

Abstract
Background:
Depression is a common mental disorder that significantly contributes to the global burden of disease. Studies have consistently reported that migrant workers experience higher levels of depressive symptoms, especially women.
Aims:
This study aimed to examine the mediation role of sexual self-efficacy on the relationship between psychological wellbeing, and depressive symptoms among young female migrant workers in Vietnam’s industrial zones.
Methods:
A cross-sectional study was conducted among 1061 female migrant workers aged 18 to 29 from January to November 2020 in Hanoi, Vietnam. Anonymous interview questionnaires were used to collect data on demographic characteristics, psychosocial wellbeing (PWB), sexual self-efficacy, and depressive symptoms. Mediation analysis was conducted to explore the mediation effect of sexual self-efficacy on the relationship between PWB and depressive symptoms.
Results:
Nearly 8% of the female migrant workers reported experiencing depressive symptoms. The final mediation model showed that the effect of overall psychological wellbeing on depressive symptoms was partially mediated by sexual self-efficacy. Specifically, 4.1% of the effect of overall PWB on depressive symptoms was mediated through sexual self-efficacy. In the PWB subdimension analyses, sexual self-efficacy mediated 14.3% of the effect of personal growth, 8.8% of the effect of purpose in life, 8.0% of the effect of autonomy, and 7.8% of the effect of environmental mastery on depressive symptoms, respectively.
Conclusion:
The study findings demonstrate that sexual self-efficacy plays an important role in the relationship between psychosocial wellbeing and depressive symptoms among female migrant workers in industrial zones in Vietnam. Improving psychosocial wellbeing and promoting sexual health including sexual self-efficacy should be prioritized when addressing depressive symptoms and mental health concerns among industrial zone female migrant workers in Vietnam, which may also be applicable in other low- and middle-income countries with similar socio-cultural settings.
Keywords: Sexual self-efficacy, psychological wellbeing, depressive symptoms, migrant workers, Vietnam, industrial zones
Introduction
Since 1986, liberal economic policies and rapid urbanization in Vietnam have led numerous foreign investors to establish businesses and factories in the country, particularly in major urban areas (IMF, 2018). Consequently, Vietnam has witnessed a significant internal migration pattern as people flock from rural areas to urban areas seeking better employment opportunities and improved livelihoods (Vo, 2021). This internal migration is characterized by increasing proportions of female migrants over male migrants over time (UNFPA, 2016). A significant factor contributing to this internal migration pattern is the establishment of industrial parks or industrial zones (IZs) in major urban areas. These IZs have become vital economic hubs, supporting various industries such as electronics, textiles, footwear, and automobile parts. As a result, a substantial number of migrant workers, particularly women from rural areas, are drawn to these IZs for employment opportunities. These young women often come from low income, patriarchal families in the rural areas where they have had limited education (Bélanger, 2010). As of May 2021, Vietnam had a total of 284 operational IZs with approximately 3.78 million workers, of which the great majority are young women (Savills, 2022).
Rural-to-urban migration is a complex process that offers both benefits and challenges to migrant workers, influencing their overall well-being and mental health. Several studies conducted in different countries have found that rural-to-urban migrant workers are vulnerable to mental health issues, particularly depressive symptoms, due to factors such as social and residential isolation in urban areas (Hu et al., 2008; Jirapramukpitak et al., 2008; Li et al., 2006; Mucci et al., 2020), poor living conditions (B. L. Zhong et al., 2018), long working hours (B. X. Tran, Vu, et al., 2019), unfavorable working conditions, financial difficulties (Kesornsri et al., 2014; B. L. Zhong et al., 2018), lack of social support (Lu, 2010b; Pyakuryal et al., 2011), and social exclusion (Nikoloski et al., 2019). These studies have consistently reported that migrant workers experience higher levels of depressive symptoms. Moreover, research has consistently shown that migrant workers are at a greater risk of depression compared to the general population (Hasan et al., 2021; Hnuploy, 2019; Mucci et al., 2020; Yang et al., 2020) with women experiencing a higher risk than men (Albers et al., 2016; Lu, 2010a).
In Vietnam, IZs jobs are often low-paying and require long hours of work, but they provide a means of income for women who otherwise would have limited opportunities for employment. Working in the IZs offers limited opportunities for personal growth, education, and autonomy (Tran & Pham, 2015). Most migrant workers in IZs often face long working hours, live in unhygienic housing and living conditions, low occupational safety, and have limited access to public services (Bui et al., 2021; UNFPA, 2016). These challenges can lead to health problems, including physical health problems and depression (Do et al., 2020; Pham et al., 2019; B. X. Tran, Vu, et al., 2019). Recent studies conducted among IZ workers in Vietnam found depressive symptoms ranging from 30.5% (Do et al., 2020) to 38.6% (B. X. Tran, Vu, et al., 2019). These findings underscore the need for interventions to enhance the mental health of migrant workers in industrial zones in Vietnam, particularly in reducing depressive symptoms and providing access to mental health services and support.
According to self-efficacy theory (Bandura, 1977), individuals who possess confidence in their ability to perform a task are more likely to engage in that behavior and achieve positive results. Individuals with higher levels of self-efficacy are more likely to engage in adaptive behaviors, cope effectively with stressors, and maintain positive mental health outcomes. Conversely, those with lower levels of self-efficacy may be more vulnerable to negative outcomes, such as depression (Schwarzer, 1995; Trenoweth, 2017). In the context of sexual behaviors, sexual self-efficacy plays a crucial role. Sexual self-efficacy is multidimensional concept that include an individual’s perceived control over or confidence in their capacity to achieve a particular sexual outcome (Closson et al., 2018). Sexual self-efficacy pertains to one’s self-confidence for effectively managing sexual relationships and appropriately adapting to the sexual partner (Atrian et al., 2019). It is a health behavior that demands cognitive effort, self-control, and consistent practice (Alvy et al., 2011). Previous research has demonstrated that there is a positive relationship between sexual self-efficacy and mental health. For instance, previous studies have found that lower sexual assertiveness and sexual self-efficacy was negatively associated with higher depression among sexual minority women (Engelbrecht, 2020), while female sexual self-efficacy has been found to be negatively associated with the cognitive dimension of the Beck Depression Inventory (Finotelli Jr. et al., 2023). When individuals are unable to consistently display sexual self-efficacy, they may experience pressure and worry, which can lead to feelings of inadequacy and nervousness in social situations. These emotions can further intensify anxiety and depression (Alvy et al., 2011).
