

Abstract
Objective:
To compare weight loss response and changes in cardiometabolic risk markers in post-menopausal women using semaglutide with and without menopause hormone therapy (HT) use.
Methods:
Retrospective cohort study of post-menopausal women treated with semaglutide for overweight or obesity for ≥3 months. Endpoints: total body weight loss percentage (TBWL%) at three, six, nine, and twelve months after semaglutide initiation; and percentage of women achieving ≥5% and ≥10% TBWL and changes in cardiometabolic risk markers (glucose, blood pressure, and lipids) at twelve months.
Results:
There were 16 women on HT and 90 on no-HT; mean age 56 ± 8 vs 59 ± 8 years, P=0.2 and mean BMI 36 ± 5 vs 39 ± 8 kg/m2, P=0.1; respectively. Among women on no-HT, White race, dyslipidemia, and depression were more prevalent. Women on HT had a higher TBWL% at three, six, nine, and twelve months: 7 ± 3% vs 5 ± 4%, P=0.01; 13 ± 6% vs 9 ± 5%, P=0.01; 15 ± 6% vs 10 ± 6%, P=0.02; and 16 ± 6% vs 12 ± 8%, P=0.04; respectively. After adjusting for potential confounders, this association remained significant across time. At twelve months, a greater percentage of women on HT achieved ≥5% and ≥10% TBWL. Both groups experienced an improvement in cardiometabolic risk markers.
Conclusion:
In post-menopausal women with overweight or obesity treated with semaglutide, HT use was associated with an improved weight loss response. This association was maintained when adjusted for confounders. Larger studies should be conducted to confirm these results.
Keywords: Menopause, Hormone Therapy, Obesity, Antiobesity Medications, Semaglutide
Introduction
During the menopause transition, up to 70% of women experience weight gain1. Weight gain is typically modest and estimated at 2.1 kg2–5. While aging and estrogen decline play a key role, additional factors have also been identified6,7. For instance, through the menopause transition, women experience a decrease in total 24-hour energy expenditure by 9% and a decrease in spontaneous physical activity energy expenditure by 30%8. Aside from weight gain, the menopause transition is associated with changes in body composition including an increase in fat mass, a decrease in lean mass, and an increase in abdominal adiposity8,9. These changes in weight and body composition increase the risk for cardiometabolic diseases, as evidenced by the increased prevalence of type 2 diabetes, dyslipidemia, metabolic dysfunction-associated steatotic liver disease (MASLD-previously referred to as non-alcoholic fatty liver disease), and cardiovascular disease (CVD) after menopause10–14.
There is evidence that use of menopause hormone therapy (HT) can partially mitigate these changes. During menopause, HT use, compared to no-HT use, has been shown to attenuate the increase in total and visceral abdominal adiposity by around 60% and to decrease waist circumference and body mass index (BMI) by 0.8%9,15–19. HT use has not only been associated with the attenuation of lean mass loss but with an increase in lean mass by 1%15,20. Furthermore, HT use decreases vasomotor symptoms during the menopause transition which can lead to improved sleep, increased activity, and overall increased quality of life, all factors that can further mitigate the changes in body composition experienced during menopause21. Additional favorable effects of HT use include an improvement in glucose metabolism, a reduction in the risk of diabetes, an improvement in the lipid profile, a decrease in the incidence of MASLD, and an overall favorable impact on CVD risk10,16,18,22.
Weight loss can improve cardiometabolic diseases, consequently decreasing CVD and mortality risks23. As CVD is the leading cause of mortality in women and menopause is an independent risk factor for CVD, interventions to prevent weight gain and manage overweight and obesity are of particular importance in post-menopausal women24. Semaglutide is a glucagon-like peptide 1 receptor agonist approved for the treatment of overweight and obesity that leads to a mean weight loss of 15% after 68 weeks, weight loss that is superior to other antiobesity medications25–32. Furthermore, a recent press release reported that semaglutide decreases the risk of major adverse cardiovascular events by 20%, becoming the only antiobesity medication shown to improve cardiovascular outcomes in patients with overweight and obesity33.
This study compared weight loss response to semaglutide between post-menopausal women with and without HT use. It further determined if cardiometabolic risk markers such as fasting glucose, glycosylated hemoglobin A1c (HbA1c), blood pressure, and lipid profile changed over twelve months of semaglutide use by group. We hypothesized that in post-menopausal women using semaglutide for the treatment of overweight and obesity, HT use would be associated with an improved weight loss response as compared to post-menopausal women without HT use. We further hypothesized that this improvement would result in a more favorable cardiometabolic risk profile.
Methods
Study Design and Participants
This study is a retrospective review of the electronic medical records (EMRs) of patients in the Mayo Clinic Health System using semaglutide for the treatment of overweight or obesity (BMI >27 kg/m2) between January 1, 2021, and March 31, 2023. This study compared weight loss outcomes and changes in cardiometabolic risk markers in response to semaglutide between post-menopausal women with and without systemic HT use (HT vs no-HT). Menopause status was defined as women ≥40 years old who had ≥12 months of amenorrhea not related to other causes (e.g., use of contraceptives) or women with a history of bilateral oophorectomy. Women older than age 40 years with a history of hysterectomy or endometrial ablation with a documented follicle stimulating hormone (FSH) level greater than 50 IU/L were also included. Women in the no-HT group had to have never received systemic HT. Women were included in the HT group only if HT was started prior to semaglutide initiation and continued throughout the duration of semaglutide treatment. Exclusion criteria included less than three months of semaglutide use, history of bariatric surgery, and active malignancy. HT consisted of transdermal or oral estradiol with or without a progestogen based on hysterectomy status. The Mayo Clinic Institutional Review Board (IRB) waived the need for obtaining informed consent from our patients due to minimal risk attributed to this study.
Data Collection
Data was collected from the EMRs at baseline (i.e., at semaglutide initiation) and at three, six, nine, and twelve months after semaglutide initiation. A 30-day range was implemented for each of the time points. Data collected included basic demographic and social characteristics including age, race, ethnicity, marital status, level of education (classified as lesser than College, i.e., high or middle school; College; and more than College, i.e., Master and Doctoral degrees), and financial situation (self-reported and classified by the existence of financial strain). Additional data collected included anthropometrics (weight, height, and BMI); blood pressure; medical history pertaining to adiposity-related diseases including dyslipidemia, hypertension, type 2 diabetes, gastroesophageal reflux disease, MASLD, and obstructive sleep apnea; mental health history including depression and anxiety; and laboratory data including HbA1c, fasting glucose, total cholesterol, low-density lipoprotein (LDL) cholesterol, high-density lipoprotein (HDL) cholesterol, and triglycerides. Medication data included semaglutide dosing, which was categorized as low dose (0.25 to 1 mg weekly) and high dose (1.7 to 2.4 mg weekly), and dose and type of systemic HT (i.e., transdermal or oral estrogen and progestogen use). Information on the use of weight-promoting medications during the time of semaglutide treatment was also collected. These medications included insulin, sulfonylureas, thiazolidinediones, antipsychotics (olanzapine, clozapine, risperidone, quetiapine, haloperidol, among others), antidepressants (selective serotonin reuptake inhibitors, monoamine oxidase inhibitors, and tricyclics), antihistamines, anticonvulsants (gabapentin, valproic acid, carbamazepine, among others), β-blockers, and corticosteroids 34. Age at menopause was collected when reported in the EMR. Furthermore, data on whether patients met with a dietitian or a behavior modification therapist for weight loss, and the number of visits with each provider were also collected.
Study End Points
The primary endpoint was the percentage of total body weight loss (TBWL%) at twelve months after semaglutide initiation by HT use. TBWL% was calculated using the formula:
The secondary endpoints included: TBWL% at three, six, and nine months after semaglutide initiation and percentage of women achieving ≥5%, ≥10%, ≥15%, and ≥20% of TBWL twelve months after semaglutide initiation by HT use. Additionally, changes in cardiometabolic risk markers from baseline to twelve months were evaluated including blood pressure, fasting glucose, HbA1c, total cholesterol, LDL-cholesterol, HDL-cholesterol, and triglycerides. A subgroup analysis of women on high dose of semaglutide (i.e., semaglutide 1.7–2.4 mg weekly) was performed for all primary and secondary endpoints.
