

Abstract
Background
Outcome monitoring of depression treatment is recommended but there is a lack of evidence on patient benefit in primary care.
Aim
To test monitoring depression using the Patient Health Questionnaire (PHQ-9) with patient feedback.
Design and setting
An open cluster-randomised controlled trial was undertaken in 141 group practices.
Method
Adults with new depressive episodes were recruited through record searches and opportunistically. The exclusion criteria were as follows: dementia; psychosis; substance misuse; and suicide risk. The PHQ-9 was administered soon after diagnosis, and 10–35 days later. The primary outcome was the Beck Depression Inventory (BDI-II) score at 12 weeks. The secondary outcomes were as follows: BDI-II at 26 weeks; Work and Social Adjustment Scale (WSAS) and EuroQol EQ-5D-5L quality of life at 12 and 26 weeks; antidepressant treatment; mental health and social service contacts; adverse events, and Medical Interview Satisfaction Scale (MISS) over 26 weeks.
Results
In total, 302 patients were recruited to the intervention arm and 227 to the controls. At 12 weeks, 254 (84.1%) and 199 (87.7%) were followed-up, respectively. Only 40.9% of patients in the intervention had a GP follow-up PHQ-9 recorded. There was no significant difference in BDI-II score at 12 weeks (mean difference −0.46; 95% confidence interval [CI] = −2.16 to 1.26; adjusted for baseline depression, baseline anxiety, sociodemographic factors, and clustering by practice). EQ-5D-5L quality-of-life scores were higher in the intervention arm at 26 weeks (adjusted mean difference 0.053; 95% CI = 0.013 to 0.093. A clinically significant difference in depression at 26 weeks could not be ruled out. No significant differences were found in social functioning, adverse events, or satisfaction. In a per-protocol analysis, antidepressant use and mental health contacts were significantly greater in patients in the intervention arm with a recorded follow-up PHQ-9 (P = 0.025 and P = 0.010, respectively).
Conclusion
No evidence was found of improved depression outcome at 12 weeks from monitoring. The findings of possible benefits over 26 weeks warrant replication, investigating possible mechanisms, preferably with automated delivery of monitoring and more instructive feedback.
Keywords: primary health care, mental health, mood disorders, depression, patient reported outcome measures
Introduction
Guidelines on the management of depression in adults recommend practitioners consider using validated patient-reported outcome measures (PROMs) to inform treatment at diagnosis and follow-up of people with depression,1–4 but there is insufficient evidence that they improve depression management and outcomes for patients in primary care.5,6
Relatively few studies of PROMs for depression have been conducted in primary care, and there is almost a complete lack of evidence on important outcomes including social functioning, patient satisfaction, quality of life, cost-effectiveness, and possible adverse effects.5,6
The aim of the study was to answer the research question: what is the effectiveness of assessing primary care patients with depression or low mood after diagnosis and again at follow-up 10–35 days later, using the Patient Health Questionnaire (PHQ-9) as a PROM, giving practitioners guidance on assessment and feedback to patients on their progress?
Method
Design and setting
A parallel group open cluster-randomised superiority trial was set in 141 group general practices in England and Wales. A cluster-randomised design was chosen based on a significant risk of contamination between arms identified through qualitative interviews with GPs in a prior feasibility trial; that is, that it would be difficult to forget and avoid using the PHQ-9 questions when treating a control patient in an individually randomised trial.
How this fits in
| Follow-up monitoring of people with depression, using patient-reported outcome measures (PROMs), is recommended but evidence of benefit in primary care is lacking. Monitoring patients’ progress with the Patient Health Questionnaire (PHQ-9) produced no benefit in terms of depressive symptoms at 12 weeks follow-up, but at 26 weeks a significant difference in depression could not be ruled out, and patients’ quality of life was significantly improved (P = 0.01). Only 40.9% of patients in the intervention arm had a follow-up PHQ-9 recorded in the GP records. Further research should test PROMS that measure anxiety as well as depression, which are automatically delivered and integrated into patients’ records, and produce specific treatment recommendations. |
Randomisation
Randomisation was carried out remotely by a clinical trials unit statistician using computerised sequencing, with minimisation for three factors: recruiting centres; small or large practices (dichotomised around 8000 patients); and urban or rural locations by local authority classification.