Psychosocial wellbeing (PWB) is a comprehensive construct that encompasses psychological, social, and personal factors that affect an individual’s ability to achieve their full potential in society (Kumar, 2020). It also refers to the interconnectedness between an individual’s mental health and their social experiences (Kumar, 2020). According to Ryff (1989), this construct can be characterized by six dimensions: autonomy, environmental mastery, personal growth, positive relationships, purpose in life, and self-acceptance. Previous studies have found an association between sexual self-efficacy and PWB dimensions. For example, having confidence in one’s ability to experience pleasure during sexual activity and effectively use condoms has been shown to be related to greater levels of global self-esteem, identity achievement, and overall life satisfaction (Zimmer-Gembeck & French, 2016). Autonomy is a crucial component of PWB, and it has been shown to be positively associated with sexual self-efficacy. For instance, a study among young rural to urban migrants in China found that those who had higher sexual self-efficacy and autonomy were more likely to engage in safer sexual behaviors (Xiao et al., 2013).
Studies have also found PWB to be associated with depression. A systematic review among migrant workers and psychological health found that those with low PWB were more likely to experience depression (Mucci et al., 2020). Similarly, a longitudinal study of medical interns found that low PWB at baseline was associated with increased depression symptoms over time (Grant et al., 2013). In addition, a recent study among older adults in the United States found that PWB was negatively associated with depressive symptoms with autonomy, environmental mastery, purpose in life, and self-acceptance being significant predictors of lower depressive symptoms (Zimmer-Gembeck & French, 2016). These studies highlight the potential importance of PWB in the development of depression. However, further research is needed to fully understand the complexities of this relationship.
Mediation analysis is a statistical approach that involves estimating the total effect of an independent variable on a dependent variable into a direct effect and an indirect effect through a mediator variable (Mackinnon, 2012). Mediation analysis allows researchers to go beyond observing a simple association between variables and enables them to investigate the intermediate processes that occur between the independent and dependent variables. It provides a framework to assess whether the effect of the independent variable on the dependent variable is fully or partially mediated by the mediator variable (MacKinnon et al., 2007). Despite previous research, no known studies have investigated the mediating effects of sexual self-efficacy in the relationship between PWB and depressive symptoms among migrant workers or how different PWB dimensions impact depressive symptoms among this population. Examining these potential mediating effects and gaining an enhanced understanding of their underlying mechanisms could offer valuable insights for designing interventions to prevent and mitigate depression among female migrant workers.
The purpose of this study is to assess the mediating role of sexual self-efficacy in the relationship between PWB and depressive symptoms among female migrant workers employed in IZs in Vietnam. Specifically, we hypothesize that (1) higher levels of PWB will be associated with lower levels of depressive symptoms; (2) greater sexual self-efficacy will be associated with lower levels of depressive symptoms; and (3) higher levels of PWB will be associated with higher levels of sexual self-efficacy, which in turn will be associated with a decrease in depressive symptoms (Figure 1).
Figure 1.
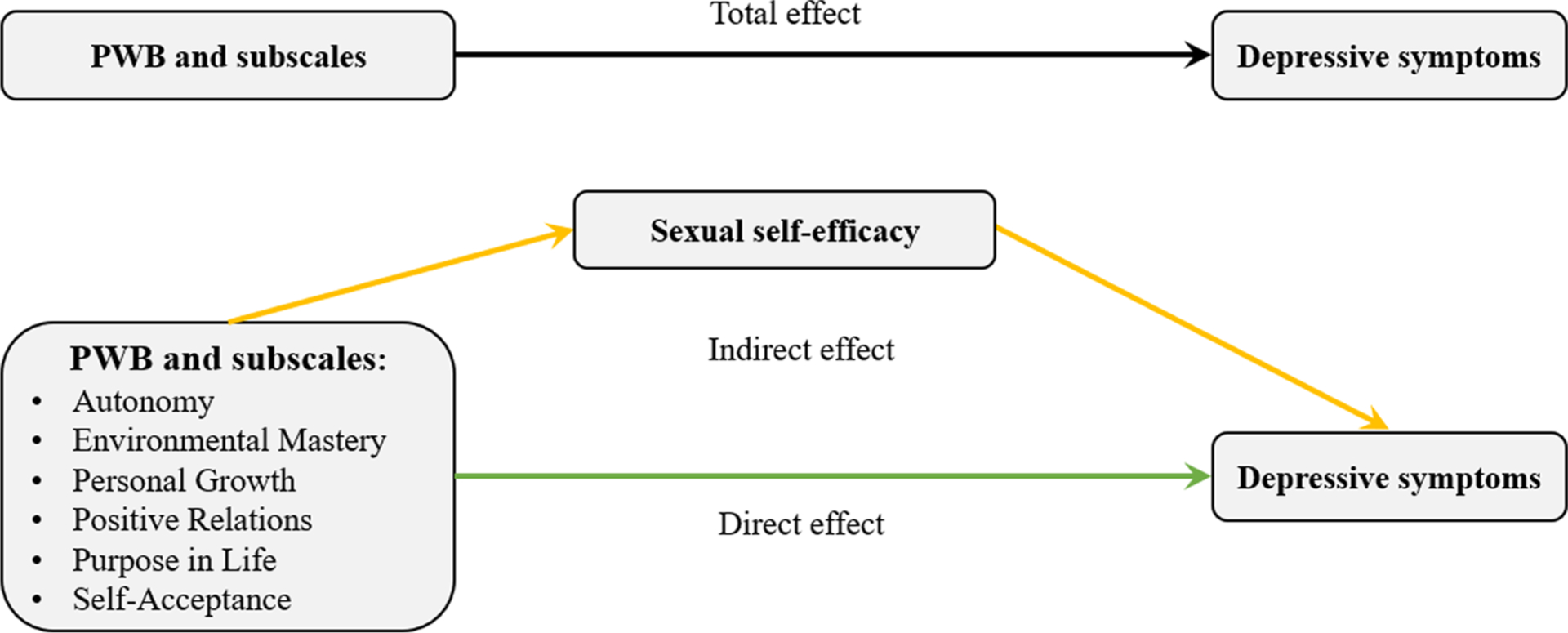
Conceptual diagram of the mediation model of sexual self-efficacy on the relationship between psychosocial wellbeing (PWB), PWB subscales, and depressive symptoms.
Materials and methods
Study site and participants
Data were collected from a study titled “HIV risk among young women migrant workers in the industrial zones in Vietnam,” which is described in detail in prior publications (Ha et al., 2022; Ha et al., 2021). A cross-sectional study was conducted among 1061 young migrant women from January 2019 to November 2020 in Thang Long Industrial Park on the outskirts of Hanoi, the capital of Vietnam. Eligibility criteria for participation in the study included: (1) identify as a woman; (2) aged 18 to 29 years; (3) either single, currently married but not living with a husband or partner while working in the IZ, separated, divorced, or widowed; (4) have worked in the IZ for six or more months; and (5) relocated from a rural area or another province prior to IZ employment. The original study’s primary objective was to investigate the prevalence of HIV and associated risks among female migrant workers as this group has been previously found to engage in risky sexual behavior with low levels of condom use (B. X. Tran, Vo, et al., 2019). We then utilized this dataset to explore the relationship between psychosocial well-being, sexual self-efficacy, and depressive symptoms among this population.