Statistical Analysis
Data analysis was performed using JMP®, Version 16 (SAS Institute Inc., Cary, NC, 1989–2019). Given the normal distribution of variables, continuous data were summarized as mean and standard deviation (mean ± SD). Categorical data were reported as frequencies and percentages. The independent t-test and Pearson χ2 were used to compare continuous and categorical variables among the two groups, respectively. Paired t-test was used to compare changes from baseline and twelve months within each group. Multiple regression analyses were performed to adjust TBWL% outcomes for variables that were significantly different between groups at baseline. Similarly, TBWL% outcomes were adjusted for variables known to affect weight loss response to semaglutide, including age, baseline weight, type 2 diabetes at baseline, as well as nutritional and behavioral support. Mixed linear models were used to estimate associations with weight loss across time. A compound symmetric covariance structure was used. For regression analyses, the β-coefficient with 95% confidence interval (CI) were reported. All two-tailed P values < 0.05 were considered statistically significant. The Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) reporting guideline were followed.
Results
A total of 1,023 patients from the Mayo Clinic Health System were prescribed semaglutide injections for weight loss between January 2021 and March 2023. Seven-hundred and nineteen patients (70%) were excluded due to prescription insurance denial, inability to use the medication due to the national shortage in 2021 and 2022, and less than three months of medication use. From the 304 patients taking semaglutide for the treatment of overweight or obesity, 82 (27%) were men and 63 (21%) were women under 40 years and were therefore excluded. All women ≥40 years old, 159 women, were screened for menopause status and current HT use. From these, 53 (33%) were excluded as they were premenopausal, their last menstrual period was unknown with no documented FSH levels, or because they had a hysterectomy with no documented FSH levels. Figure 1 summarizes the process for patient selection.
Figure 1. Study Flowchart.
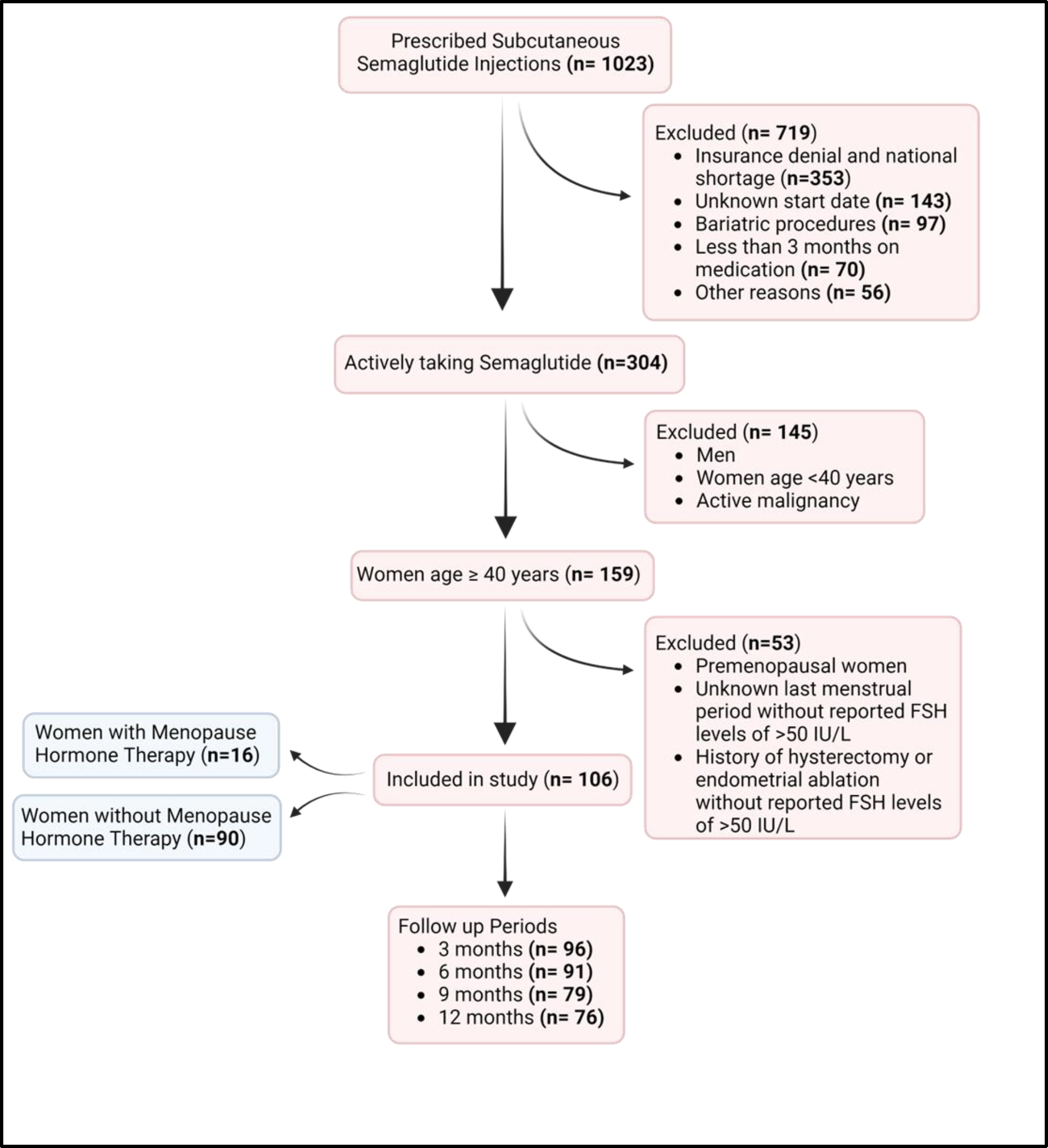
Abbreviations used: FSH, Follicle-Stimulating Hormone.
Baseline characteristics
There was a total of 106 post-menopausal women taking semaglutide for the treatment of overweight or obesity. The cohort was mostly comprised of White, married, college-educated women in their late 50’s with an average BMI in the obesity category class II (Table 1). Most of our cohort was not on HT (n=90 vs n=16 for HT). There were no differences in age, weight, BMI, or type of menopause (natural vs surgical) among the two groups (Table 1). White race was more prevalent in women in the no-HT group compared to HT group (93% vs 65%, P=0.04). There were no differences in ethnicity, marital status, level of education, or financial strain among the two groups.
Table 1.
