

Abstract
SARS-CoV-2 infections elicit antibodies against the viral spike (S) and nucleocapsid (N) proteins; COVID-19 vaccines against the S-protein only. The BCG-Corona trial, initiated in March 2020 in SARS-CoV-2-naïve Dutch healthcare workers, captured several epidemic peaks and the introduction of COVID-19 vaccines during the one-year follow-up. We assessed determinants of systemic anti-S1 and anti-N immunoglobulin type G (IgG) responses using trial data. Participants were randomised to BCG or placebo vaccination, reported daily symptoms, SARS-CoV-2 test results, and COVID-19 vaccinations, and donated blood for SARS-CoV-2 serology at two time points. In the 970 participants, anti-S1 geometric mean antibody concentrations (GMCs) were much higher than anti-N GMCs. Anti-S1 GMCs significantly increased with increasing number of immune events (SARS-CoV-2 infection or COVID-19 vaccination): 104.7 international units (IU)/mL, 955.0 IU/mL, and 2290.9 IU/mL for one, two, and three immune events, respectively (p < 0.001). In adjusted multivariable linear regression models, anti-S1 and anti-N log10 concentrations were significantly associated with infection severity, and anti-S1 log10 concentration with COVID-19 vaccine type/dose. In univariable models, anti-N log10 concentration was also significantly associated with acute infection duration, and severity and duration of individual symptoms. Antibody concentrations were not associated with long COVID or long-term loss of smell/taste.
Keywords: SARS-CoV-2, COVID-19, serology, infection, vaccination, BCG
1. Introduction
The systemic humoral immune response to SARS-CoV-2 is characterized by antigen-specific antibodies, which play a crucial role in host defence and protection against re-infection. Following an infection, systemic immunoglobulins type G (IgG) specific to SARS-CoV-2, including antibodies against the viral spike (S) and nucleocapsid (N) proteins, are detected in the majority of patients within two weeks, with peak concentrations at around three weeks after symptom onset [1,2,3,4]. While natural infection typically gives rise to both anti-S and anti-N antibodies, the COVID-19 vaccines that were authorized in the European Union within the first two years of the epidemic (mRNA [5,6] and viral vector vaccines [7,8]) were engineered to elicit an anti-S immune response only [3,9]. The presence of anti-S antibodies is a more sensitive and specific marker for the presence of a SARS-CoV-2 infection than the presence of anti-N antibodies [10,11], with a reported sensitivity of 91.3–97.1% (depending on infection severity) and specificity of 98.1% [12]. Anti-N sensitivities are estimated to be 85% for mild infections and 67% for asymptomatic infections, with a specificity of 97% (96–98%) [13].
The S-protein, containing the S1 subunit with the receptor binding domain, is abundant and readily accessible on the viral surface. Conversely, the N-protein resides within the core of the viral structure and is less exposed to the host immune system [3]. Furthermore, the N-protein is highly conserved among the different coronaviruses, including some common cold-causing coronaviruses that circulate widely, and existing immunity to anti-N is therefore present in most populations [14,15]. However, anti-N is the only biomarker currently available to detect recent natural infections in a vaccinated population [13].
Studies have suggested that antibody concentrations over time likely vary by numbers, types, and combinations of immune events (SARS-CoV-2 infections or COVID-19 vaccinations), disease severity, and other virus, host, and vaccine characteristics [16,17,18,19]. However, asymptomatic and very mild cases in relatively healthy hosts were under-represented in studies thus far, with most research focused on the broad WHO-defined mild, moderate, and severe infections [20]. We therefore used data from our previously published BCG-Corona trial in healthy healthcare workers [21] to assess systemic anti-S1 IgG and anti-N IgG responses at the end of the first year of the SARS-CoV-2 epidemic in The Netherlands. Previous BCG-Corona trial analyses found that baseline BCG vaccination did not reduce SARS-CoV-2 infection incidence, duration, or severity, nor SARS-CoV-2 antibody responses, in the first year after vaccination [21]. In this paper, our aim was to assess whether numbers, types, and combinations of immune events, SARS-CoV-2 infection severity and duration, and participant characteristics (including having received BCG or placebo vaccination at baseline) were associated with systemic SARS-CoV-2-specific antibody concentrations after one year of follow-up. The strengths of these analyses include coverage of the first year of the epidemic when participants were still immunologically naïve for SARS-CoV-2 and the completeness of the dataset. BCG-Corona study participants reported symptoms daily, and positive SARS-CoV-2 test results, healthcare seeking behaviour, and vaccinations weekly, and donated blood samples for serology twice in one year. This comprehensive data enabled us to characterize infections, including asymptomatic and very mild infections, in great detail.
2. Materials and Methods
2.1. Study Design and Participants
The BCG-Corona trial was a multi-centre, double-blind, placebo-controlled randomised trial. The study protocol was approved by the institutional review board of the University Medical Center Utrecht, The Netherlands, and, registered at clinicaltrials.gov (identifier: NCT04328441). The primary results of the trial have been published [21]. Healthcare workers from nine Dutch hospitals who were expected to be in direct contact with COVID-19 patients were vaccinated with BCG or placebo vaccine (1:1) during the first SARS-CoV-2 epidemic wave in March/April 2020 and followed up for about one year. The participating study sites were categorized into core hospitals (n = 3) that implemented on-site venepuncture sampling, and other hospitals (n = 6) that implemented at-home fingerprick sampling (full eligibility criteria and sampling procedures in Supplementary Material).
2.2. Data Collection and Seroconversion Periods
Participants were invited to donate a blood sample at two time points during follow-up. This divided the follow-up time into two potential seroconversion periods. The first seroconversion period started on the date of randomisation and continued until the date of the first sampling round, about three months (M3) following BCG/placebo vaccination for the core hospitals and about six months (M6) for the other hospitals. The second seroconversion period was between the first sampling round and the second sampling round, approximately 12 months (M12) after BCG/placebo vaccination for all hospitals. Total follow-up time for each participant was the number of days between randomisation and the date of M12 sampling. Baseline characteristics were entered into an online questionnaire by study staff at the time of randomisation (Research Online, Julius Center, UMC Utrecht, The Netherlands). Participants were instructed to report daily symptoms including their severity, using a smartphone diary application (Research Follow App, Your Research BV, Huizen, The Netherlands) as well as the dates and results of any SARS-CoV-2 test, any other healthcare-seeking behaviour, and any vaccination (Supplementary Methods).
2.3. COVID-19 Vaccinations
The COVID-19 vaccine roll-out in The Netherlands began on 6 January 2021, and the diary app was updated with weekly questions about the date(s) and types of COVID-19 vaccinations at this time. The COVID-19 vaccines available during the study period were the mRNA vaccines Spikevax (Moderna Biotech, Cambridge, MA, USA) and Comirnaty (Pfizer/BioNTech, New York, NY, USA), and the vector vaccines Vaxzevria (AstraZeneca AB, Sodertalje, Sweden) and Jcovden (Janssen Vaccines, Leiden, The Netherlands). By the time the M12 blood sampling was completed in June 2021, healthcare workers could have received zero, one, or two doses, of only one vaccine type.
2.4. Antibody Measurements
All systemic antibody testing was conducted by the Center for Immunology of Infections and Vaccines at the National Institute for Public Health and the Environment in Bilthoven, The Netherlands. In the first seroconversion period, prior to the start of the COVID-19 vaccination campaign, only anti-S1 IgG antibodies were assessed. At M12, both anti-S1 and anti-N IgG antibodies were assessed to enable differentiation between natural infections and vaccine-induced antibodies. Anti-S1 and anti-N concentrations were measured using an in-house magnetic immunoassay on a Luminex platform, with reported sensitivities of 91.3–97.1% and 67–85% (depending on infection severity) for anti-S1 and anti-N respectively, and specificities of 98.1% and 97%, respectively [12,13]. Anti-S1 and anti-N concentrations were measured simultaneously, if applicable. The concentrations were subsequently calibrated against the international standard for human anti-SARS-CoV-2 immunoglobulin (20/136 NIBSC standard [22]) and expressed as international units per mL (IU/mL) [13,23]. The threshold for seropositivity was set to 10.1 IU/mL for anti-S1 and 14.3 IU/mL for anti-N. Samples that were below these thresholds were considered to have concentrations of zero. The anti-S1 and anti-N concentrations displayed gamma distributions and were log10 transformed after adding a pseudocount of +1 to each value to eliminate zero values (Figure S1). We focused the analyses on the M12 antibody concentrations, because most immune events took place between the first (M3/M6) and second (M12) sampling rounds.
2.5. Definitions of Antibody Concentration Determinants
A single immune event was defined as one SARS-CoV-2 infection episode or one dose of a COVID-19 vaccine. An infection episode was defined as a positive test (PCR or rapid antigen test) reported by the participant and/or evidence of seroconversion (for anti-S1 in the first seroconversion period and anti-S1 plus anti-N in the second seroconversion period). We also categorized participants by the vaccination types and doses that they received, and immunity type: natural immunity, vaccine immunity (after one or two doses), or hybrid immunity (a combination of natural infection and one or two vaccine doses).
To determine infection severity, we matched each infection episode with corresponding self-reported symptoms and healthcare-seeking behaviour information (Supplementary Methods). We subsequently categorized each infection episode in accordance with World Health Organisation (WHO) severity categories of asymptomatic, mild, moderate and severe [20]. However, only three BCG-Corona participants were hospitalized (WHO moderate category), and all other symptomatic episodes qualified as WHO mild. We therefore further subdivided the WHO mild category into very-mild and mild subcategories (Supplementary Methods): mild episodes were accompanied by more severe respiratory symptoms and/or fever, and lasted longer, compared to very mild episodes. The duration of the acute phase of the infection episode was defined as the number of consecutive days during which the participant reported symptoms, not including standalone loss of smell/taste. Long-term loss of smell/taste and long COVID (lingering symptoms other than standalone loss of smell/taste) were defined as continuing to report the respective symptoms for at least 60 days after the end of the acute infection episode. Duration of episodes that were ongoing at the end of follow-up were coded as unknown. Chronic symptoms that were reported regularly throughout follow-up were ignored.