Inclusion and exclusion criteria
Adults with new episodes of depression were recruited mainly through frequent practice record searches, but also opportunistically in consultations. Exclusion criteria were as follows: existing treatment for depression; dementia; psychosis; substance misuse; or suicide risk.
Intervention
The PHQ-97 was administered by a researcher as soon as possible after recruitment (within 2 weeks), and the GP was asked to repeat the PHQ-9 at a follow-up consultation 10–35 days later. Patients were given written feedback on their PHQ-9 scores and potential treatments to discuss with their GPs. The GPs were given 2 hours online training in interpreting PHQ-9 scores and taking them into account in management (Supplementary Information S1). They were tested on their understanding of the trial processes together with the strengths and limitations of the PHQ-9, and how it might be used in practice (Supplementary Information S2). Use of the PHQ-9 in practice was modelled by one of the co-principal investigators (CD), with a simulated patient, in videos representing the first and second follow-up consultations for depression with a practitioner in the study (Supplementary Information S3).
Outcomes
The primary outcome was depression on the Beck Depression Inventory (BDI-II)8 at 12 weeks. The secondary outcomes at 26 weeks were as follows: BDI-II scores; social functioning (Work and Social Adjustment Scale [WSAS]);9 quality of life (EuroQol EQ-5D-5L);10 patient satisfaction (Medical Interview Satisfaction Scale [MISS]);11 antidepressant treatment; mental health and social service contacts; and adverse events.
Blinding
Blinding of participants to allocation was impossible given the pragmatic cluster randomised design, but self-report outcome measures were used to prevent observer bias, and analysis was blind to allocation.
Sample size calculation
A baseline mean BDI-II score of 24.0 was assumed with a standard deviation (SD) of 10.0 (derived from a feasibility trial),12 and mean scores of 14.0 and 17.0 at 12 weeks in the intervention and control groups, respectively. An effect size of 0.3 SD represented the minimum clinically important difference (MCID) on the BDI-II.13 At 5% significance, for 90% power, 235 patients were needed to be analysed per group. An intracluster correlation coefficient (ICC) of 0.03 was assumed (from the feasibility trial)12 and mean cluster size of six, which gave a design effect of 1.15, giving 270 per group. With 20% loss to follow-up, the target was 676 patients recruited from 113 practices.
The target was subsequently (10 June 2021) revised on finding a correlation of greater than P = 0.5 between baseline and follow-up for the primary outcome, meaning only 222 patients were needed to be analysed per group and total target of 554 recruited.
Analysis
A detailed statistical analysis plan was drawn up before analysis of the results (Supplementary Information S4). Differences between arms in depressive symptoms, social functioning, and quality of life at 12 and 26-weeks follow-up were analysed using linear mixed models, adjusting for baseline values; baseline anxiety (measured using the Generalised Anxiety Disorder-7item [GAD-7]);14 sociodemographic factors, past history of depression, and clustering including a random effect for practice. Patient satisfaction was compared between arms over the 26-week period.
Differences between arms in the process of care for depression were also analysed from practice medical record data over 26 weeks including PHQ-9s recorded, antidepressant prescribing, and mental health and social service contacts.
Suicide risk
If patients scored other than 0 on suicide or self-harm questions on the BDI-II or PHQ-9 at screening, baseline, or follow-up, or indicated suicidal ideas in other ways, a standard operating procedure (SOP) was implemented, requiring further assessment using the P4 screener suicide risk assessment.15 Based on the patients’ responses, the risk of suicide was categorised as minimal, lower, or higher, and the GP was informed immediately. Care of all patients remained the responsibility of participating GPs, as in usual practice.
More information on the methods can be found in the published protocol.16
Results
Recruitment of practices
The study aimed to recruit 113 practices between November 2018 and August 2019. Owing to slow recruitment of patients, the recruitment process had to continue much longer than planned (made worse by the COVID-19 pandemic), eventually a total of 189 was reached by December 2021. Then 48 withdrew before recruiting patients (24 in each arm), leaving 141: 72 intervention and 69 control-arm practices. Minimisation ensured practice characteristics were balanced by arm (Table 1).
