

Abstract
Background:
Kawasaki disease (KD) and Multisystem Inflammatory Syndrome in Children (MIS-C) associated with COVID-19 show clinical overlap and both lack definitive diagnostic testing, making differentiation challenging. We sought to determine how cardiac biomarkers might differentiate KD from MIS-C.
Methods:
The International Kawasaki Disease Registry enrolled contemporaneous KD and MIS-C pediatric patients from 42 sites from January 2020 through June 2022. The study population included 118 KD patients who met American Heart Association KD criteria and compared them to 946 MIS-C patients who met 2020 Centers for Disease Control and Prevention case definition. All included patients had at least one measurement of amino-terminal prohormone brain natriuretic peptide (NTproBNP) or cardiac troponin I (TnI), and echocardiography. Regression analyses were used to determine associations between cardiac biomarker levels, diagnosis, and cardiac involvement.
Results:
Higher NTproBNP (≥1500 ng/L) and TnI (≥20 ng/L) at presentation were associated with MIS-C versus KD with specificity of 77 and 89% respectively. Higher biomarker levels were associated with shock and intensive care unit admission; higher NTproBNP was associated with longer hospital length of stay. Lower left ventricular ejection fraction, more pronounced for MIS-C, was also associated with higher biomarker levels. Coronary artery involvement was not associated with either biomarker.
Conclusions:
Higher NTproBNP and TnI levels are suggestive of MIS-C versus KD and may be clinically useful in their differentiation. Consideration might be given to their inclusion in the routine evaluation of both conditions.
Keywords: Kawasaki disease (KD), Multisystem Inflammatory Syndrome in Children (MIS-C), Cardiac biomarkers, Amino-terminal prohormone brain natriuretic peptide (NTproBNP), Troponin I (TnI)
Introduction:
Kawasaki disease (KD) and Multisystem Inflammatory Syndrome in Children (MIS-C) associated with COVID-19 show considerable clinical overlap, often making differentiation challenging. KD is an acute systemic vasculitis, typically affecting children under 5 years of age, with potential for coronary artery aneurysms [1]. There is no diagnostic test for KD; rather, the American Heart Association (AHA) criteria for diagnosis requires fever for at least 5 days, combined with at least 4 of 5 clinical findings (rash, conjunctivitis, oral mucosa changes, palmar/plantar erythema, and cervical adenopathy) [1]. Atypical or incomplete KD, without fulfillment of classic diagnostic criteria, often places patients at increased risk for cardiovascular sequelae due to delayed or missed treatment [2].
In Spring 2020, reports emerged of children presenting with a multisystem inflammatory condition with “KD-like” features, following or concurrent to the novel SARS-CoV-2 infection, which became known as MIS-C [3, 4]. Despite clinical similarities to KD, MIS-C behaved differently to deserve development of its own case definition and diagnostic criteria [5, 6]. Like KD, MIS-C lacks a definitive diagnostic test, and has a range of clinical presentations and cardiovascular involvement.
Cardiac biomarkers, including amino-terminal prohormone brain natriuretic peptide (NTproBNP), and cardiac troponin I (TnI), are utilized in the assessment of congestive heart failure or cardiac dysfunction [7–10]. Studies of the role of cardiac biomarkers in the diagnosis and management of KD have shown variable results [11–16]. Abnormal cardiac biomarkers have been noted in patients with MIS-C and may help differentiate this from other diseases [17–23]. Prior studies have compared cardiac biomarker levels in MIS-C cohorts to non-contemporaneous KD cohorts [24], and have shown that MIS-C patients tend to have higher levels. A single center, small contemporaneous study supported the same conclusion [19]. Therefore, using data from a large, prospective, multicenter, international cohort of contemporaneous KD and MIS-C patients, we sought to determine the utility of cardiac biomarkers in differentiating KD versus MIS-C, and their relationship to clinical features.
Methods:
Study Design and Population
The International Kawasaki Disease Registry (IKDR) originated in 2013 with the aim of determining factors associated with outcomes for patients who had coronary artery aneurysms following KD [25]. In response to the initial reports of MIS-C and its similarities to KD, the IKDR began prospectively enrolling acute KD and MIS-C patients into an observational, multi-center, international cohort study. From January 1, 2020, through June 30, 2022, the IKDR enrolled 2903 contemporaneous KD (both with complete or incomplete clinical features), MIS-C, and acute COVID-19 patients <21 years of age from 42 sites. For the purposes of the current analysis, the study population included acute KD patients as diagnosed by the contributing site and confirmed by verification of AHA diagnostic criteria [1], together with documented evidence of no prior SARS-CoV-2 infection to ensure that no MIS-C cases were mis-categorized as KD. MIS-C patients were likewise included as diagnosed by the contributing site and confirmed by verification of 2020 CDC criteria [6], with documented evidence of prior SARS-CoV-2 infection (test-confirmed household exposure, positive PCR, or positive serology). Included patients had at least one measurement of NTproBNP or TnI (the most obtained biomarkers) and echocardiogram performed. See Figure 1.
Figure 1.
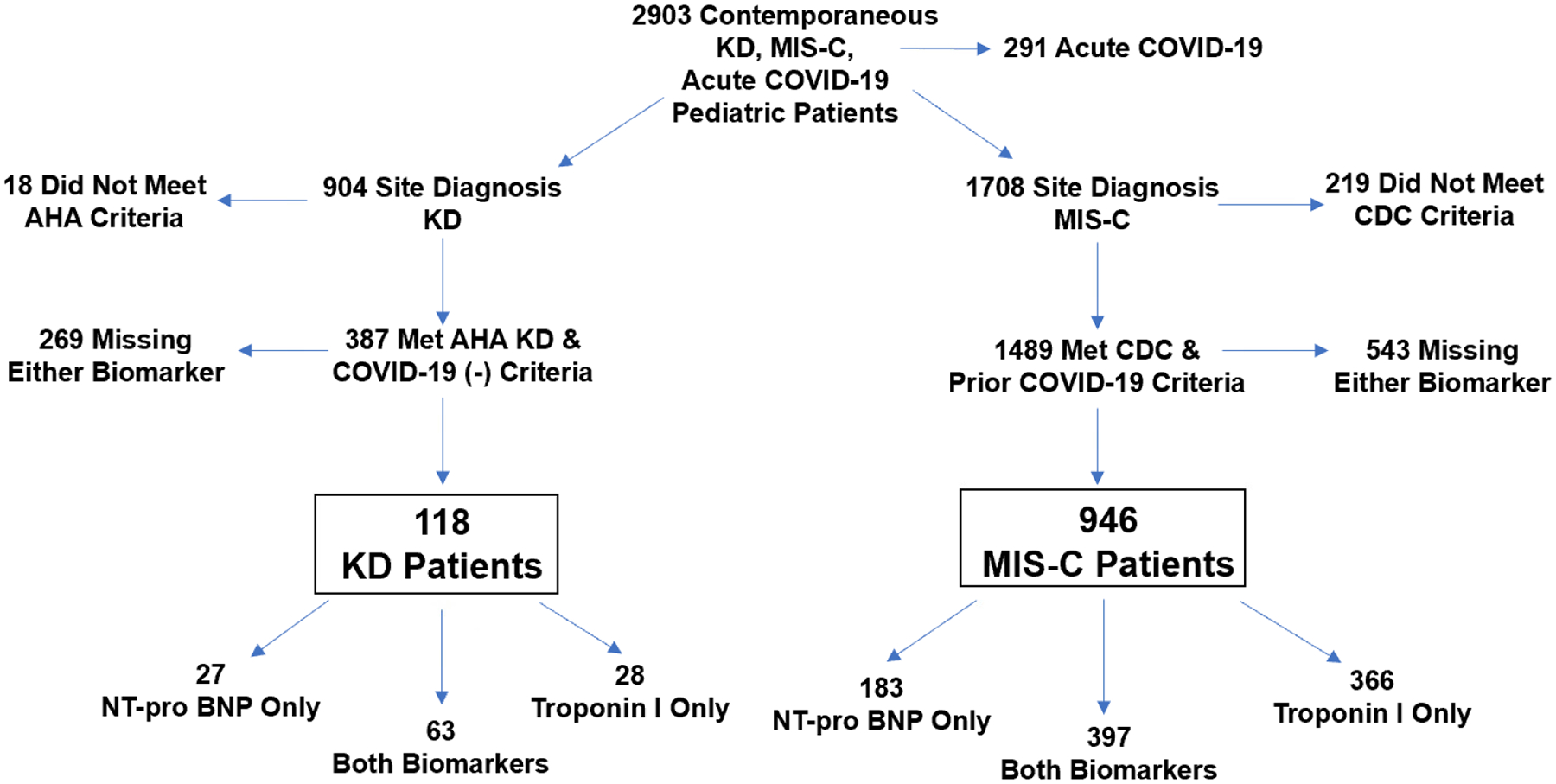
Inclusion and Exclusion Criteria
AHA: American Heart Association, CDC: Centers for Disease Control and Prevention, KD: Kawasaki disease, MIS-C: Multisystem Inflammatory Syndrome in Children, NTproBNP: amino-terminal prohormone brain natriuretic peptide
Data Coordinating Center
The IKDR Data Coordinating Centre (DCC) is located at the Hospital for Sick Children in Toronto, Canada and maintains local research ethics board approval. All participating sites have data-sharing agreements in place with the DCC and obtain and maintain local institutional review board’s approval for their site’s participation. All patients and parents either provided written informed consent/assent or data were submitted with an approved waiver of consent, as per the local institutional review board requirements. All data were submitted and maintained without patient identifiers, and standard data security/confidentiality measures were maintained. The IKDR is governed by bylaws and a steering committee.