2.6. Statistical Analyses
Statistical analyses were performed in R version 4.2.2 (PBC, Boston, MA, USA). Participants were excluded from the total-analysis population if they did not donate an M12 sample, their infection status was unsure, or their sample was taken in a seroconversion window after infection or vaccination. Infection status was considered unsure if a participant never reported a positive test but had completed less than 80% of diary entries, or had anti-N but no anti-S1 antibodies at M12. The seroconversion window was defined as 14 days, but sensitivity analyses were conducted using 7 and 0 days. Participants who were in the seroconversion window for the second dose of a COVID-19 vaccine were included as having received only one dose.
Characteristics between groups were compared using Chi-squared test for categorical variables and Wilcoxon rank sum test for continuous variables. The antilog 10x of mean concentrations was taken to obtain geometric mean concentrations (GMCs). Mean log10-transformed antibody concentrations between groups were compared using Kruskal–Wallis tests. Associations between covariates (with categorical variables analysed as indicator variables) and log10-transformed anti-S1 and anti-N concentrations at M12 were assessed using linear regression models. BCG-versus-placebo vaccination at baseline, age, and sex were forced into each multivariable model. Other covariates were considered for inclusion in multivariable models based on statistical significance in univariable linear regression, using p < 0.05 as the cut-off value. To avoid multicollinearity, we included combination variables for COVID-19 vaccination (number of doses received plus vaccine product if at least one dose received) and overall infection severity (whether an infection took place, and if so, its overall severity based on both symptom severity and duration), but not the number of immune events, overall acute infection episode duration, or severity/duration of individual symptoms.
3. Results
3.1. Participant Characteristics
Of the 1511 randomised participants (randomised population), 970 were selected for at least one of the analyses included in this paper (total-analysis population) (Figure 1). Baseline characteristics were comparable between the randomised population and the total-analysis population, and between the BCG and placebo groups within the total-analysis population (Table 1) [21]. The majority of the participants (74.7%) were female, with a mean age of 42.5 years (range 18–67), and had high (60%) to medium risk (24.7%) of work-related SARS-CoV-2 exposure (Supplementary Methods). The prevalence of chronic comorbidities other than hay fever was low. As expected, immune event-related characteristics during follow-up differed between the total analysis and randomised populations (Table 1) because application of the 14-day seroconversion window resulted in the removal of some immune events from the total-analysis population (Figure S2; Table S1).
Figure 1.

Population and study flow: Participants who did not have evidence of a SARS-CoV-2 infection and less than 80% diary app completion (n = 166) were excluded because the probability of having missed infections in that group is high. We also excluded participants with inconclusive serology at M12 (n = 36, seroconverted for anti-N but not anti-S1) and those who did not donate a blood sample at M12 (n = 206): 114 in the BCG group and 92 in the placebo group (p = 0.237). The four participants who reported more than one infection during follow-up (two infections in all cases) were excluded because that group was too small to generate meaningful results. In the main analyses, the seroconversion window was considered to be from 14 days before the M12 sampling date until the date of sampling; in sensitivity analyses, we also considered seroconversion windows of 7 and 0 days (Supplementary Methods and Results).
Table 1.
Participant baseline characteristics and immune events during follow-up.
|
Baseline Characteristics Cells contain n (% of N) unless stated otherwise |
Total-analysis population | Randomised population | ||||
|
Placebo
N = 480 |
BCG
N = 490 |
p 1,2 |
Overall
N = 970 |
Overall
N = 1511 |
p 1,3 | |
| Age in years, mean (SD) | 43.0 (12.6) | 42.0 (12.6) | 0.208 | 42.5 (12.6) | 42.0 (12.7) | 0.366 |
| Female | 355 (74.0) | 369 (72.3) | 0.683 | 724 (74.7) | 1122 (74.3) | 0.868 |
| Smoking status | 0.143 | 0.258 | ||||
| Current | 31 (6.5) | 34 (6.9) | 65 (6.7) | 123 (8.1) | ||
| Former | 136 (28.3) | 166 (33.9) | 302 (31.1) | 436 (28.9) | ||
| Never | 313 (65.2) | 290 (59.2) | 603 (62.2) | 952 (63.0) | ||
| Work-related exposure 4 | 0.936 | 0.492 | ||||
| Low | 72 (15.0) | 76 (15.5) | 148 (15.3) | 213 (14.1) | ||
| Medium | 121 (25.2) | 119 (24.3) | 240 (24.7) | 356 (23.6) | ||
| High | 287 (59.8) | 295 (60.2) | 582 (60.0) | 942 (62.3) | ||
| History of BCG vaccination | 83 (17.3) | 91 (18.6) | 0.663 | 174 (17.9) | 256 (16.9) | 0.559 |
| Past TB test results 5 | 0.135 | 0.491 | ||||
| Tested negative | 320 (66.7) | 320 (66.7) | 640 (66.0) | 1016 (67.2) | ||
| Tested positive | 49 (10.2) | 45 (9.2) | 94 (9.7) | 136 (9.0) | ||
| Never tested | 109 (22.7) | 115 (23.5) | 224 (23.1) | 347 (23.0) | ||
| Unknown | 2 (0.4) | 10 (2.0) | 12 (1.2) | 12 (0.8) | ||
| Respiratory infection in winter 2019–2020 | 0.310 | 0.748 | ||||
| No | 349 (72.7) | 364 (74.3) | 713 (73.5) | 1090 (72.1) | ||
| Yes, with fever | 35 (7.3) | 44 (9.0) | 79 (8.1) | 127 (8.4) | ||
| Yes, without fever | 96 (20.0) | 82 (16.7) | 178 (18.3) | 294 (19.5) | ||
| Influenza vaccination in winter 2020–2021 6 | 0.239 | <0.001 | ||||
| Yes | 273 (56.9) | 255 (52.0) | 528 (54.4) | 697 (46.1) | ||
| No | 142 (29.6) | 169 (34.5) | 311 (32.1) | 428 (28.3) | ||
| Missing | 65 (13.5) | 66 (13.5) | 131 (13.5) | 386 (25.5) | ||
| Influenza vaccination prior to follow-up | 278 (57.9) | 282 (57.6) | 0.960 | 560 (57.7) | 872 (57.7) | 1.000 |
| Any other vaccination in past year 7 | 51 (10.6) | 54 (11.0) | 0.924 | 105 (10.8) | 162 (10.7) | 0.988 |
| Current use of anti-hypertensive medication | 33 (6.9) | 28 (5.7) | 0.540 | 61 (6.3) | 99 (6.6) | 0.860 |
| History of cardiovascular disease | 14 (2.9) | 9 (1.8) | 0.371 | 23 (2.4) | 34 (2.3) | 0.953 |
| Current use of anti-diabetic medication | 2 (0.4) | 3 (0.6) | 1.000 | 5 (0.5) | 9 (0.6) | 1.000 |
| History of asthma | 35 (7.3) | 34 (6.9) | 0.929 | 69 (7.1) | 101 (6.7) | 0.740 |
| History of hay fever | 130 (27.1) | 158 (32.2) | 0.091 | 288 (29.7) | 441 (29.2) | 0.823 |
| History of other pulmonary disease | 12 (2.5) | 11 (2.2) | 0.960 | 23 (2.4) | 32 (2.1) | 0.781 |
| Any lung disease (previous three combined) | 154 (32.1) | 175 (35.7) | 0.260 | 329 (33.9) | 497 (32.9) | 0.628 |
|
Immune Events Cells contain n (% of N) unless stated otherwise |
Total-analysis population | Randomised population | ||||
|
Placebo
N = 480 |
BCG
N = 490 |
p 1,2 |
Overall
N = 970 |
Overall
N = 1511 |
p 1,3 | |
| Number of immune events 8 | 0.323 | <0.001 | ||||
| 0 | 218 (45.4) | 235 (48.0) | 453 (46.7) | 679 (46.0) | ||
| 1 | 93 (19.4) | 94 (19.2) | 187 (19.3) | 487 (33.0) | ||
| 2 | 127 (26.5) | 133 (27.1) | 260 (26.8) | 216 (14.6) | ||
| 3 | 42 (8.8) | 28 (5.7) | 70 (7.2) | 94 (6.4) | ||
| Immune event type | 0.614 | <0.001 | ||||
| None | 218 (45.4) | 235 (48.0) | 453 (46.7) | 680 (45.0) | ||
| Infection 9 | 62 (12.9) | 61 (12.4) | 123 (12.7) | 158 (10.5) | ||
| Vaccine 1 dose | 31 (6.5) | 33 (6.7) | 64 (6.6) | 177 (11.7) | ||
| Vaccine 2 doses | 112 (23.3) | 118 (24.1) | 230 (23.7) | 320 (21.2) | ||
| Infection + 1 dose | 15 (3.1) | 15 (3.1) | 30 (3.1) | 54 (3.6) | ||
| Infection + 2 doses | 42 (8.8) | 28 (5.7) | 70 (7.2) | 86 (5.7) | ||
| COVID-19 vaccine product and dose 10 | 0.148 | 0.002 | ||||
| None | 280 (58.3) | 296 (60.4) | 576 (59.4) | 868 (57.4) | ||
| mRNA 1 dose | 30 (6.2) | 25 (5.1) | 55 (5.7) | 125 (8.3) | ||
| mRNA 2 doses | 154 (32.1) | 146 (29.8) | 300 (30.9) | 416 (27.5) | ||
| Vector 1 dose | 13 (2.7) | 23 (4.7) | 36 (3.7) | 86 (5.7) | ||
| Vector 2 doses | 0 (0.0) | (0.0) | (0.0) | 7 (0.5) | ||
| Unknown 1 dose | 3 (0.6) | 0 (0.0) | 3 (0.3) | 9 (0.6) | ||
| Had SARS-CoV-2 infection during follow-up 11 | 119 (24.8) | 104 (21.2) | 0.214 | 223 (21.2) | 298 (19.7) | 0.109 |
| Infection severity 12 | 0.727 | 0.541 | ||||
| No infection | 361 (75.2) | 386 (78.8) | 747 (77.0) | 1213 (77.9) | ||
| Asymptomatic | 15 (3.1) | 18 (3.7) | 33 (3.4) | 42 (2.8) | ||
