

Abstract
Purpose
Operations for malignant diseases of the bile duct, pancreas, and esophagus are the most invasive gastroenterological surgeries. The frequency of complications after these surgeries is high, which affects the postoperative course and mortality. In patients who undergo these types of surgeries, continuous monitoring of the perioperative central venous oxygen saturation (ScvO2) is possible via a central venous catheter. We aimed to investigate the relationship between continuously monitored perioperative ScvO2 values and postoperative complications.
Methods
The medical records of 115 patients who underwent highly invasive gastroenterological surgeries and ScvO2 monitoring from April 2012 to March 2014 were analyzed. Sixty patients met the inclusion criteria, and their ScvO2 levels were continuously monitored perioperatively. The relationship between ScvO2 levels and major postoperative complications, defined as Clavien–Dindo grade ≥ III, was examined using uni‐ and multivariate analysis.
Results
Thirty patients developed major postoperative complications. The adequate cut‐off value derived from receiver operating curves of the postoperative average ScvO2 levels for predicting major complications was 75%. Multivariate analysis revealed that low average postoperative ScvO2 levels (p = 0.016) and blood loss ≥ 1000 mL (p = 0.039) were significant predictors of major postoperative complications.
Conclusions
Low perioperative ScvO2 values were associated with an increased risk of major postoperative complications. Continuous ScvO2 monitoring will help prevent postoperative complications.
Keywords: anastomotic failure, central venous oxygen saturation, gastroenterological surgery, postoperative complications, surgical site infection
The relationship between perioperative central venous oxygen saturation and postoperative complications in highly invasive gastroenterological surgery.

1. INTRODUCTION
Surgical procedures for malignant diseases of the bile duct, pancreas, and esophagus are lengthy and highly invasive, involving complicated procedures ranging from resection to reconstruction. 1 , 2 , 3 , 4 The frequency of postoperative complications in these invasive gastroenterological surgeries is high, which has a significant effect on morbidity and mortality. 2 , 3 , 4 Therefore, continuous monitoring of key risk indicators are necessary to predict complications and facilitate early therapeutic interventions.
Many postoperative complications in gastroenterological surgery, including anastomotic failure and surgical site infection, are reportedly caused by metabolic disturbances due to a decrease in tissue oxygenation. 5 , 6 Anastomotic failure is the most critical complication in gastroenterological surgery. Although indocyanine green fluorescence imaging and a Doppler blood flow meter are used to evaluate anastomotic blood flow, they are usually only used before performing anastomosis. 7 , 8 Moreover, these devices are not used after surgery to predict anastomotic failure. It has also been reported that surgical site infection, 6 liver dysfunction, 9 postoperative cognitive dysfunction, and delirium 10 , 11 are associated with reduced tissue oxygenation, which greatly affects the postoperative course.
The central venous oxygen saturation (ScvO2) value is an index that reflects the balance between oxygen supply and consumption, which may be useful in predicting postoperative complications. The factors affecting ScvO2 are cardiac output, hemoglobin concentration, inspired oxygen concentration, and tissue oxygen consumption. 12 When tissue oxygen consumption exceeds the oxygen supply, complications occur due to tissue hypoxia. ScvO2 is used as an index of the supply–demand balance of oxygen in the tissues, which is similar to mixed venous oxygen saturation (SvO2) used in highly invasive surgeries. 13 ScvO2 can be monitored via a central venous catheter, unlike SvO2 which requires the insertion of a catheter into the pulmonary artery; therefore, measurements of ScvO2 are minimally invasive unlike SvO2. 14
There are only a few studies on whether ScvO2 can be used to predict postoperative complications; one study has reported that postoperative complications can be reduced by monitoring intraoperative ScvO2 and by performing therapeutic interventions in high‐risk surgical patients. 15 Few previous reports exist on the continuous monitoring of ScvO2 during lengthy and highly invasive operations for malignant diseases of the bile duct, pancreas, and esophagus. 9 , 16 , 17 Reports on the use of ScvO2 as an index of perioperative management, apart from those for specific operations such as heart surgery 18 and liver transplant, 19 are scarce. No consensus has been reached for the target value of perioperative ScvO2.
A randomized controlled trial of patients with sepsis revealed that targeting ScvO2 ≥ 70% during initial resuscitation from severe sepsis or septic shock could reduce in‐hospital mortality 20 ; this has been strongly recommended in the Surviving Sepsis Campaign Guidelines. 21 However, multicenter randomized controlled trial 22 did not confirm these findings, and the evaluation of ScvO2 in patients with sepsis remains controversial. 23 The factors leading to low ScvO2 values in patients with postoperative complications remain unclear.