Measurements
Participating sites extracted data from their medical records including patient demographics, clinical features and details of the clinical course including deidentified reports of echocardiogram. Serial laboratory findings were submitted directly to the DCC for centralized data entry into a secure Research Electronic Data Capture database maintained by the IKDR DCC. Values for serial measures of NTproBNP and TnI (not high sensitivity) were entered. Sites submitted deidentified copies of echocardiogram reports, and DCC staff abstracted the relevant variables. All entered data were reviewed by the DCC. Queries were sent to the sites for clarifications, and all queries were resolved prior to patient inclusion in the data analyses. Cardiac biomarker levels were identified at presentation and at peak where available, and echocardiographic variables included the lowest left ventricular ejection fraction (LVEF) and peak coronary artery Z scores.
Data Analysis
Data were described as frequencies, medians with values at the 25th and 75th percentiles, and means with standard deviation as appropriate to the level of measurement and the distribution of values for a given variable. KD and MIS-C patients were compared using Fisher’s Exact Test and Mantel-Hazel chi-squared analysis, Student’s t-test, and Kruskal-Wallis ANOVA. The distribution of values of cardiac biomarkers was highly skewed, so normalizing natural logarithmic transformation was applied to the biomarker levels before analysis. Multiple imputation of missing values of independent variables was performed before multivariable linear regression analyses to determine factors associated with cardiac biomarker levels (threshold for missingness for inclusion <25%). Regression models were adjusted for diagnosis, age (due to biomarker variance with age), and creatinine (due to renal clearance of biomarkers) at presentation, and then explored for associations of biomarkers with clinical presentation, laboratory values and cardiac involvement. Receiver operating curves (ROC) were used to determine biomarker cut points differentiating KD versus MIS-C. SAS statistical software Version 9.4 (Cary, NC) was used for analyses with p<0.05 set as the threshold for statistical significance.
Results:
Demographics, Clinical Features, and Treatment of KD versus MIS-C Patients
The study population included 118 acute KD and 946 MIS-C contemporaneous patients from Canada, Chile, Egypt, India, Italy, Mexico, Spain, and the United States. Patient characteristics are outlined in Table 1. Both KD and MIS-C patients showed a similar predominance of males to females. East Asian ethnicity was significantly greater in the KD group, which Black ethnicity was significantly greater in the MIS-C group. KD patients were younger and had lower body mass index Z-score (WHO algorithms).
Table 1.
Characteristics of Patients with KD versus MIS-C
| Variable | N | KD | N | MIS-C | P value |
|---|---|---|---|---|---|
| Sex – Male | 118 | 74 (63) | 946 | 574 (6) | 0.67 |
| Age at presentation (years) | 118 | 2.5 (1.1, 4.3) | 946 | 8.9 (5.4, 12.5) | <0.001 |
| Body mass index z-score | 111 | 0.03 (−0.60, 1.20) | 908 | 0.7 (−0.2, 1.6) | <0.001 |
| Ethnicity: | 79 | 624 | |||
| Black | 6 (8) | 141 (23) | 0.002 | ||
| White | 28 (35) | 237 (38) | 0.67 | ||
| East Asian | 14 (18) | 3 (0.5) | <0.001 | ||
| South Asian | 7 (9) | 18 (3) | 0.007 | ||
| Arabic | 3 (4) | 28 (4) | 0.78 | ||
| Hispanic | 23 (29) | 197 (32) | 0.66 | ||
| Duration of symptom onset prior to admission (days) | 117 | 5 (4, 7) | 917 | 4 (3, 6) | 0.003 |
| Shock | 118 | 3 (3) | 943 | 296 (3) | <0.001 |
| Renal dysfunction | 118 | 1.0 (0.8) | 942 | 80 (8) | 0.004 |
| Respiratory support | 118 | 4 (4) | 945 | 357 (38) | <0.001 |
| Intensive care unit admission | 118 | 8 (7) | 946 | 531 (56) | <0.001 |
| Inotropic medication | 118 | 4 (3) | 945 | 371 (39) | <0.001 |
| Intravenous immunoglobulin | 118 | 111 (94) | 946 | 894 (95) | 0.85 |
| Intravenous steroids | 118 | 25 (21) | 944 | 736 (78) | <0.001 |
| Oral steroids | 118 | 45 (38) | 940 | 612 (65) | <0.001 |
| Total hospital length of stay (days) | 118 | 5 (4,6) | 946 | 7 (5,9) | <0.001 |
| Creatinine (umol/L) | 72 | 30 (22, 39) | 862 | 49 (35, 65) | <0.001 |
| NTproBNP (ng/L) | 90 | 370 (162, 1230) | 580 | 1944 (469, 8420) | <0.001 |
| TnI (ng/L) | 91 | <10 (<10, <10) | 763 | 15 (4, 83) | <0.001 |
Data are presented as n (%) for categorical and median [IQR: interquartile range (25th and 75th percentiles)] for continuous variables. Lab values were obtained at presentation.