| Very Mild | 65 (13.5) | 55 (11.2) | 120 (12.4) | 163 (10.8) | ||
| Mild | 25 (5.2) | 19 (3.9) | 44 (4.5) | 61 (4.0) | ||
| Moderate | 1 (0.2) | 1 (0.2) | 2 (0.2) | 3 (0.2) | ||
| Unknown | 13 (2.7) | 11 (2.2) | 24 (2.5) | 29 (1.9) | ||
| Acute duration of infection 13 | 0.401 | 0.908 | ||||
| 0 days/no infection | 377 (78.5) | 405 (82.7) | 782 (80.6) | 1251 (82.8) | ||
| 0–1 weeks | 20 (4.2) | 9 (1.8) | 29 (3.0) | 44 (2.9) | ||
| 1–2 weeks | 22 (4.6) | 23 (4.7) | 45 (4.6) | 61 (4.0) | ||
| 2–3 weeks | 17 (3.5) | 15 (3.1) | 32 (3.3) | 42 (2.8) | ||
| 3–4 weeks | 9 (1.9) | 8 (1.6) | 17 (1.8) | 20 (1.3) | ||
| 4+ weeks | 10 (2.1) | 5 (1.0) | 15 (1.5) | 18 (1.2) | ||
| Lingering | 10 (2.1) | 12 (2.4) | 22 (2.3) | 34 (2.3) | ||
| Ongoing/UNK | 15 (3.1) | 13 (2.7) | 28 (2.9) | 41 (2.7) | ||
| Long COVID | 0.489 | 0.975 | ||||
| No | 106 (89.1) | 87 (83.7) | 193 (86.5) | 256 (85.9) | ||
| Yes | 8 (6.7) | 11 (10.6) | 19 (8.5) | 27 (5.0) | ||
| Unknown | 5 (4.2) | 6 (5.8) | 11 (4.9) | 15 (9.1) | ||
| Long-term loss of smell/taste | 0.208 | 0.711 | ||||
| No | 112 (94.1) | 99 (95.2) | 211 (94.6) | 278 (93.3) | ||
| Yes | 5 (4.2) | 1 (1.0) | 6 (2.7) | 12 (4.0) | ||
| Unknown | 2 (1.7) | 4 (3.8) | 6 (2.7) | 8 (2.7) | ||
Abbreviations: BCG = Bacillus Calmette–Guérin vaccine; M = month; SD = standard deviation; TB = tuberculosis. p-values in bold indicate p < 0.05. 1 Chi-squared tests for categorical variables and Wilcoxon rank sum test for continuous variables. 2 Statistical test comparing baseline characteristics between the BCG and placebo group in the total-analysis population. 3 Statistical test comparing baseline characteristics between the total analysis (N = 970) and randomised populations (N = 1511). 4 Work-related exposure is a combination of participants expected to work in a COVID-19 ward and the percentage of work hours with direct patient contact (Supplementary Methods). 5 Tuberculosis tests include the Mantoux and/or TB QuantiFERON tests. A person who tested positive could have tested positive on either or both tests. 6 Only the missing category is statistically significantly different for the randomised and total-analysis populations. 7 Includes DTaP-IPV, hepatitis A, hepatitis B, yellow fever, typhoid, rabies, mumps-measles-rubella, meningococcal, pneumococcal, Haemophilus influenza type B, Ebola, tick-borne encephalitis, human papillomavirus, and unknown. 8 An immune event is considered to be either one natural infection or one dose of a COVID-19 vaccine. 9 No-one in the total-analysis population, and four persons in the randomised population, experienced more than one infection (two each). 10 COVID-19 vaccines available in The Netherlands during the study period are listed in the methods. In addition, one person received an experimental mRNA vaccine by CureVac N.V. in a clinical trial setting. That vaccine was never marketed due to insufficient efficacy, but the person was included in the mRNA vaccines group. 11 A natural infection was defined as a reported positive test (by the participants through the diary app) or identified by serology (evidence of anti-S1 at sampling round 1 or both anti-S1 and anti-N at sampling round 2). None of the participants in the total-analysis population reported a positive PCR test prior to follow-up at baseline. 12 Participants with an unsure infection status at M12 (never reported a positive test and/or seropositive for anti-N but not anti-S1 at M12; n = 36) were considered as never having had an infection during follow-up in the randomised population and were removed from the total-analysis population. 13 Participants who never had an infection during follow-up are included in the 0 days/no infection category.
3.2. M12 Anti-S1 and Anti-N IgG GMCs by Immune Events
In the total-analysis population, the M12 anti-S1 and anti-N GMCs did not differ between the BCG and placebo groups (Table 2, Figure 2A,B), or after stratification by number of immune events or immunity type (Figure 3). About half of the participants (517; 53.3%) experienced an immune event during follow up: 187 (19.3%) experienced one, 260 (26.8%) two, and 70 (7.2%) three immune events (Table 1). About two-thirds (65.8%) of the participants who experienced one immune event had an infection and 34.2% received one dose of a COVID-19 vaccine; 11.5% of the participants who experienced two immune events had an infection and had received one dose of a COVID-19 vaccine, while 88.5% received two doses of a COVID-19 vaccine. All participants with three immune events had an infection and had received two doses of a COVID-19 vaccine. M12 anti-S1 GMCs were higher with increasing numbers of immune events: 104.7 IU/mL (standard deviation (SD) = 7.2) for one, 955.0 IU/mL (SD = 4.1) for two, and 2290.9 IU/mL (SD = 2.6) for three immune events (p < 0.001; Table 2, Figure 2C,E). The M12 anti-S1 GMC was higher after one COVID-19 vaccine dose compared to after one infection: 177.8 IU/mL (SD = 7.59) and 79.4 IU/mL (SD = 6.61), respectively (p = 0.010). The M12 anti-N GMC increased after infection but not after vaccination(s) as expected (Table 2, Figure 2D,F), and was lower than the anti-S1 GMC after infection: 26.3 IU/mL (SD = 4.5) compared to 79.4 IU/mL (SD = 6.6), respectively (p < 0.001). M12 anti-S1 and anti-N log10 concentrations by time since an immune event showed considerable inter-individual variability but not a general downward trend, suggesting the follow-up period was not long enough for antibody waning (Figure S3). Therefore, SARS-CoV-2 anti-S1 and anti-N GMCs were associated with the number and type of immune events experienced by an individual, but not with BCG vs. placebo vaccination.
Table 2.
M12 anti-S1 and anti-N geometric mean concentrations by number and type of immune events.
| Determinants Cells contain mean (SD) | M12 Anti-S1 | M12 Anti-N | ||||
|---|---|---|---|---|---|---|
| Log10 Conc (IU/mL) |
GMC 1 (IU/mL) |
p 2 | Log10 Conc (IU/mL) |
GMC 1 (IU/mL) |
p 2 | |
| Overall mean | 1.55 (1.39) | 35.48 (24.55) | 0.73 (0.52) | 5.37 (3.31) | ||
| Intervention | 0.431 | 0.096 | ||||
| BCG | 1.51 (1.36) | 32.36 (22.91) | 0.71 (0.53) | 5.13 (3.38) | ||
| Placebo | 1.59 (1.41) | 38.90 (25.70) | 0.75 (0.52) | 5.62 (3.31) | ||
| Number of immune events 3 | <0.001 | <0.001 | ||||
| 0 | 0.25 (0.32) | 1.78 (2.09) | 0.54 (0.28) | 3.47 (1.91) | ||
| 1 | 2.02 (0.86) | 104.71 (7.24) | 1.12 (0.70) | 13.18 (5.01) | ||
| 2 | 2.98 (0.61) | 954.99 (4.07) | 0.65 (0.47) | 4.47 (2.95) | ||
| 3 | 3.36 (0.42) | 2290.87 (2.63) | 1.28 (0.51) | 19.05 (3.23) | ||
| Immunity type | <0.001 | <0.001 | ||||
| None | 0.25 (0.32) | 1.78 (2.09) | 0.54 (0.28) | 3.47 (1.91) | ||
| Infection only 4 | 1.90 (0.82) | 79.43 (6.61) | 1.42 (0.65) | 26.30 (4.47) | ||
| Vaccine 1 dose | 2.25 (0.88) | 177.83 (7.59) | 0.53 (0.26) | 3.39 (1.82) | ||
| Vaccine 2 doses | 2.90 (0.54) | 794.33 (3.47) | 0.54 (0.26) | 3.47 (1.82) | ||
| Infection + 1 dose | 3.60 (0.73) | 3981.07 (5.37) | 1.50 (0.75) | 31.62 (5.62) | ||
| Infection + 2 doses | 3.36 (0.42) | 2290.87 (2.63) | 1.28 (0.51) | 19.05 (3.24) | ||
| COVID-19 vaccine product and dose 5 | <0.001 | 0.956 | ||||
| None | 0.25 (0.32) | 1.78 (2.09) | 0.54 (0.28) | 3.47 (1.91) | ||
| mRNA 1 dose | 2.67 (0.76) | 467.73 (5.75) | 0.56 (0.28) | 3.36 (1.91) | ||
| mRNA 2 doses | 2.90 (0.54) | 794.33 (3.47) | 0.54 (0.26) | 3.47 (1.82) | ||
| Vector 1 dose | 1.80 (0.70) | 63.10 (5.01) | 0.51 (0.23) | 3.24 (1.70) | ||
| Infection severity 6 | 0.566 | 0.002 | ||||
| Asymptomatic | 2.54 (0.90) | 346.74 (7.94) | 1.14 (0.49) | 13.80 (3.09) | ||
| Very mild | 2.52 (1.03) | 331.13 (10.72) | 1.36 (0.66) | 22.91 (4.57) | ||
| Mild | 2.67 (1.13) | 467.73 (13.49) | 1.65 (0.52) | 44.67 (3.31) | ||
| Moderate | 3.36 (0.56) | 2290.87 (3.63) | 1.66 (1.41) | 45.71 (25.70) | ||
| Acute-episode duration 7 | 0.755 | 0.128 | ||||
| 0 days/no infection | 2.53 (0.92) | 33.84 (8.32) | 1.13 (0.48) | 13.49 (3.02) | ||
| 0–1 weeks | 2.45 (1.11) | 281.84 (12.88) | 1.37 (0.65) | 23.44 (4.47) | ||
| 1–2 weeks | 2.49 (1.04) | 309.03 (10.96) | 1.32 (0.64) | 20.89 (4.37) | ||
| 2–3 weeks | 2.80 (0.91) | 630.96 (8.13) | 1.56 (0.69) | 36.31 (4.90) | ||
| 3–4 weeks | 2.38 (0.97) | 239.88 (9.33) | 1.37 (0.67) | 23.44 (4.68) | ||
| 4+ weeks | 2.61 (1.28) | 407.38 (19.05) | 1.57 (0.53) | 37.15 (3.39) | ||
| Lingering | 2.80 (1.07) | 630.96 (11.75) | 1.49 (0.62) | 30.90 (4.17) | ||
| Ongoing/UNK | 2.63 (1.22) | 426.58 (16.60) | 1.46 (0.66) | 28.84 (4.57) | ||
| Long COVID 7,8 | 0.973 | 0.194 | ||||