Baseline Demographic, Social, and Clinical Characteristics of the Cohort by HT Use (n=106)
| All Cohort | HT | no-HT | P-value | ||
|---|---|---|---|---|---|
| N=106 | N=16 | N=90 | |||
| Demographic and Social Characteristics | |||||
| Age, years | 58.4 ± 7.5 | 56.2 ± 7.6 | 58.9 ± 7.5 | 0.2 | |
| Race | White (%) | 96 (91%) | 12(75%) | 84 (93%) | 0.04 |
| African American (%) | 5 (5%) | 1 (6%) | 4 (4%) | ||
| Asian Indian | 3 (3%) | 2 (12%) | 1 (1%) | ||
| Asian Japanese | 1 (1%) | 0 (0%) | 1 (1%) | ||
| Ethnicity, Not Hispanic or Latino | 102 (96%) | 15 (94%) | 87 (97%) | 0.3 | |
| Marital Status | Married (%) | 77 (73%) | 14 (87%) | 63 (70%) | 0.1 |
| Divorced (%) | 13 (12%) | 2 (13%) | 11 (12%) | ||
| Single (%) | 12 (11%) | 0 (0%) | 12 (13%) | ||
| Widowed (%) | 4 (4%) | 0 (0%) | 4 (5%) | ||
| Level of Education | Less than College | 19 (19%) | 1 (6%) | 18 (21%) | 0.4 |
| College | 40 (39%) | 7 (47%) | 33 (38%) | ||
| More than College | 43 (42%) | 7 (47%) | 36 (41%) | ||
| Financial Strain, No | 74 (90%) | 11 (100%) | 63 (89%) | 0.12 | |
| Baseline Body Composition | |||||
| Weight, kg | 104.6 ± 20.2 | 98.3 ± 16.1 | 105.9 ± 20.6 | 0.1 | |
| Body Mass Index, kg/m2 | 38.5 ± 7.5 | 36.4 ± 5.1 | 38.9 ± 7.8 | 0.1 | |
| Obesity Category | |||||
| Overweight (≥25 kg/m2) | 8(8%) | 0(0%) | 8(9%) | 0.15 | |
| Obesity Class I (≥30 kg/m2) | 32(30%) | 8(50%) | 24(27%) | ||
| Obesity Class II (≥35 kg/m2) | 30(28%) | 4(25%) | 26(29%) | ||
| Obesity Class III (≥40 kg/m2) | 36(34%) | 4(25%) | 32(36%) | ||
| Adiposity-Related Diseases | |||||
| Dyslipidemia | 65(61%) | 4(25%) | 61(68%) | 0.001 | |
| Hypertension | 63(59%) | 7(44%) | 56(62%) | 0.2 | |
| Gastroesophageal Reflux Disease | 43(41%) | 6(38%) | 37(41%) | 0.8 | |
| Obstructive Sleep Apnea | 42(40%) | 3(19%) | 39(43%) | 0.053 | |
| Depression | 35(33%) | 2 (13%) | 33 (38%) | 0.04 | |
| Type 2 Diabetes | 30(28%) | 2(13%) | 28(31%) | 0.1 | |
| Anxiety | 27(26%) | 4 (25%) | 23 (26%) | 0.9 | |
| Non-Alcoholic Fatty Liver Disease | 15(14%) | 1(6%) | 14(16%) | 0.3 | |
| Anti-Obesity Medication Dosing | |||||
| 0.25 to 1 mg weekly SQ | 33(31%) | 2(13%) | 31(34%) | 0.06 | |
| 1.7 to 2.4 mg weekly SQ | 73(69%) | 14(88%) | 59(66%) | ||
| Weight-Promoting medications | |||||
| Concomitant Use of Weight-Promoting Medications, Yes | 15 (14%) | 2 (13%) | 13 (14%) | 0.8 | |
| Use of More Than One Weight-Promoting Medication, Yes | 1/15 (7%) | 0/2 | 1/13 (5%) | 0.6 | |
| Weight Management Components | |||||
| Dietitian Visit | |||||
| Yes | 25(24%) | 4(25%) | 21(23%) | 0.9 | |
| Number of Visits (Median, IQ) | 1(1–2.5) | 1.5(1–2) | 1(1–3.5) | 0.1 | |
| Behavioral Therapy | |||||
| Yes | 12(11%) | 2(13%) | 10(11%) | 0.9 | |
| Number of Visits (Median, IQ) | 0(0–3.75) | 0.5(0–1.75) | 0(0–4) | 0.07 | |
| Menopause | |||||
| Natural (vs Surgical) | 82 (77%) | 10 (62%) | 72 (80%) | 0.15 | |
| Type of HT | |||||
| Estrogen Delivery | |||||
| Transdermal | NA | 8 (50%) | NA | ||
| Oral | 8 (50%) | ||||
| Progestogen Use | |||||
| Yes | NA | 6 (38%) | NA | ||
All P values <.05 are considered significant.
Abbreviations used: HT, With Hormone Therapy; IQ, Interquartile Range; no-HT, Without Hormone Therapy; SD, Standard Deviation; SQ, Subcutaneous.
Continuous data are summarized as mean ± SD, unless noted otherwise. Categorical data are summarized as frequency and percentage.
In women using systemic HT, 50% used transdermal estradiol at variable doses between 0.025 to 0.1 mg/day. The other half received oral estradiol between 0.5 and 1 mg daily. Six women (38%) were concomitantly using 100 mg of oral progesterone daily. More women using HT achieved a high dose of semaglutide (1.7–2.4 mg/weekly), although this difference did not reach statistical significance (88% vs 66%, P=0.06; Table 1). In those women achieving a high dose of semaglutide, there were no differences in any of the baseline demographic, social, and anthropometric characteristics among HT and no-HT use (Supplemental Table 1). Among the entire cohort, 14% were using weight-promoting medications at the same time of semaglutide use. There were no differences in the prevalence of weight-promoting medication use among the two groups (Table 1).
The prevalence of adiposity-related diseases varied among the two groups. In women using HT, the most common adiposity-related diseases were hypertension (44%), followed by gastroesophageal reflux disease (38%) and dyslipidemia (25%). In women on no-HT, the most common adiposity-related diseases were dyslipidemia (68%), followed by hypertension (62%) and obstructive sleep apnea (43%). While the prevalence of adiposity-related diseases varied among the two groups, the differences were not statistically significant except for dyslipidemia and depression which were more prevalent in women on no-HT. In women achieving a high dose of semaglutide, only dyslipidemia was more prevalent among no-HT users compared to HT users: 64% vs 27%, P=0.008 (Supplemental Table 1).
Nutrition and behavioral support were offered to all women as part of the comprehensive weight management program, however only 25% and 23% of women elected nutritional support in the HT and no-HT groups, respectively; and 13% and 11% elected behavioral support in the HT and no-HT groups, respectively. There were no differences in nutritional and behavioral support among the two groups.
Total body weight loss outcomes
When compared to the no-HT use, women on HT achieved greater TBWL% at three, six, nine, and twelve months: 7 ± 3% vs 5 ± 4 % (mean difference 2%, P=0.01), 13 ± 6 % vs 9 ± 5 % (mean difference 4%, P=0.01), 15 ± 6 % vs 10 ± 6 % (mean difference 5%, P=0.02), 16 ± 6 % vs 12 ± 8 % (mean difference 4%, P=0.04), respectively (Figure 2A). Similarly, compared to no-HT use, a higher proportion of women using HT achieved TBWL ≥5% and ≥10% at twelve months, respectively (Figure 2B). There was no significant difference in the proportion of women achieving categorical TBWL ≥15% and ≥20% between the two groups at twelve months.
Figure 2.