KD: Kawasaki disease, MIS-C: Multisystem Inflammatory Syndrome in Children, ng/L: nanograms per liter, NTproBNP: amino-terminal prohormone brain natriuretic peptide, TnI: troponin I, umol/L: micromoles per liter
While KD clinical features were also prevalent in MIS-C patients (418 had either 2 or 3 features and 124 had either 4 or 5 features), KD patients manifested a significantly greater number of KD clinical features (Figure 2). MIS-C patients were more likely to present with shock, renal dysfunction, require inotropic and respiratory support, and ICU admission. The MIS-C group tended to have a longer total duration of hospital stay (LOS). The groups did not differ regarding the use of intravenous immune globulin (IVIG) or anti-platelet therapies. Although infrequent, a greater proportion of MIS-C patients received additional forms of anticoagulation. MIS-C patients were also more likely to have received both intravenous and enteral steroid therapy.
Figure 2.
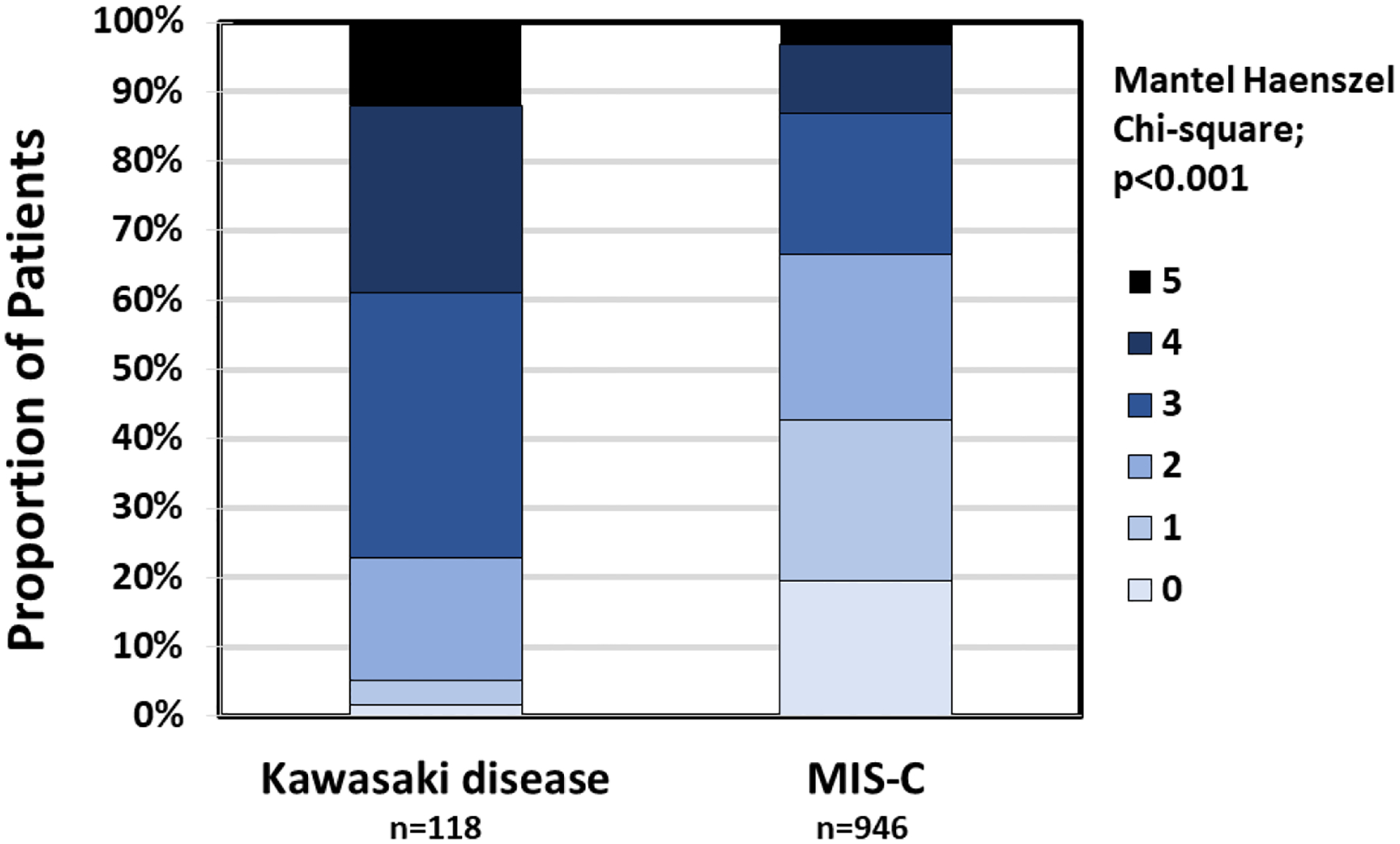
Number of KD Clinical Criteria Present for KD Versus MIS-C Patients
KD: Kawasaki disease, MIS-C: Multisystem Inflammatory Syndrome in Children
Cardiac Biomarker Distribution by Diagnosis
Figure 1 shows the number of patients within each diagnosis who had either NTproBNP or TnI or both at presentation. In the KD group, median NTproBNP was 370 ng/L; (IQR 162, 1230) and TnI was <10 ng/L; (IQR <10, <10). Among MIS-C patients, NTproBNP was 1944 ng/L; (IQR 469, 8420; p<0.001 versus KD) and TnI was 15.0 ng/L; (IQR 4.4, 83; p<0.001 versus KD) Table 1. Figures 3A and 3B show the distribution of the cardiac biomarkers (after natural logarithmic transformation given the non-normal distribution of values) by diagnosis. Baseline logNTproBNP and logTnI were weakly correlated (r=0.10; p=0.03). Both logNTproBNP and logTnI did not correlate with age (r=0.01, p=0.76; r=0.05, p=0.12; respectively), but higher levels of both correlated with higher creatinine levels (r=0.22, p<0.001; r=0.08, p=0.03; respectively).
Figure 3.
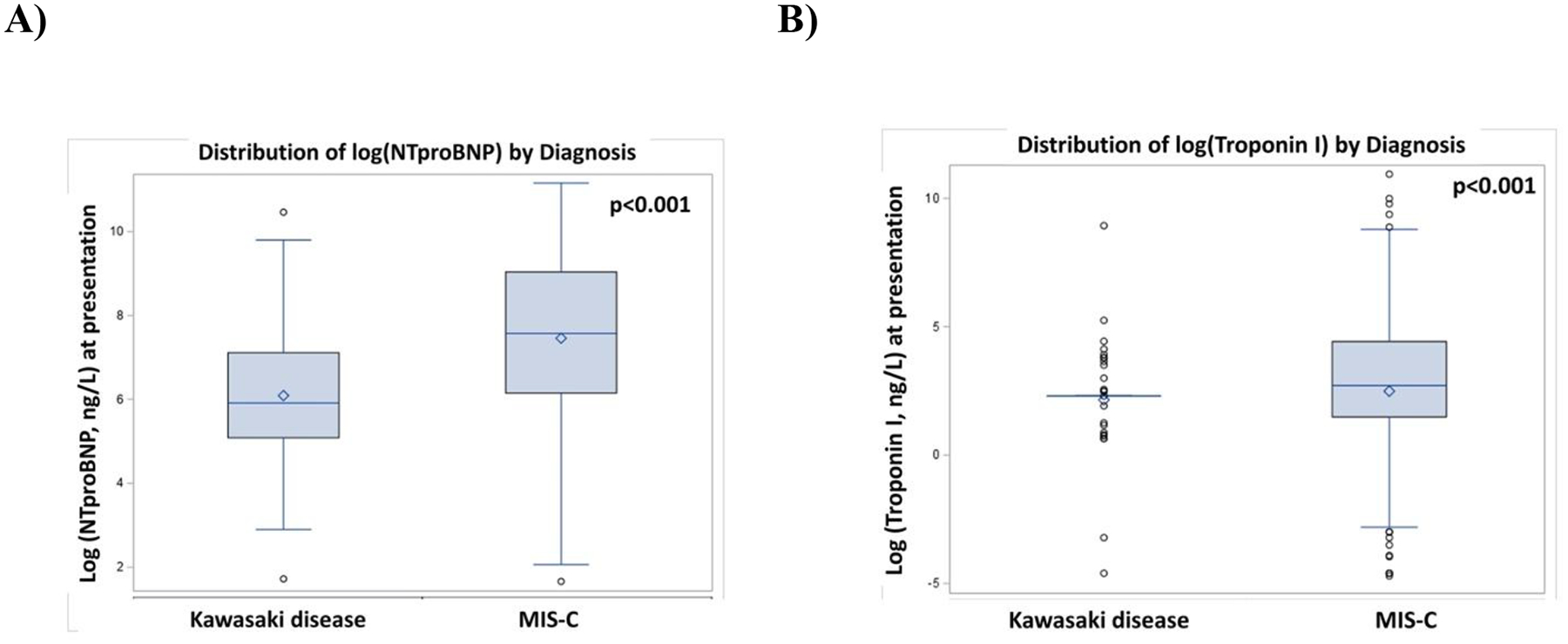
Distribution of Cardiac Biomarkers by Diagnosis: A) log(NTproBNP) and B) log(TnI) at Presentation
Box encloses the 25th to 75th percentiles with the line indicating the median and diamond the mean. Whiskers range from the maximum to minimum value within the fence, with circles indicating outliers.