| No | 2.59 (1.03) | 389.05 (10.72) | 1.36 (0.63) | 22.91 (4.27) | ||
| Yes | 2.57 (1.25) | 371.54 (17.78) | 1.53 (0.66) | 33.88 (4.57) | ||
| Unknown | 2.55 (1.07) | 354.81 (11.75) | 1.63 (0.54) | 42.66 (3.47) | ||
| Long-term loss taste/smell 7,9 | 0.572 | 0.541 | ||||
| No | 2.57 (1.04) | 371.54 (10.96) | 1.38 (0.63) | 23.99 (4.27) | ||
| Yes | 3.06 (1.11) | 1148.15 (12.88) | 1.30 (0.49) | 19.95 (3.09) | ||
| Unknown | 2.56 (1.25) | 363.08 (17.78) | 1.62 (0.74) | 41.69 (5.50) | ||
| Dyspnoea severity 10,11 | 0.938 | 0.239 | ||||
| 0 | 2.57 (1.07) | 371.54 (11.75) | 1.35 (0.61) | 22.39 (4.07) | ||
| 1–3 | 2.63 (0.99) | 426.58 (9.77) | 1.42 (0.68) | 26.30 (4.79) | ||
| 4–5 | 2.55 (0.99) | 354.81 (9.77) | 1.54 (0.60) | 34.67 (3.98) | ||
| Dyspnoea duration (days) 11 | 0.373 | 0.280 | ||||
| 0 | 2.59 (1.08) | 389.05 (12.02) | 1.36 (0.62) | 22.91 (4.17) | ||
| 1–3 | 2.72 (0.94) | 524.81 (8.71) | 1.28 (0.58) | 19.05 (3.80) | ||
| 4–7 | 2.32 (0.96) | 208.93 (9.12) | 1.38 (0.73) | 23.99 (5.37) | ||
| Week+ | 2.84 (0.94) | 691.83 (8.71) | 1.62 (0.54) | 41.69 (3.47) | ||
| Resp. symptoms severity 10,12,13 | 0.240 | 0.003 | ||||
| 0 | 2.48 (0.97) | 302.00 (9.33) | 1.12 (0.55) | 13.18 (3.55) | ||
| 1–3 | 2.42 (1.11) | 263.03 (12.88) | 1.38 (0.65) | 23.99 (4.47) | ||
| 4–5 | 2.73 (0.97) | 537.03 (9.33) | 1.54 (0.61) | 34.67 (4.07) | ||
| Resp. symptoms duration (days) 12,14 | 0.641 | 0.006 | ||||
| 0 | 2.46 (0.96) | 288.40 (9.12) | 1.12 (0.55) | 13.18 (3.55) | ||
| 1–3 | 2.56 (1.13) | 363.08 (13.49) | 1.42 (0.62) | 26.30 (4.17) | ||
| 4–7 | 2.37 (1.15) | 234.42 (14.13) | 1.29 (0.68) | 19.50 (4.79) | ||
| Week+ | 2.65 (1.02) | 446.68 (10.47) | 1.52 (0.62) | 33.11 (4.17) | ||
| Fever 10,15 | 0.845 | 0.029 | ||||
| No | 2.57 (1.06) | 371.54 (11.48) | 1.31 (0.61) | 20.42 (4.07) | ||
| Yes | 2.60 (1.01) | 398.11 (10.23) | 1.50 (0.63) | 31.62 (4.27) | ||
| Fever duration (days) 10,15 | 0.781 | 0.024 | ||||
| 0 | 2.57 (1.06) | 371.54 (11.48) | 1.31 (0.61) | 20.42 (4.07) | ||
| 1–3 | 2.63 (1.09) | 426.58 (12.03) | 1.29 (0.53) | 19.50 (3.39) | ||
| 4–7 | 2.48 (0.93) | 302.00 (8.51) | 1.51 (0.68) | 32.36 (4.79) | ||
| Week+ | 2.74 (1.07) | 549.54 (11.75) | 1.69 (0.60) | 48.98 (3.98) | ||
| Non-resp. symptoms severity 10,16,17 | 0.225 | 0.002 | ||||
| 0 | 2.35 (1.07) | 223.87 (11.75) | 1.13 (0.54) | 13.48 (3.47) | ||
| 1–3 | 2.73 (0.95) | 537.03 (8.91) | 1.38 (0.59) | 23.99 (3.89) | ||
| 4–5 | 2.55 (1.05) | 354.81 (11.22) | 1.50 (0.65) | 31.62 (4.47) | ||
Abbreviations: BCG = Bacillus Calmette–Guerin; conc = concentration; GMC = geometric mean concentration; IU = international units; M = month; resp = respiratory; SD = standard deviation. p-values in bold indicate p < 0.05. 1 Antilog 10x of the log10-transformed mean concentration. 2 Kruskal–Wallis p-values for comparisons of mean log10-transformed concentrations in IU/mL after adding a pseudocount of 1. 3 One immune event (N = 187): 123 (65.8%) had an infection and 64 (34.2%) received one dose of a COVID-19 vaccine. Two immune events (N = 260): 30 (11.5%) had an infection and received one dose of a COVID-19 vaccine, while 230 (88.5%) received two doses of a COVID-19 vaccine. All participants with three immune events (N = 70) had an infection and received two COVID-19 vaccine doses. 4 No-one in this dataset experienced more than one infection. 5 Denominator is 747 because participants with infections were excluded as well as an additional participant, due to missing vaccine type. The number of COVID-19 vaccine doses was calculated as the total number of doses received by the participant during follow-up, regardless of whether the primary vaccination series consisted of one or two doses. The COVID-19 vaccines available during the study period in The Netherlands are listed in the methods. 6 Denominator is 199 because only participants who experienced an infection were included and 24 participants with unknown infection severity were removed. We also performed Jonckheere’s tests for trend with an a priori ordering of infection severity for mean anti-S1 log10-transformed concentrations (p-value = 0.367) and mean anti-N log10-transformed concentrations (p-value < 0.001). 7 Denominator is 223 because only participants who experienced an infection were included. 8 Long COVID was defined as continuing to report symptoms other than standalone loss of smell/taste for at least 60 days after the end of the acute infection episode. “Unknown” includes participants who were reporting symptoms past the end of the acute infection episode but had not yet reached 60 days at the time the diary app was discontinued. There were 23 cases but 4 were excluded from the total-analysis population for being in the seroconversion window of the first COVID-19 vaccine dose. Of the remaining 19 cases, 5 had the infection in the first period and 14 in the second period; 8 received at least one COVID-19 vaccine dose in the first period and 11 were never vaccinated. 9 Long-term loss of smell/taste was defined as continuing to report standalone loss of smell/taste for at least 60 days after the end of the acute infection episode. “Unknown” includes participants who were reporting loss of smell/taste past the end of the acute infection episode but had not reached 60 days at the time the diary app was discontinued. There were nine cases but three were excluded from the total-analysis population for being in the seroconversion window of the first COVID-19 vaccine dose. When excluding the unknown category from the analysis, p = 0.290. 10 Symptoms were reported on a scale of 0–5: 0 for not present and 1–5 for present, with increasing severity. Fever was reported as present or not and was defined as having a temperature above 38 °C. 11 Denominator is 218 because only participants who experienced an infection were included and five additional participants were removed due to unknown dyspnoea severity and/or duration. 12 Respiratory symptoms exclude dyspnoea. Most participants reported more than one type of respiratory symptom during an infection episode; we took the highest severity reported for any respiratory symptom. The duration was calculated from the day on which the first respiratory symptom was reported until the day a respiratory symptom was reported. 13 Denominator is 205 because only participants who experienced an infection were included and 18 additional participants were removed due to unknown respiratory symptom severity. 14 Denominator is 200 because only participants who experienced an infection were included and 23 additional participants were removed due to unknown or ongoing respiratory-symptom duration. 15 Denominator is 217 because only participants who experienced an infection were included and six additional participants were removed due to unknown presence of fever or unknown fever duration. 16 Non-respiratory symptoms exclude fever. Most participants reported more than one type of non-respiratory symptom during an infection episode; we took the highest severity reported for any non-respiratory symptom. The duration was calculated from the day on which the first non-respiratory symptom was reported until the last day a non-respiratory symptom was reported. 17 Denominator is 205 because only participants who experienced an infection were included and 18 additional participants were removed due to unknown non-respiratory symptom severity.
Figure 2.


M12 anti-S1 and anti-N log10 concentrations by number and type of immune events. Abbreviations: BCG = Bacillus Calmette–Guérin vaccine; Inf = infection; Inf + Vac1 = infection and one dose of a COVID-19 vaccine; Inf + Vac2 = infection and two doses of a COVID-19 vaccine; Vac1 = one dose of a COVID-19 vaccine; Vac2 = two doses of a COVID-19 vaccine. Kruskal–Wallis for overall statistical testing of mean log10-transformed M12 antibody concentrations and Wilcoxon sum rank test for within group: ns: non-significant; *: p <= 0.05, **: p <= 0.01, ***: p <= 0.001; ****: p <= 0.0001. (A,B): Total-analysis population: denominator N = 970. The green point range indicates the mean and standard deviation. (C–F): Total-analysis population: denominator N = 970. The point range shows the mean and standard deviation. (G–I): Participants with an infection were excluded; denominator N = 747. (J–M): Only participants with an infection included: denominator N = 199; 24/223 participants with unknown severity were excluded. The point range indicates the mean and standard deviation.
Figure 3.