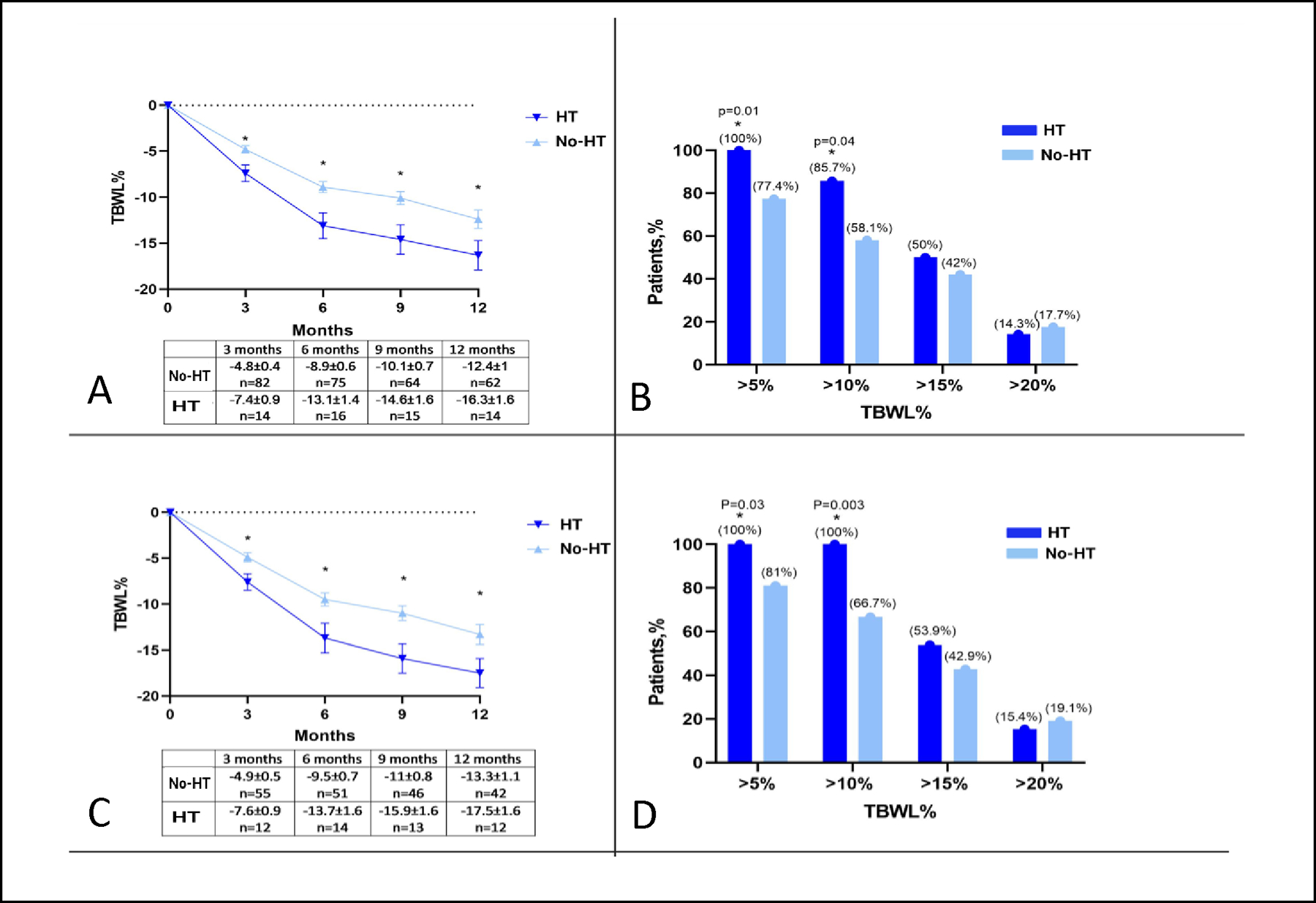
A. Total Body Weight Loss (TBWL) at 3, 6, 9, and 12 Months by Hormone Therapy (HT) Use in All Women (n=106); B. Percentage of Women Achieving ≥5%, ≥10%, ≥15%, and ≥20% of TBWL at 12 Months by HT Use in All Women (n=106); C. TBWL at 3, 6, 9, and 12 Months by HT Use in Women on High Dose a of Semaglutide (n=73); D. Percentage of Women on High Dose a of Semaglutide Achieving ≥5%, ≥10%, ≥15%, and ≥20% of TBWL at 12 months by HT use (n=73).
a High dose of semaglutide was defined as a dose of 1.7 to 2.4 mg weekly.
Abbreviations used: HT, With Hormone Therapy; no-HT, Without Hormone Therapy; TBWL, Total Body Weight Loss.
All P values <0.05 are considered significant.
Data in the figures is presented as mean ± standard error of the mean.
When TBWL% was adjusted for semaglutide dose intensity (high [1.7–2.4 mg weekly] vs low [0.25–1 mg weekly]) the differences persisted. Furthermore, in the subgroup analysis of women on a high dose of semaglutide, the differences among the two groups in TBWL% at all timepoints, and the differences in the proportion of women achieving ≥5 and ≥10% TBWL at twelve months also persisted (Figure 2C and 2D). No differences in weight loss response to semaglutide among postmenopausal women with oral vs transdermal estrogen delivery, or with or without concomitant progesterone use were observed (Supplemental Figures 1A and B).
Multiple regression analyses taking into consideration weight loss across all timepoints were performed to account for variables that were statistically different at baseline, including race and the presence of dyslipidemia and depression (Table 2, Model 1A). In this mode, HT use was an independent predictor of TBWL%. A separate multiple regression model took into consideration known variables that affect weight loss response to antiobesity medications including age, baseline weight, type 2 diabetes, and nutritional and behavioral support (Table 2, Model 2A). In this model, HT use also predicted TBWL% with significance. Similar results of these two models were also observed in the subgroup analysis of women taking high doses of semaglutide with or without HT use (Table 2, Models 1B and 2B).
Table 2.
Mixed-Model Multiple Regression Analyses Considering HT Use, Race, and Depression and Dyslipidemia Diagnoses at Baseline (Model 1); and Considering HT Use, Age, Race, Weight and Diabetes Diagnosis at Baseline, and Dietitian and Behavioral Psychology Support (Model 2). Each model was performed in All Women (n=106, Models 1A and 2A) and in Women on High Dose a of Semaglutide only (n=73, Models 1B and 2B).
| Model 1: Mixed-Model Multiple Regression Analyses Considering HT Use, Race, and Depression and Dyslipidemia Diagnoses at Baseline | ||||||||
|---|---|---|---|---|---|---|---|---|
| Model 1A: All Women (N=106) | Model 1B: Women on High Dose of Semaglutide (N=73) | |||||||
| β coefficient | 95% IC | P | β coefficient | 95% IC | P | |||
| HT use (Yes vs. No) | 4.1 | 1.1 | 7 | 0.007 | 3.7 | 1.9 | 5.5 | <.0001 |
| Race (White vs. others) | 0.4 | −3 | 3.8 | 0.8 | 2 | −0.3 | 4.1 | 0.05 |
| Depression (Yes vs. No) | 1.4 | −0.8 | 3.5 | 0.2 | 0.5 | 1 | 2 | 0.5 |
| Dyslipidemia (Yes vs. No) | −0.8 | −2.9 | 1.3 | 0.5 | −2.1 | −3.5 | −0.7 | 0.004 |
| 3 Months (vs. 12 months) | −8.3 | −9.3 | −7.4 | <.0001 | −8.8 | −10.8 | −6.2 | <.0001 |
| 6 Months (vs. 12 months) | −3.7 | −4.7 | −2.8 | <.0001 | −4 | −5.9 | −2 | <.0001 |
| 9 Months (vs. 12 months) | −1.9 | −2.9 | −0.9 | 0.0002 | −2.3 | −4.2 | −0.3 | 0.02 |
| Model 2: Mixed-Model Multiple Regression Analyses Considering HT Use, Age, Race, Weight and Diabetes Diagnosis at Baseline, and Dietitian and Behavioral Psychology Support | ||||||||
| Model 2A: All Women (N=106) | Model 2B: Women on High Dose of Semaglutide (N=73) | |||||||
| β coefficient | 95% IC | P | β coefficient | 95% IC | P | |||
| HT use (Yes vs. No) | 3.4 | 1.8 | 5 | <.0001 | 4.1 | 2.4 | 5.7 | <.0001 |
| Age (Each 1-year increase) | −0.01 | −0.1 | 0.08 | 0.9 | 0.02 | −0.08 | 0.1 | 0.7 |
| Race (White vs. others) | 0.8 | −1.2 | 2.7 | 0.4 | 2.3 | 0.3 | 4.3 | 0.03 |
| Baseline Weight (Each 1 kg increase) | 0.05 | 0.02 | 0.08 | 0.003 | 0.08 | 0.04 | 0.1 | <.0001 |
| Diabetes (Yes vs. No) | −1.5 | −3 | −0.06 | 0.04 | −1 | −2.8 | 0.8 | 0.3 |
| Dietitian Visit (Yes vs. No) | −0.7 | −2.1 | 0.8 | 0.4 | 0.6 | −1.1 | 2.3 | 0.5 |
| Psychology Visit (Yes vs. No) | 0.3 | −1.8 | 2.4 | 0.8 | −0.15 | −2.5 | 2.2 | 0.9 |
| 3 Months (vs. 12 months) | −7.7 | −9.3 | −6.1 | <.0001 | −8.7 | −10.5 | −6.9 | <.0001 |
| 6 Months (vs. 12 months) | −3.4 | −5.1 | −1.8 | <.0001 | −4 | −5.9 | −2.2 | <.0001 |
| 9 Months (vs. 12 months) | −2.1 | −3.8 | −0.4 | 0.01 | −2.2 | −4.1 | −0.3 | 0.02 |
High dose of semaglutide was defined as a dose of 1.7 to 2.4 mg weekly.
