mobile application to support self-management for individuals with diabetes, and to assess the usability and efficacy of this intervention.
Method
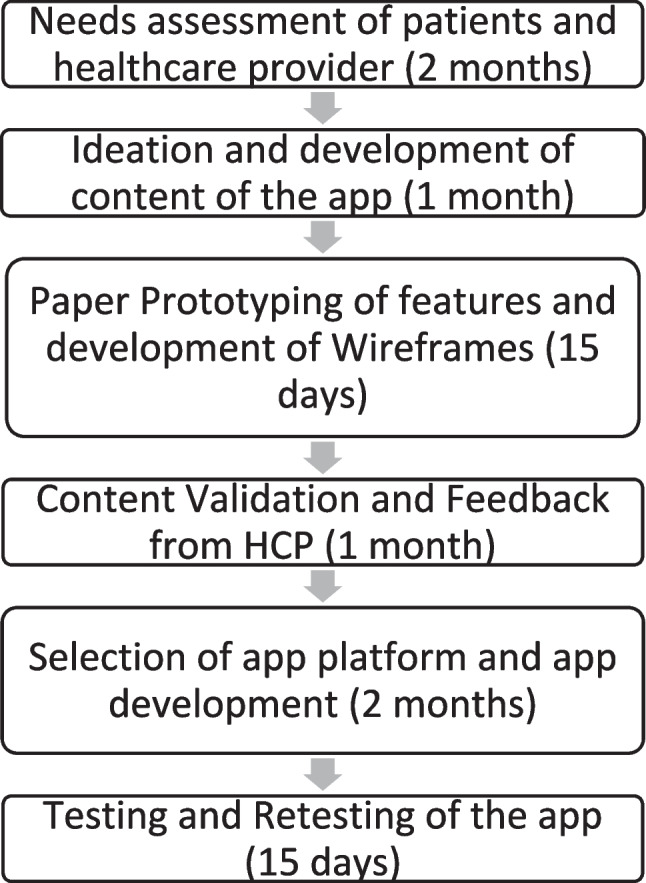
The study used the mixed method design. The app was developed and tested from July 2018 to June 2019. The design of the mhealth intervention was developed by a team of researchers that included experts in the fields of nutrition and clinical management of type 2 diabetes. The app was developed in multiple steps based on evidence-based clinical guidelines. The steps involved in app development are given in Fig. 1.
Needs assessment of patients and healthcare providers: Extensive literature search was conducted to gather existing data about types of apps, for the ideation of the app to generate secondary data. For primary data generation interviews with 15, healthcare providers were conducted. Based on the outcomes of the need assessment, suggestions provided by HCPs and patients and a literature review of the basic features of the app were outlined.The details of this step is published elsewhere [14].
Ideation of App features: The outcomes of the needs assessment of patients were assessed and related app features were identified. Once the basic features were identified, the content required for the app was listed and was collected from evidence-based information and national guidelines for Diabetes management.
Paper Prototyping of features and development of Wireframes: After the development of the basic content of the app paper prototype of the app was developed. Paper prototyping also called the “sketching exercise” is a quick and inexpensive method of generating concepts and solutions. In this step, all the app ideas were listed and sketched. All the screens were drawn and further forward and backward data requirements were listed. This helped in identifying the data source and standard guidelines required. Diabetes management guidelines are given by ICMR, IDF, and WHO were utilized to develop content relevant and covering all non-pharmacological aspects. Once the paper prototype was finalized wireframes of the features were developed to make screen-by-screen visuals of the app. An App wireframe, also called a page schematic, is a visual guide that represents the skeletal framework of an app. In short, wireframes are a two-dimensional representation of any screen interface.
-
Content Validation and Feedback of Healthcare Providers: The content of the app was validated with the help of 10 HCPs. Experts in the field of Diabetes management were invited to collect survey data using the Content Validity Survey Tool. Expert reviewers had relevant content knowledge and experience, disciplinary diversity was maintained to provide useful balance by engaging 3 medical practitioners in the field of diabetes management, 3 Diabetes educators, and 4 Dietitians. The features of the app were discussed with the reviewers with the help of a PowerPoint presentation in which every wireframe and background content used in the app was given.
A tool developed by Kassam-Adams et al. 2015 was used for content validation modifying it for Type 2 Diabetes intervention [15]. Content Validity Survey Tool is a tool that uses a 5-point Likert-type scale (1-5), covering the following three parameters: (1) Relevance (the extent to which this specific intervention activity is pertinent to the intended intervention target) with 1 defined as “Irrelevant/Extraneous to this target” and 4 defined as “Central/Key/Essential to this target”; (2) Effectiveness (the likelihood that this specific activity will successfully modify the intended intervention target), with 1 defined as “Not likely to be effective” and 5 defined as “Very likely to be effective”; and (3) Appropriateness for the intended audience, which considers the extent to which the language, content, and nature of activities were clear, easy to understand, and appropriate for Type 2 Diabetes Patients, with 1 defined as “Inappropriate” and 5 defined as “Appropriate”.