M12 anti-S1 and anti-N log10 concentrations for BCG vs. placebo stratified by number of immune events. Abbreviations: Inf = infection; Inf + Vac1 = infection and one dose of a COVID vaccine; Inf + Vac2 = infection and two doses of a COVID vaccine; Vac1 = one dose of a COVID vaccine; Vac2 = two doses of a COVID vaccine. Systemic antibody concentrations were log10-transformed (after adding a pseudocount of 1). An immune event was defined as one SARS-CoV-2 infection or one dose of a COVID-19 vaccine. The blue point range indicates the mean and standard deviation of the log10 concentrations. Statistical testing (****) shows the significance for within-group comparisons. All statistical testing between BCG and placebo groups were non-significant. ns: non-significant, *: p <= 0.05, **: p <= 0.01, ***: p <= 0.001, ****: p <= 0.0001.
3.3. M12 Anti-S1 and Anti-N IgG GMCs by COVID-19 Vaccinations
Of the 394/970 (40.6%) participants who received COVID-19 vaccination during follow-up, 94/970 (9.7%) received one dose and 300/970 (30.9%) received two doses. The majority (355/394; 90.1%) received an mRNA vaccine (305 Comirnaty, 49 Spikevax, and one an experimental vaccine by CureVac N.V. in a clinical trial setting), 36/394 (9.1%) received a viral vector vaccine (32 Vaxzevria and 4 Jcovden), and for three (0.8%) information on the vaccine type was missing (Table 1). It should be noted that all participants who received two vaccine doses received mRNA vaccines, while those who received one dose received either a first dose of an mRNA vaccine (58.5%), or a first or only dose of a vector vaccine (38.3%) or of an unknown vaccine type (3.2%). When excluding all participants who experienced an infection, M12 anti-S1 GMCs were significantly higher in participants who had received one dose of an mRNA vaccine (467.7 IU/mL; SD = 5.8) compared to one dose of a viral vector vaccine (63.1 IU/mL; SD = 5.0; p < 0.001; Table 2, Figure 2G–I). Two doses of an mRNA vaccine resulted in a higher anti-S1 GMC than one (Table 2). M12 anti-S1 concentrations were higher in the Spikevax compared to the Comirnaty group; 562.3 IU/mL (SD = 5.6) and 120.2 IU/mL (SD = 4.6) for a single dose of Spikevax and Comirnaty, respectively (p = 0.165), and 1230.2 IU/mL (SD = 2.1) and 794.33 IU/mL (SD = 3.5) for two doses of Spikevax and Comirnaty, respectively (p = 0.583; Table S2). M12 anti-S1 GMCs were highest in participants who had an infection and also received one or two COVID-19 vaccinations: 3981.07 IU/mL (SD = 5.37) and 2290.87 IU/mL (SD = 2.63), respectively (Table 2). Overall, receiving the mRNA vaccines elicited higher anti-S1 responses compared to the viral vector vaccines, while the combination of an infection plus vaccination(s) resulted in the largest anti-S1 response.
Eight participants were above the threshold for anti-S1 seropositivity but negative for anti-N at M12 and never reported a SARS-CoV-2 infection or COVID-19 vaccination. Three of them had high anti-S1 concentrations, while five had concentrations near the threshold. These participants most likely failed to report a COVID-19 vaccination, or experienced a very mild/asymptomatic infection that did not elicit an anti-N response, respectively. Additionally, three participants received two doses of a COVID-19 vaccine but had failed to develop anti-S1 antibodies by M12.
3.4. M12 Anti-S1 and Anti-N IgG GMCs by SARS-CoV-2 Infections
A total of 223 first infections occurred in the total-analysis population during follow-up: 33 (14.8%) were asymptomatic, 120 (53.8%) very mild, 44 (19.7%) mild, 2 (0.90%) moderate, and 24 (10.8%) of unknown severity. Among those who experienced an infection during follow-up, 30/223 (13.5%) received one COVID-19 vaccine dose and 70/223 (31.4%) received two doses. The M12 anti-S1 GMCs did not statistically significantly differ by overall infection severity when analysed as an ordinal variable (p = 0.566), and this remained the case after stratifying by the number of COVID-19 vaccine doses received (Table 2, Figure 2J,K). In contrast, the M12 anti-N GMCs significantly increased with increasing overall infection severity: 13.8 IU/mL (SD = 3.1) for asymptomatic, 22.9 IU/mL (SD = 4.6) for very mild, 44.7 IU/mL (SD = 3.3) for mild, and 45.7 IU/mL (SD = 25.7) for moderate infection (p = 0.002; Table 2, Figure 2L,M). The M12 anti-S1 and anti-N GMCs were not associated with increasing acute-episode duration, long COVID or long-term loss of smell/taste (Table 2, Figure S4A–F). M12 anti-S1 GMCs were not associated with the severity or duration of specific individual symptoms (analysed as ordinal variables), either. In contrast, M12 anti-N GMCs were higher, with higher severity and longer duration of respiratory symptoms excluding dyspnoea, with the presence and duration of fever, and with the severity of non-respiratory symptoms other than fever (Table 2, Figure S4G–T). Of note, the severity and duration of dyspnoea were not associated with either M12 anti-S1 or M12 anti-N GMCs (Table 2, Figure S4G–J). Therefore, overall infection severity, as well as severity and duration of specific symptoms, were associated with anti-N GMCs but not with anti-S1 GMCs.
The M12 anti-S1 and anti-N GMCs of participants who experienced an infection were correlated at the individual level: participants with a higher M12 anti-S1 GMC also had a higher M12 anti-N GMC (Figure S5). This correlation was most pronounced for those who never received a COVID-19 vaccine during follow-up (Spearman’s ρ = 0.69; p < 0.001) and weakened in participants who had received one (ρ = 0.54; p = 0.003) or two vaccinations (ρ = 0.32; p = 0.006) which boosted anti-S1 GMCs only.
3.5. Linear Regression Models of M12 Anti-S1 and Anti-N Concentrations
In univariable models including the total-analysis population (N = 970), the number of immune events, immune event type, overall infection severity (analysed as an indicator variable), and work-related exposure risk were statistically significantly associated with both M12 anti-S1 and anti-N log10 concentrations (Table S3A). Vaccine doses and types (combined into one variable) were only associated with M12 anti-S1 log10 concentration, while hypertensive medication use and history of pulmonary disease other than asthma and hay fever were only associated with M12 anti-N log10 concentrations. BCG/placebo vaccination at baseline, age, sex, smoking, history of BCG vaccination, influenza vaccination during follow-up, recent respiratory tract infections, and the comorbidities that were not already mentioned were not associated with M12 anti-S1 or anti-N log10 concentrations (Table S3A). In univariable subgroup analyses limited to participants who experienced an infection (n = 223), overall infection severity, overall acute-episode duration, and specific symptom severity and duration, with the exception of dyspnoea, were significantly associated with M12 anti-N log10 concentrations (all as indicator variables; Table S3B). Long COVID and long-term loss of smell/taste were not associated with M12 anti-S1 or anti-N log10 concentrations in individuals who had experienced an infection.
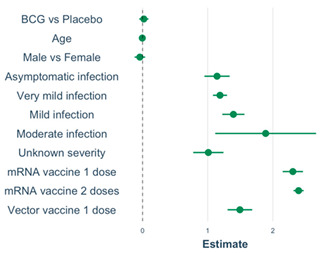
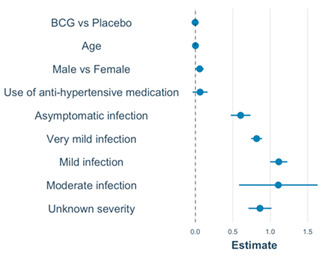
The final multivariable models with M12 anti-S1 or anti-N log10 concentrations as the outcomes and BCG/placebo vaccination at baseline, age, and sex forced into the models are shown in Table 3. Age, vaccine-type plus dose (indicator variable), and overall infection severity (indicator variable) were statistically significantly associated with M12 anti-S1 log10 concentration. Sex and overall infection severity (indicator variable) were associated with M12 anti-N log10 concentration. Current use of hypertensive medication was associated with M12 anti-N log10 concentration in univariable analysis but was no longer significant in the multivariable model. Sensitivity analyses adding more covariates (Figure S6), or reducing the seroconversion windows to 7 and 0 days (Table S4), produced similar results with two exceptions. The positive associations between M12 anti-S1 log10 concentration and mild- or moderate-infection severity (compared to no infection) and having received one dose of an mRNA or vector vaccine (compared to no vaccination) changed in magnitude, but remained statistically significant, when the seroconversion period was reduced to 7 or 0 days (Table S4; Supplementary Results). To summarise, in our multivariable linear models, overall infection severity was associated with M12 anti-S1 log10 concentration in the total-analysis population, and with COVID-19 vaccine doses and types. Only infection severity was associated with M12 anti-N log10 concentration. BCG vs. placebo vaccination was not associated with M12 log10 antibody concentration.
Table 3.