Abbreviations used: HT, With Hormone Therapy; no-HT, Without Hormone Therapy
All P values <.05 are considered significant.
Changes in Cardiometabolic Risk Markers
Both groups had improvement in cardiometabolic risk markers (Figure 3 and Supplemental Table 2). Women on no-HT had a significant improvement in fasting glucose, HbA1c, and systolic blood pressure. Women on HT had significant improvement in HbA1c, triglycerides, and total cholesterol. For these women, there was a near significant improvement in systolic blood pressure and LDL-cholesterol (P=0.06 for both). In the women on high doses of semaglutide, women on no-HT had a significant improvement in HbA1c and systolic blood pressure and women on HT had a significant improvement in HbA1c, triglycerides, and total cholesterol, with a trend toward improvement in systolic blood pressure and LDL-cholesterol (Supplemental Table 3). We compared the changes from baseline to twelve months of each cardiometabolic risk marker among the two groups and no differences were observed (data not shown).
Figure 3. Changes in Fasting Glucose, HbA1c, Lipid Profile, and Blood Pressure by Hormone Therapy Use in All Women (n=106).
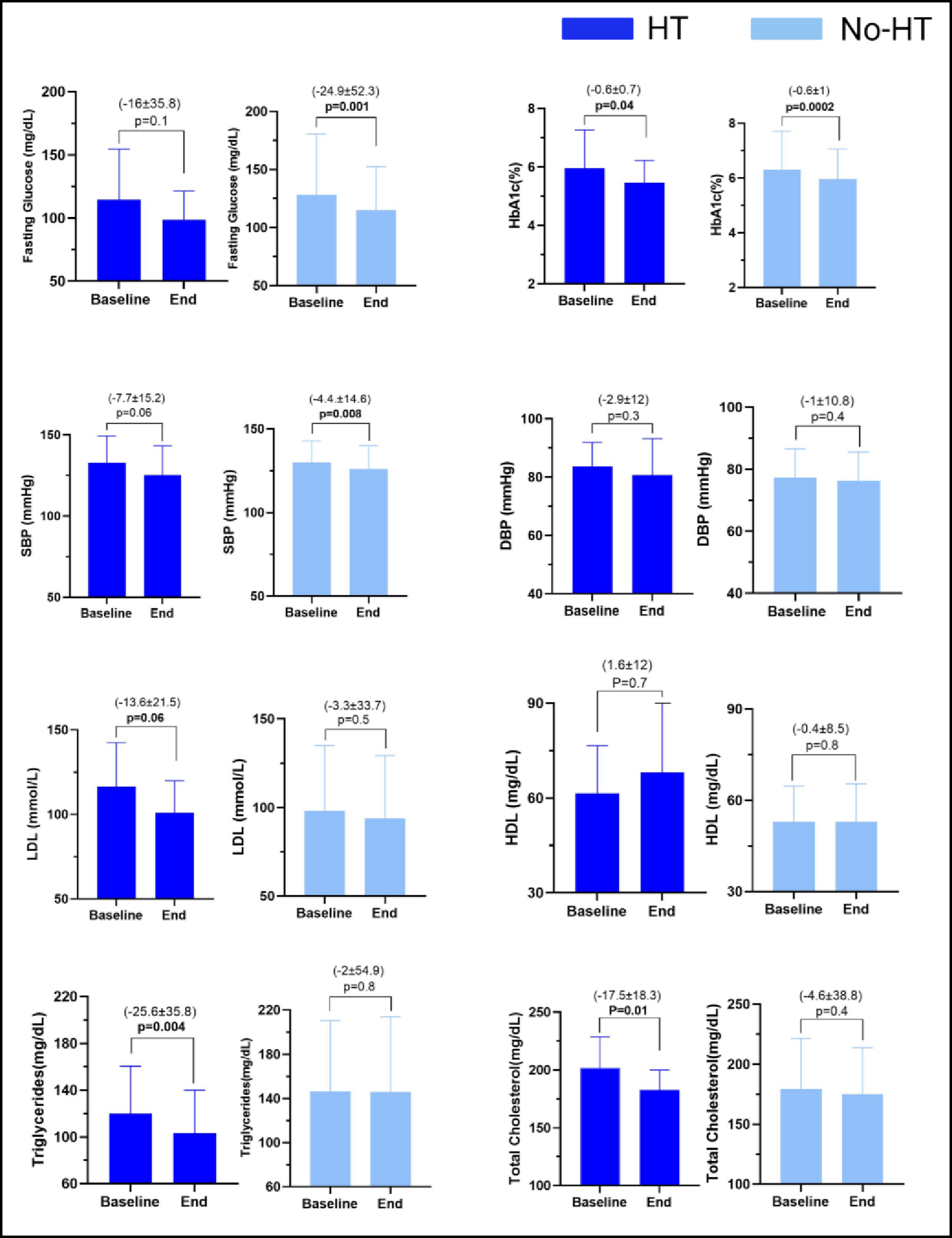
Abbreviations used: DBP, Diastolic Blood Pressure; HbA1c, Glycosylated Hemoglobin; HDL, High Density Lipoprotein; HT, With Hormone Therapy; LDL, Low Density Lipoprotein; no-HT, Without Hormone Therapy; SBP, Systolic Blood Pressure; SD, Standard Deviation.
All P values <0.05 are considered significant.
Data in the figures is presented as mean ± standard deviation.
Discussion
In this study, the weight loss response to semaglutide differed between post-menopausal women with and without HT use. Three, six, nine, and twelve months after semaglutide initiation, HT use was associated with approximately 30% more weight loss. After adjusting for potential confounding variables this association remained significant across time. Similarly, at twelve months, HT use was associated with a greater probability of achieving ≥5% and ≥10% TBWL. The weight loss observed in our study was associated with an improvement in cardiometabolic risk markers, regardless of HT use.
These results replicate the effectiveness of semaglutide in phase 3 clinical trials and real-world studies26,28. The 16% total body weight loss observed in the HT group, is similar to the weight loss response to semaglutide in pivotal studies25,26. We observed an inferior weight loss response in the no-HT group that cannot be explained by the presence of factors that can affect weight loss, such as age, baseline weight, the presence of type 2 diabetes at baseline, and semaglutide dosage. Given the retrospective nature of the study, we were unable to identify factors other than HT use that could explain this differential response.
While the difference in weight loss response among the two groups may be explained by the positive effects of HT on body composition changes, other factors need to be considered9,15. The primary indication for HT is for the treatment of vasomotor symptoms which impact 80% of women during the menopause transition and can last a mean of seven to ten years35. Improving vasomotor symptoms can consequently lead to improved sleep, physical activity, and overall quality of life, all factors that can affect response to weight loss interventions21. An additional consideration that can occur in observational studies is healthy-user bias. Healthy-user bias arises when users of preventive medications are healthier due to factors other than medication effect36. This has been well-established in research involving HT use, particularly as it relates to better CVD outcomes37–39. Compared to no-HT users, HT users generally pursue healthier lifestyle, are more physically active, leaner, and less likely to smoke, and have better access to medical care40,41. In this study, it is therefore possible that women on HT were more amenable to make healthier dietary changes and exercise more regularly.
In this study we considered other potential confounders, including the use of weight-promoting medications. Weight-promoting medications can affect weight loss response to weight loss interventions. It is estimated that 11% of post-menopausal take weight-promoting medications, and their use has been associated with greater increase in BMI and waist circumference during this stage of life42. In our study, the prevalence of weight-promoting medications use among HT users and non-users was virtually the same, and thereby this variable may not explain the difference in weight loss outcomes among the two groups. Another important variable to consider, that this retrospective study was not able to fully assess, is the allostatic load. The allostatic load is a measure of cumulative biological risk as people age that can be associated with negative health outcomes and certainly blunted weight loss response to antiobesity interventions43. Our study did however compare certain components that are considered for the allostatic load calculation, including BMI, blood pressure, lipid profile, glucose, and HbA1c, with no differences among the two groups.