The survey form included Powerpoint slides from the App design to help expert reviewers to evaluate the features and screens they were rating. The scale used in this study was an open-access scale that permitted unrestricted use, till the original work was cited properly.
Identification and Selection of App Platform: Identification and selection of the app platform was a difficult process due to the presence of multiple operating systems for mobile devices, though some of these have marginal market share. To avoid the high cost associated with the Apple Operating System and limitations in operations of the Android Operating System a novel cross-platform Hybrid Web App platform was used. From a user’s point of view, there is little difference between a native app and a hybrid app. As long as the device has a web browser, a hybrid app can run just like a native app [16]. After the selection of the front-end platform of the app as a hybrid app, the backend of the app was developed using PHP as the programming language, and word a press content management system was used to host the app. Codes were developed and the programs were written for every feature. In the end, features were integrated and published in word press.
-
Testing and Retesting of the app: After the initial development phase, the app underwent a rigorous and multifaceted testing process to ensure its overall quality and reliability. Functionality testing was conducted to confirm that all features and functions worked as intended. Usability testing focused on evaluating the app's user-friendliness, examining factors such as ease of navigation and the intuitiveness of the user interface.
Interface testing delved into the details of design, including backward and forward hyperlinking, the landing page's effectiveness, and the validation of HTML and CSS components. Compatibility testing ensured that the app functioned seamlessly across various devices, operating systems, and web browsers, providing a consistent user experience. Performance testing assessed the app's responsiveness, speed, and stability, particularly in high-demand scenarios.
Security testing aimed to identify and rectify potential vulnerabilities, safeguarding user data and protecting against unauthorized access. Furthermore, the app was scrutinized for browser compatibility, its ability to handle web load and stress, and its capacity to provide informative and user-friendly error messages for invalid entries. This comprehensive testing process aimed to deliver a reliable and secure app with a user-friendly interface, ensuring a smooth and consistent experience for all users across different platforms and scenarios.
Development of Educational and reminder messages: In addition to the mobile app educational and reminder messages were developed to send to the patients. The content of the messages was developed by utilizing the results of interviews with healthcare providers and a literature search.
Fig. 1.
Steps in development of app design
Evaluation of the app using the Users Mobile App Rating Scale (uMARS)
Users Mobile App Rating Scale (uMARS) was developed by Stoyanoy et al. (2016) to assess Health mobile apps. uMARS is a 20 items scale that is divided into 5 subscales that assess the app quality. The subscales are as follows a) engagement, b) functionality, c) aesthetics, d) information quality, and e) subjective quality.
In the user’s evaluation of the app, 40 patients newly diagnosed with T2D (< 1 year of diagnosis) having an android smartphone with the ability to handle multimedia mobile apps were included. They were provided with the app for 3 months. At the end of three months, the app was rated by the study subjects on the uMARS questionnaire.
Results
In the study Diabetes Sutra app was developed by combining the results of secondary data (gathered by a thorough literature review utilizing online databases, extracting information from government health websites, reviewing clinical trials, and exploring research reports), need assessment, and suggestions given by Type 2 Diabetes Patients and Healthcare providers (Table 1).
Table 1.
Results of need assessment and corresponding app feature
| Need identified during need assessment and catered in app | Corresponding feature of app |
|---|---|
| 1. About symptoms of hypoglycemia and hyperglycemia | Symptom checker and Log book |
| 2. What to do with blood glucose values obtained after testing? | Log book |
| 3. Meaning of HbA1c | Log book |
| 4. Regular monitoring of blood glucose | Log book and messages |
| 5. Basic information about diabetes | Frequently Asked Question |
| 6. Information about dietary modifications | Plate method is introduced and messages |
| 7. Nutritional information of foods should be given | Food nutrition section |
| 8. Patient-healthcare provider communications should be increased | Queries and feedback |
| 9. Steps required for prevention of comorbidities | Log book and Symptom checker |
| 10. Information about the recommended Duration and type of Physical activity | Physical activity and messages |
| 11. Patient education |
Education modules given for dietary management (plate method), Physical Activity, self-monitoring of blood glucose, stress management Blog |
Content validation of the app
The content of the app was developed with the help of 10 experts in the field of diabetes management. The content of each feature was validated for relevance, effectiveness, and appropriateness. The result of content validation is given in Table 2.
Table 2.