The study was approved by the University of Connecticut Health Center Institutional Review Board and the Institute for Social and Medical Studies, Vietnam (IRB approval number: 19–134O-1 on 10/13/2020). Written informed consent in Vietnamese was obtained from all participants in the study.
Sample size and sampling recruitment process
The study used a cluster sampling design to select groups of women living and working in close proximity, such as those in rent clusters or dormitories. Since this design can include similar-behaving subjects that may impact the study’s power, we accounted for this by considering the intra-class correlation within the primary sampling units (Killip et al., 2004). As a result, a total of 1061 participants were determined to be needed for the survey.
To support with recruitment, the research team obtained information about rent clusters, including the names of owners, total workers, and the number of women workers aged 18 to 29 years from officials of the local administrative authority. To enroll eligible participants, the team used a multistage clustered sampling method. First, we mapped and enumerated 779 rent clusters and two dormitories located near the industrial zone. We then selected rental clusters with six or more eligible participants, which resulted in the exclusion of 360 rental clusters and left 419 qualifying rental clusters. The research team, along with the collaborators who were former IZ women workers and invited to be part of the study advisory board, directly contacted women in the eligible age group for screening and enrollment. These former IZ women workers, having firsthand experience and knowledge of the challenges faced by women in the IZs, were able to establish a relatable connection with the participants and helped foster a sense of trust and understanding between the research team and the potential participants. Moreover, their involvement during the recruitment process created a supportive and empathetic environment. Initially, 1316 eligible migrant workers from the 419 rent clusters were contacted to participate in the study, but 320 refused to participate, resulting in a total of 936 participants from the rent clusters being selected for the study. For the two qualifying dormitories, the dormitory manager provided a list of 175 eligible participants who were contacted, and 125 agreed to participate in the study.
Data collection
Eligible participants were invited to an information session held after working hours at a nearby commune health center, which was organized by the research team in collaboration with guides who were current or former IZ women workers. During the meeting, participants were given a comprehensive explanation of the study, including the activities they would be expected to engage in, the survey topics, the expected time commitment for the study, their right to decline or withdraw, and the measures in place to safeguard confidentiality. A written informed consent form was provided to each participant, which they were asked to review, and the research team was on hand to answer any questions or concerns that arose. Participants were given ample time to weigh the risks and benefits of participation before being asked to provide written informed consent to enroll in the study. Those who agreed to participate were invited to a face-to-face, hour-long anonymous interview using closed-ended questions, which was conducted by trained field researchers. All interviewers were trained in interviewing techniques, establishing rapport, ensuring confidentiality, and addressing questions raised by participants.
Measures
Sociodemographic characteristics.
We collected demographic characteristics of participants, including age, marital status, education, ethnicity, monthly income, residence type (rent clusters or dormitories), and number of working hours per day.
Psychological wellbeing
Psychological wellbeing was measured using 18-item Ryff’s scale of Psychological Wellbeing (Ryff & Keyes, 1995). The scale includes three items for each of the six dimensions of wellbeing: self-acceptance, autonomy, environmental mastery, purpose in life, positive relations with others, and personal growth. The scale has been validated in Vietnam (Calderon Jr et al., 2019). Autonomy assesses the degree of self-determination and freedom from societal norms; Environmental mastery evaluates one’s ability to manage life events; Personal growth assesses openness to new experiences and growth; Purpose in life measures the sense of purpose and meaningfulness in life; Positive relations with others assesses the extent of satisfying relationships with others; and Self-acceptance assesses one’s attitude toward oneself. Participants were asked to rate the extent to which each item describes themselves on a 7-point Likert scale, ranging from 1 (“strongly disagree”) to 7 (“strongly agree”). In the analysis, the total score was reverse-coded so that higher scores represented higher levels of wellbeing.
Sexual self-efficacy
Sexual self-efficacy was assessed using a four-item scale measuring participants’ self-confidence in refusing sexual activity with their partner(s) under specific circumstances. For example, “How confident are you that you could refuse to engage in sexual activity with your boyfriend if you didn’t want to?” Participants responded to each item using a four-point Likert scale ranging from 1 (“Not at all”) to 4 (“Very sure”). The responses were averaged to create a composite score. The Cronbach’s alpha was 0.75.
Depressive symptoms
Depressive symptoms were assessed using a nine-item PHQ scale (Kroenke et al., 2001, 2010), which asked how often the participants had been bothered by any of the nine items during the immediately preceding two weeks (e.g., “Over the past two weeks, how often have you been bothered by any of the following problems?” Each item of PHQ-9 was scored on a scale of 0–3 (0 = not at all; 1 = several days; 2 = more than a week; and 3 = nearly every day). The PHQ-9 total score ranges from 0 to 27, with scores of 0–4 indicating no depression, 5–9 indicating mild depression, 10–14 indicating moderate depression, 15–19 indicating moderately severe depression, and ⩾20 indicating severe depression. The scale has been validated among the Vietnamese population (Vu et al., 2022). The Cronbach’s alpha was 0.85. To determine the presence of depressive symptoms, we used a cut-off point of eight, which has been previously established in the literature (Manea et al., 2012).
Other covariates.
Other covariates included (1) use of sexual and reproductive health (SRH)/HIV services since working in the IZ (Yes/No) and (2) the number of health problems experienced by the participants during the past year in which participants were provided with a list of common health problems and asked to indicate which problems they had personally experienced (Yes/No).
Statistical analysis
Descriptive statistics.
The data are presented as means and standard deviations (SD) for variables that follow a normal distribution, and as medians with interquartile ranges (IQR) for non-normally distributed variables. The scores for psychosocial wellbeing (PWB) and its subscales were reported as means (SD), medians (IQR), and range.
Multivariable linear regression models.
Multiple linear regression models were used to examine the relationship between depressive symptoms and overall psychosocial wellbeing (PWB), as well as each of its subcomponents: autonomy, environmental mastery, personal growth, positive relations, purpose in life, and self-acceptance. The models were adjusted for covariates, including socio-demographic variables, health problems, use of SRH/HIV services, and sexual self-efficacy. The distribution of depressive symptoms was not normally distributed and was natural log transformed before conducting the regression analysis. Prior to the multivariable linear regression analyses, we conducted bivariate analyses between each outcome (e.g., depressive symptoms), independent factors (e.g., PWB), and covariates (e.g., age, education). Only those variables that were significant at p < .25 in the bivariate models were included in the multivariable regression models. p-value < .05 was considered statistically significant. All analyses were performed using Stata Statistical Software (version 17.0, Stata Corp, College Station, TX) and SAS (version 9.4; SAS Institute, Cary, NC).