log(NTproBNP): logarithmic transformation of amino-terminal prohormone brain natriuretic peptide, log(troponin I): logarithmic transformation of troponin I, MIS-C: Multisystem Inflammatory Syndrome in Children
Associations of Cardiac Biomarkers at Presentation with Clinical Findings
Higher logNTproBNP was associated with shock at presentation (Parameter Estimate [PE]1.26; Standard Error [SE] 0.17; p<0.001), ICU admission (PE 1.50; SE 0.14; p<0.001) and longer LOS (PE 0.044 per day; SE 0.010; p<0.001). Associations were not changed with adjustment for age, diagnosis, and creatinine level at presentation (data not shown).
Higher logTnI was associated with shock at presentation (PE 1.01; SE 0.22; p<0.001) and ICU admission (PE 0.68; SE 0.20; p<0.001), but not with longer LOS (PE −0.020 per day; SE 0.019; p=0.28). Again, associations were not changed with adjustment for age, diagnosis, and creatinine at presentation (data not shown).
Associations of Cardiac Biomarkers at Presentation with Laboratory Values
Laboratory values at presentation that were independently associated with cardiac biomarkers were adjusted for diagnosis, age, and creatinine in multivariable models. Higher logNTproBNP was independently associated with higher white blood cell count, higher lymphocyte count, lower platelet count, lower albumin, lower sodium, higher chloride, and higher fibrinogen (Table 2A). After accounting for these laboratory values, a diagnosis of MIS-C (versus KD) continued to be associated with significantly higher levels of logNTproBNP. Higher levels of logTnI were independently associated higher alanine aminotransferase, international normalized ratio (INR), fibrinogen and lower lactate dehydrogenase, albeit with a lower model R2 (Table 2B).
Table 2A.
Laboratory Values at Presentation Independently Associated with Higher Baseline log(NTproBNP)*
| Variable | Unit | Parameter Estimate | Standard Error | P value |
|---|---|---|---|---|
| Intercept | 15.99 | 2.38 | ||
| Diagnosis of MIS-C (vs KD) | 1.00 | 0.22 | <0.001 | |
| Age at presentation | per year | −0.05 | 0.02 | 0.002 |
| Creatinine | per umol/L | 0.005 | 0.001 | <0.001 |
| White cell count | per x109/L | 0.07 | 0.01 | <0.001 |
| Lymphocytes | per x109/L | 0.09 | 0.04 | 0.03 |
| Platelets | per x109/L | −0.003 | 0.001 | <0.001 |
| Albumin | per g/L | −0.08 | 0.01 | <0.001 |
| Sodium | per mmol/L | −0.09 | 0.02 | <0.001 |
| Chloride | per mmol/L | 0.04 | 0.02 | 0.02 |
| Fibrinogen | per g/L | 0.09 | 0.04 | 0.02 |
From general linear regression model after multiple imputation of missing values of independent variables; diagnosis, age at presentation and creatinine at presentation are included as adjustment factors; Adjusted model R2 0.29
g/L: grams per liter, KD: Kawasaki disease, log(NTproBNP): logarithmic transformation of amino-terminal prohormone brain natriuretic peptide, MIS-C: Multisystem Inflammatory Syndrome in Children, mmol/L: millimoles per liter, umol/L: micromoles per liter
Table 2B.
Laboratory Values At Presentation Independently Associated with Higher Baseline log(TnI)*
| Variable | Unit | Parameter Estimate | Standard Error | P value |
|---|---|---|---|---|
| Intercept | −1.05 | 1.10 | ||
| Diagnosis of KD (vs MIS-C) | −0.24 | 0.43 | 0.59 | |
| Age at presentation | per year | −0.02 | 0.03 | 0.47 |
| Creatinine | per umol/L | −0.0005 | 0.0028 | 0.87 |
| Alanine aminotransferase | per U/L | 0.007 | 0.002 | 0.003 |
| International normalized ratio | per unit | 2.30 | 0.77 | 0.004 |
| Ferritin | per ug/L | 0.0002 | 0.0001 | 0.02 |
| Fibrinogen | per g/L | 0.22 | 0.08 | 0.005 |
| Lactate dehydrogenase | per U/L | −0.0016 | 0.0005 | <0.001 |
From general linear regression after multiple imputation of missing values for independent variables; diagnosis, age at presentation and creatinine at presentation are included as adjustment factors; Adjusted model R2 0.07
KD: Kawasaki disease, log(TnI): logarithmic transformation of troponin I, MIS-C: Multisystem Inflammatory Syndrome in Children, U/L: units per liter, umol/L: micromoles per liter, ug/L: micrograms per liter
Association of Cardiac Biomarkers at Presentation and Ventricular Function
Lowest LVEF from all timepoints was significantly lower for MIS-C versus KD (55±10% versus 63±6%, respectively; p<0.001), with a higher proportion having lowest LVEF <55% (43% versus 4%, respectively; p<0.001). After adjusting for diagnosis, age, and creatinine in a multivariable general linear regression model, having lower LVEF was significantly associated with higher baseline logNTproBNP (PE −1.75, SE 0.21; p<0.001) and higher baseline logTnI (PE −0.27, SE 0.12; p=0.02).
Association of Cardiac Biomarkers at Presentation and Coronary Artery Abnormalities
Maximum coronary artery Z-score (of any branch and at any timepoint, i.e., “worst”) was significantly greater for KD versus MIS-C (median +1.36 [IQR, +0.77, +2.14] versus +1.23 [+0.38, +1.91]; p<0.05). After adjusting for diagnosis, age and creatinine in a general linear regression model, maximum coronary artery Z-score was not associated with baseline logNTproBNP (PE 0.041, SE 0.044; p=0.36) or baseline logTnI (PE −0.028, SE 0.023; p=0.23).