Score obtained in content validation of app
| App feature | Maximum score | Relevance Mean ± SD | Effectiveness Mean ± SD |
Appropriateness Mean ± SD |
|---|---|---|---|---|
| Log Book | 5 | 4.8 ± 0.3 | 4.7 ± 0.4 | 4.8 ± 0.3 |
| Diet | 5 | 4.6 ± 0.5 | 4.5 ± 0.5 | 4.7 ± 0.4 |
| Physical activity | 5 | 4.7 ± 0.4 | 4.7 ± 0.4 | 4.7 ± 0.6 |
| Frequently asked question (FAQ) | 5 | 4.8 ± 0.4 | 4.6 ± 0.3 | 4.7 ± 0.7 |
| Blog | 5 | 4.7 ± 0.4 | 4.6 ± 0.5 | 4.6 ± 0.5 |
| Queries and feedback | 5 | 4.8 ± 0.3 | 4.7 ± 0.4 | 4.8 ± 0.3 |
| Mood meter | 5 | 4.5 ± 1 | 4.6 ± 0.7 | 4.4 ± 1 |
| Symptom checker | 5 | 5 ± 0 | 4.8 ± 0.3 | 4.8 ± 0.3 |
In all the features, experts gave a score to the content of the app of more than 4 out of a maximum score of 5. All the features of the app were approved. Suggestions provided by experts were incorporated into the app.
Description of intervention features
In the app, patients were given the required information. They were motivated to adhere to the app with the help of motivational messages sent to them through the mobile app in the form of notifications and separate messages through messaging services. Behavioral skills were monitored through a mobile app with the help of features purposefully developed to increase adherence.
Diabetes Sutra app consists of three modules:
- Patient module: This is the application that is available to the patient. It provides the following functionalities:
- Patient Dashboard: The app comprises 8 main features (Fig. 2):
- Log Book
- Diet
- Physical Activity
- FAQ
- Blog
- Queries and Feedback
- Mood Meter
- Symptom Checker
-
Log Book: The first sub-module of the patient interface was the Logbook. Diabetes patients need to monitor their biochemical values. The app has the facility to enter and record blood glucose values, HbA1c, lipid values, and blood pressure. In a recent study, it was found that self-monitoring of blood glucose as a standalone intervention does not have any significant impact on blood glucose control [17]. However, another study inferred that reason why patients did not benefit from Self-Monitoring of Blood Glucose was due to the lack of associated education needed to derive meaningful and actionable information from the blood glucose readings [18]. Hence, mere monitoring and recording blood glucose values regularly do not create any impact and it was essential to develop a feature that can explain to the user the significance of any value obtained and the action that is required when obtaining that value. As a result of synthesis from a literature search and suggestions from healthcare providers, the logbook feature was developed such that the blood glucose readings captured were paired with related lifestyle information to provide feedback and help in individualized education.Patient-recorded data was made available at the end of the respective screen in the form of a table. Blood glucose cut-offs given by ICMR (2018) were utilized to develop the messages. For eg. in fasting blood glucose three conditions were considered:
- Condition 1: Normal values- 80–110 mg/dl: Under this condition, the patient was congratulated for achieving normal blood glucose values and encouraged to follow a healthy lifestyle. A link is provided in the message which directs the user toward the screen explaining the meaning of a healthy lifestyle. Patients were informed that they can control their blood glucose levels by Using a meal plan, being physically more active, taking their medicines on time, and keeping track of their blood glucose.
- Condition II: When the user’s blood glucose value was above 110 mg/dl it was considered Hyperglycemia and 2 types of messages were given for two ranges.
-
The range I = (111- 125 mg/dl): In this message flashes in the yellow box which informs the patient that their blood glucose is higher than the target range. Then they were requested to log their blood glucose, diet, and physical activity entries for the coming 7 days. A link was provided in the message to inform them what may be the cause of the increase in blood glucose value. The screen appears as given in the Fig. 3.On further clicks, screens appear giving patients information about the Plate method for diet management with drop-down menus of the list of food items recommended on the plate. Patients were also provided information about recommended physical activities along with their recommended duration and tips to increase physical activity in their daily routine in the office, at home, and in other places.
- Range II = (> 125 mg/dl)- Blood glucose values in this range were considered to be in the dangerous range and users were informed that their blood glucose is much higher than the target range and they were suggested to consult their Healthcare team.
- Condition 3 (Hypoglycemia): When Blood Glucose falls below 80 mg/dl, three ranges were taken:
- Glucose Alert Value I (between 80–70 mg/dl): in this condition a yellow box appears with the message “Your Blood glucose is low, it’s time to have a meal”.
- Glucose Alert Value II (69–54 mg/dl): This range was considered clinically Hypoglycemia. In this case, the user was cautioned about the condition informing that their blood glucose is lower than the target value causing hypoglycemia. They were alerted that action is required as given in Fig. 4(a).