In this study, we aimed to investigate the relationship between continuously monitored ScvO2 values in the intra‐/postoperative periods and postoperative complications in patients undergoing major hepatobiliary, pancreatic, and esophageal surgeries and define the target ScvO2 value.
2. METHODS
2.1. Patients
We retrospectively analyzed the electronic health records of 115 consecutive patients who underwent gastroenterological surgeries and ScvO2 monitoring in the Department of Gastroenterological Surgery II, Hokkaido University Hospital from April 2012 to March 2014. Nine patients who underwent surgical procedures other than radical resection and 46 patients with incomplete ScvO2 data, including improper pre‐, intra‐, or postoperative measurements or inaccurate values [signal quality index (SQI) = 4; Unacceptable] were excluded from the study. A total of 60 patients who underwent radical surgery for hepatobiliary, pancreatic, and esophageal diseases were included in the study and their medical records were analyzed to obtain information on background factors, surgical procedure performed, and postoperative complications. Postoperative complication was defined as any event affecting a patient that is undesirable, unintended, and a direct result of operative procedure. In this study, we evaluated the in‐hospital postoperative complication as per the Clavien–Dindo classification, and defined Clavien–Dindo grades ≥ III as major complication. The patients were divided into two groups depending on whether the major complication has happened or not (Figure 1). The two groups were compared in terms of background factors, surgical outcomes, and ScvO2 values.
FIGURE 1.

Flow diagram of this study. The intraoperative ScvO2 of 115 patients was monitored. Nine patients were excluded due to the surgical procedure received and 46 patients were excluded because of incomplete ScvO2 data. The remaining 60 cases were included. Major complications graded as Clavien–Dindo ≥ III were observed in 30 patients. ScvO2, central venous oxygen saturation.
This study was approved by the institutional review board (authorization number: 020–0272) and conformed to the provisions of the Declaration of Helsinki. The records of patients who refused access to their data were excluded from the analysis.
2.2. Monitoring of ScvO2
A PreSep oximetry catheter and Vigileo monitor (Edwards Lifescience Corporation, California, USA) were used to monitor the ScvO2. Patients were placed under ultrasound and fluoroscopy to confirm that the target of the catheter tip was 2 cm distal to the tracheal bifurcation, as this position was considered to have the best SQI based on a pilot study in our department. The preoperative ScvO2 was recorded and the Vigileo monitor was calibrated after the catheter placement. The intra‐ and postoperative ScvO2 levels were monitored continuously using a Vigileo monitor for up to 12 h after surgery. The ScvO2 values were recorded every 20 s. All recorded ScvO2 values were summed up and divided by the total number of measurements to calculate the average ScvO2.
2.3. Statistical analyses
Continuous data were evaluated with the Mann–Whitney U test and nominal data with the chi‐square test. The limit for inclusion of new terms was set at p < 0.05, and a multiple logistic regression model was used to identify independent risk factors for major postoperative complications. Univariate analysis was used to compare the ScvO2 values and background factors between patients with and without major postoperative complications. Receiver operating curves (ROC) were generated to identify the cut‐off values of postoperative ScvO2 for predicting major complications, and the area under the ROC curve was calculated. The analysis was performed using EZR (Ver. 1.42, Saitama Medical Center, Jichi Medical University, Saitama, Japan), which is a graphical user interface for R (The R Foundation for Statistical Computing, Vienna, Austria), 24 and significance was set at p < 0.05.
3. RESULTS
The mean age of the patients in our cohort was 65 (range, 13–80) years. The surgical procedures performed included the following 17 liver lobectomies, 17 pancreaticoduodenectomies, three hepatopancreaticoduodenectomies, 11 esophagectomies, and 12 others (e.g. distal pancreatectomies, and partial hepatectomies). The mean duration of the surgical procedures was 629 (range, 311–994) min, and the mean blood loss was 1677 (range, 120–8510) mL. Major complications were observed in 30 patients (30/60, 50%). The most common complication was anastomotic failure seen in 17 patients (28%). Seven patients underwent a reoperation (12%), and postoperative mortality was 3% (2/60 patients) (Table 1). Univariate analysis of ScvO2 values and major complications revealed that the intraoperative and postoperative average (p = 0.032/0.014) and lowest (p = 0.047/0.040) ScvO2 values were associated with major postoperative complications (Table 2). Univariate analysis of the background factors showed that only factor associated with major postoperative complications was blood loss (p = 0.015) (Table 3).