Mediation analysis.
Mediation models were conducted using the mediation package in R (bruceR:PROCESS function, version 0.8.8) [49] to estimate the coefficients of the total, indirect, and direct effects of sexual self-efficacy on the relationship between overall PWB, PWB subcomponents (i.e., autonomy, environmental mastery, personal growth, positive relations, purpose in life, self-acceptance) and depressive symptoms. The models were adjusted for age, education, marital status, ethnicity, monthly income, residence type, the use of SRH/HIV services, and health problems. We used the bias-corrected bootstrap method to estimate the coefficients of the total, indirect, and direct effects and calculate their 95% confidence intervals. The proportion of mediation (PM, %) was computed using the indirect effect divided by the total effect. Statistical significance was defined p-value < .05, and all analyses were performed using Stata statistical software version 17.0 (Stata Corp, College Station, TX) and R statistical software version 4.0.3 (R Studio).
Results
Table 1 displays the sample’s socio-demographic characteristics. Of the total 1061 young women workers who completed the survey, the mean age was 22.8 years and ranged from 18 to 29 (Table 1). Most respondents had completed high school. Over two-thirds of the respondents (n = 760) reported never being married. Respondents’ years of working at the current IZ ranged from less than 1 year to over 5 years with two-thirds in the 2- to 5-year category and 14% over 5 years. While most of the respondents worked 8 hours or less a day, nearly 24% were working over 8 hours a day. The mean monthly income was US$294, with a range of $195 to $652. The study found that 7.7% of participants reported experiencing depressive symptoms.
Table 1.
Sample demographic characteristics (n = 1,061).
| Characteristic | N = 1,061a |
|---|---|
| Age (years), n (%) | |
| 18–24 | 699 (65.9%) |
| 25–29 | 362.0 (34.1%) |
| Education, n (%) | |
| Less than high school | 109 (10.3%) |
| High school or above | 952.0 (89.7%) |
| Marital status, n (%) | |
| Single | 760.0 (71.6%) |
| Married | 301.0 (28.4%) |
| Ethnicity, n (%) | |
| Kinh (the majority) | 735.0 (69.3%) |
| Other minority groups | 326 (30.7%) |
| Income per month (USD), median (IQR) | 282.6 (195.7, 478.3) |
| Residence type, n (%) | |
| Dormitory | 125 (11.8%) |
| Rent cluster | 936.0 (88.2%) |
| Use of SRH/HIV since living in the IZ | |
| No | 693 (65.3%) |
| Yes | 368.0 (34.7%) |
| Health problem score, median (IQR) | 7.0 (4.0, 10.0) |
| Sexual self-efficacy, median (IQR) | 10.0 (8.0, 12.0) |
| Depressive symptoms, mean (SD) | 3.4 (3.3) |
Median (IQR) or frequency (%).
Associations between overall PWB and PWB subdimensions and depressive symptoms
Table 3 presents the results of the multivariable linear regression analysis examining the relationship between depressive symptoms and both overall psychosocial well-being and its six subdimensions (autonomy, environmental mastery, personal growth, positive relations, purpose in life, and self-acceptance). The results showed a significant negative association between depressive symptoms and overall PWB (β = −.023, 95% CI [−0.027, −0.018], p < .001). Additionally, significant negative associations between depressive symptoms and each of the PWB sub-dimensions were found: autonomy (β = −.023, 95% CI [−0.038, −0.009], p = .001), environmental mastery (β = −.050, 95% CI [−0.066, −0.035], p < .001), personal growth (β = −.023, 95% CI [−0.043, −0.004], p = .018), positive relations (β = −.052, 95% CI [−0.066, −0.038], p < .001), purpose in life (β = −.031, 95% CI [−0.047, −0.015], p < .001), and self-acceptance (β = −.059, 95% CI [−0.072, −0.046], p < .001).
Table 3.
Associations between PWB and PWB subscales and depressive symptoms.
| Predictors | β | SE | p-value | 95% CI | R2 (%) |
|---|---|---|---|---|---|
| Overall PWB | |||||
| Model 1 | −.036 | .002 | <.001** | [−0.041, −0.031] | 18.9 |
| Model 2 | −.024 | .002 | <.001** | [−0.028, −0.020] | 39.0 |
| Model 3 | −.023 | .002 | <.001** | [−0.027, −0.018] | 39.4 |
| Autonomy | |||||
| Model 1 | −.045 | .009 | <.001** | [−0.062, −0.028] | 5.3 |
| Model 2 | −.025 | .007 | .001* | [−0.040, −0.011] | 33.2 |
| Model 3 | −.023 | .007 | .001* | [−0.038, −0.009] | 34.3 |
| Environmental mastery | |||||
| Model 1 | −.085 | .009 | <.001** | [−0.102, −0.067] | 10.3 |
| Model 2 | −.054 | .008 | <.001** | [−0.069, −0.038] | 35.3 |
| Model 3 | −.050 | .008 | <.001** | [−0.066, −0.035] | 36.1 |
| Personal growth | |||||
| Model 1 | −.048 | .011 | <.001** | [−0.071, −0.025] | 4.3 |
| Model 2 | −.028 | .010 | .005* | [−0.047, −0.008] | 32.9 |
| Model 3 | −.023 | .010 | .018* | [−0.043, −0.004] | 34.0 |
| Positive relations | |||||
| Model 1 | −.077 | .009 | <.001** | [−0.094, −0.060] | 9.8 |
| Model 2 | −.055 | .007 | <.001** | [−0.069, −0.040] | 35.8 |
| Model 3 | −.052 | .007 | <.001** | [−0.066, −0.038] | 36.7 |
| Purpose in life | |||||
| Model 1 | −.046 | .010 | <.001** | [−0.065, −0.026] | 4.8 |
| Model 2 | −.034 | .008 | <.001** | [−0.050, −0.018] | 33.5 |
| Model 3 | −.031 | .008 | <.001** | [−0.047, −0.015] | 34.5 |
| Self-acceptance | |||||
| Model 1 | −.099 | .007 | <.001** | [−0.114, −0.085] | 16.8 |
| Model 2 | −.062 | .007 | <.001** | [−0.075, −0.048] | 37.3 |
| Model 3 | −.059 | .007 | <.001** | [−0.072, −0.046] | 38.1 |
Note. Model 1: adjusted for age, education, marital status, ethnicity, income per month, and residence type; Model 2: adjusted for model 1 + health problems score and SRH/HIV service usage; Model 3: adjusted for model 2 + sexual self-efficacy. PWB = psychological wellbeing scale; R2 = R-squared.
p < .05.
p < .001.