-
Severe Hypoglycemia (less than 54 mg/dl): In this condition, the patient was asked to follow 15 g carbohydrate cycle as mentioned above and given in Fig. 4(b) and was suggested to contact their healthcare team immediately.Similar messages flashed on entering Post Prandial Blood Glucose values.A similar log book was created for recording HbA1c, Blood Pressure, and Lipid profile. Automated messages specifying the meaning of the parameter and recommendations were flashed. Some other tests were suggested for a regular checkup: Liver Function test, Kidney Function test, and Eye Test were recommended. Similar to the blood glucose log, the HbA1c log, lipid log, and blood pressure log give information about the significance of the value obtained.In the Blood pressure log, pictorial information on the appropriate time and posture to get the correct blood pressure value is also provided.
- Diet: The diet sub-module of the app contains three main features: Diet log, Nutrition information, and Plate method (Fig. 5). The description of each feature is as follows:
-
Diet log: This feature helps the user to log food by entering every food consumed in a day after selecting it from the food database.A database of more than 1000 foods was developed using a standard food database [19] and the nutritional value of common restaurant foods was given on their websites. Additionally, the nutritional value of common snacks and packed food like biscuits, etc. were also included.Subjects could keep track of the nutritional value of their daily food intake, by entering the food consumed from the list of items provided in the food database. For this, they need to select the food from the drop-down menu (with the facility of smart search), select meal type (breakfast, lunch, etc.), meal time, and serving size. It gives the calculated nutritional value of each meal and at the end of the day, cumulative nutritional values of foods consumed throughout the day can be obtained.A table appears at the end of the screen which shows the nutrients taken in every meal and the cumulative value of all nutrients consumed in a day. With a date change, a new log appears and the previous log appears at the bottom of the screen in the form of a table. The nutrients whose value appears are total calories, carbohydrates, proteins, fat, iron, calcium, sodium, vitamin B2, and vitamin C. This functionality can be accessed in the Diet section of the main interface.
- Nutrition Information: In this section, the patient can check the nutritional value of the individual item by selecting a food item from the list of foods given in the food database. The patient then selects the food item and serving size, and the nutritional information of that food appears in the form of the table at the bottom of the screen.
-
Plate method: As a result of the need assessment and literature review, it was observed that patients find it difficult to follow a written meal plan and often eat any food of their choice without considering its nutritional value. The reason for this behavior, as mentioned by patients and HCPs, was the lack of choices provided to them while giving a meal plan. To cater to this problem plate method was introduced in the app to educate patients about healthy foods and provide them with multiple options for every meal.In addition to the plate method, an exchange list was also given in the app to educate patients about healthy food choices. Tips for making healthy food choices and the significance of meal timings and portion sizes were also explained to patients in the app.
- Physical Activity Log and prompts: Under this section patients can record their daily physical activity duration. It gives the option to enter the duration of both aerobic exercises like walking, jogging, etc., and resistance exercises like stretching, weight lifting, yoga, etc. Automated messages in response to entered value of the duration of exercise flash on the screen. Physical activity guidelines for Indians as recommended by Misra et al. 2012 were utilized to develop this feature [20]. The guidelines recommend 60 min of daily physical activity including 15 min of resistance exercises. Physical Activity Guidelines: In this feature, physical activity guidelines were given. From the result of the need assessment, it was inferred that patients find it difficult to take out separate time from their daily routine for physical activity. To facilitate patients following physical activity guidelines, tips to increase physical activity in their daily routine were provided. Tips were provided to them to increase physical activity at work, at home, and in other places.
- FAQ: This feature was developed to answer frequently asked questions by patients. Questions included were: what is diabetes, the importance of diet, regular check-ups, complications of diabetes, the role of family and friends, etc. Answers to these questions were developed utilizing evidence-based scientific literature and national and international guidelines.
- Blog: The blog was developed to post informational articles on diabetes management at regular intervals. Articles on the topic of the importance of dietary fiber in the diet, food exchange list, glycemic index of foods, diabetes screening, stress management, etc. were given.
- Queries and Feedback: This section was created to get any queries related to app use or lifestyle management. Patients were also encouraged to give feedback to make the app better.
- Mood meter: According to the suggestions of healthcare providers, there is a requirement for better mental stress management in patients to manage their blood glucose values better. Stress is considered a risk factor for diabetes and its management is desirable in proper diabetes management [21]. A mood meter scale was used to measure the stress level in the patient. The scale was adapted from the Ottawa mood Scale (2011) developed by Dr. Michael Cheng [22]. In this scale, patients were asked to rate their stress on a scale of 1–10 where 1 is extreme calmness and 10 is extreme stress. Whenever the patient marks a stress level of more than 5, they are redirected toward tips for the management of stress, as recommended by American Diabetes Association. The stress score was recorded in the app creating a log for stress.
- Symptom checker: To educate patients and make them aware of the co-morbidities associated with Diabetes a section of symptom checker was created. In this section through pictorial depiction, symptoms of Hyperglycemia, Hypoglycemia, Hypertension, Diabetic Foot, Neuropathy, and Retinopathy were shown. Based on the result of the quantitative survey it was found that people have low knowledge about the symptoms of Hyperglycemia and Hypoglycemia and their awareness of Diabetes comorbidities was found to be less. To cater to this low level of awareness, physical symptoms of the aforementioned co-morbidities were included in the app.