To date, there are no studies comparing weight loss outcomes to any of the antiobesity interventions, including semaglutide, among post-menopausal women with and without HT use. This study is relevant because menopause is associated with significant metabolic changes, including weight gain and body composition changes44. As the prevalence of overweight and obesity among post-menopausal women increases, so does the risk of cardiometabolic diseases and CVD mortality45–47. Further, menopause, independent of aging, accelerates CVD risk 24. Therefore, as CVD is the leading cause of death among women, there is a critical need to implement interventions to reduce this risk, including interventions that target excess adiposity. The importance of these interventions is further underscored by the fact that women spend one-half of their adult life in menopause, and as such, improving overall health and quality of life, and decreasing CVD risk is of utmost importance48.
The strengths of the study include a high level of detail regarding data collection. Although this study was limited by the observational and retrospective design, it is the first to assess the response to semaglutide among post-menopausal women with and without current HT use. Furthermore, we report data on cardiometabolic risk markers that may influence weight and overall health management in menopause. Our study has limitations. The retrospective nature of the study does not allow for the establishment of a causal relation between HT use and weight loss response to semaglutide or for the minimization of confounding factors. Despite including women across the Mayo Clinic Health system, our cohort included 106 women, and only a minority, 15%, were on HT. This is not surprising as the prescription rate of HT among women with clinical indications remains below 10%49,50. Although we observed significant differences in weight loss at all time points, our small sample size may have affected the statistical significance of some of our endpoints. Importantly, the sample size reflects the strict inclusion and exclusion criteria used to avoid potential confounders, which is a strength of this study. Additionally, our study consisted of mostly White, college-educated women with no financial strain, potentially limiting the generalizability of the findings.
To establish a more definitive relationship between HT use and weight loss response to semaglutide in post-menopausal women, future prospective studies should incorporate the age at menopause; type of menopause; the duration, type, and dose of HT use; data on sleep quality, vasomotor symptoms, quality of life, activity, diet, and allostatic load; and the timing of semaglutide initiation in relation to HT initiation. Similarly, it would be interesting to investigate if there are differences in weight loss response to antiobesity medications among pre-, peri- and post-menopausal women not using HT (after adjusting for age and body composition), and if there are differences, if these are mitigated with HT use.
Conclusion
The menopause transition is associated with weight gain. As a woman’s predicted lifespan continues to increase, women will spend a greater percentage of their lives in menopause. This, added to the fact that the obesity prevalence continues to rise in midlife women, underscores the importance of weight management interventions in post-menopausal women. In this study, HT use in post-menopausal women was associated with a greater weight loss with semaglutide. Larger studies are needed to confirm these results. Further, future studies are needed to identify the mechanisms behind this differential weight loss response. While the effect of HT use on body composition could partly explain this difference, additional mechanisms are probably involved, such as the effect of HT on sleep quality, vasomotor symptoms, and quality of life.
Supplementary Material
Supplemental Table 1. Baseline Demographic, Social, and Clinical Characteristics of Women on High Dose a of Semaglutide by HT Use (n=73)
a High dose of semaglutide was defined as a dose of 1.7 to 2.4 mg weekly.
Continuous data are summarized as mean ± SD, unless noted otherwise. Categorical data are summarized as frequency and percentage.
Abbreviations used: HT, With Hormone Therapy; IQ, Interquartile Range; no-HT, Without Hormone Therapy; SD, Standard Deviation; SQ, Subcutaneous.
All P values <0.05 are considered significant.
Supplemental Table 2. Changes in Fasting Glucose, HbA1c, Lipid Profile, and Blood Pressure by HT Use in All Women (n=106)
Abbreviations used: DBP, Diastolic Blood Pressure; HbA1c, Glycosylated Hemoglobin A1c; HDL, High Density Lipoprotein; HT, With Hormone Therapy; LDL, Low Density Lipoprotein; no-HT, Without Hormone Therapy; SBP, Systolic Blood Pressure; SD, Standard Deviation.
All P values <0.05 are considered significant.
Supplemental Table 3. Changes in Fasting Glucose, HbA1c, Lipid Profile, and Blood Pressure by HT Use in Women on High Dose a of Semaglutide (n=73)
a High dose of semaglutide was defined as a dose of 1.7 to 2.4 mg weekly.
Abbreviations used: DBP, Diastolic Blood Pressure; HbA1c, Glycosylated Hemoglobin A1c; HDL, High Density Lipoprotein; HT, With Hormone Therapy; LDL, Low Density Lipoprotein; no-HT, Without Hormone Therapy; SBP, Systolic Blood Pressure; SD, Standard Deviation.
All P values <0.05 are considered significant.
Supplemental Figure 1. A. Total body Weight Loss Percentage (TBWL%) at 3, 6, 9, and 12 Months in Women with HT Use with Oral vs Transdermal Estrogen; B. TBWL% at 3, 6, 9, and 12 Months in Women with HT Use With vs Without Progesterone Use.
Abbreviations used: HT, With Hormone Therapy; no-HT, Without Hormone Therapy; OE, Oral Estrogen; P+, With Progesterone Use; P-, Without Progesterone Use; TBWL, Total Body Weight Loss; TE, Transdermal Estrogen.
Data in the figures is presented as means.
Funding:
This publication was supported by Grant Number K12 HD065987 and by the Mayo Clinic Center for Women’s Health Research.
Funding Sources:
The funding sources were not involved in the study design, in the collection, analysis, and interpretation of the data, in writing the report, or in the decision to submit the paper for publication.
Abbreviations:
- BMI
Body-Mass Index
- CVD
Cardiovascular Disease
- FSH
Follicle- Stimulating Hormone
- HBA1C
Glycosylated Hemoglobin A1c
- HDL
High Density Lipoprotein
- HT
Hormone Therapy
- LDL
Low Density Lipoprotein
- MASLD
Metabolic Dysfunction-Associated Steatotic Liver Disease
- SD
Standard Deviation
- TBWL
Total Body Weight Loss
Footnotes
Disclosures: Dr. Acosta is a stockholder in Gila Therapeutics, Phenomix Sciences; he served as a consultant for Rhythm Pharmaceuticals, Amgen, Structure Therapeutics, Bausch Health. Other Authors have nothing to disclose.