Mediating effects
The results of mediation effects of sexual self-efficacy on the relationship between depressive symptoms and overall PWB and its subdimensions are presented in Table 4. The results indicate that that overall PWB was negatively associated with depressive symptoms (β = −.023, 95% CI [−0.032, −0.014], p < .001). We also observed sexual self-efficacy was found to partially mediate the associations between overall PWB and depressive symptoms (β = −.001, 95% CI [−0.002, −0.000], p = .013), with a proportion of mediation accounting for 4.2%. When investigating the mediation effects of sexual self-efficacy on six sub-dimensions of psychological wellbeing and depressive symptoms among young female migrant workers in Vietnam’s industrial zones, results showed that sexual self-efficacy played a significant mediating role between each of the six PWB sub-dimensions and depressive symptoms. However, the extent of the mediation effects varied across the sub-dimensions. Specifically, personal growth had the highest proportion of mediation effect (14.3%), followed by purpose in life (8.8%) and autonomy (8.0%). On the other hand, the sub-dimensions of environmental mastery (4.4%), self-acceptance (4.8%), and positive relations with others (5.5%) had the lowest proportions of mediation.
Table 4.
Direct effect of PWB and its subscales, and indirect effects of sexual self-efficacy on the risk of depressive symptoms and the proportion mediated by sexual self-efficacy.
| Predictors | Direct effect | Indirect effect | Proportion mediated (%) | ||||
|---|---|---|---|---|---|---|---|
| βDir (Boot 95% CI) | Z | p value | βInd (Boot 95% CI) | Z | p value | ||
| PWB total score | −.023 (−0.028, −0.018) | −9.482 | <.001** | −.001 (−0.002, −0.000) | −2.487 | .013* | 4.2 |
| Autonomy | −.023 (−0.038, −0.009) | −3.141 | .002* | −.002 (−0.005, −0.000) | −1.897 | .058 | 8.0 |
| Environmental mastery | −.050 (−0.066, −0.035) | −6.341 | <.001** | −.004 (−0.006, −0.001) | −2.709 | .007* | 7.4 |
| Personal growth | −.023 (−0.042, −0.004) | −2.389 | .017* | −.004 (−0.008, −0.002) | −2.668 | .008* | 14.3 |
| Positive relations | −.052 (−0.066, −0.039) | −7.394 | <.001** | −.003 (−0.005, −0.001) | −2.353 | .019** | 5.5 |
| Purpose in life | −.031 (−0.048, −0.013) | −3.479 | <.001** | −.003 (−0.006, −0.001) | −2.394 | .017** | 8.8 |
| Self-acceptance | −.059 (−0.073, −0.045) | −8.269 | <.001** | −.003 (−0.005, −0.001) | −2.390 | .017** | 4.8 |
Note. Models were adjusted by age, education, marital status, ethnicity, monthly income, residence type, health problems, and used SRH/HIV services. PWB = psychological wellbeing scale.
p < .05.
p < .001.
Discussion
This is the first known study to explore the mediating role of sexual self-efficacy in the association between psychosocial wellbeing (PWB) and depressive symptoms among young female migrant workers in Vietnam’s industrial zones (IZs). Specifically, higher PWB is associated with higher sexual self-efficacy which in turn is associated with lower levels of depressive symptoms. These findings emphasize the importance of considering both PWB and sexual self-efficacy in the design of interventions and programs aimed at improving the mental health outcomes of this vulnerable population. By recognizing the significant mediating effect of sexual self-efficacy on PWB and depressive symptoms, mental health interventions can take a more holistic approach to addressing the mental health needs of this population.
The findings further indicate that sexual self-efficacy plays a significant mediating role in the relationship between specific sub-dimensions of PWB and depressive symptoms among female migrant workers in Vietnam’s IZs. The highest proportion of mediation effect was observed for personal growth (14.3%), followed by purpose in life (8.8%) and autonomy (8.0%). On the other hand, the lowest proportion of mediation effect was observed for environmental mastery (4.4%), followed by self-acceptance (4.8%) and positive relations with others (5.5%). These results underscore the importance of prioritizing specific domains of PWB in mental health interventions for this population. Efforts aimed at reducing depressive symptoms and improving the mental health of female migrant workers in Vietnam’s IZs should prioritize strategies that enhance sexual self-efficacy, as well as promote personal growth, purpose in life, and autonomy.
Among the female migrant workers studied in this research, nearly 8% reported experiencing depressive symptoms, which is lower than the prevalence reported in a previous study conducted among migrant workers in IZs in Vietnam (38.6%) (B. X. Tran, Vu, et al., 2019) and factory migrant workers in China (34.4%) (B. L. Zhong et al., 2018). However, it is important to consider that the nature of work may vary between these studies, which could contribute to differences in the levels of depressive symptoms observed. For instance, a study among Vietnamese IZ workers revealed that those who were exposed to toxic gas and workplace hazards with a higher risk of accidents reported higher levels of depressive symptoms compared to those who were not exposed (B. X. Tran, Vu, et al., 2019). Another study showed that workers in the electronics factory reported higher levels of depressive symptoms (37%) compared to those working in the textile/shoe-making factories (Do et al., 2020).
The results of this study indicate that overall PWB and its subdimensions have a significant negative association with depressive symptoms, which is consistent with previous research (Grant et al., 2013; Zimmer-Gembeck & French, 2016). The findings suggest that enhancing the psychological wellbeing of female migrant workers is crucial. However, achieving this goal can be challenging because of the demanding nature of their jobs, which often involve heavy workloads and long working hours. As a result, they may not have sufficient opportunities to engage in activities that could improve their PWB. For example, a previous study of migrant workers in Vietnam’s garment factories found that low wages, job insecurity, and being exhausted from working long hours limited their personal and professional growth, visiting friends/families and affected their happiness and status in the family (OXFAM, 2019; Siu & Unger, 2019). Similarly, service industry migrant workers in China often face social isolation and a lack of opportunities for personal growth and social interaction due to their low-income status and demanding work schedules (B. Zhong et al., 2016). High work demands and lack of decision-making autonomy have been shown to contribute to stress among factory migrant workers (Lau et al., 2012). Therefore, improving the PWB of female migrant workers may require creating enabling activities to promote autonomy, personal growth, and purpose in life, as well as advocating for increased minimum wage and better living conditions. Given that the majority of migrant workers in Hanoi reside in rented clusters located in suburban areas and isolated locations, which often lack a supportive living environment for their personal development, it is imperative to address this issue. Establishing supportive environments and social networks that facilitate social support and encouraging engagement in local social activities is vital for enhancing their psychosocial wellbeing. These measures may contribute to creating a positive and fulfilling experience for migrant workers in their new surroundings.