- Automated messages and Diabetes education Modules: Automated messages were sent to patients as notifications which appeared on the screen as soon as the patient enters his/her data. These messages contain precise information about the condition and links which further take them to comprehensive Diabetes education modules. The messages provide any information only when any value is entered thus making it more interactive and user-friendly. Diabetes education modules could be accessed directly from the onscreen icons along with the links given in automated messages which appear as and when required on entering a particular value of blood glucose, physical activity, diet, and stress. These modules contain comprehensive information about lifestyle modification recommendations provided in the guidelines.
- Patient Data: The user can monitor the record of all the data entered in the form of tables at the end of respective screens. This data could be shared with their contacts through e-mail. This data is automatically available to the healthcare team, which can monitor the data and can contact the patient as required through the patient’s registered contact information.
- Application setting: User can change user's password, update their weight, habits, physical activity routine, alternate phone number, etc.
- Messages: During the period of intervention, messages were sent to patients. Fifty-five messages were sent which included reminder messages, educational messages, and motivational messages. Reminder messages were sent for medication, physical activity, and dietary adherence. Educational messages related to diet, physical activity, and self-monitoring of blood glucose were sent regularly. Motivational messages were sent to patients to motivate them to adhere to the recommended regime. These messages were sent to facilitate patient adherence to recommended lifestyle.
-
Evaluation module: Data entered by the patient is automatically evaluated following the Indian Council of Medical Research (ICMR) guideline’s targeted values—optimally, blood glucose below 110 mg/dl fasting, below 140 mg/dl postprandial; blood pressure below 130/80 mmHg; BMI, HbA1c and physical activity duration of 1 h daily. In response, automated messages appear on the screen with different messages recommending changes that should be made to achieve optimal control.
Healthcare Provider Module: This module was used by healthcare providers. It interacts with the server module to provide them with patient data which includes glucose measurement history, physical activity, food intake, stress scores, and patient comments and feedback. The healthcare team utilized this facility to contact the patient as and when required as the data was transmitted in real-time. With one click Healthcare team can access the data of all the patients individually.
Fig. 2.

Main menu of the app
Fig. 3.

Screens for hyperglycemia with follow-up screen
Fig. 4.

Screens at the event of hypoglycemia and treatment of hypoglycemia
Fig. 5.

First screen of the diet feature
Evaluation of DiabetesSutra app by T2D patients using uMARS scale
The app was tested for using uMARS with 40 subjects. the socio-demographic and vital parameters of the study participants are given in the Table 3
Table 3.
Sociodemographic information of study participants
| Characteristics | Intervention group Mean ± SD/Frequency (%) n = 40 |
|
|---|---|---|
| Gender | Female | 17(43%) |
| Male | 23(57%) | |
| Age (years) | 45 ± 9.7 | |
| 21–30 | 1(2.5%) | |
| 31–40 | 11(27.5%) | |
| 41–50 | 16 (40%) | |
| 51–60 | 12 (30%) | |
| Education level | Up to Intermediate | 2 (5%) |
| Graduate or Post-graduate | 26 (65%) | |
| Profession or Honors | 12 (30%) | |
| Occupation | Professional | 8 (20%) |
| Semi-Professional | 11 (27.5%) | |
| Clerical/Shop owner | 11 (27.5%) | |
| Homemaker | 10 (25%) | |
| Weight (kg) | Female | 63.3 ± 7.1 |
| Male | 72 ± 8.7 | |
| Height (cm) | Female | 156.5 ± 7.1 |
| Male | 166.8 ± 7.2 | |
| BMI | 25.24 ± 2.1 | |
| HbA1c | 8.6 ± 1.6 | |
| Fasting blood Glucose (mg/dl) | 123.8 ± 26.8 | |
| Post prandial Blood glucose (mg/dl) | 238 ± 44 | |
The app scored approximately 3.6 out of 5 in both app quality mean score and app star rating. There was an increase in self-monitoring of blood glucose in the group and weekly monitoring of blood glucose almost doubled. The app performed well when it comes to Engagement, Functionality, and Information but obtained a slightly lower score in Aesthetics when compared to other parameters. Since the app was a prototype hence graphics and visuals were low in aesthetic value. The overall star rating obtained by the app was 3.60 which was in the Acceptable to Good range. The app got only a 2.91 ± 0.4 score in aesthetics mean score. This may be because the app was developed on a hybrid platform and the user experience was affected as the page-to-page navigation was less seamless. It is essential to develop the aesthetics of the app as it enhances user experience which increases the engagement time and app quality (Table 4).
Table 4.