Predictive Characteristics of Cardiac Biomarkers at Presentation for Diagnosis
Using ROC curves derived from univariable logistic regression (Figures 4A and 4B), baseline TnI ≥10 ng/L (c-statistic 0.65) predicted MIS-C versus KD with a sensitivity of 58% and specificity of 77%; TnI ≥20 ng/L predicted MIS-C versus KD with 44% sensitivity and 89% specificity. Baseline NTproBNP ≥500 ng/L (c-statistic 0.71) predicted MIS-C versus KD with a sensitivity of 74% and specificity of 54%, ≥1000 ng/L 61% and 72%, and ≥1500 ng/L 56% and 77%. The c-statistic improved to 0.74 with both biomarkers at presentation together, and to 0.78 with both biomarkers at peak levels.
Figure 4.
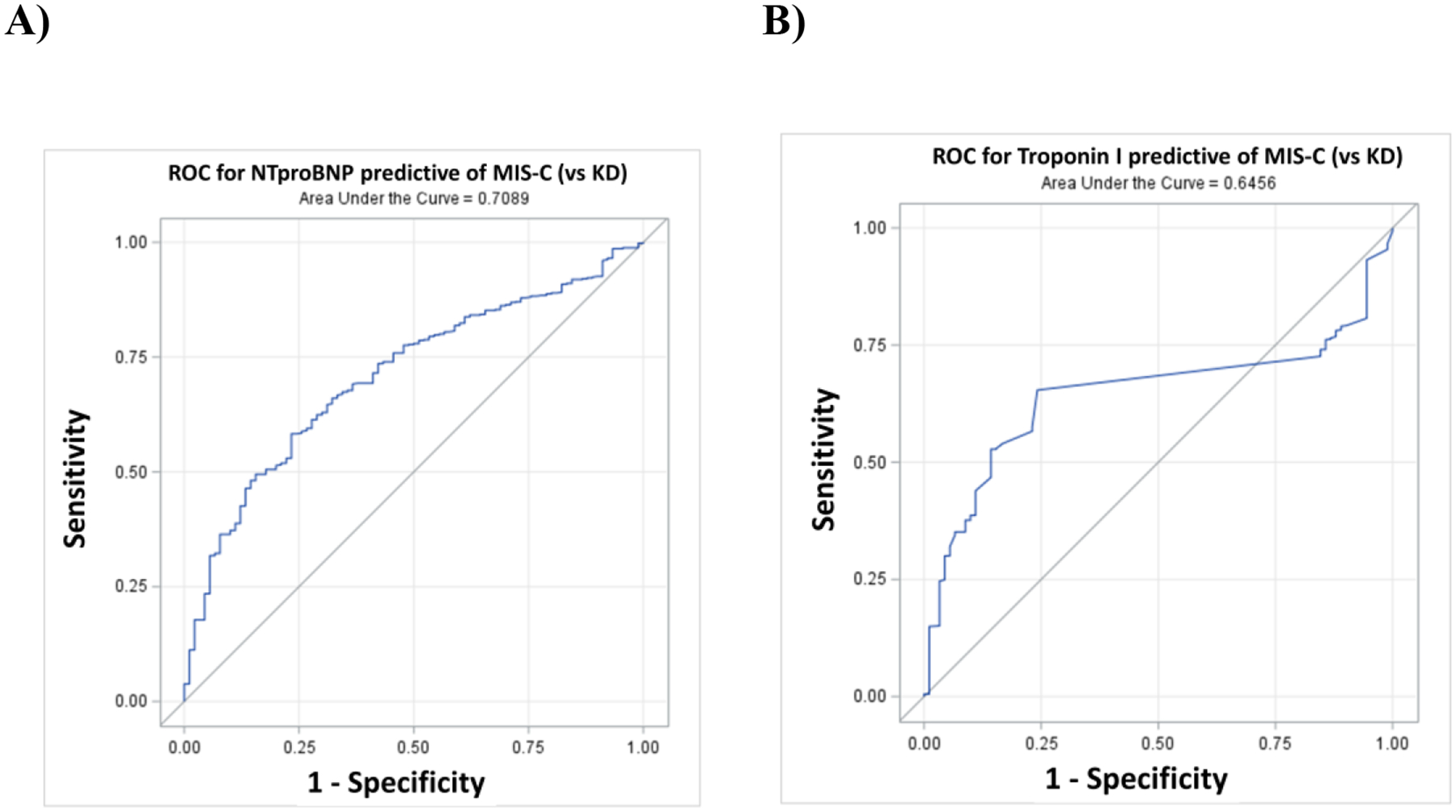
Receiver Operating Characteristic Curves Predicting MIS-C (vs KD) for A) NTpro BNP and B) TnI at Presentation
KD: Kawasaki Disease, MIS-C: Multisystem Inflammatory Syndrome in Children, NTproBNP: amino-terminal prohormone brain natriuretic peptide, ROC: receiver operating characteristic, TnI: troponin I
Discussion:
While KD and MIS-C share phenotypic similarities, the diagnoses have different risks of cardiovascular involvement and clinical decompensation. Both, however, are clinical diagnoses that lack definitive diagnostic testing. This presents a clinical conundrum, as there is limited ability to differentiate the diagnoses, especially for patients with atypical presentations. Differentiation will be more difficult, as prior SARS-CoV-2 infection and vaccination may confound the fulfillment of clinical diagnostic criteria.
NTproBNP is upregulated by myocardial stress imposed by pressure or volume overload and cardiac dysfunction [26], and is typically used for the diagnosis and risk stratification of congestive heart failure. TnI is a cardiac myocyte-associated protein that is released into the blood circulation during cell injury, particularly in the setting of myocardial ischemia [9, 27], but can also be used to detect cardiac injury due to inflammatory processes [26]. The greater elevation in both cardiac biomarkers observed in MIS-C may offer insight into the difference in pathogenesis between KD and MIS-C. Systolic dysfunction observed in MIS-C may be a function of myocardial stress due to excess wall tension and cardiac injury, in combination with myocardial inflammation. The observed lack of association of cardiac biomarkers with coronary artery involvement may indicate that their development is not solely associated with myocyte stress and/or inflammation [22]. Thus, the predictive value of cardiac biomarkers is in association with ventricular function and not with coronary artery involvement.
A meta-analysis published in 2022 comparing several non-cardiac and cardiac biomarker characteristics and treatment of pre-pandemic KD versus MIS-C patients reported that MIS-C patients had higher cardiac biomarker levels, including NTproBNP and TnI, and worse LV systolic function [24]. It is important to note the distinction that these studies were single-center or single-country studies, supplementing the KD cohort with pre-pandemic data, thus the comparison is not fully contemporaneous. More recently, Fridman et al published a small, single-center study comparing MIS-C patients with contemporaneous KD patients, showing that greater elevations in NTproBNP and TnI were in fact associated with MIS-C; neither biomarker was associated with coronary artery abnormalities [19].
The goal of our larger, contemporaneous study was to determine if these observations of higher cardiac biomarkers associated with MIS-C could be applied to predicting KD versus MIS-C. We showed that NTproBNP ≥1500 ng/L or TnI ≥20 ng/L at presentation was predictive of MIS-C with reasonable specificity. Advantageously, this study includes a large and diverse population of contemporaneous KD and MIS-C patients, thus, the findings of our study may offer greater generalizability. We also confirm important clinical similarities and differences between KD and MIS-C patients using a contemporaneous, rather than historical, cohort with MIS-C patients tending to be older and having greater clinical severity. NTproBNP and TnI may be useful in differentiating MIS-C from KD, although they should be interpreted in the context of the larger clinical picture due to their somewhat limited sensitivity and specificity.