Table 1.
Cluster level (participating general practice) characteristics at baseline
| Characteristic | Intervention | Control | Total |
|---|---|---|---|
| Centre | |||
| Southampton | 25 | 27 | 52 |
| Liverpool | 31 | 28 | 59 |
| London | 40 | 38 | 78 |
|
| |||
| List size | |||
| Small | 34 | 32 | 66 |
| Large | 62 | 61 | 123 |
|
| |||
| Location | |||
| Urban | 77 | 77 | 154 |
| Rural | 19 | 16 | 35 |
Recruitment of patients
Of 11 468 patients approached in consultations or through mailed invitations, 1058 (9.2%) returned reply slips; 574/5429 (10.6%) patients approached in the intervention arm and 484/6039 (8.0%) patients approached in the control (Figure 1). After exclusion of patients declining participation, ineligible, or uncontactable, 529 were assessed at baseline: 302/5429 (5.5%) in the intervention arm and 227/6039 (3.8%) in the control, between January 2019 and March 2022. The ratio of intervention to control arm patients was therefore 1.3 to 1.
Figure 1.
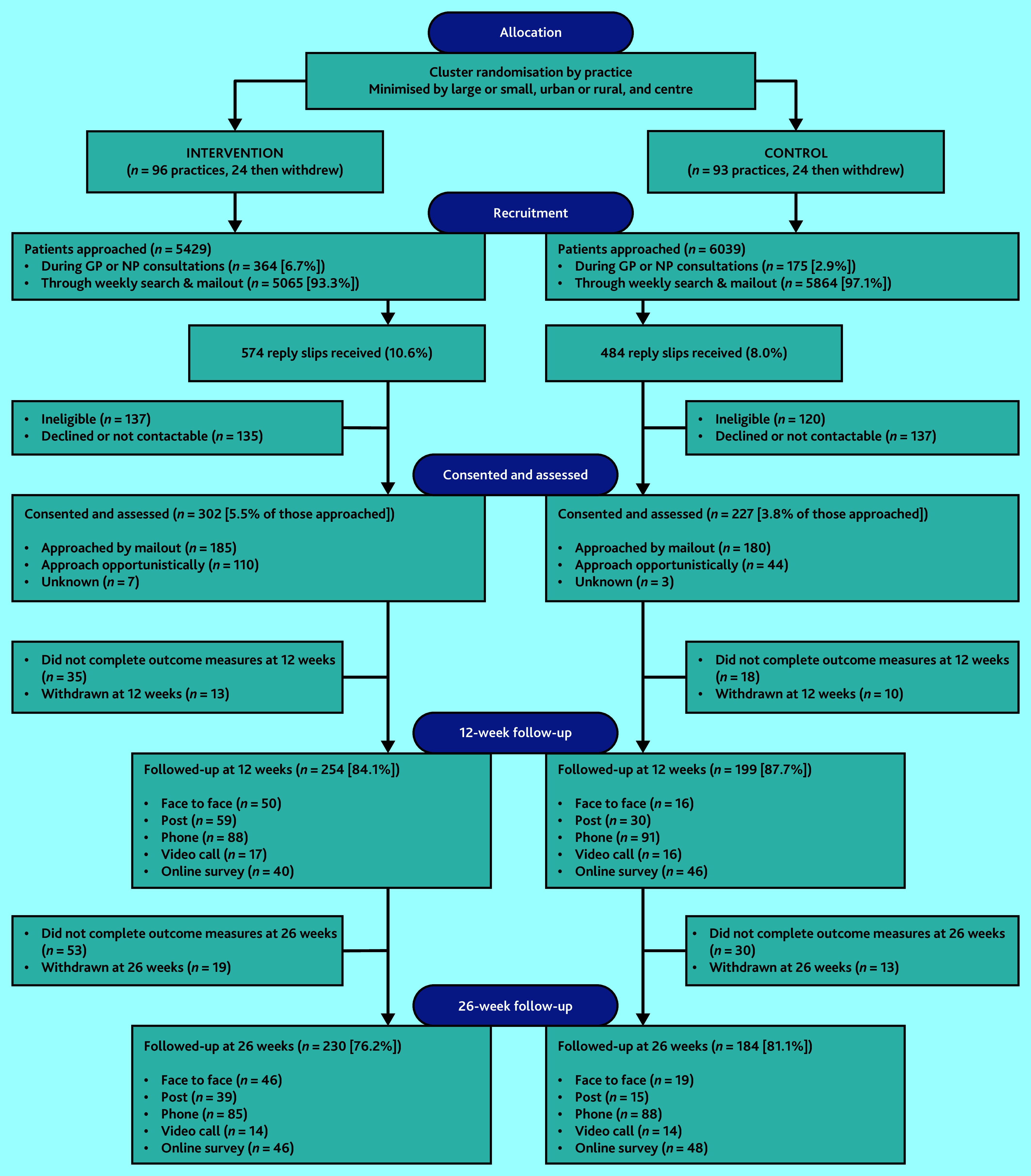
CONSORT diagram. NP = nurse practitioner. NB: 58 intervention arm patients who missed follow-up at 12 weeks returned to follow-up at 26 weeks.