Multivariable models with M12 anti-S1 and anti-N log10 concentrations as outcome.
| Model: M12 Anti-S1 6,7 | Covariate | Estimate (95% CI) | Exp 4 (Estimate) (95% CI) | p | VIF 5 | |
| Model intercept 1 | 0.50; (0.36, 0.64) | 3.02; (2.19, 4.17) | <0.001 |
|
||
| BCG vs. placebo 2 | 0.02; (−0.05, 0.09) | 1.05; (0.89, 1.23) | 0.585 | 1.01 | ||
| Age (per year) | −0.004; (−0.01, −0.007) | 0.99; (0.98, 0.99) | 0.008 | 1.04 | ||
| Male sex | −0.04; (−0.12, 0.04) | 0.91; (0.76, 1.10) | 0.311 | 1.01 | ||
| All the below compared to participants who never had an infection or vaccination during follow-up: | ||||||
| Asymptomatic | 1.14; (0.95, 1.34) | 14.13; (8.91, 21.88) | <0.001 | 1.01 | ||
| Very mild | 1.19; (1.08, 1.30) | 16.22; (12.59, 20.42) | <0.001 | 1.02 | ||
| Mild | 1.39; (1.22, 1.56) | 25.12; (16.98, 38.02) | <0.001 | 1.02 | ||
| Moderate | 1.89 (1.12, 2.66) | 74.13; (12.30, 446.68) | <0.001 | 1.01 | ||
| Unknown severity | 1.01; (0.78, 1.24) | 10.96; (6.46, 18.62) | <0.001 | 1.02 | ||
| mRNA 1 dose | 2.31; (2.15, 2.46) | 112.20; (47.86, 263.03) | <0.001 | 1.06 | ||
| mRNA 2 doses | 2.40; (2.32, 2.47) | 245.47; (204.17, 295.12) | <0.001 | 1.06 | ||
| Vector 1 dose | 1.49; (1.31, 1.68) | 223.87; (151.36, 331.13) | <0.001 | 1.06 | ||
| Model : M12 Anti-N 8,9 | Covariate | Estimate (95% CI) | Exp 4 (estimate) | p | VIF 5 | |
| Model intercept 3 | 0.48; (0.39, 0.57) | 2.95; (2.40, 3.63) | <0.001 |
|
||
| BCG vs. placebo 2 | −0.003; (−0.05, 0.04) | 0.99; (0.89, 1.10) | 0.901 | 1.01 | ||
| Age (per year) | 0.001; (−0.007, 0.003) | 1.00; (0.98, 1.01) | 0.312 | 1.06 | ||
| Male sex | 0.06; (0.005, 0.11) | 1.15; (1.01, 1.29) | 0.040 | 1.01 | ||
| Hypertension med | 0.06; (−0.04, 0.16) | 1.15; (0.91, 1.44) | 0.222 | 1.07 | ||
| All the below compared to participants who never had an infection or vaccination during follow-up: | ||||||
| Asymptomatic | 0.60; (0.47, 0.74) | 4.07; (2.95, 5.50) | <0.001 | 1.01 | ||
| Very mild | 0.82; (0.74, 0.89) | 6.61; (5.62, 7.94) | <0.001 | 1.04 | ||
| Mild | 1.11; (1.00, 1.23) | 13.18; (10.0, 16.98) | <0.001 | 1.01 | ||
| Moderate | 1.11; (0.58, 1.63) | 13.48; (4.07, 45.71) | <0.001 | 1.01 | ||
| Unknown severity | 0.86; (0.71, 1.02) | 7.24; (5.13, 10.23) | <0.001 | 1.01 | ||
Abbreviations: BCG = Bacillus Calmette–Guérin vaccine; CI = confidence interval; M = month; VIF = variance of inflation factor. Indicator variables were created, and model building is described in more detail in Supplementary Methods. p-values in bold indicate p < 0.05. 1 The reference is an individual in the placebo group, zero years old, who never had a SARS-CoV2 infection and was never vaccinated for COVID-19. 2 Baseline BCG or placebo vaccination was forced into the models to take the original randomisation into account. Age and sex were forced into the models because of their well-documented effects on immune responses. 3 The reference is a female individual in the placebo group, zero years old, who never experienced a SARS-CoV-2 infection. 4 Antilog 10x of the model estimates. 5 The VIF values for this model are all less than 5, which means that there was no evidence of multicollinearity. 6 The model includes N = 967 participants (three participants with unknown vaccine types dropped out of the model). 7 Therefore, the linear equation is Log10(anti-S1 concentration M12) = 0.50 + 0.02 × BCG + 1.14 × Asymptomatic infection + 1.19 × Very mild infection + 1.39 × Mild infection + 1.89 × Moderate infection + 1.01 × infection with unknown severity + 2.31 × One dose of mRNA + 2.40 × Two doses of mRNA + 1.49×One dose of vector − 0.004 × per year of age −0.04 × Male. 8 The model includes N = 970 participants. 9 Therefore, the linear equation is Log10(anti-N concentration M12) = 0.48 − 0.003 × BCG + 0.60 × Asymptomatic Infection + 0.82 × Very mild infection + 1.11 × Mild infection + 1.11 × Moderate infection + 0.86 × Infection with unknown severity + 0.06 × Male + 0.001×per year of age + 0.06 × Use of anti-hypertensive medication.
4. Discussion
SARS-CoV-2 anti-S1 and anti-N GMCs approximately one year after the start of the Dutch SARS-CoV-2 epidemic were associated with the number of immune events and overall infection severity when an infection took place, but not with having had or having long COVID or long-term loss of smell/taste. Anti-S1 GMCs were also associated with COVID-19 vaccination, and anti-N GMCs with specific symptom severity and duration, except for dyspnoea. Anti-S1 GMCs were higher after one vaccination than after one infection, and after one mRNA than one vector vaccination, and highest after a combination of infection and vaccination(s).
Our finding of higher anti-S1 GMCs with an increasing number of immune events, and after vaccination with mRNA compared to vector vaccines, is in agreement with the published literature [24,25,26]. However, published reports for infection versus vaccination are inconsistent [27]. Important variables in that context are the severity and duration of infections, waning antibody concentrations over time, and the timing of boosting events. We were able to investigate the former, but not the latter. We did not detect a downward trend in antibody GMCs by time period between the last immune event and M12 sampling, but we could not evaluate antibody concentrations longitudinally for individual participants due to the low number of immune events in the first seroconversion period. The COVID-19 vaccination campaign in The Netherlands began eight months after the start of the study and SARS-CoV-2 infections took place throughout follow-up. Our finding of higher anti-S1 GMC after one vaccination than after one infection could therefore be explained by the timing of immune events and subsequent waning antibody concentrations over time. However, the follow-up time was short, with little opportunity for waning, and our findings were robust after applying seroconversion windows of 14, 7 or 0 days. Another potential explanation is lower antigen exposure during a mild infection than after vaccination. Participants with hybrid immunity due to infection plus vaccination(s) had higher anti-S1 GMCs than those with infection or vaccination (one or two doses) immunity only. This is also in agreement with the published literature [26,28,29]. Studies have shown that within the hybrid immunity group, concentrations depend on the type(s) of vaccine(s) used, the number of doses, and the severity of the infection [29,30,31].
As we had already shown earlier, BCG vaccination administered at the beginning of the study did not influence SARS-CoV-2 specific antibody concentrations approximately one year later. This is in agreement with most other BCG trials conducted during the COVID-19 epidemic, which failed to demonstrate benefits of BCG vaccination on COVID-19-related endpoints [21,32,33].
Overall infection severity was associated with M12 anti-S1 (when analysed as an indicator variable but not as an ordinal variable) and anti-N GMCs (when analysed as an indicator or ordinal variable), and individual symptom severity and durations with M12 anti-N GMCs only. However, the latter associations did show non-statistical trends in the same direction for M12 anti-S1 GMCs. The somewhat inconsistent findings for higher M12 anti-S1 GMCs with increasing infection severity could be explained by the fact that this increase was non-linear, with GMCs starting out higher than anti-N GMCs (likely because the host immune system is highly exposed to the viral S1-protein and less so to the N-protein) [3], and reaches a plateau more easily. Several other studies have reported increasing anti-S1 and anti-N antibody concentrations with increasing infection severity [1,16,34], but some studies did not find this association [35,36]. Many of these studies, however, compared WHO-defined mild, moderate and severe infections (with the latter two requiring hospitalisation). Our study was conducted in a generally healthy population below the age of 65, and the detailed and comprehensive diary data allowed us to also include asymptomatic infections and to subdivide the WHO-defined mild category into very-mild and mild subcategories. Even within this range of asymptomatic-to-mild infections, differences in impact on antibody responses were measurable.
Our analyses did not reveal associations between M12 antibody concentrations and having had or having long COVID or long-term loss of smell/taste, but the total-analysis population included only 19 long COVID cases. Several other studies reported weaker SARS-CoV-2-specific antibody responses following an infection in long COVID cases [37,38,39]. However, one study reported similar anti-S1 and anti-N concentrations between fully recovered and long COVID patients after infection, but aberrant immune responses in long COVID patients following COVID-19 vaccination [40]. The potential associations between immune responses and development of long COVID requires further study.
The main strengths of the study were that we captured the entire first year of the Dutch COVID-19 epidemic and had detailed and comprehensive data, allowing us to identify asymptomatic infections and to subdivide WHO mild infections into very-mild and mild. A main limitation was that we could not account for antibody waning at the individual participant level, but we think that follow-up time after most immune events was too short for waning to have influenced results significantly. Other limitations include the use of two different blood sampling methods (venepuncture and fingerprick sampling) and the suboptimal sensitivity of the anti-N assay for detecting asymptomatic infections (67%) [12]. We may, therefore, have missed some asymptomatic infections and overestimated the M12 anti-N GMC in the asymptomatic group.
5. Conclusions
Our study confirmed that anti-S1 and anti-N GMCs were associated with overall infection severity, but, additionally, showed that this was the case even in infections ranging from asymptomatic to mild in an otherwise healthy population. Anti-S1 GMCs were also associated with numbers and types of COVID-19 vaccinations, with the combination of infection and vaccination(s) eliciting the greatest response. Anti-S1 and anti-N GMCs were not associated with having had or having long COVID or long-term loss of smell/taste.
Acknowledgments
We thank the healthcare workers for their participation, and colleagues in the UMC Utrecht and participating hospitals and laboratories who implemented the BCG-Corona trial during the Dutch COVID-19 epidemic.
Supplementary Materials
The following supporting information can be downloaded at: https://www.mdpi.com/article/10.3390/vaccines12060691/s1 References [41,42,43,44,45] are in supplementary materials only.
Author Contributions
Conceptualization, J.H.H.M.v.d.W., T.t.D., M.J.M.B. and M.G.N.; data curation, J.C. and J.H.H.M.v.d.W.; formal analysis, J.C.; funding acquisition, J.H.H.M.v.d.W., T.t.D., M.J.M.B. and M.G.N.; investigation, J.H.H.M.v.d.W., J.C., T.t.D., E.T. and P.A.D.; methodology, J.C. and J.H.H.M.v.d.W.; resources, G.S., R.v.B., F.v.d.K., L.M.V. and M.I.d.J.; software, J.C.; supervision, J.H.H.M.v.d.W. and T.t.D.; visualization, J.C.; writing—original draft, J.C.; writing—review and editing, J.H.H.M.v.d.W., T.t.D., E.T., P.A.D., G.S., R.v.B., F.v.d.K., L.M.V., M.I.d.J., M.J.M.B., and M.G.N. All authors have read and agreed to the published version of the manuscript.