App quality score (uMARS score)
| Parameters (App Quality score) | Maximum score | Obtained score (Mean ± SD) |
App quality |
|---|---|---|---|
| i Engagement mean score | 5 | 3.56 ± 0.2 | Acceptable-Good |
| ii Functionality mean Score | 5 | 3.76 ± 0.3 | Acceptable-Good |
| iii. Aesthetic Mean Score | 5 | 2.91 ± 0.4 | Poor-Acceptable |
| iv. Information Mean Score | 5 | 4.45 ± 0.2 | Acceptable-Good |
| v. App quality mean score | 5 | 3.42 ± 0.5 | Acceptable-Good |
| vi. App Subjective score | 5 | 3.64 ± 0.5 | Acceptable-Good |
| vii. App Star rating | 5 | 3.47 ± 0.5 | Acceptable-Good |
| Overall Mean Score | 5 | 3.60 ± 0.27 | Acceptable-Good |
Use of the app by the participants
The main outcome measure for the intervention group that was assessed was the use of the app by the participants and it was measured by counting total number of logs entered by the participants under various heads. The description of the log of patient’s is given in the following Table 5. There was on an average of approximately 42 entries per participation in the duration of first 3 months of the intervention. This indicates that on an average data was entered by patient about every alternate day. Most utilized feature of the app was log book for entry of blood glucose, followed by physical activity and diet log. Out of 40 participants of intervention group, 18 participants entered their data more than 50 times in the duration of 3 months of study period. Highest number of entries done by any participant was 73 and lowest number of entries done by any participant was 12 during the study period of 3 months (Table 5).
Table 5.
Use of app by the participants
| Use of the app by participants (n = 40) | Values entered by patients (n) in 3 months | (Mean ± SD)/Person |
|---|---|---|
| Total entered values | 1670 | 49.12 ± 14.66 |
| Blood glucose and other logs | 1407 | 41.4 ± 13 |
| Diet log | 38 | 1.1 ± 0.8 |
| Physical activity log | 225 | 6.62 ± 3 |
Weekly data entry done by participants
There was a variation in the number of entries by subjects in each week of intervention. Maximum number of entries was observed in the first week of intervention with a mean of 6.3 entries. From the second week onwards, there was a consistent fall in number of entries per week with lowest number of entries being recorded in the sixth week at an average of 2.9 entries. The number of entries per week again increased when the reminder and education message service was started in 6th week, thereby highlighting the importance of continuous engagement and two-way flow of communication in enhancing use of mobile app. For most of the weeks average number of entries per participant was between 3 to 4 per participant per week.
Discussion
Diabetes applications differ in the features they provide, including tracking blood glucose values, nutrition database and carbohydrate counting, physical activity tracking and weight tracking, sharing information with clinicians or family members, peer support, informational messages and reminders messages [23]. The use of these functions may help patients in adhering to diet, exercise, and medication. This adherence could lead to improvement in diabetes-related results. There is considerable inconsistency in how mobile apps are developed and utilized in health care. There are apps which provide only single functionality on the other hand there as some which provides a range of features. Some apps consist of features to be used only in online patient portal. In such portals patients and healthcare providers can exchange information or other health related messages, whereas others get connected to the patient’s electronic medical record and automatically transfer data [24] In previous few years development of new technology and apps brought significant increase in new apps and technology in healthcare sector also, though the effectiveness and usability of the Apps are not reliable. A recent study evaluated 65 freely available at play store and reported that out of 65 apps only nine could be useful for self-management of diabetes. There is a need for reliable mobile apps for self-management of diabetes with better quality and more features to influence a large number of long-term users and thus provide better self-management of the disease [25]. Arsand et al. (2015) in their study suggested that the development of health care tools for patient groups like those with diabetes or chronic diseases needs deep understanding of current challenges and barriers to self-care [26]. This approach gives the chance for exploring patient’s needs at a particular time and visualizing what may evolve with time. This can help in envisaging the use of the app as users’ demands change [27, 28]. Though there are thousands of mobile applications for Diabetes management are available in both Android and Apple play store scientifically proven and evidenced based apps are few.
A recent study reviewed 15 commercial apps for diabetes prevention on the google play store using MARS scale reported that all the apps had a mean MARS score above 3.75 except for one. On evaluating the individual aspects of the app quality mean score, we found the mean score for Engagement to be the lowest (3.6) for all the 15 apps, followed by Information (4.0) [29]. Which suggests that those mobile apps had an overall acceptable level of quality. The present app has overall score of 3.6 ± 0.27 which is similar to the rating obtained by the commercial appsIn the Information section the DiabetesSutra app obtained user rating of 4.45 ± 0.2 indicating towards user satisfaction towards information provided in the app.