This study found that higher sexual self-efficacy was associated with lower depressive symptoms among female migrant workers. According to Alvy et al. (2011), if individuals are unable to display consistent sexual self-efficacy, they may experience pressure and worry, leading to feelings of inadequacy and nervousness in social situations. These emotions can further intensify anxiety and depression (Alvy et al., 2011). Our findings suggest interventions aimed at enhancing sexual self-efficacy could be an effective strategy to help female migrant workers develop the skills and confidence necessary to engage in healthy sexual practices, which can ultimately improve their overall mental health.
It is important to consider the important role of empowerment in the context of improving sexual self-efficacy among migrant women workers in this study. The World Health Organization defines empowerment as a progressive process in which individuals and communities attain increased control over the decisions and actions that impact their health (WHO, 1998). Empowerment involves setting goals, enhancing self-efficacy and skills, taking actions, and reflecting on outcomes (Cattaneo & Chapman, 2010). As suggested by Rawlett (2014), self-efficacy and empowerment are interconnected, as a strong sense of self-efficacy often leads to empowerment, and in turn, empowerment further reinforces and strengthens self-efficacy for both present and future situations (Rawlett, 2014). A study conducted with women who had a history of drug use revealed the effectiveness of empowerment-based interventions in enhancing sexual self-efficacy (Faridi et al., 2022). These findings suggest that similar approaches can be applied to migrant women workers. By incorporating empowerment strategies into interventions, their sexual self-efficacy can be improved. This will enable them to make informed choices, set personal boundaries, and navigate their sexual lives with greater confidence.
This study has some limitations that should be taken into consideration when interpreting the findings. First, the cross-sectional design of the study limits the ability to establish causality between the variables. Second, the study included a sample of young female migrant workers in Vietnam’s IZs, which may limit the generalizability of the findings to other populations. Another limitation is the reliance on self-reported measures, which are susceptible to bias and social desirability. Additionally, our study did not collect information about the effects of those with peer support on sexual self-efficacy among the participants. This omission may introduce bias in the study results, as it restricts our ability to examine potential differences in participants’ sexual efficacy based on the presence or absence of a support network. It is possible that individuals from a particular region who have experienced strong peer support may exhibit higher levels of sexual efficacy compared to those who migrated in isolation. To gain a more comprehensive understanding of the influence of peer support on sexual self-efficacy among migrant workers, it is important to further investigate and control such confounding variables. Despite these limitations, the current study provides important insights into the relationships between sexual self-efficacy, psychosocial wellbeing, and depressive symptoms among young female migrant workers in Vietnam’s industrial zones.
Conclusion
This study provides empirical evidence that sexual self-efficacy plays an important role in the relationship between psychosocial wellbeing (PWB) and depressive symptoms among female migrant workers in industrial zones (IZs) in Vietnam. Interventions that address PWB as well as improving sexual self-efficacy may have a greater impact on reducing depressive symptoms among this population. Improving PWB and promoting sexual health, including sexual self-efficacy, should be prioritized when addressing depressive symptoms and mental health concerns among female migrant workers in IZs in Vietnam, which may also be applicable in other low- and middle-income countries with similar socio-cultural settings.
Table 2.
PWB score and PWB subscale distribution (n = 1,061).
| Overal PWB score and its six dimensions | Mean (SD) | Median (IQR) | Range |
|---|---|---|---|
| Overall PWB score | 88.4 (8.9) | 89.0 (82.0, 94.0) | 44.0–111.0 |
| Autonomy | 14.6 (2.8) | 14.0 (13.0, 17.0) | 5.0–21.0 |
| Environmental mastery | 14.6 (2.6) | 14.0 (13.0, 17.0) | 6.0–20.0 |
| Personal growth | 14.0 (2.0) | 14.0 (12.0, 16.0) | 4.0–19.0 |
| Positive relations | 14.3 (2.7) | 14.0 (13.0, 17.0) | 6.0–20.0 |
| Purpose in life | 16.2 (2.4) | 18.0 (14.0, 18.0) | 6.0–21.0 |
| Self-acceptance | 14.6 (3.0) | 15.0 (13.0, 17.0) | 5.0–21.0 |
Note. PWB = psychological wellbeing scale.
Acknowledgements
The authors are grateful to migrant workers who agreed to participate in this study.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the National Institute of Mental Health/National Institutes of Health, USA [grant number R21MH118986].
References
- Albers HM, Kinra S, Radha Krishna KV, Ben-Shlomo Y, & Kuper H (2016). Prevalence and severity of depressive symptoms in relation to rural-to-urban migration in India: A cross-sectional study. BMC Psychology, 4(1), 47. 10.1186/s40359-016-0152-1 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Alvy LM, McKirnan DJ, Mansergh G, Koblin B, Colfax GN, Flores SA, & Hudson S (2011). Depression is associated with sexual risk among men who have sex with men, but is mediated by cognitive escape and self-efficacy. AIDS and Behavior, 15(6), 1171–1179. 10.1007/s10461-010-9678-z [DOI] [PubMed] [Google Scholar]
- Atrian MK, Dehnavi ZM, & Kamali Z (2019). The relationship between sexual self-efficacy and sexual function in married women. Journal of Midwifery and Reproductive Health, 7(2), 1703–1711. 10.22038/jmrh.2018.30672.1333 [DOI] [Google Scholar]
- Bandura A (1977). Self-efficacy: Toward a unifying theory of behavioral change. Psychological Review, 84(2), 191–215. 10.1037//0033-295x.84.2.191 [DOI] [PubMed] [Google Scholar]
- Bélanger DPK (2010). Vietnamese daughters in transition: Factory work and family relations. The Asia-Pacific Journal, 8(5), 3295. [Google Scholar]