Institutional Review Board Statement
The study protocol was approved by the institutional review board of the University Medical Center Utrecht, The Netherlands on 17 March 2020 (protocol number 20-139/G-M), and, registered at clinicaltrials.gov (identifier: NCT04328441).
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Data Availability Statement
Individual participant data that underlie the results reported in this article will be made available after de-identification to investigators whose proposed use of the data has been approved by an independent review committee for up to 5 years following publication. The study protocol will be available to anyone during this same time frame. Information regarding submitting proposals and accessing data may be found on https://dataverse.nl/, accessed on 19 June 2024.
Conflicts of Interest
L.M.V. reports consulting fees from MSD in the last 36 months (unrelated to the work in this manuscript, payments to institution). M.J.M.B. reports research grants from Janssen Vaccines, Novartis, CureVac, and Merck, Advisory Board memberships of Spherecydes, Pfizer, MSD, Novartis and AstraZeneca, and DSMB membership of Sanofi, in the last 36 months (unrelated to the work in this manuscript, payments to institution). M.G.N. is scientific founder and a scientific advisory board member of Trained Therapeutix Discovery (TTxD) and scientific founder of Lemba Therapeutics, has obtained research grants from GSK Biologicals, TTxD, and Ono Pharma, and consultancy fees from TTxD. J.H.H.M.v.d.W. reports payments for meeting attendance from the Dutch Ministry of Health and Sports and The Netherlands Organization for Health Research and Development (ZonMw) in the last 36 months (unrelated to the work in this manuscript, payments to institution). All other authors declare no competing interests.
Funding Statement
The original BCG-Corona trial was not externally funded. The additional work included in this publication is part of the project “BCG vaccination to minimize COVID-19 disease severity and duration” with project number 10430 01 201 0026 of the research programme COVID-19 which is financed by The Netherlands Organization for Health Research and Development (ZonMw). M.G.N. was also funded by an ERC Advanced Grant (grant number 833247) and Spinoza grant of The Netherlands Organization for Scientific Research (NWO). L.M.V. was also funded by a Hypatia Tenure Track grant of the Radboud University Medical Center (Nijmegen). The funders did not have any role in the collection, analysis, and interpretation of data; in the writing of the report; and in the decision to submit the paper for publication.
Footnotes
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content.
References
- 1.Munitz A., Edry-Botzer L., Itan M., Tur-Kaspa R., Dicker D., Marcoviciu D., Goren M.G., Mor M., Lev S., Gottesman T., et al. Rapid Seroconversion and Persistent Functional IgG Antibodies in Severe COVID-19 Patients Correlates with an IL-12p70 and IL-33 Signature. Sci. Rep. 2021;11:3461. doi: 10.1038/s41598-021-83019-0. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.McAndrews K.M., Dowlatshahi D.P., Dai J., Becker L.M., Hensel J., Snowden L.M., Leveille J.M., Brunner M.R., Holden K.W., Hopkins N.S., et al. Heterogeneous Antibodies against SARS-CoV-2 Spike Receptor Binding Domain and Nucleocapsid with Implications for COVID-19 Immunity. JCI Insight. 2020;5:e142386. doi: 10.1172/jci.insight.142386. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Yang H., Rao Z. Structural Biology of SARS-CoV-2 and Implications for Therapeutic Development. Nat. Rev. Microbiol. 2021;19:685–700. doi: 10.1038/s41579-021-00630-8. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Seow J., Graham C., Merrick B., Acors S., Pickering S., Steel K.J.A., Hemmings O., O’Bryne A., Kouphou N., Galao R.P., et al. Longitudinal Evaluation and Decline of Antibody Responses in SARS-CoV-2 Infection. Nat. Microbiol. 2020;5:1598–1607. doi: 10.1038/s41564-020-00813-8. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Walsh E.E., Frenck R.W., Falsey A.R., Kitchin N., Absalon J., Gurtman A., Lockhart S., Neuzil K., Mulligan M.J., Bailey R., et al. Safety and Immunogenicity of Two RNA-Based COVID-19 Vaccine Candidates. N. Engl. J. Med. 2020;383:2439–2450. doi: 10.1056/NEJMoa2027906. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Baden L.R., El Sahly H.M., Essink B., Kotloff K., Frey S., Novak R., Diemert D., Spector S.A., Rouphael N., Creech C.B., et al. Efficacy and Safety of the mRNA-1273 SARS-CoV-2 Vaccine. N. Engl. J. Med. 2021;384:403–416. doi: 10.1056/NEJMoa2035389. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Sadoff J., Gray G., Vandebosch A., Cárdenas V., Shukarev G., Grinsztejn B., Goepfert P.A., Truyers C., Fennema H., Spiessens B., et al. Safety and Efficacy of Single-Dose Ad26.COV2.S Vaccine against COVID-19. N. Engl. J. Med. 2021;384:2187–2201. doi: 10.1056/NEJMoa2101544. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Barrett J.R., Belij-Rammerstorfer S., Dold C., Ewer K.J., Folegatti P.M., Gilbride C., Halkerston R., Hill J., Jenkin D., Stockdale L., et al. Phase 1/2 Trial of SARS-CoV-2 Vaccine ChAdOx1 nCoV-19 with a Booster Dose Induces Multifunctional Antibody Responses. Nat. Med. 2021;27:279–288. doi: 10.1038/s41591-020-01179-4. [DOI] [PubMed] [Google Scholar]
- 9.Sternberg A., Naujokat C. Structural Features of Coronavirus SARS-CoV-2 Spike Protein: Targets for Vaccination. Life Sci. 2020;257:118056. doi: 10.1016/j.lfs.2020.118056. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Solastie A., Virta C., Haveri A., Ekström N., Kantele A., Miettinen S., Lempainen J., Jalkanen P., Kakkola L., Dub T., et al. A Highly Sensitive and Specific SARS-CoV-2 Spike- and Nucleoprotein-Based Fluorescent Multiplex Immunoassay (FMIA) to Measure IgG, IgA, and IgM Class Antibodies. Microbiol. Spectr. 2021;9:e01131-21. doi: 10.1128/Spectrum.01131-21. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Kontou P.I., Braliou G.G., Dimou N.L., Nikolopoulos G., Bagos P.G. Antibody Tests in Detecting SARS-CoV-2 Infection: A Meta-Analysis. Diagnostics. 2020;10:319. doi: 10.3390/diagnostics10050319. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.den Hartog G., Schepp R.M., Kuijer M., GeurtsvanKessel C., van Beek J., Rots N., Koopmans M.P.G., van der Klis F.R.M., van Binnendijk R.S. SARS-CoV-2–Specific Antibody Detection for Seroepidemiology: A Multiplex Analysis Approach Accounting for Accurate Seroprevalence. J. Infect. Dis. 2020;222:1452–1461. doi: 10.1093/infdis/jiaa479. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.van den Hoogen L.L., Smits G., van Hagen C.C.E., Wong D., Vos E.R.A., van Boven M., de Melker H.E., van Vliet J., Kuijer M., Woudstra L., et al. Seropositivity to Nucleoprotein to Detect Mild and Asymptomatic SARS-CoV-2 Infections: A Complementary Tool to Detect Breakthrough Infections after COVID-19 Vaccination? Vaccine. 2022;40:2251–2257. doi: 10.1016/j.vaccine.2022.03.009. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Tilocca B., Soggiu A., Sanguinetti M., Musella V., Britti D., Bonizzi L., Urbani A., Roncada P. Comparative Computational Analysis of SARS-CoV-2 Nucleocapsid Protein Epitopes in Taxonomically Related Coronaviruses. Microbes Infect. 2020;22:188–194. doi: 10.1016/j.micinf.2020.04.002. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Tan Y.-J., Goh P.-Y., Fielding B.C., Shen S., Chou C.-F., Fu J.-L., Leong H.N., Leo Y.S., Ooi E.E., Ling A.E., et al. Profiles of Antibody Responses against Severe Acute Respiratory Syndrome Coronavirus Recombinant Proteins and Their Potential Use as Diagnostic Markers. Clin. Diagn. Lab. Immunol. 2004;11:362–371. doi: 10.1128/cdli.11.2.362-371.2004. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Cervia C., Nilsson J., Zurbuchen Y., Valaperti A., Schreiner J., Wolfensberger A., Raeber M.E., Adamo S., Weigang S., Emmenegger M., et al. Systemic and Mucosal Antibody Responses Specific to SARS-CoV-2 during Mild versus Severe COVID-19. J. Allergy Clin. Immunol. 2021;147:545–557.e9. doi: 10.1016/j.jaci.2020.10.040. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Lou B., Li T.-D., Zheng S.-F., Su Y.-Y., Li Z.-Y., Liu W., Yu F., Ge S.-X., Zou Q.-D., Yuan Q., et al. Serology Characteristics of SARS-CoV-2 Infection since Exposure and Post Symptom Onset. Eur. Respir. J. 2020;56:2000763. doi: 10.1183/13993003.00763-2020. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Zervou F.N., Louie P., Stachel A., Zacharioudakis I.M., Ortiz-Mendez Y., Thomas K., Aguero-Rosenfeld M.E. SARS-CoV-2 Antibodies: IgA Correlates with Severity of Disease in Early COVID-19 Infection. J. Med. Virol. 2021;93:5409–5415. doi: 10.1002/jmv.27058. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Wölfel R., Corman V.M., Guggemos W., Seilmaier M., Zange S., Müller M.A., Niemeyer D., Jones T.C., Vollmar P., Rothe C., et al. Virological Assessment of Hospitalized Patients with COVID-2019. Nature. 2020;581:465–469. doi: 10.1038/s41586-020-2196-x. [DOI] [PubMed] [Google Scholar]