We recommend routine measurement of cardiac biomarkers for all suspected KD and MIS-C cases. As the outcomes differ and MIS-C tends to be more severe acutely [20], it is important to make the distinction between KD (particularly atypical forms of KD) and MIS-C early in the clinical course to better tailor management [21]. For example, recommended treatment for MIS-C includes IVIG and steroids [28], whereas current KD guidelines typically recommend only IVIG [1]. Utilization of cardiac biomarkers in the differentiation of KD versus MIS-C may thus help clinicians in management decisions and anticipating clinical course [19, 29]. For example, one might apply these cutoffs to a likely KD patient that does not have sufficient SARS-CoV-2 ‘negative’ criteria.
Limitations
The results of this study should be interpreted in the context of the following limitations. This is a registry-based study and, thus, limited to the variables collected and subject to incomplete data entry and selection bias. For example, the cardiac biomarkers obtained and thus analyzed in the KD cohort were likely obtained in unclear or clinically severe KD cases and may not be representative of all KD cases. The KD and MIS-C groups were of unbalanced size. Our study methodology is prone to information bias due to heterogeneity in the laboratory methods, such as assay methods and range of cardiac biomarker values, between sites. While we did not have details of the specific assay method / equipment used for tests performed at the various sites, assessment of NTproBNP is standardized with less variation. There may be more variation regarding TnI. Note that our study analysis was based on TnI and not high sensitivity TnI (as there were few values of this). Nonetheless, the same method would be used at a site for both KD and MIS-C patients, which minimizes bias. Additionally, the range of elevated values is not subtle, and would be well outside above the upper limit of normal, regardless of lab methods used. It is important to note that this study focused on associations, rather than specific cardiac biomarker ranges, which also minimizes the influence of this bias. An additional source of inter-center variability is the timing of blood draw to obtain cardiac biomarkers as values differ by illness day. While the cardiac biomarkers used for analysis were obtained at presentation, it is not known on what day of illness the patient presented and samples were obtained. Additionally, timing of obtaining samples with respect to IVIG administration was not collected. We do, however, know that these labs were obtained at the time of presentation and hence the majority would likely be before administration of any immunomodulatory therapy. The c-statistic for the cardiac biomarkers is reasonable, and while reassuring in indicating the ability to differentiate MIS-C versus KD, nonetheless is imperfect. The use of cardiac biomarkers in isolation might lead to misclassification and should be viewed in the context of other clinical findings. It has been reported that NTproBNP in the setting of inflammatory disease may be an acute phase reactant, suggesting that it may be a marker of general inflammation, instead of a specific cardiac marker [30, 31]. Despite these limitations, we believe that this cohort with well-characterized contemporaneous KD and MIS-C patients is a unique strength, supporting the reliability and generalizability of our findings.
Conclusions:
This study demonstrated that higher NTproBNP and TnI levels at presentation were associated with the diagnosis of MIS-C versus KD with reasonable specificity. Thus, NTproBNP and TnI may be an additional marker differentiating MIS-C from KD, although the results should be interpreted in the context of the larger clinical picture. Higher cardiac biomarker levels were also associated with an increased likelihood of shock and ICU admission. Ventricular dysfunction, more common in MIS-C, was associated with higher cardiac biomarker levels, while coronary artery involvement, more common in KD, was not associated with either cardiac biomarker, presumably because of differences in the pathophysiological mechanisms of the two diseases. As evidence of associated or prior SARS-CoV-2 infection becomes more challenging to determine, as well as ongoing occurrence of KD cases with atypical or incomplete presentation, routine assessment of cardiac biomarkers in all suspected KD and MIS-C patients may be useful.
Acknowledgements:
The team of the IKDR Coordinators and Primary Investigators from all participating centers: Abdelwahab Ahmed (Pediatric Cardiology Division, Department of Pediatrics, Ain-Shams University, Cairo, Egypt), Jessica Bainton (Labatt Family Heart Centre, The Hospital for Sick Children, Department of Pediatrics, University of Toronto, Toronto, ON, Canada), Annette L. Baker (Boston Children’s Hospital, Harvard Medical School, Boston, MA, USA), Mikayla A. Beckley (Seattle Children’s Research Institute, Seattle, WA, USA), Bailey Bernknopf (Labatt Family Heart Centre, The Hospital for Sick Children, Department of Pediatrics, University of Toronto, Toronto, ON, Canada), Jacobo Borovoy-Gurwitz (Hospital Angeles Lomas, Huixquilucan, Mexico), Jane C. Burns (University of California San Diego/Rady Children’s Hospital San Diego, CA USA), Ana Caro Barri (Hospital 12 de Octubre (Imas12), Madrid, Spain), Tanveer Collins (Labatt Family Heart Centre, The Hospital for Sick Children, Department of Pediatrics, University of Toronto, Toronto, ON, Canada), Amy Cooper (The Heart Center at Nationwide Children’s Hospital, Columbus, OH, USA), Jamie Cruz (Hospital 12 de Octubre (Imas12), Madrid, Spain), Catherine Dimes (The Heart Center at Nationwide Children’s Hospital, Columbus, OH, USA), Elías Duck-Hernández (Hospital Angeles Lomas, Huixquilucan, Mexico), Manar Elansary (Pediatric Cardiology Division, Department of Pediatrics, Ain-Shams University, Cairo, Egypt), Kevin G. Friedman (Boston Children’s Hospital, Harvard Medical School, Boston, MA, USA), Fiorentina Guida (Pediatric Emergency Unit, IRCCS Azienda Ospedaliero Universitaria di Bologna, Bologna, Italy), Jonathan Hazlewood (Labatt Family Heart Centre, The Hospital for Sick Children, Department of Pediatrics, University of Toronto, Toronto, ON, Canada), Ashley Herzberg (Phoenix Children’s Hospital, Phoenix, AZ, USA), Kelli Kaneta (Children’s Hospital of Los Angeles, Los Angeles, CA, USA), Katherine Kanwar (The Heart Center at Nationwide Children’s Hospital, Columbus, OH, USA), Jong Mi Ko (Johns Hopkins School of Medicine, Baltimore MD, USA), Rita Long (Johns Hopkins School of Medicine, Baltimore MD, USA), Simran Mahanta (Boston Children’s Hospital, Harvard Medical School, Boston, MA, USA), Sara Mahfouz (Pediatric Cardiology Division, Department of Pediatrics, Ain-Shams University, Cairo, Egypt), Irene Maulen-Radovan (Hospital Angeles Lomas, Huixquilucan, Mexico), Matteo Meli (Pediatric Emergency Unit, IRCCS Azienda Ospedaliero Universitaria di Bologna, Bologna, Italy), Sahar Mohamed (Kingston Health Science Centre, Kingston, ON, Canada), Deepthi G. Nair (Seattle Children’s Research Institute, Seattle, WA, USA), Divya Nandakumar (Kanchi Kamakoti Childs Trust Hospital, Chennai, India), Jane W. Newburger (Boston Children’s Hospital, Harvard Medical