TABLE 1.
Patient demographics and complications.
| Background factors | Number of patients (%), n = 60 or mean (range) |
|---|---|
| Age, years | 65 (13–80) |
| Sex, male/female | 39/21 |
| BMI, kg/m2 | 22.7 (16.8–31.6) |
| ASA status, 1/2/3 | 9/48/3 |
| Surgical procedure | |
| Liver lobectomy | 17 (28) |
| PD | 17 (28) |
| HPD | 3 (5) |
| Esophagectomy | 11 (18) |
| Others (e.g., DP, partial hepatectomy.) | 12 (20) |
| Length of operation, min | 629 (311–994) |
| Blood loss, mL | 1677 (120–8510) |
| Complication | |
| Anastomotic failure | 17 (28) |
| Intra‐abdominal/thoracic abscess | 13 (22) |
| Sepsis | 11 (18) |
| Bleeding | 10 (17) |
| Organ dysfunction | 6 (10) |
| Re‐operation | 7 (12) |
| CD grade | |
| IIIa | 22 (37) |
| IIIb | 2 (3) |
| IVa | 2 (3) |
| IVb | 2 (3) |
| V | 2 (3) |
| Major complications | 30 (50) |
Note: The definition of a major complication of Clavien–Dindo grade III or higher.
Abbreviations: ASA, American Society of Anesthesiologists physical status; BMI, body mass index; CD, Clavien–Dindo; DP, distal pancreatectomy; HPD, hepatopancreaticoduodenectomy; min, minute; PD, pancreaticoduodenectomy.
TABLE 2.
Univariate analysis of ScvO2 value and major postoperative complications.
| ScvO2 value | Patients without major complications (n = 30) | Patients with major complications (n = 30) | p |
|---|---|---|---|
| Preoperative scvo2, % (range) | 67.9 (51.0–83.4) | 65.6 (49.4–80.9) | 0.23 |
| Intraoperative scvo2, average % | 80.3 (61.9–91.7) | 77.5 (68.2–86.1) | 0.032* |
| Intraoperative scvo2, lowest % (range) | 67.4 (40–83) | 61.3 (27–80) | 0.047* |
| Postoperative scvo2, average % (range) | 81.0 (65.6–93.3) | 75.3 (47.3–86.1) | 0.014* |
| Postoperative scvo2, lowest % (range) | 61.2 (43–89) | 48.6 (14–78) | 0.040* |
Note: The definition of a major complication is a complication graded Cravien‐Dindo grade III or higher.
Abbreviation: ScvO2 central venous oxygen saturation.
Significant p value.
TABLE 3.
Univariate analysis of background factors and major complications.
| Background factor | Patients without major complications (n = 30) | Patients with major complications (n = 30) | p |
|---|---|---|---|
| Age, years | 66 (13–78) | 69 (45–80) | 0.17 |
| Sex, male/female | 18/12 | 21/9 | 0.59 |
| BMI, kg/m2 (range) | 23.4 (18.2–31.3) | 22.0 (16.8–31.6) | 0.060 |
| ASA status, 1/2/3 |
4/25/1 |
5/23/2 | 0.16 |
|
Surgical procedures Liver lobectomy/pancreatectomy/esophagectomy |
9/12/9 | 14/12/4 | 0.23 |
| Length of operation, min (range) | 594 (311–931) | 622 (419–994) | 0.21 |
| Blood loss, mL (range) | 887 (170–7680) | 1715 (120–8510) | 0.015* |
| Diabetes, +/− | 5/25 | 6/24 | 1.0 |
| Heart disease, +/− | 5/25 | 2/28 | 0.24 |
| Pulmonary dysfunction, +/− | 6/24 | 7/23 | 0.76 |
Note: The definition of a major complication is a complication graded Clavien‐Dindo grade III or higher.
Abbreviations: ASA, American Society of Anesthesiologists physical status; BMI, body mass index.
Significant p value.
We selected postoperative average ScvO2 for the multivariate analysis and ROC because intraoperative ScvO2 fluctuated greatly due to the introduction of anesthesia and surgical intervention. Moreover, range of postoperative average ScvO2 value is wider, which is advantageous as an indicator (Figure 2). The cut‐off values of postoperative ScvO2 derived from ROC curves was set to 75% (Figure 3). After multivariate analyses, postoperative ScvO2 values (p = 0.016) and blood loss ≥ 1000 mL (p = 0.039) were found to be independently associated with major postoperative complications (Table 4).