- Bui HTT, Duong DM, Pham TQ, Mirzoev T, Bui ATM, & La QN (2021). COVID-19 stressors on migrant workers in Vietnam: Cumulative risk consideration. International Journal of Environmental Research and Public Health, 18(16), 8757. 10.3390/ijerph18168757 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Calderon R Jr, Nguyen N, Truong Quang T, Bui Q, Thuận N, & Viet Bao V (2019). Adapting the ryff scales of psychological well-being: A 28-item Vietnamese version for university students. Asian Journal of Social Sciences & Humanities, 5, 176–197. 10.33100/jossh5.2.Calderon.etal [DOI] [Google Scholar]
- Cattaneo LB, & Chapman AR (2010). The process of empowerment: A model for use in research and practice. American Psychologist, 65(7), 646–659. 10.1037/a0018854 [DOI] [PubMed] [Google Scholar]
- Closson K, Dietrich JJ, Lachowsky NJ, Nkala B, Palmer A, Cui Z, Beksinska M, Smit JA, Hogg RS, Gray G, Miller CL, & Kaida A (2018). Sexual self-efficacy and gender: A review of condom use and sexual negotiation among young men and women in Sub-Saharan Africa. The Journal of Sex Research, 55(4–5), 522–539. 10.1080/00224499.2017.1421607 [DOI] [PubMed] [Google Scholar]
- Do HN, Nguyen AT, Nguyen HQT, Bui TP, Nguyen QV, Tran NTT, Nguyen LH, Pham HQ, Ha GH, Hoang CL, Tran BX, Latkin CA, Ho RCM, & Ho CSH (2020). Depressive symptoms, suicidal ideation, and mental health service use of industrial workers: Evidence from Vietnam. International Journal of Environmental Research and Public Health, 17(8), 2929. 10.3390/ijerph17082929 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Engelbrecht E (2020). Sexual experiences and association with depression and anxiety sexual experiences and association with depression and anxiety among sexual minority women among sexual minority women [Master’s theses]. University of Massachusetts Amherst [Google Scholar]
- Faridi N, Vakilian K, & Yousefi A (2022). Effect of sexual empowerment counseling on self-efficacy, assertive sexual communication, self-awareness, and sexual attitude, awareness of sexually transmitted diseases, and HIV in addicted women - an interventional study. Current Womens Health Reviews, 19, 1–12. 10.2174/1573404819666220901152502 [DOI] [Google Scholar]
- Finotelli I Jr., Rodrigues O Jr., Braga MR, Carvalho MM, Tavares EP, & do Couto Tavares M (2023). Association between female sexual self-efficacy and depression and anxiety symptoms [Paper presentation]. VII World Congress of Behavioural and Cognitive Therapies, Lima, Peru. [Google Scholar]
- Grant F, Guille C, & Sen S (2013). Well-being and the risk of depression under stress. PLoS One, 8(7), e67395. 10.1371/journal.pone.0067395 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Hasan SI, Yee A, Rinaldi A, Azham AA, Mohd Hairi F, & Amer Nordin AS (2021). Prevalence of common mental health issues among migrant workers: A systematic review and meta-analysis. PLoS One, 16(12), e0260221. 10.1371/journal.pone.0260221 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Ha T, Givens D, Nguyen T, & Nguyen N (2022). Stigmatizing attitudes toward people living with HIV among young women migrant workers in Vietnam. International Journal of Environmental Research and Public Health, 19(11), 6366. 10.3390/ijerph19116366 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Ha T, Schensul SL, Schensul JJ, Nguyen T, & Nguyen N (2021). Sexual risk behaviors, HIV prevalence and access to reproductive health services among young women migrant workers in the industrial zones in Vietnam. Frontiers in Reproduction Health, 3, 775375. 10.3389/frph.2021.775375 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Hnuploy K, Laohasiriwong W, Sornlorm K, & Nutrawong T (2019). Influence of living and working environments on depressive symptoms among Myanmar migrant workers in the South of Thailand. Journal of Clinical Diagnostic Research, 13, 1–5. [Google Scholar]
- Hu X, Cook S, & Salazar MA (2008). Internal migration and health in China. Lancet, 372(9651), 1717–1719. 10.1016/s0140-6736(08)61360-4 [DOI] [PMC free article] [PubMed] [Google Scholar]
- IMF. (2018). Vietnam: Raising millions out of poverty. https://www.imf.org/en/Countries/VNM/vietnam-raising-millions-out-of-poverty
- Jirapramukpitak T, Prince M, & Harpham T (2008). Rural-urban migration, illicit drug use and hazardous/harmful drinking in the young Thai population. Addiction, 103(1), 91–100. 10.1111/j.1360-0443.2007.02059.x [DOI] [PMC free article] [PubMed] [Google Scholar]
- Kesornsri S, Sitthimongkol Y, & Hegadoren KM (2014). Mental health problems among migrant workers: Challenges for nurses in Thailand. Journal of Nursing Science, 32(3), 9–19. [Google Scholar]
- Killip S, Mahfoud Z, & Pearce K (2004). What is an intra-cluster correlation coefficient? Crucial concepts for primary care researchers. Annals of Family Medicine, 2(3), 204–208. 10.1370/afm.141 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Kroenke K, Spitzer RL, & Williams JB (2001). The PHQ-9: Validity of a brief depression severity measure. Journal of General Internal Medicine, 16(9), 606–613. 10.1046/j.1525-1497.2001.016009606.x [DOI] [PMC free article] [PubMed] [Google Scholar]
- Kroenke K, Spitzer RL, Williams JB, & Löwe B (2010). The patient health questionnaire somatic, anxiety, and depressive symptom scales: A systematic review. General Hospital Psychiatry, 32(4), 345–359. 10.1016/j.genhosppsych.2010.03.006 [DOI] [PubMed] [Google Scholar]
- Kumar C (2020). Psychosocial well-being of individuals. In Leal Filho W, Azul AM, Brandli L, Özuyar PG & Wall T (Eds.), Quality Education (pp. 676–686). Springer International Publishing. [Google Scholar]
- Lau JT, Cheng Y, Gu J, Zhou R, Yu C, Holroyd E, & Yeung NC (2012). Suicides in a mega-size factory in China: Poor mental health among young migrant workers in China. Occupational and Environmental Medicine, 69(7), 526. 10.1136/oemed-2011-100593 [DOI] [PubMed] [Google Scholar]
- Li X, Stanton B, Fang X, & Lin D (2006). Social stigma and mental health among rural-to-urban migrants in China: A conceptual framework and future research needs. World Health and Population, 8(3), 14–31. 10.12927/whp.2006.18282 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Lu Y (2010a). Mental health and risk behaviours of rural-urban migrants: Longitudinal evidence from Indonesia. Population Studies, 64(2), 147–163. 10.1080/00324721003734100 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Lu Y (2010b). Rural-urban migration and health: Evidence from longitudinal data in Indonesia. Social Science and Medicine, 70(3), 412–419. 10.1016/j.socscimed.2009.10.028 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Mackinnon DP (2012). Introduction to statistical mediation analysis. Routledge. 10.4324/9780203809556 [DOI] [Google Scholar]