School, Boston, MA, USA), Martin Ogwuru (Kingston Health Science Centre, Kingston, ON, Canada), Sunita O’Shea (Labatt Family Heart Centre, The Hospital for Sick Children, Department of Pediatrics, University of Toronto, Toronto, ON, Canada), Susan S. Park (Phoenix Children’s Hospital, Phoenix, AZ, USA), Jade Porche (Phoenix Children’s Hospital, Phoenix, AZ, USA), Sulochana Putlibai (Kanchi Kamakoti Childs Trust Hospital, Chennai, India), Itzel Estefani Ríos-Olivares (Instituto Nacional de Pediatría, Mexico City, Mexico), Martha Rolland (Labatt Family Heart Centre, The Hospital for Sick Children, Department of Pediatrics, University of Toronto, Toronto, ON, Canada), Christina Hayden Rush (Children’s Hospital of Philadelphia, Philadelphia, PA, USA), Kristy Rutt (Banner Children’s at Desert Medical Center, Mesa, AZ, USA), Senthilnathan S. (Kanchi Kamakoti Childs Trust Hospital, Chennai, India), Seaher Sakha (Labatt Family Heart Centre, The Hospital for Sick Children, Department of Pediatrics, University of Toronto, Toronto, ON, Canada), Mina Sidhom (Pediatric Cardiology Division, Department of Pediatrics, Ain-Shams University, Cairo, Egypt), John Smythe (Kingston Health Science Centre, Kingston, ON, Canada), Samantha Stack (Phoenix Children’s Hospital, Phoenix, AZ, USA), Amullya Sudhakar (Kanchi Kamakoti Childs Trust Hospital, Chennai, India), Sharon Wagner-Lees (Children’s Hospital of Los Angeles, Los Angeles, CA, USA), Patricia Walter (Labatt Family Heart Centre, The Hospital for Sick Children, Department of Pediatrics, University of Toronto, Toronto, ON, Canada)
Sources of Funding:
This work was partially supported by Grant R61HD105591 from the Eunice Kennedy Shriver National Institute of Child Health & Human Development and the Office of the Director, National Institute of Health (OD). Its contents are solely the responsibility of the authors and do not necessarily represent the official views of the Eunice Kennedy Shriver National Institute of Child Health & Human Development or the Office of the Director, National Institute of Health (OD). Dr. Truong is supported by NIH OTA-21-015E, to study genetic risk factors for the development of MIS-C and more severe disease; and NIH/NHLBI OT2HL161847-01, to characterize the clinical spectrum of post-acute sequelae of COVID-19 (PASC), organ dysfunction in sub-phenotypes of PASC, and the underlying biological mechanisms. Dr. Portman is supported by R01 HL143130. Dr. Dahdah is supported by BoBeau Coeur funds for applied clinical research in pediatric cardiology. Dr. Dionne is supported by McCance Family Fund
*. Authors from the International Kawasaki Disease Registry (IKDR):
Mahmoud Alsalehi, MD (Kingston Health Science Centre, Kingston, ON, Canada), Jean A. Ballweg, MD (Helen DeVos Children’s Hospital, Grand Rapids, MI, USA), Benjamin T. Barnes, MD (Johns Hopkins School of Medicine, Baltimore MD, USA), Elizabeth Braunlin, MD, PHD (University of Minnesota, Minneapolis, MN, USA)
Ashley Buffone, MD (Division of Pediatric Cardiology, CHU Ste-Justine, University of Montreal, Montreal, QC, Canada), Juan Carlos Bustamante-Ogando, MD (Hospital Angeles Lomas, Huixquilucan, Mexico), Arthur J. Chang, MD (Jacobs School of Medicine and BioMedical Sciences, University at Buffalo, Buffalo, NY, USA), Nicolas Corral, MD (Childrens Hospital at Montefiore, Albert Einstein College of Medicine, Bronx, NY, USA), Heather Cowles, FNP-BC (New York Medical College/Maria Fareri Children’s Hospital at Westchester Medical Center, Valhalla, NY, USA), Paul Dancey, MD, FRCPC (Janeway Children’s Health and Rehabilitation Centre, Saint John’s, NL, Canada), Sarah D de Ferranti, MD, MPH (Boston Children’s Hospital, Harvard Medical School, Boston, MA, USA), Mona El Ganzoury, MD, PhD (Pediatric Cardiology Division, Department of Pediatrics, Ain-Shams University, Cairo, Egypt)
Matthew D. Elias, MD (Children’s Hospital of Philadelphia, Philadelphia, PA, USA), Nora Elsamman, MD, PhD (Pediatric Cardiology Division, Department of Pediatrics, Ain-Shams University, Cairo, Egypt), Elisa Fernández Cooke, MD, PhD (Hospital 12 de Octubre (Imas12), Madrid, Spain), Guillermo Larios Goldenberg, MD (Hospital Clínico UC-Christus, Pontificia Universidad Católica de Chile, Santiago, Chile), Michelle M. Grcic, APRN (The Heart Center at Nationwide Children’s Hospital, Columbus, OH, USA), Kevin C. Harris, MD, MHSc (Children’s Heart Centre, BC Children’s Hospital and University of British Columbia, Vancouver, BC, Canada), Pei-Ni Jone, MD (Children’s Hospital Colorado, University of Colorado Anschutz Medical Campus - Now affiliated with Lurie Children’s Hospital, Northwestern University Feinberg School of Medicine), Hidemi Kajimoto, MD, PhD (Seattle Children’s Research Institute, Seattle, WA, USA), Manaswitha Khare, MD (University of California San Diego/Rady Children’s Hospital San Diego, CA USA), Shelby Kutty, MD, PhD (Johns Hopkins School of Medicine, Baltimore MD, USA), Marcello Lanari, MD, PhD (Pediatric Emergency Unit, IRCCS Azienda Ospedaliero Universitaria di Bologna, Bologna, Italy), Daniel Mauriello, MD (Johns Hopkins All Children’s Hospital, Saint Petersburg, FL, USA), Kimberly E. McHugh, MD (Medical University of South Carolina, Charleston, SC, USA), Shae A. Merves, MD (Arkansas Children’s Hospital/University of Arkansas for Medical Sciences, Little Rock, AR, USA), Sindhu Mohandas, MD (Children’s Hospital of Los Angeles, Los Angeles, CA, USA), Tapas Mondal, MD (Division of Cardiology, Department of Pediatrics, McMaster University, Hamilton, ON, Canada), Joseph J. Pagano, MD, PhD (Division of Pediatric Cardiology, Department of Pediatrics, University of Alberta, Edmonton, AB, Canada), Deepa Prasad, MD (Banner Children’s at Desert Medical Center, Mesa, AZ, USA), Prasad Ravi, MD (Banner Children’s at Desert Medical Center, Mesa, AZ, USA), Arash A. Sabati, MD (Phoenix Children’s Hospital, Phoenix, AZ, USA), Anupam Sehgal, MBBS (Kingston Health Science Centre, Kingston, ON, Canada), Ashish Shah, MD, MBA (Johns Hopkins All Children’s Hospital, Saint Petersburg, FL, USA), Balasubramanian Sundaram, MD (Kanchi Kamakoti Childs Trust Hospital, Chennai, India), Belén Toral Vázquez, MD (Hospital 12 de Octubre (Imas12), Madrid, Spain), Adriana H. Tremoulet, MD (University of California San Diego/Rady Children’s Hospital San Diego, CA USA), Aishwarya Venkataraman, MRCPCH (Kanchi Kamakoti Childs Trust Hospital, Chennai, India), Robert W.Lowndes, (Children’s National Hospital, The George Washington University School of Medicine & Health Sciences, Washington, DC, USA), Laurence Watelle, MD (Department of pediatrics, Université de Sherbrooke, and Centre de Recherche du Centre Hospitalier Universitaire de Sherbrooke, Sherbrooke, QC, Canada), Marco Antonio Yamazaki-Naksahimada, MD (Instituto Nacional de Pediatría, Mexico City, Mexico), Anji T. Yetman, MD (Children’s Hospital and Medical Center. University of Nebraska Medical Center, Omaha, NE USA), Varsha Zadokar, MBBS (Nemours Children’s Hospital, Wilmington, DE, USA)
Footnotes
Disclosures: Dr. Truong is an MPI on an NHLBI Pediatric Heart Network-Pfizer Partnership to Study COVID-19 Vaccine-Associated Myocarditis. Dr. Harahsheh serves as a scientific advisory board member of OP2 DRUGS (“OP2”) but this advisory position has no relevant disclosures for this manuscript.