FIGURE 2.
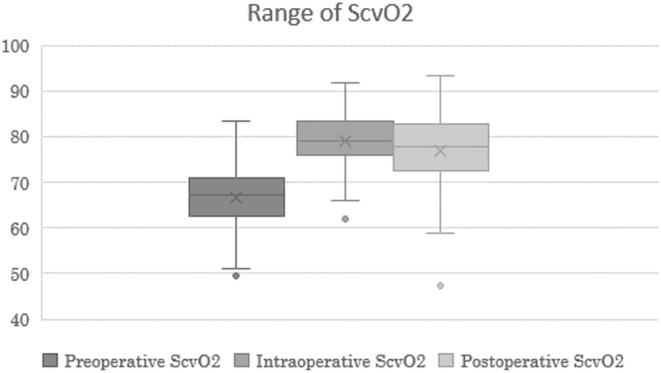
Range of perioperative ScvO2. The postoperative ScvO2 was monitored for up to 12 h. ScvO2, central venous oxygen saturation.
FIGURE 3.
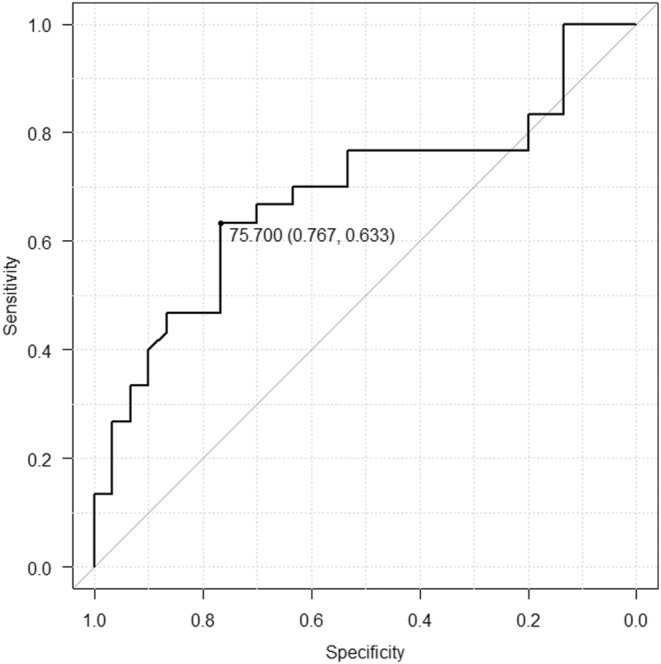
ROC curve of postoperative ScvO2 (average) and major complications; 75% was the most suitable threshold. ROC, receiver operating characteristics; ScvO2, central venous oxygen saturation.
TABLE 4.
Multivariable analyses of postoperative ScvO2 values (average) and major complications.
| Factor | Univariate | Multivariate | ||||
|---|---|---|---|---|---|---|
| OR | 95% CI | p Values | OR | 95% CI | p Values | |
| Age (≥70 years) | 2.41 | 0.82–7.10 | 0.11 | |||
| Sex (Male) | 1.56 | 0.53–4.53 | 0.42 | |||
| BMI (≥25 kg/m2) | 0.88 | 0.75–1.03 | 0.12 | |||
| ASA (1/2 or 3) | 0.77 | 0.19–3.20 | 0.72 | |||
|
Surgical procedure (liver lobectomy or pancreatectomy/esophagectomy) |
0.36 | 0.10–1.33 | 0.13 | |||
| Length of operation (≥600 min) | 1.50 | 0.53–4.17 | 0.44 | |||
| Blood loss (≥1000 mL) | 3.14 | 1.07–9.27 | 0.038* | 3.39 | 1.06–10.8 | 0.039* |
| Diabetes (+/−) | 1.25 | 0.34–4.64 | 0.74 | |||
| Heart disease (+/−) | 0.36 | 0.06–2.01 | 0.24 | |||
| Pulmonary dysfunction (+/−) | 1.22 | 0.36–4.17 | 0.75 | |||
| Postoperative scvo2 (average, ≤75%) | 4.37 | 1.32–14.5 | 0.016* | 4.69 | 1.33–16.95 | 0.016* |
Note: The definition of a major complication is a complication graded Clavien‐Dindo grade III or higher.