Follow-up of patients
Of 529 patients recruited, 453 (85.6%) were followed up at 12 weeks: 254/302 in the intervention arm (84.1%) and 199/227 in the controls (87.7%). At 26 weeks, 414 (78.3%) were followed-up: 230/302 in the intervention arm (76.2%) and 184/227 (81.1%) in the controls (Figure 1). Medical records data were collected for 259 (85.8%) patients in the intervention arm and 201 (88.5%) controls.
Baseline characteristics
Mean baseline BDI-II score was higher in the intervention arm at 24.1 (SD 8.89) compared with 22.4 (SD 9.52) in the control (Table 2). Baseline anxiety and quality of life were also worse in the intervention arm. Patients in the control arm were more likely to have had two or more previous depressive episodes. Sociodemographic characteristics were relatively well-balanced, apart from patients in the control arm being more likely to have no dependants (Table 2).
Table 2.
Participating patient characteristics at baseline
| Characteristic | Intervention (n = 302) | Control (n = 227) | Total (n = 529) |
|---|---|---|---|
| Mean baseline depression score on the BDI-II (SD) | 24.1 (8.89) | 22.4 (9.52) | 23.4 (9.2) |
|
| |||
| Mean baseline anxiety score on the GAD-7 (SD) | 12.8 (5.31) | 11.8 (5.58) | 12.4 (5.45) |
|
| |||
| Mean baseline quality-of-life score on the EQ-5D-5L (SD) | 0.659 (0.232) | 0.667 (0.226) | 0.663 (0.230) |
|
| |||
| Mean duration of depression in years (SD) | 3.4 (5.13) | 2.6 (5.56) | 3.1 (5.33) |
|
| |||
| Previous depression, n (%) | |||
| None | 87 (28.8) | 46 (20.3) | 133 (25.1) |
| Once before | 79 (26.2) | 62 (27.3) | 141 (26.7) |
| Twice or more before | 135 (44.7) | 119 (52.4) | 254 (48.0) |
|
| |||
| Female, n (%) (Self-declared gender) | 192 (63.6) | 136 (59.9) | 328 (62.0) |
|
| |||
| Mean age in years at baseline (SD) | 45.2 (15.94) | 45.0 (17.17) | 45.1 (16.46) |
|
| |||
| Ethnic group, n (%) | |||
| White | 255 (84.4) | 193 (85.0) | 448 (84.9) |
| Black Caribbean | 1 (0.3) | 3 (1.3) | 4 (0.8) |
| Black African | 3 (1.0) | 4 (1.8) | 7 (1.3) |
| Black other | 2 (0.7) | 0 (0.0) | 2 (0.4) |
| Indian | 13 (4.3) | 4 (1.8) | 17 (3.2) |
| Pakistani | 6 (2.0) | 4 (1.8) | 10 (1.9) |
| Bangladeshi | 0 (0.0) | 1 (0.4) | 1 (0.2) |
| Chinese | 4 (1.3) | 3 (1.3) | 7 (1.3) |
| Other Asian group | 5 (1.7) | 3 (1.3) | 8 (1.5) |
| Other ethnic group | 12 (4.0) | 12 (5.3) | 24 (4.5) |
|
| |||
| Socioeconomic position, n (%) | |||
| Full-time work | 140 (46.4) | 113 (49.8) | 253 (47.8) |
| Part-time work | 55 (18.2) | 28 (12.3) | 83 (15.7) |
| Permanently sick or disabled | 5 (1.7) | 6 (2.6) | 11 (2.1) |