References
- 1.Pimenta F, Maroco J, Ramos C, Leal I. Predictors of weight variation and weight gain in peri- and post-menopausal women. J Health Psychol. Aug 2014;19(8):993–1002. doi: 10.1177/1359105313483153 [DOI] [PubMed] [Google Scholar]
- 2.Greendale GA, Sternfeld B, Huang M, et al. Changes in body composition and weight during the menopause transition. JCI Insight. Mar 7 2019;4(5)doi: 10.1172/jci.insight.124865 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Sternfeld B, Wang H, Quesenberry CP Jr., et al. Physical activity and changes in weight and waist circumference in midlife women: findings from the Study of Women’s Health Across the Nation. Am J Epidemiol. Nov 1 2004;160(9):912–22. doi: 10.1093/aje/kwh299 [DOI] [PubMed] [Google Scholar]
- 4.Field AE, Willett WC, Lissner L, Colditz GA. Dietary fat and weight gain among women in the Nurses’ Health Study. Obesity (Silver Spring). Apr 2007;15(4):967–76. doi: 10.1038/oby.2007.616 [DOI] [PubMed] [Google Scholar]
- 5.Guthrie JR, Dennerstein L, Dudley EC. Weight gain and the menopause: a 5-year prospective study. Climacteric. Sep 1999;2(3):205–11. doi: 10.3109/13697139909038063 [DOI] [PubMed] [Google Scholar]
- 6.Ambikairajah A, Walsh E, Tabatabaei-Jafari H, Cherbuin N. Fat mass changes during menopause: a metaanalysis. Am J Obstet Gynecol. Nov 2019;221(5):393–409 e50. doi: 10.1016/j.ajog.2019.04.023 [DOI] [PubMed] [Google Scholar]
- 7.Thurston RC, Karvonen-Gutierrez CA, Derby CA, El Khoudary SR, Kravitz HM, Manson JE. Menopause versus chronologic aging: their roles in women’s health. Menopause. Aug 2018;25(8):849–854. doi: 10.1097/GME.0000000000001143 [DOI] [PubMed] [Google Scholar]
- 8.Lovejoy JC, Champagne CM, de Jonge L, Xie H, Smith SR. Increased visceral fat and decreased energy expenditure during the menopausal transition. Int J Obes (Lond). Jun 2008;32(6):949–58. doi: 10.1038/ijo.2008.25 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Papadakis GE, Hans D, Gonzalez Rodriguez E, et al. Menopausal Hormone Therapy Is Associated With Reduced Total and Visceral Adiposity: The OsteoLaus Cohort. J Clin Endocrinol Metab. May 1 2018;103(5):1948–1957. doi: 10.1210/jc.2017-02449 [DOI] [PubMed] [Google Scholar]
- 10.Mauvais-Jarvis F, Manson JE, Stevenson JC, Fonseca VA. Menopausal Hormone Therapy and Type 2 Diabetes Prevention: Evidence, Mechanisms, and Clinical Implications. Endocr Rev. Jun 1 2017;38(3):173–188. doi: 10.1210/er.2016-1146 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.de Kat AC, Dam V, Onland-Moret NC, Eijkemans MJ, Broekmans FJ, van der Schouw YT. Unraveling the associations of age and menopause with cardiovascular risk factors in a large population-based study. BMC Med. Jan 4 2017;15(1):2. doi: 10.1186/s12916-016-0762-8 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Long MT, Pedley A, Massaro JM, et al. A simple clinical model predicts incident hepatic steatosis in a community-based cohort: The Framingham Heart Study. Liver Int. Aug 2018;38(8):1495–1503. doi: 10.1111/liv.13709 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Khan ZA, Janssen I, Mazzarelli JK, et al. Serial Studies in Subclinical Atherosclerosis During Menopausal Transition (from the Study of Women’s Health Across the Nation). Am J Cardiol. Oct 1 2018;122(7):1161–1168. doi: 10.1016/j.amjcard.2018.06.039 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.El Khoudary SR, Shields KJ, Janssen I, et al. Postmenopausal Women With Greater Paracardial Fat Have More Coronary Artery Calcification Than Premenopausal Women: The Study of Women’s Health Across the Nation (SWAN) Cardiovascular Fat Ancillary Study. J Am Heart Assoc. Jan 29 2017;6(2)doi: 10.1161/JAHA.116.004545 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Chen Z, Bassford T, Green SB, et al. Postmenopausal hormone therapy and body composition - a substudy of the estrogen plus progestin trial of the Women’s Health Initiative. American Journal of Clinical Nutrition. Sep 2005;82(3):651–656. doi:DOI 10.1093/ajcn/82.3.651 [DOI] [PubMed] [Google Scholar]
- 16.Costa GBC, Carneiro G, Umeda L, Pardini D, Zanella MT. Influence of Menopausal Hormone Therapy on Body Composition and Metabolic Parameters. Biores Open Access. 2020;9(1):80–85. doi: 10.1089/biores.2019.0050 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Kristensen K, Pedersen SB, Vestergaard P, Mosekilde L, Richelsen B. Hormone replacement therapy affects body composition and leptin differently in obese and non-obese postmenopausal women. J Endocrinol. Oct 1999;163(1):55–62. doi: 10.1677/joe.0.1630055 [DOI] [PubMed] [Google Scholar]
- 18.Salpeter SR, Walsh JM, Ormiston TM, Greyber E, Buckley NS, Salpeter EE. Meta-analysis: effect of hormone-replacement therapy on components of the metabolic syndrome in postmenopausal women. Diabetes Obes Metab. Sep 2006;8(5):538–54. doi: 10.1111/j.1463-1326.2005.00545.x [DOI] [PubMed] [Google Scholar]
- 19.Margolis KL, Bonds DE, Rodabough RJ, et al. Effect of oestrogen plus progestin on the incidence of diabetes in postmenopausal women: results from the Women’s Health Initiative Hormone Trial. Diabetologia. Jul 2004;47(7):1175–1187. doi: 10.1007/s00125-004-1448-x [DOI] [PubMed] [Google Scholar]
- 20.Sorensen MB, Rosenfalck AM, Hojgaard L, Ottesen B. Obesity and sarcopenia after menopause are reversed by sex hormone replacement therapy. Obes Res. Oct 2001;9(10):622–6. doi: 10.1038/oby.2001.81 [DOI] [PubMed] [Google Scholar]
- 21.Khan SJ, Kapoor E, Faubion SS, Kling JM. Vasomotor Symptoms During Menopause: A Practical Guide on Current Treatments and Future Perspectives. Int J Womens Health. 2023;15:273–287. doi: 10.2147/IJWH.S365808 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.DiStefano JK. NAFLD and NASH in Postmenopausal Women: Implications for Diagnosis and Treatment. Endocrinology. Oct 1 2020;161(10)doi: 10.1210/endocr/bqaa134 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.Deibert P, Konig D, Vitolins MZ, et al. Effect of a weight loss intervention on anthropometric measures and metabolic risk factors in pre- versus postmenopausal women. Nutr J. Oct 25 2007;6:31. doi: 10.1186/1475-2891-6-31 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.El Khoudary SR, Aggarwal B, Beckie TM, et al. Menopause Transition and Cardiovascular Disease Risk: Implications for Timing of Early Prevention: A Scientific Statement From the American Heart Association. Circulation. Dec 22 2020;142(25):e506–e532. doi: 10.1161/CIR.0000000000000912 [DOI] [PubMed] [Google Scholar]
- 25.Wadden TA, Bailey TS, Billings LK, et al. Effect of Subcutaneous Semaglutide vs Placebo as an Adjunct to Intensive Behavioral Therapy on Body Weight in Adults With Overweight or Obesity: The STEP 3 Randomized Clinical Trial. JAMA. Apr 13 2021;325(14):1403–1413. doi: 10.1001/jama.2021.1831 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26.Wilding JPH, Batterham RL, Calanna S, et al. Once-Weekly Semaglutide in Adults with Overweight or Obesity. N Engl J Med. Mar 18 2021;384(11):989–1002. doi: 10.1056/NEJMoa2032183 [DOI] [PubMed] [Google Scholar]
- 27.Calderon G, Gonzalez-Izundegui D, Shan KL, et al. Effectiveness of anti-obesity medications approved for long-term use in a multidisciplinary weight management program: a multi-center clinical experience. Int J Obes (Lond). Mar 2022;46(3):555–563. doi: 10.1038/s41366-021-01019-6 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28.Ghusn W, De la Rosa A, Sacoto D, et al. Weight Loss Outcomes Associated With Semaglutide Treatment for Patients With Overweight or Obesity. JAMA Netw Open. Sep 1 2022;5(9):e2231982. doi: 10.1001/jamanetworkopen.2022.31982 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29.Wadden TA, Foreyt JP, Foster GD, et al. Weight loss with naltrexone SR/bupropion SR combination therapy as an adjunct to behavior modification: the COR-BMOD trial. Obesity (Silver Spring). Jan 2011;19(1):110–20. doi: 10.1038/oby.2010.147 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 30.Gadde KM, Allison DB, Ryan DH, et al. Effects of low-dose, controlled-release, phentermine plus topiramate combination on weight and associated comorbidities in overweight and obese adults (CONQUER): a randomised, placebo-controlled, phase 3 trial. Lancet. Apr 16 2011;377(9774):1341–52. doi: 10.1016/S0140-6736(11)60205-5 [DOI] [PubMed] [Google Scholar]