Abbreviations: ASA, American Society of Anesthesiologists physical status; BMI, body mass index; CI, confidence interval; OR, odds ratio; ScvO2, central venous oxygen saturation.
Significant p value.
Sub analysis was done by grouping patients into postoperative ScvO2 ≤ 75% group and ScvO2 > 75% group. No significant differences were found between two groups in the comparison of perioperative factors. The incidence of any complication and perioperative factors were compared. Significant differences in major complications (p = 0.025) and anastomotic failure (p = 0.035) were identified between the two groups (Table 5).
TABLE 5.
Comparison of perioperative factors affect ScvO2 and complications based on a 75% mean postoperative ScvO2 cut‐off value.
| Factor | ScvO2 ≤ 75% (n = 19) | ScvO2 > 75% (n = 41) | p |
|---|---|---|---|
| Respiratory dysfunction (+/−) | 2/17 | 11/30 | 0.18 |
| Preoperative scvo2 values(range) | 66.9(53.7–79.0) | 66.7(49.4–83.4) | 0.93 |
| Perioperative lowest hemoglobin concentration(range) | 8.5(6.3–11.5) | 8.4(5.9–12.8) | 0.83 |
| Blood transfusion (+/−) | 8/11 | 16/25 | 0.63 |
| Average cardiac output(range) | 4.6(3.4–6.6) | 4.6(3.2–7.2) | 0.85 |
| Complication (+/−) | |||
| Anastomotic failure | 9/10 | 8/33 | 0.035* |
| Intra‐abdominal/thoracic abscess | 6/13 | 7/34 | 0.30 |
| Sepsis | 6/13 | 5/36 | 0.086 |
| Bleeding | 4/15 | 6/35 | 0.67 |
| Organ dysfunction | 1/18 | 5/36 | 0.65 |
| Reoperation | 4/15 | 3/38 | 0.19 |
| Major complications | 14/5 | 16/25 | 0.025* |
Note: The definition of a major complication is a complication graded Clavien‐Dindo grade III or higher.
Abbreviation: ScvO2, central venous oxygen saturation.
Significant p value.
4. DISCUSSION
The main finding of this study was the association of low intra‐ and postoperative ScvO2 values with an increased risk of major postoperative complications after highly invasive gastroenterological surgery. Supporting our results, the association of intraoperative ScvO2 values with anastomotic failure in colectomy and postoperative organ dysfunction in surgical patients has been reported. 9 , 25
Our results suggest that optimization of ScvO2 may contribute to the prevention of major postoperative complications and anastomotic failure. The supply of high concentration oxygen is known to be effective in preventing surgical site infection, 26 and ScvO2 can be a useful index of tissue oxygenation. The average value of ScvO2 in a healthy person is about above 70%. 13 In our study, we set the cut‐off line for ScvO2 at 75%, which is higher than the average of a healthy person. According to our result, the postoperative ScvO2 should be maintained high, to prevent the postoperative complication. Low ScvO2 can be caused by respiratory distress, anemia, etc. Oxygenation should be facilitated by proper management, including reintubation and blood transfusion in case of low ScvO2.
Of 14 patients who had developed major complications with perioperative ScvO2 < 75%, half were observed anemia: one had intraoperative blood loss of more than 2000 mL, one had intraoperative Hb below 8.0 g/dL, and five cases had both. This indicates that intraoperative blood loss plays a significant role in the decline in ScvO2 value. In contrast, two cases in low perioperative ScvO2 group with blood loss less than 500 mL had also developed complications. Cardiotonic agents should be considered for decreased cardiac output, and treatment needs to be commenced if there are signs of sepsis. Reduction of ScvO2 can be caused by multiple factors. Cause‐specific approaches and target thresholds should be considered based on individual patient characteristics and clinical context.