- 20.WHO Working Group on the Clinical Characterisation and Management of COVID-19 infection A Minimal Common Outcome Measure Set for COVID-19 Clinical Research. Lancet Infect. Dis. 2020;20:e192–e197. doi: 10.1016/S1473-3099(20)30483-7. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Claus J., ten Doesschate T., Gumbs C., van Werkhoven C.H., van der Vaart T.W., Janssen A.B., Smits G., van Binnendijk R., van der Klis F., van Baarle D., et al. BCG Vaccination of Health Care Workers Does Not Reduce SARS-CoV-2 Infections nor Infection Severity or Duration: A Randomized Placebo-Controlled Trial. mBio. 2023;14:e00356-23. doi: 10.1128/mbio.00356-23. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.World Health Organization . First WHO International Standard for Anti-SARS-CoV-2 Immunoglobulin (Human) World Health Organization; Geneva, Switzerland: 2020. [Google Scholar]
- 23.Vos E.R.A., van Boven M., den Hartog G., Backer J.A., Klinkenberg D., van Hagen C.C.E., Boshuizen H., van Binnendijk R.S., Mollema L., van der Klis F.R.M., et al. Associations between Measures of Social Distancing and Severe Acute Respiratory Syndrome Coronavirus 2 Seropositivity: A Nationwide Population-Based Study in the Netherlands. Clin. Infect. Dis. Off. Publ. Infect. Dis. Soc. Am. 2021;73:2318–2321. doi: 10.1093/cid/ciab264. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.van den Hoogen L.L., Verheul M.K., Vos E.R.A., van Hagen C.C.E., van Boven M., Wong D., Wijmenga-Monsuur A.J., Smits G., Kuijer M., van Rooijen D., et al. SARS-CoV-2 Spike S1-Specific IgG Kinetic Profiles Following mRNA or Vector-Based Vaccination in the General Dutch Population Show Distinct Kinetics. Sci. Rep. 2022;12:5935. doi: 10.1038/s41598-022-10020-6. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.Wei J., Stoesser N., Matthews P.C., Ayoubkhani D., Studley R., Bell I., Bell J.I., Newton J.N., Farrar J., Diamond I., et al. Antibody Responses to SARS-CoV-2 Vaccines in 45,965 Adults from the General Population of the United Kingdom. Nat. Microbiol. 2021;6:1140–1149. doi: 10.1038/s41564-021-00947-3. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26.Eyre D.W., Lumley S.F., Wei J., Cox S., James T., Justice A., Jesuthasan G., O’Donnell D., Howarth A., Hatch S.B., et al. Quantitative SARS-CoV-2 Anti-Spike Responses to Pfizer–BioNTech and Oxford–AstraZeneca Vaccines by Previous Infection Status. Clin. Microbiol. Infect. 2021;27:1516.e7–1516.e14. doi: 10.1016/j.cmi.2021.05.041. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27.Pooley N., Abdool Karim S.S., Combadière B., Ooi E.E., Harris R.C., El Guerche Seblain C., Kisomi M., Shaikh N. Durability of Vaccine-Induced and Natural Immunity against COVID-19: A Narrative Review. Infect. Dis. Ther. 2023;12:367–387. doi: 10.1007/s40121-022-00753-2. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28.Hall V., Foulkes S., Insalata F., Kirwan P., Saei A., Atti A., Wellington E., Khawam J., Munro K., Cole M., et al. Protection against SARS-CoV-2 after COVID-19 Vaccination and Previous Infection. N. Engl. J. Med. 2022;386:1207–1220. doi: 10.1056/NEJMoa2118691. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29.Bobrovitz N., Ware H., Ma X., Li Z., Hosseini R., Cao C., Selemon A., Whelan M., Premji Z., Issa H., et al. Protective Effectiveness of Previous SARS-CoV-2 Infection and Hybrid Immunity against the Omicron Variant and Severe Disease: A Systematic Review and Meta-Regression. Lancet Infect. Dis. 2023;23:556–567. doi: 10.1016/S1473-3099(22)00801-5. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 30.Legros V., Denolly S., Vogrig M., Boson B., Siret E., Rigaill J., Pillet S., Grattard F., Gonzalo S., Verhoeven P., et al. A Longitudinal Study of SARS-CoV-2-Infected Patients Reveals a High Correlation between Neutralizing Antibodies and COVID-19 Severity. Cell. Mol. Immunol. 2021;18:318–327. doi: 10.1038/s41423-020-00588-2. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 31.Shrotri M., Navaratnam A.M.D., Nguyen V., Byrne T., Geismar C., Fragaszy E., Beale S., Fong W.L.E., Patel P., Kovar J., et al. Spike-Antibody Waning after Second Dose of BNT162b2 or ChAdOx1. Lancet. 2021;398:385–387. doi: 10.1016/S0140-6736(21)01642-1. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 32.Koekenbier E.L., Fohse K., van de Maat J.S., Oosterheert J.J., van Nieuwkoop C., Hoogerwerf J.J., Grobusch M.P., van den Bosch M.A.A.J., van de Wijgert J.H.H., Netea M.G., et al. Bacillus Calmette-Guérin Vaccine for Prevention of COVID-19 and Other Respiratory Tract Infections in Older Adults with Comorbidities: A Randomized Controlled Trial. Clin. Microbiol. Infect. Off. Publ. Eur. Soc. Clin. Microbiol. Infect. Dis. 2023;29:781–788. doi: 10.1016/j.cmi.2023.01.019. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 33.Moorlag S.J.C.F.M., Taks E., Ten Doesschate T., van der Vaart T.W., Janssen A.B., Müller L., Ostermann P., Dijkstra H., Lemmers H., Simonetti E., et al. Efficacy of BCG Vaccination against Respiratory Tract Infections in Older Adults during the Coronavirus Disease 2019 Pandemic. Clin. Infect. Dis. Off. Publ. Infect. Dis. Soc. Am. 2022;75:e938–e946. doi: 10.1093/cid/ciac182. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 34.Patil H.P., Rane P.S., Shrivastava S., Palkar S., Lalwani S., Mishra A.C., Arankalle V.A. Antibody (IgA, IgG, and IgG Subtype) Responses to SARS-CoV-2 in Severe and Nonsevere COVID-19 Patients. Viral Immunol. 2021;34:201–209. doi: 10.1089/vim.2020.0321. [DOI] [PubMed] [Google Scholar]
- 35.To K.K.-W., Tsang O.T.-Y., Leung W.-S., Tam A.R., Wu T.-C., Lung D.C., Yip C.C.-Y., Cai J.-P., Chan J.M.-C., Chik T.S.-H., et al. Temporal Profiles of Viral Load in Posterior Oropharyngeal Saliva Samples and Serum Antibody Responses during Infection by SARS-CoV-2: An Observational Cohort Study. Lancet Infect. Dis. 2020;20:565–574. doi: 10.1016/S1473-3099(20)30196-1. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 36.Takita M., Yoshida T., Tsuchida T., Nakagama Y., Kido Y., Suzuki S., Imamura M., Kawahata K., Shimizu G., Yoshida H., et al. Low SARS-CoV-2 Antibody Titers May Be Associated with Poor Clinical Outcomes for Patients with Severe COVID-19. Sci. Rep. 2022;12:9147. doi: 10.1038/s41598-022-12834-w. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 37.García-Abellán J., Padilla S., Fernández-González M., García J.A., Agulló V., Andreo M., Ruiz S., Galiana A., Gutiérrez F., Masiá M. Antibody Response to SARS-CoV-2 Is Associated with Long-Term Clinical Outcome in Patients with COVID-19: A Longitudinal Study. J. Clin. Immunol. 2021;41:1490–1501. doi: 10.1007/s10875-021-01083-7. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 38.Cervia C., Zurbuchen Y., Taeschler P., Ballouz T., Menges D., Hasler S., Adamo S., Raeber M.E., Bächli E., Rudiger A., et al. Immunoglobulin Signature Predicts Risk of Post-Acute COVID-19 Syndrome. Nat. Commun. 2022;13:446. doi: 10.1038/s41467-021-27797-1. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 39.Augustin M., Schommers P., Stecher M., Dewald F., Gieselmann L., Gruell H., Horn C., Vanshylla K., Cristanziano V.D., Osebold L., et al. Post-COVID Syndrome in Non-Hospitalised Patients with COVID-19: A Longitudinal Prospective Cohort Study. Lancet Reg. Health Eur. 2021;6:100122. doi: 10.1016/j.lanepe.2021.100122. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 40.Joung S., Weber B., Wu M., Liu Y., Tang A.B., Driver M., Sternbach S., Wynter T., Hoang A., Barajas D., et al. Serological Response to Vaccination in Post-Acute Sequelae of COVID. BMC Infect. Dis. 2023;23:97. doi: 10.1186/s12879-023-08060-y. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 41.Zhao J., Yuan Q., Wang H., Liu W., Liao X., Su Y., Wang X., Yuan J., Li T., Li J., et al. Antibody Responses to SARS-CoV-2 in Patients with Novel Coronavirus Disease 2019. Clin. Infect. Dis. 2020;71:2027–2034. doi: 10.1093/cid/ciaa344. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 42.Long Q.-X., Liu B.-Z., Deng H.-J., Wu G.-C., Deng K., Chen Y.-K., Liao P., Qiu J.-F., Lin Y., Cai X.-F., et al. Antibody Responses to SARS-CoV-2 in Patients with COVID-19. Nat. Med. 2020;26:845–848. doi: 10.1038/s41591-020-0897-1. [DOI] [PubMed] [Google Scholar]
- 43.Soriano J.B., Murthy S., Marshall J.C., Relan P., Diaz J.V., WHO Clinical Case Definition Working Group on Post-COVID-19 Condition A Clinical Case Definition of Post-COVID-19 Condition by a Delphi Consensus. Lancet Infect. Dis. 2022;22:e102–e107. doi: 10.1016/S1473-3099(21)00703-9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 44.Úri K., Fagyas M., Kertész A., Borbély A., Jenei C., Bene O., Csanádi Z., Paulus W.J., Édes I., Papp Z., et al. Circulating ACE2 Activity Correlates with Cardiovascular Disease Development. J. Renin-Angiotensin-Aldosterone Syst. JRAAS. 2016;17:1470320316668435. doi: 10.1177/1470320316668435. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 45.Li X.C., Zhang J., Zhuo J.L. The Vasoprotective Axes of the Renin-Angiotensin System: Physiological Relevance and Therapeutic Implications in Cardiovascular, Hypertensive and Kidney Diseases. Pharmacol. Res. 2017;125:21–38. doi: 10.1016/j.phrs.2017.06.005. [DOI] [PMC free article] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
Data Availability Statement
Individual participant data that underlie the results reported in this article will be made available after de-identification to investigators whose proposed use of the data has been approved by an independent review committee for up to 5 years following publication. The study protocol will be available to anyone during this same time frame. Information regarding submitting proposals and accessing data may be found on https://dataverse.nl/, accessed on 19 June 2024.