- MacKinnon DP, Fairchild AJ, & Fritz MS (2007). Mediation analysis. Annual Review of Psychology, 58, 593–614. https://pubmed.ncbi.nlm.nih.gov/16968208 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Manea L, Gilbody S, & McMillan D (2012). Optimal cut-off score for diagnosing depression with the patient health questionnaire (PHQ-9): A meta-analysis. CMAJ, 184(3), E191–E196. 10.1503/cmaj.110829 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Mucci N, Traversini V, Giorgi G, Tommasi E, De Sio S, & Arcangeli G (2020). Migrant workers and psychological health: A systematic review. Sustainability, 12(1), 120. https://www.mdpi.com/2071-1050/12/1/120 [Google Scholar]
- Nikoloski Z, Zhang A, Hopkin G, & Mossialos E (2019). Self-reported symptoms of depression among Chinese rural-to-urban migrants and left-behind family members. JAMA Network Open, 2(5), e193355. 10.1001/jamanetworkopen.2019.3355 [DOI] [PMC free article] [PubMed] [Google Scholar]
- OXFAM. (2019). The consequences of low wages – a study on fashion suppliers in Vietnam. https://www.oxfam.org.au/wp-content/uploads/2021/11/The-Consequences-of-Low-Wages-a-Study-on-Fashion-Suppliers-in-Vietnam-.pdf
- Pham KTH, Nguyen LH, Vuong QH, Ho MT, Vuong TT, Nguyen HT, Vu GT, Nguyen HLT, Tran BX, Latkin CA, Ho CSH, & Ho RCM (2019). Health inequality between migrant and non-migrant workers in an industrial zone of Vietnam. International Journal of Environmental Research and Public Health, 16(9), 1502. 10.3390/ijerph16091502 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Pyakuryal A, Tausig M, Subedi S, & Subedi J (2011). Strangers in a familiar land: The psychological consequences of internal migration in a developing country. Stress and Health, 27(3), e199–e208. https://doi.org/ 10.1002/smi.1363 [DOI] [Google Scholar]
- Rawlett K (2014). Journey from self-efficacy to empowerment. Health Care, 2, 1–9. 10.12966/hc.02.01.201426250079 [DOI] [Google Scholar]
- Ryff CD (1989). Happiness is everything, or is it? Explorations on the meaning of psychological well-being. Journal of Personality and Social Psychology, 57(6), 1069–1081. 10.1037/0022-3514.57.6.1069 [DOI] [Google Scholar]
- Ryff CD, & Keyes CLM (1995). The structure of psychological well-being revisited. Journal of Personality and Social Psychology, 69, 719–727. 10.1037/0022-3514.69.4.719 [DOI] [PubMed] [Google Scholar]
- Savills. (2022). The guide to Vietnam industrial zone. https://industrial.savills.com.vn/2022/01/vietnam-industrial-zone/#:~:text=The%20nation%20contains%20394%20industrial,hectares%20as%20of%20May%202021
- Schwarzer R, & Jerusalem M (1995). Generalized self-efficacy scale. In Weinman SWJ & Johnston M (Eds.), Measures in health psychology: A user’s portfolio. Causal and Control Beliefs (pp. 35–37). NFER-NELSON. [Google Scholar]
- Siu K, & Unger J (2019). Work and family life among migrant factory workers in China and Vietnam. Journal of Contemporary Asia, 50, 1–20. 10.1080/00472336.2019.1673465 [DOI] [Google Scholar]
- Tran BX, Vo T, Dang AK, Nguyen QN, Vu GT, Vu LG, Do KN, Latkin CA, Ho CSH, & Ho R (2019). Characterizing unsafe sexual behavior among factory workers in the context of rapid industrialization in Northern Vietnam. International Journal of Environmental Research and Public Health, 16(24), 5085. 10.3390/ijerph16245085 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Tran BX, Vu GT, Pham KTH, Vuong QH, Ho MT, Vuong TT, Nguyen HT, Nguyen CT, Latkin CA, Ho CSH, & Ho RCM (2019). Depressive symptoms among industrial workers in Vietnam and correlated factors: A multi-site survey. International Journal of Environmental Research and Public Health, 16(9), 1642. 10.3390/ijerph16091642 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Tran KV, & Pham QV (2015). Access to social services: How poor migrants experience their life in contemporary Vietnamese urban areas. Journal of Social Sciences and Humanities, 1(3), 277–290. [Google Scholar]
- Trenoweth S (2017). Strengths and mental well-being. In Trenoweth SM (Ed.), Psychosocial assessment (pp. 164–183). Sage Publications. [Google Scholar]
- UNFPA, G. S. O. (2016). The 2015 national internal migration survey: Major findings. https://vietnam.unfpa.org/sites/default/files/pub-pdf/PD_Migration%20Booklet_ENG_printed%20in%202016.pdf
- Vo H (2021). Understanding urban migration in Viet Nam: Evidence from a micro–macro link. (ADBI Working Paper No. 1233). ADBI Institute. https://www.adb.org/publications/understanding-urban-migration-viet-nam-micro-macro-link [Google Scholar]
- Vu LG, Le LK, Dam AVT, Nguyen SH, Vu TTM, Trinh TTH, Do AL, Do NM, Le TH, Latkin C, Ho RCM, & Ho CSH (2022). Factor structures of patient health questionnaire-9 instruments in exploring depressive symptoms of suburban population. Frontier Psychiatry, 13, 838747. 10.3389/fpsyt.2022.838747 [DOI] [PMC free article] [PubMed] [Google Scholar]
- WHO. (1998). Health promotion glossary. https://apps.who.int/iris/handle/10665/64546
- Xiao Z, Li X, Lin D, Jiang S, Liu Y, & Li S (2013). Sexual communication, safer sex self-efficacy, and condom use among young Chinese migrants in Beijing, China. AIDS Education and Prevention, 25(6), 480–494. 10.1521/aeap.2013.25.6.480 [DOI] [PubMed] [Google Scholar]
- Yang W, Li D, Gao J, Zhou X, & Li F (2020). Decomposing differences in depressive symptoms between older rural-to-urban migrant workers and their counterparts in mainland China. BMC Public Health, 20(1), 1442. 10.1186/s12889-020-09374-1 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Zhong BL, Liu TB, Chan SSM, Jin D, Hu CY, Dai J, & Chiu HFK (2018). Common mental health problems in rural-to-urban migrant workers in Shenzhen, China: Prevalence and risk factors. Epidemiology and Psychiatric Sciences, 27(3), 256–265. 10.1017/s2045796016001141 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Zhong B, Xu Y, Jin D, Zou X, & Liu T (2016). Prevalence and correlates of loneliness among Chinese service industry migrant workers: A cross-sectional survey. Medicine (Baltimore), 95(24), e3903. 10.1097/md.0000000000003903 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Zimmer-Gembeck MJ, & French J (2016). Associations of sexual subjectivity with global and sexual well-being: A new measure for young males and comparison to females. Archives of Sex Behavior, 45(2), 315–327. 10.1007/s10508-014-0387-y [DOI] [PubMed] [Google Scholar]