Several procedures exist to monitor ScvO2, including intermittent or continuous monitoring and choosing the lowest or the average values. ScvO2 varies greatly depending on the status of the patient; therefore, we applied continuous ScvO2 monitoring and analyzed the average values of ScvO2 instead of considering the lowest values. Continuous ScvO2 monitoring and evaluation of the average value makes it possible to eliminate bias caused by the intraoperative state of patients, and the risk of complications can be predicted more accurately. Sankar et al. reported that continuous monitoring of ScvO2 and therapeutic intervention in patients with sepsis improved prognosis as compared to intermittent monitoring. 27
Perioperative monitoring of ScvO2 may be a more sensitive indicator of oxygen supply–demand balance than other types of monitoring. For example, perioperative peripheral capillary oxygen saturation (SpO2) and central venous pressure (CVP) are monitored continuously to evaluate the tissue oxygenation status 28 ; however, unlike ScvO2, the SpO2 and CVP values do not vary significantly (SpO2 is often 95%–100% throughout surgery) and therefore are not sensitive indicators. In this study, ScvO2 demonstrated a wide fluctuation range of approximately 40%–90% and was therefore considered a more sensitive indicator of oxygen supply–demand balance. Perioperative monitoring of serum lactate is another method used to evaluate the tissue oxygen supply–demand balance. 29 Study has shown that serum lactate values are useful in monitoring patients with septic shock. 30 However, serum lactate is typically measured withy blood gas analyses. Continuous serum lactate measurement will require specialized equipment, which is not clinically practical.
In contrast to the hyperdynamic state of sepsis, which ScvO2 is commonly higher. In our study, high ScvO2 values did not adversely affect postoperative outcomes. This difference may be due to differences in sepsis and perioperative pathology. Investigating the underlying pathophysiological mechanisms would require further research, including experimental and mechanistic studies.
Our study demonstrates that intra‐ and postoperative ScvO2 were associated with major postoperative complications in highly invasive gastroenterological surgeries for hepatobiliary, pancreatic, and esophageal diseases.
This study has some limitations. First, 46 patients were excluded from the study due to incomplete ScvO2 data. In our institution, fluoroscopy was used to confirm the position of the catheter tip at 2 cm distal to the tracheal bifurcation, as this position was considered to have the best SQI index based on a pilot study done by our department. Despite this, some patients presented poor SQI indices and were excluded from this study. The optimal position of the catheter tip for accurate ScvO2 monitoring and the confirmation method used are subjects for future research. Second, this study was conducted as a single‐center, retrospective study; for this reason, many factors regarding perioperative management were not assessed, which created bias in the data regarding postoperative complications. Third, the intra‐ and postoperative oxygen supply was determined by the anesthesiologist, which affected the ScvO2 values. Although we estimated the cut‐off value of postoperative ScvO2 as 75%, further research is required to determine its validity and ability to facilitate the prevention of postoperative complications.
5. CONCLUSIONS
In this study, we observed that low intra‐ and postoperative ScvO2 were associated with an increased risk of major postoperative complications in highly invasive gastroenterological surgery. The adequate cut‐off value of postoperative ScvO2 for predicting major complications was estimated at 75%. Continuous intra‐ and postoperative ScvO2 monitoring and therapeutic interventions may facilitate the prevention of postoperative complications. Further studies are required to reveal the underlying mechanisms of decreased ScvO2 in patients with postoperative complications and to validate the potential benefits of ScvO2 monitoring.
AUTHOR CONTRIBUTIONS
D.M. did the study design, analyzed the data, interpreted the results, and wrote the manuscript. T.S. is the corresponding author of the manuscript; contributed to conception and design, analyzed data, revised the article. Y.K. contributed to the conception and design, interpreted and offered analyses of the results. Y.W. verified the study design and contributed to the process of the ethics review and statements. S.H. supervised the hole research and revised the article. All of the authors made substantial contributions to the study concept or the data analysis or interpretation, revised it critically for important intellectual content, approved the final version of the manuscript to be published, and agreed to be accountable for all aspects of the work.
FUNDING INFORMATION
We have no funding of interest to declare.
CONFLICT OF INTEREST STATEMENT
The authors declare no conflicts of interest for this article.
ETHICS STATEMENTS
Approval of the research protocol: This study was approved by the institutional review board (authorization number: 020–0272) and conformed to the provisions of the Declaration of Helsinki (as revised in Fortaleza, Brazil, October 2013), available at: https://www.wma.net/what‐we‐do/medical‐ethics/declaration‐of‐helsinki/.Informed consent: In accordance with the Japan Ethical Guidelines for Medical and Health Research Involving Human Subjects, informed consent was obtained from all participants on the Hokkaido University Hospital website (https://www.huhp.hokudai.ac.jp/wp‐content/uploads/2021/03/020‐0272.pdf).Registry and the Registration No. of the study/Trial: N/A.Animal Studies: N/A.
ACKNOWLEDGMENTS
The authors thank all the staff in the Department of Anesthesia at Hokkaido University Hospital for their cooperation in this study.