- 31.Rubino DM, Greenway FL, Khalid U, et al. Effect of Weekly Subcutaneous Semaglutide vs Daily Liraglutide on Body Weight in Adults With Overweight or Obesity Without Diabetes: The STEP 8 Randomized Clinical Trial. JAMA. Jan 11 2022;327(2):138–150. doi: 10.1001/jama.2021.23619 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 32.Idrees Z, Cancarevic I, Huang L. FDA-Approved Pharmacotherapy for Weight Loss Over the Last Decade. Cureus. Sep 2022;14(9):e29262. doi: 10.7759/cureus.29262 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 33.Novo Nordisk A/S: Semaglutide 2.4 mg reduces the risk of major adverse cardiovascular events by 20% in adults with overweight or obesity in the SELECT trial. https://www.novonordisk.com/news-and-media/news-and-ir-materials/news-details.html?id=166301
- 34.Welcome A Medications That May Increase Weight. Updated June 21, 2017. https://obesitymedicine.org/medications-that-cause-weight-gain/ [Google Scholar]
- 35.The Hormone Therapy Position Statement of The North American Menopause Society” Advisory P. The 2022 hormone therapy position statement of The North American Menopause Society. Menopause. Jul 1 2022;29(7):767–794. doi: 10.1097/GME.0000000000002028 [DOI] [PubMed] [Google Scholar]
- 36.Shrank WH, Patrick AR, Brookhart MA. Healthy user and related biases in observational studies of preventive interventions: a primer for physicians. J Gen Intern Med. May 2011;26(5):546–50. doi: 10.1007/s11606-010-1609-1 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 37.Stampfer MJ, Willett WC, Colditz GA, Rosner B, Speizer FE, Hennekens CH. A prospective study of postmenopausal estrogen therapy and coronary heart disease. N Engl J Med. Oct 24 1985;313(17):1044–9. doi: 10.1056/NEJM198510243131703 [DOI] [PubMed] [Google Scholar]
- 38.Rossouw JE, Anderson GL, Prentice RL, et al. Risks and benefits of estrogen plus progestin in healthy postmenopausal women: principal results From the Women’s Health Initiative randomized controlled trial. JAMA. Jul 17 2002;288(3):321–33. doi: 10.1001/jama.288.3.321 [DOI] [PubMed] [Google Scholar]
- 39.Hulley S, Grady D, Bush T, et al. Randomized trial of estrogen plus progestin for secondary prevention of coronary heart disease in postmenopausal women. Heart and Estrogen/progestin Replacement Study (HERS) Research Group. JAMA. Aug 19 1998;280(7):605–13. doi: 10.1001/jama.280.7.605 [DOI] [PubMed] [Google Scholar]
- 40.Michels KB, Manson JE. Postmenopausal Hormone Therapy in the 21st Century: Reconciling Findings from Observational Studies and Randomized Clinical Trials. In: Lobo RA, ed. Treatment of the Postmenopausal Woman. Academic Press; 2007:619–626. [Google Scholar]
- 41.Gleason CE, Dowling NM, Friedman E, Wharton W, Asthana S. Using predictors of hormone therapy use to model the healthy user bias: how does healthy user status influence cognitive effects of hormone therapy? Menopause. May 2012;19(5):524–33. doi: 10.1097/gme.0b013e318238ff2c [DOI] [PMC free article] [PubMed] [Google Scholar]
- 42.Stanford FC, Cena H, Biino G, et al. The association between weight-promoting medication use and weight gain in postmenopausal women: findings from the Women’s Health Initiative. Menopause. Oct 2020;27(10):1117–1125. doi: 10.1097/GME.0000000000001589 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 43.Chyu L, Upchurch DM. A Longitudinal Analysis of Allostatic Load among a Multi-Ethnic Sample of Midlife Women: Findings from the Study of Women’s Health Across the Nation. Women’s Health Issues. May-Jun 2018;28(3):258–266. doi: 10.1016/j.whi.2017.11.002 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 44.Abdulnour J, Doucet E, Brochu M, et al. The effect of the menopausal transition on body composition and cardiometabolic risk factors: a Montreal-Ottawa New Emerging Team group study. Menopause. Jul 2012;19(7):760–7. doi: 10.1097/gme.0b013e318240f6f3 [DOI] [PubMed] [Google Scholar]
- 45.Ogden CL, Carroll MD, Curtin LR, McDowell MA, Tabak CJ, Flegal KM. Prevalence of overweight and obesity in the United States, 1999–2004. JAMA. Apr 5 2006;295(13):1549–55. doi: 10.1001/jama.295.13.1549 [DOI] [PubMed] [Google Scholar]
- 46.Hales CM, Carroll MD, Fryar CD, Ogden CL. Prevalence of Obesity and Severe Obesity Among Adults: United States, 2017–2018. NCHS Data Brief. Feb 2020;(360):1–8. [PubMed] [Google Scholar]
- 47.Davis SR, Castelo-Branco C, Chedraui P, et al. Understanding weight gain at menopause. Climacteric. Oct 2012;15(5):419–429. doi: 10.3109/13697137.2012.707385 [DOI] [PubMed] [Google Scholar]
- 48.Barati M, Akbari-Heidari H, Samadi-Yaghin E, Jenabi E, Jormand H, Kamyari N. The factors associated with the quality of life among postmenopausal women. BMC Womens Health. May 18 2021;21(1):208. doi: 10.1186/s12905-021-01361-x [DOI] [PMC free article] [PubMed] [Google Scholar]
- 49.Lagro-Janssen A, Knufing MW, Schreurs L, van Weel C. Significant fall in hormone replacement therapy prescription in general practice. Fam Pract. Aug 2010;27(4):424–9. doi: 10.1093/fampra/cmq018 [DOI] [PubMed] [Google Scholar]
- 50.Gass ML, Stuenkel CA, Utian WH, et al. Use of compounded hormone therapy in the United States: report of The North American Menopause Society Survey. Menopause. Dec 2015;22(12):1276–84. doi: 10.1097/GME.0000000000000553 [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
Supplemental Table 1. Baseline Demographic, Social, and Clinical Characteristics of Women on High Dose a of Semaglutide by HT Use (n=73)
a High dose of semaglutide was defined as a dose of 1.7 to 2.4 mg weekly.
Continuous data are summarized as mean ± SD, unless noted otherwise. Categorical data are summarized as frequency and percentage.
Abbreviations used: HT, With Hormone Therapy; IQ, Interquartile Range; no-HT, Without Hormone Therapy; SD, Standard Deviation; SQ, Subcutaneous.
All P values <0.05 are considered significant.
Supplemental Table 2. Changes in Fasting Glucose, HbA1c, Lipid Profile, and Blood Pressure by HT Use in All Women (n=106)
Abbreviations used: DBP, Diastolic Blood Pressure; HbA1c, Glycosylated Hemoglobin A1c; HDL, High Density Lipoprotein; HT, With Hormone Therapy; LDL, Low Density Lipoprotein; no-HT, Without Hormone Therapy; SBP, Systolic Blood Pressure; SD, Standard Deviation.
All P values <0.05 are considered significant.
Supplemental Table 3. Changes in Fasting Glucose, HbA1c, Lipid Profile, and Blood Pressure by HT Use in Women on High Dose a of Semaglutide (n=73)
a High dose of semaglutide was defined as a dose of 1.7 to 2.4 mg weekly.
Abbreviations used: DBP, Diastolic Blood Pressure; HbA1c, Glycosylated Hemoglobin A1c; HDL, High Density Lipoprotein; HT, With Hormone Therapy; LDL, Low Density Lipoprotein; no-HT, Without Hormone Therapy; SBP, Systolic Blood Pressure; SD, Standard Deviation.
All P values <0.05 are considered significant.
Supplemental Figure 1. A. Total body Weight Loss Percentage (TBWL%) at 3, 6, 9, and 12 Months in Women with HT Use with Oral vs Transdermal Estrogen; B. TBWL% at 3, 6, 9, and 12 Months in Women with HT Use With vs Without Progesterone Use.
Abbreviations used: HT, With Hormone Therapy; no-HT, Without Hormone Therapy; OE, Oral Estrogen; P+, With Progesterone Use; P-, Without Progesterone Use; TBWL, Total Body Weight Loss; TE, Transdermal Estrogen.
Data in the figures is presented as means.