In this app on an average 42 entries were done by patients in the duration of 3 months which indicates that one entry was done on alternate days and the blood glucose log book was the most used features of the app and diet log is the least used feature. This is similar to the finding of a study conducted to assess the utility of app features reported that blood glucose diary was the most utilized feature among features of mobile app and carbohydrate calculator was utilized by minimum number of users [30]. Similar results were also reported by a study in which a survey conducted in a hospital to assess the most favored features of apps among health app users and non-users of any health app it was found that the most favored feature by the health app users was glucose diary. Eighty seven percent participant among app users responded that glucose diary was their most utilized feature. Similarly, 65% participant in non-app users group responded that glucose diary was the most desirable feature of any diabetes app [31]. In the same study it was found that diet diary was the least desirable as well as used features with only 38% users using it. This may be attributed to the fact that diet diary requires multiple entries to be done and requires a lot of effort to add each item consumed along with quantity and time. Some Artificial Intelligence based feature may be developed for dietary monitoring to facilitate the patients in monitoring their diet. In a study conducted on adult diabetes patients to assess the usage of app and most utilized features it was found that respondents favored many potential features, including glucose diary and reminders. The study also reported that while mHealth acceptance was high but the engagement level was low [11].
Conclusion
Acceptability of mobile apps as an assisting tool is increasing over time. It is essential to develop a very user-friendly app with high aesthetics which attracts users. It is also important to develop features that require minimum effort and time from the side of the user. In addition information about key concepts must be given in a precise manner to increase the knowledge of the user.
Declarations
Conflict of interest
The authors declare no conflic of interests.
Footnotes
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
References
- 1.IDF. International Diabetes federation. https://idf.org/our-network/regions-members/south-east-asia/members/94-india.html. Published 2022. Accessed 24 Aug 2022.
- 2.World Health Organization. Diabetes: scale up prevention, strengthen care & enhance surveillance. 2016.
- 3.WHO. Diabetes India. http://www.searo.who.int/india/topics/diabetes_mellitus/en/. Published 2019. Accessed 13 May 2019.
- 4.International Telecommunication Union. Measuring the Information Society Report, vol 1. 2018. https://www.itu.int/en/ITU-D/Statistics/Documents/publications/misr2018/MISR2018-ES-PDF-E.pdf. Accessed 23 May 2022.
- 5.International Diabetes Federation. IDF diabetes atlas eighth edition 2017. Int Diabetes Fed. 2017;150. 10.1016/j.diabres.2009.10.007.
- 6.Jeffrey B, Bagala M, Creighton A, et al. Mobile phone applications and their use in the self-management of Type 2 Diabetes Mellitus: a qualitative study among app users and non-app users. Diabetol Metab Syndr. 2019;11(1):84. doi: 10.1186/s13098-019-0480-4. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Zhai Y, Yu W. A mobile app for diabetes management: impact on self-efficacy among patients with type 2 diabetes at a community hospital. Med Sci Monit. 2020;26. 10.12659/MSM.926719. [DOI] [PMC free article] [PubMed]
- 8.Kwan YH, Ong ZQ, Choo DYX, Phang JK, Yoon S, Low LL. A mobile application to improve diabetes self-management using rapid prototyping: iterative co-design approach in asian settings. Patient Prefer Adherence. 2023;17(null):1–11. doi: 10.2147/PPA.S386456. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Böhm A-K, Jensen ML, Sørensen MR, Stargardt T. Real-world evidence of user engagement with mobile health for diabetes management: longitudinal observational study. JMIR Mhealth Uhealth. 2020;8(11):e22212. doi: 10.2196/22212. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Maharaj A, Lim D, Murphy R, Serlachius A. Comparing two commercially available diabetes apps to explore challenges in user engagement: randomized controlled feasibility study. JMIR Form Res. 2021;5. 10.2196/25151. [DOI] [PMC free article] [PubMed]
- 11.Conway N, Campbell I, Forbes P, Cunningham S, Wake D. mHealth applications for diabetes: user preference and implications for app development. Health Informatics J. 2015;22(4):1111–1120. doi: 10.1177/1460458215616265. [DOI] [PubMed] [Google Scholar]
- 12.Joshua SR, Abbas W, Lee J-H, Kim SK. Trust components: an analysis in the development of Type 2 diabetic mellitus mobile application. Appl Sci. 2023;13(3). 10.3390/app13031251.
- 13.Adu MD, Malabu UH, Callander EJ, Malau-Aduli AEO, Malau-Aduli BS. Considerations for the development of mobile phone apps to support diabetes self-management: systematic review. J Med Internet Res. 2018;20(6):1–21. doi: 10.2196/10115. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Tripathi D, Vikram NK, Chaturvedi S, Bhatia N. Barriers and facilitators in dietary and physical activity management of type 2 diabetes: perspective of healthcare providers and patients. Diabetes Metab Syndr Clin Res Rev. 2023;17(3):102741. doi: 10.1016/j.dsx.2023.102741. [DOI] [PubMed] [Google Scholar]
- 15.Kassam-Adams N, Marsac ML, Kohser KL, Kenardy JA, March S, Winston FK. A new method for assessing content validity in model-based creation and iteration of eHealth interventions. J Med Internet Res. 2015;17(4):e95. doi: 10.2196/jmir.3811. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Huynh M, Ghimire P, Truong D. Hybrid app approach: could it mark the end of native app domination?. Issues Informing Sci Inf Technol. 2017;14:049–65. 10.28945/3723.