Miyazaki D, Shichinohe T, Watanabe Y, Tanaka K, Nakanishi Y, Asano T, et al. The relationship between perioperative central venous oxygen saturation and postoperative complications in highly invasive gastroenterological surgery. Ann Gastroenterol Surg. 2024;8:660–667. 10.1002/ags3.12768
DATA AVAILABILITY STATEMENT
The datasets generated during and/or analyzed during the current study are available from the corresponding author on reasonable request.
REFERENCES
- 1. Weiser TG, Haynes AB, Molina G, Lipsitz SR, Esquivel MM, Uribe‐Leitz T, et al. Estimate of the global volume of surgery in 2012: an assessment supporting improved health outcomes. Lancet. 2015;385(Suppl 2):S11. [DOI] [PubMed] [Google Scholar]
- 2. Behrman SW, Rush BT, Dilawari RA. A modern analysis of morbidity after pancreatic resection. Am Surg. 2004;70(8):675–682. discussion 82–83. [PubMed] [Google Scholar]
- 3. Hirano S, Kondo S, Tanaka E, Shichinohe T, Tsuchikawa T, Kato K, et al. Outcome of surgical treatment of hilar cholangiocarcinoma: a special reference to postoperative morbidity and mortality. J Hepatobil Pancreat Sci. 2010;17(4):455–462. [DOI] [PubMed] [Google Scholar]
- 4. McCulloch P, Ward J, Tekkis PP. ASCOT group of surgeons, British Oesophago‐gastric cancer group. Mortality and morbidity in gastro‐oesophageal cancer surgery: initial results of ASCOT multicentre prospective cohort study. BMJ. 2003;327(7425):1192–1197. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5. Sheridan WG, Lowndes RH, Young HL. Tissue oxygen tension as a predictor of colonic anastomotic healing. Dis Colon Rectum. 1987;30(11):867–871. [DOI] [PubMed] [Google Scholar]
- 6. Ives CL, Harrison DK, Stansby GS. Tissue oxygen saturation, measured by near‐infrared spectroscopy, and its relationship to surgical‐site infections. Br J Surg. 2007;94(1):87–91. [DOI] [PubMed] [Google Scholar]
- 7. Blanco‐Colino R, Espin‐Basany E. Intraoperative use of ICG fluorescence imaging to reduce the risk of anastomotic leakage in colorectal surgery: a systematic review and meta‐analysis. Tech Coloproctol. 2018;22(1):15–23. [DOI] [PubMed] [Google Scholar]
- 8. Du CZ, Fan ZH, Yang YF, Yuan P, Gu J. Value of intra‐operative doppler sonographic measurements in predicting post‐operative anastomotic leakage in rectal cancer: a prospective pilot study. Chin Med J (Engl). 2019;132(18):2168–2176. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9. Meguro M, Mizuguchi T, Kawamoto M, Nakamura Y, Ota S, Kukita K, et al. Continuous monitoring of central venous oxygen saturation predicts postoperative liver dysfunction after liver resection. Surgery. 2013;154(2):351–362. [DOI] [PubMed] [Google Scholar]
- 10. Agnoletti V, Ansaloni L, Catena F, Chattat R, de Cataldis A, di Nino G, et al. Postoperative delirium after elective and emergency surgery: analysis and checking of risk factors. A study protocol. BMC Surg. 2005;5:12. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11. Tang L, Kazan R, Taddei R, Zaouter C, Cyr S, Hemmerling TM. Reduced cerebral oxygen saturation during thoracic surgery predicts early postoperative cognitive dysfunction. Br J Anaesth. 2012;108(4):623–629. [DOI] [PubMed] [Google Scholar]
- 12. Litton E, Silbert B, Ho KM. Clinical predictors of a low central venous oxygen saturation after major surgery: a prospective prevalence study. Anaesth Intensive Care. 2015;43(1):59–65. [DOI] [PubMed] [Google Scholar]
- 13. Dueck MH, Klimek M, Appenrodt S, Weigand C, Boerner U. Trends but not individual values of central venous oxygen saturation agree with mixed venous oxygen saturation during varying hemodynamic conditions. Anesthesiology. 2005;103(2):249–257. [DOI] [PubMed] [Google Scholar]
- 14. Goodrich C. Continuous central venous oximetry monitoring. Crit Care Nurs Clin North Am. 2006;18(2):203–209. [DOI] [PubMed] [Google Scholar]
- 15. Donati A, Loggi S, Preiser JC, Orsetti G, Münch C, Gabbanelli V, et al. Goal‐directed intraoperative therapy reduces morbidity and length of hospital stay in high‐risk surgical patients. Chest. 2007;132(6):1817–1824. [DOI] [PubMed] [Google Scholar]