References:
- 1.McCrindle BW, et al. , Diagnosis, Treatment, and Long-Term Management of Kawasaki Disease: A Scientific Statement for Health Professionals From the American Heart Association. Circulation, 2017. 135(17): p. e927–e999. [DOI] [PubMed] [Google Scholar]
- 2.Newburger JW, et al. , Diagnosis, treatment, and long-term management of Kawasaki disease: a statement for health professionals from the Committee on Rheumatic Fever, Endocarditis and Kawasaki Disease, Council on Cardiovascular Disease in the Young, American Heart Association. Circulation, 2004. 110(17): p. 2747–71. [DOI] [PubMed] [Google Scholar]
- 3.Dufort EM, et al. , Multisystem Inflammatory Syndrome in Children in New York State. N Engl J Med, 2020. 383(4): p. 347–358. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Feldstein LR, et al. , Characteristics and Outcomes of US Children and Adolescents With Multisystem Inflammatory Syndrome in Children (MIS-C) Compared With Severe Acute COVID-19. JAMA, 2021. 325(11): p. 1074–1087. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Organization, W.H. Multisystem Inflammatory Syndrome in Children and Adolescents with COVID-19. 2020. May 15 2020 [cited 2023 January 1]; Scientific Brief]. Available from: https://www.who.int/news-room/commentaries/detail/multisystem-inflammatory-syndrome-in-children-and-adolescents-with-covid-19.
- 6.Prevention, C.f.D.C.a. Multisystem Inflammatory Syndrome in Children (MIS-C) Associated with Coronavirus Disease 2019 (COVID-19). 2020. May 14, 2020 [cited 2023 January 1]; Health Advisory]. Available from: https://emergency.cdc.gov/han/2020/han00432.asp.
- 7.Bularga A, et al. , High-Sensitivity Troponin and the Application of Risk Stratification Thresholds in Patients With Suspected Acute Coronary Syndrome. Circulation, 2019. 140(19): p. 1557–1568. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Fernandes BA, Maher KO, and Deshpande SR, Cardiac biomarkers in pediatric heart disease: A state of art review. World J Cardiol, 2016. 8(12): p. 719–727. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Mair J, et al. , Cardiac biomarkers. Dis Markers, 2015. 2015: p. 370569. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.McDonagh TA, et al. , 2021 ESC Guidelines for the diagnosis and treatment of acute and chronic heart failure. Eur Heart J, 2021. 42(36): p. 3599–3726. [DOI] [PubMed] [Google Scholar]
- 11.Dahdah N, et al. , Natriuretic peptide as an adjunctive diagnostic test in the acute phase of Kawasaki disease. Pediatr Cardiol, 2009. 30(6): p. 810–7. [DOI] [PubMed] [Google Scholar]
- 12.Dionne A and Dahdah N, A Decade of NT-proBNP in Acute Kawasaki Disease, from Physiological Response to Clinical Relevance. Children (Basel), 2018. 5(10). [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Kim M and Kim K, Elevation of cardiac troponin I in the acute stage of Kawasaki disease. Pediatr Cardiol, 1999. 20(3): p. 184–8. [DOI] [PubMed] [Google Scholar]
- 14.Lin KH, et al. , Usefulness of natriuretic peptide for the diagnosis of Kawasaki disease: a systematic review and meta-analysis. BMJ Open, 2015. 5(4): p. e006703. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Rodriguez-Gonzalez M, et al. , N-terminal probrain natriuretic peptide as biomarker for diagnosis of Kawasaki disease. Biomark Med, 2019. 13(4): p. 307–323. [DOI] [PubMed] [Google Scholar]
- 16.Zheng X, et al. , N-terminal pro-brain natriuretic peptide as a biomarker for predicting coronary artery lesion of Kawasaki disease. Sci Rep, 2020. 10(1): p. 5130. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Abrams JY, et al. , Factors linked to severe outcomes in multisystem inflammatory syndrome in children (MIS-C) in the USA: a retrospective surveillance study. Lancet Child Adolesc Health, 2021. 5(5): p. 323–331. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Feldstein LR, et al. , Multisystem Inflammatory Syndrome in U.S. Children and Adolescents. N Engl J Med, 2020. 383(4): p. 334–346. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Fridman MD, et al. , Differentiation of Multi-system Inflammatory Syndrome Associated with COVID-19 Versus Kawasaki Disease Using Cardiac Biomarkers. Can J Cardiol, 2022. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Radia T, et al. , Multi-system inflammatory syndrome in children & adolescents (MIS-C): A systematic review of clinical features and presentation. Paediatr Respir Rev, 2021. 38: p. 51–57. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Rodriguez-Gonzalez M, et al. , Cardiovascular impact of COVID-19 with a focus on children: A systematic review. World J Clin Cases, 2020. 8(21): p. 5250–5283. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Whittaker E, et al. , Clinical Characteristics of 58 Children With a Pediatric Inflammatory Multisystem Syndrome Temporally Associated With SARS-CoV-2. JAMA, 2020. 324(3): p. 259–269. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.Zhao Y, et al. , Cardiac markers of multisystem inflammatory syndrome in children (MIS-C) in COVID-19 patients: A meta-analysis. Am J Emerg Med, 2021. 49: p. 62–70. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.Tong T, et al. , Similarities and differences between MIS-C and KD: a systematic review and meta-analysis. Pediatr Rheumatol Online J, 2022. 20(1): p. 112. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.McCrindle BW, et al. , Medium-Term Complications Associated With Coronary Artery Aneurysms After Kawasaki Disease: A Study From the International Kawasaki Disease Registry. J Am Heart Assoc, 2020. 9(15): p. e016440. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26.Suresh A, Martens P, and Tang WHW, Biomarkers for Myocarditis and Inflammatory Cardiomyopathy. Curr Heart Fail Rep, 2022. 19(5): p. 346–355. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27.Atallah B, et al. , A marker of systemic inflammation or direct cardiac injury: should cardiac troponin levels be monitored in COVID-19 patients? Eur Heart J Qual Care Clin Outcomes, 2020. 6(3): p. 204–207. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28.Henderson LA, et al. , American College of Rheumatology Clinical Guidance for Multisystem Inflammatory Syndrome in Children Associated With SARS-CoV-2 and Hyperinflammation in Pediatric COVID-19: Version 3. Arthritis Rheumatol, 2022. 74(4): p. e1–e20. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29.Samprathi M and Jayashree M, Biomarkers in COVID-19: An Up-To-Date Review. Front Pediatr, 2020. 8: p. 607647. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 30.Di Somma S, et al. , IL-18 stimulates B-type natriuretic peptide synthesis by cardiomyocytes in vitro and its plasma levels correlate with B-type natriuretic peptide in non-overloaded acute heart failure patients. Eur Heart J Acute Cardiovasc Care, 2017. 6(5): p. 450–461. [DOI] [PubMed] [Google Scholar]
- 31.Yanagisawa D, et al. , Factors affecting N-terminal pro-brain natriuretic peptide elevation in the acute phase of Kawasaki disease. Pediatr Int, 2016. 58(11): p. 1105–1111. [DOI] [PubMed] [Google Scholar]