- 17.Malanda UL, Welschen LM, Riphagen II, Dekker JM, Nijpels G, Bot SD. Self-monitoring of blood glucose in patients with type 2 diabetes mellitus who are not using insulin. Cochrane Database Syst Rev. 2012;1:CD005060. 10.1002/14651858.CD005060.pub3. [DOI] [PubMed]
- 18.Chomutare T, Fernandez-Luque L, Arsand E, Hartvigsen G. Features of mobile diabetes applications: review of the literature and analysis of current applications compared against evidence-based guidelines. J Med Internet Res. 2011;13(3):e65. doi: 10.2196/jmir.1874. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Longvah T, Rajendran A, Bhaskar K, Venkaiah K. Indian food Composition Tables. Indian Council of Medical Research. 2017.
- 20.Misra A, Nigam P, Hills A, et al. Consensus physical activity guidelines for Asian Indians. 2012;14. 10.1089/dia.2011.0111. [DOI] [PubMed]
- 21.World Health Organization. Global Report on Diabetes. 2016. https://www.apps.who.int/iris/bitstream/handle/10665/204871/9789241565257_eng.pdf;jsessionid=740B1057C66B622653A3BD9D39257E6C?sequence=1.
- 22.Cheng M. Ottawa Mood Scale; 2011.
- 23.Ristau RA, Yang J, White JR. Evaluation and evolution of diabetes mobile applications: key factors for health care professionals seeking to guide patients. Diabetes Spectr. 2013;26(4):211 LP–215. doi: 10.2337/diaspect.26.4.211. [DOI] [Google Scholar]
- 24.Veazie S, Winchell K, Gilbert J, Paynter R, Ivlev I, Eden K, Nussbaum K, Weiskopf N, Guise J-M, Helfand M. Mobile Applications for self-management of diabetes. Technical Brief No. 31. (Prepared by the Scientific Resource Center under Contract Nos. 290- 2012-0004-C and 290-2017-00003-C.) AHRQ Publication No. 18-EHC010-EF. Rockville, MD: Agency for Healthcare Research and Quality. Posted final reports are located on the Effective Healthcare Program search page. 2018. 10.23970/AHRQEPCTB31. [PubMed]
- 25.Brzan P, Rotman E, Pajnkihar M, Klanjsek P. Mobile applications for control and self management of diabetes: a systematic review. J Med Syst. 2016;40(9):210–217. doi: 10.1007/s10916-016-0564-8. [DOI] [PubMed] [Google Scholar]
- 26.Årsand E, Muzny M, Sc M, Bradway M, Muzik J, Hartvigsen G. Performance of the first combined smartwatch and smartphone diabetes diary application study. 2015. 10.1177/1932296814567708. [DOI] [PMC free article] [PubMed]
- 27.Petersen M, Hempler N. Development and testing of a mobile application to support diabetes selfmanagement for people with newly diagnosed type 2 diabetes: a design thinking case study. Inform Decis Mak BMC Med Inform Decis Mak. 2017;17(1):91. doi: 10.1186/s12911-017-0493-6. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28.Yardley L, Morrison L, Bradbury K, Muller I. The person-based approach to intervention development: application to digital health-related behavior change interventions. J Med Internet Res. 2015;17(1):e30. doi: 10.2196/jmir.4055. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29.Ranjani H, Nitika S, Hariharan R, et al. Systematic review and scientific rating of commercial apps available in India for diabetes prevention. J Diabetol. 2021;12(3):285. doi: 10.4103/jod.jod_68_21. [DOI] [Google Scholar]
- 30.Kebede MM, Pischke CR. Popular diabetes apps and the impact of diabetes app use on self-care behaviour: a survey among the digital community of persons with diabetes on social media. Front Endocrinol. 2019;10:135. https://www.frontiersin.org/article/10.3389/fendo.2019.00135. Accessed 25 May 2022. [DOI] [PMC free article] [PubMed]
- 31.Boyle L, Grainger R, Hall RM, Krebs JD. Use of and beliefs about mobile phone apps for diabetes self-management: surveys of people in a hospital diabetes clinic and diabetes health professionals in New Zealand. JMIR Mhealth Uhealth. 2017;5(6):e85. doi: 10.2196/mhealth.7263. [DOI] [PMC free article] [PubMed] [Google Scholar]