- 16. Kawaguchi Y, Kushikata T, Kitayama M, Hirota K. Central venous oxygen saturation monitoring was useful in two cases of hepatectomy with massive bleeding. Masui. 2006;55(12):1502–1505. [PubMed] [Google Scholar]
- 17. Mikor A, Trásy D, Németh MF, Osztroluczki A, Kocsi S, Kovács I, et al. Continuous central venous oxygen saturation assisted intraoperative hemodynamic management during major abdominal surgery: a randomized, controlled trial. BMC Anesthesiol. 2015;15:82. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18. Lequeux PY, Bouckaert Y, Sekkat H, van der Linden P, Stefanidis C, Huynh CH, et al. Continuous mixed venous and central venous oxygen saturation in cardiac surgery with cardiopulmonary bypass. Eur J Anaesthesiol. 2010;27(3):295–299. [DOI] [PubMed] [Google Scholar]
- 19. Dahmani S, Paugam‐Burtz C, Gauss T, Alves M, le Bihan E, Necib S, et al. Comparison of central and mixed venous saturation during liver transplantation in cirrhotic patients: a pilot study. Eur J Anaesthesiol. 2010;27(8):714–719. [DOI] [PubMed] [Google Scholar]
- 20. Rhodes A, Phillips G, Beale R, Cecconi M, Chiche JD, de Backer D, et al. The surviving sepsis campaign bundles and outcome: results from the international multicentre prevalence study on sepsis (the IMPreSS study). Intensive Care Med. 2015;41(9):1620–1628. [DOI] [PubMed] [Google Scholar]
- 21. Dubose JJ, Scalea TM, Holcomb JB, et al. Open abdominal management after damage‐control laparotomy for trauma: a prospective observational American Association for the Surgery of Trauma multicenter study. J Trauma Acute Care Surg. 2013;74(1):113–122. discussion 1120–1122. [DOI] [PubMed] [Google Scholar]
- 22. Mouncey PR, Osborn TM, Power GS, Harrison DA, Sadique MZ, Grieve RD, et al. Trial of early, goal‐directed resuscitation for septic shock. N Engl J Med. 2015;372(14):1301–1311. [DOI] [PubMed] [Google Scholar]
- 23. Protti A, Masson S, Latini R, Fumagalli R, Romero M, Pessina C, et al. Persistence of central venous oxygen desaturation during early sepsis is associated with higher mortality: a retrospective analysis of the ALBIOS trial. Chest. 2018;154(6):1291–1300. [DOI] [PubMed] [Google Scholar]
- 24. Kanda Y. Investigation of the freely available easy‐to‐use software ‘EZR’ for medical statistics. Bone Marrow Transplant. 2013;48(3):452–458. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25. Isaza‐Restrepo A, Moreno‐Mejia JF, Martin‐Saavedra JS, Ibañez‐Pinilla M. Low values of central venous oxygen saturation (ScvO2) during surgery and anastomotic leak of abdominal trauma patients. World J Emerg Surg. 2017;12:28. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26. Global Guidelines for the Prevention of Surgical Site Infection , 2018. https://www.who.int/publications/i/item/9789241550475
- 27. Sankar J, Singh M, Kumar K, Sankar MJ, Kabra SK, Lodha R. ‘Intermittent’ versus ‘continuous’ ScvO2 monitoring in children with septic shock: a randomised, non‐inferiority trial. Intensive Care Med. 2020;46(1):82–92. [DOI] [PubMed] [Google Scholar]
- 28. Green D, Paklet L. Latest developments in peri‐operative monitoring of the high‐risk major surgery patient. Int J Surg. 2010;8(2):90–99. [DOI] [PubMed] [Google Scholar]
- 29. Vincent JL, QE Silva A, Couto L, Taccone FS. The value of blood lactate kinetics in critically ill patients: a systematic review. Crit Care. 2016;20(1):257. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 30. Lee YK, Hwang SY, Shin TG, Jo IJ, Suh GY, Jeon K. Prognostic value of lactate and central venous oxygen saturation after early resuscitation in sepsis patients. PloS One. 2016;11(4):e0153305. [DOI] [PMC free article] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Data Availability Statement
The datasets generated during and/or analyzed during the current study are available from the corresponding author on reasonable request.