| Unemployed | 36 (11.9) | 18 (7.9) | 54 (10.2) |
| Retired | 33 (10.9) | 31 (13.7) | 64 (12.1) |
| Student | 8 (2.6) | 12 (5.3) | 20 (3.8) |
| Homemaker | 5 (1.7) | 4 (1.8) | 9 (1.7) |
| Voluntary work | 6 (2.0) | 4 (1.8) | 10 (1.9) |
| Other | 14 (4.6) | 11 (4.8) | 25 (4.7) |
|
| |||
| Accommodation, n (%) | |||
| Owner-occupied | 142 (47.0) | 106 (46.7) | 248 (46.9) |
| Council or housing association | 39 (12.9) | 20 (8.8) | 59 (11.2) |
| Private rental | 71 (23.5) | 57 (25.1) | 128 (24.2) |
| Job related | 2 (0.7) | 1 (0.4) | 3 (0.6) |
| Lives with parents | 40 (13.2) | 34 (15.0) | 74 (14.0) |
| Other | 8 (2.6) | 9 (4.0) | 17 (3.2) |
|
| |||
| Highest educational qualification,a n (%) | |||
| None | 26 (8.6) | 20 (8.8) | 46 (8.7) |
| CSE or NVQ Level 1 | 22 (7.3) | 3 (1.3) | 25 (4.7) |
| GCSE or O Level | 49 (16.2) | 33 (14.5) | 82 (15.5) |
| A Level or BTEC | 54 (17.9) | 41 (18.1) | 95 (18.0) |
| HNC, HND or City & Guilds | 24 (8.0) | 16 (7.0) | 40 (7.6) |
| Degree or higher degree | 111 (36.8) | 90 (39.6) | 201 (38.0) |
| Vocational qualification | 8 (2.6) | 14 (6.2) | 22 (4.2) |
| Other | 5 (1.7) | 8 (3.5) | 13 (2.5) |
|
| |||
| Marital status, n (%) | |||
| Married | 119 (39.4) | 83 (36.6) | 202 (38.2) |
| Cohabiting | 26 (8.6) | 26 (11.5) | 52 (9.8) |
| Widowed | 10 (3.3) | 10 (4.4) | 20 (3.8) |
| Separated | 11 (3.6) | 6 (2.6) | 17 (3.2) |
| Divorced | 25 (8.3) | 13 (5.7) | 38 (7.2) |
| Single | 111 (36.8) | 89 (39.2) | 200 (37.8) |
|
| |||
| Number of dependants in the household, n (%) | |||
| None | 174 (57.6) | 151 (66.5) | 325 (61.4) |
| 1 | 43 (14.2) | 34 (15.0) | 77 (14.6) |
| 2 | 56 (18.5) | 26 (11.5) | 82 (15.5) |
| 3 | 15 (5.0) | 11 (4.8) | 26 (4.9) |
| 4 | 9 (3.0) | 3 (1.3) | 12 (2.3) |
| 5 | 2 (0.7) | 0 (0.0) | 2 (0.4) |
CSE is the Certificate of Secondary Education, a qualification in a specific subject formerly taken by school students aged 14–16 years, at a level below O (Ordinary) level. Both the CSE and O level were replaced in 1988 by the GCSE, or General Certificate of Secondary Education. NVQ Level 1 is the first level National Vocational Qualification, a work-based job-specific qualification. A Level is the Advanced secondary education qualification in a specific subject taken by school students aged 17–19 years. BTEC is the Business and Technology Education Council certificate work-based vocational qualification taken after secondary school for aged >16 years. HNC (Higher National Certificate), HND (Higher National Diploma), and City & Guilds are more advanced vocational qualifications. BDI-II = Beck Depression Inventory, Second Edition. GAD-7 = Generalised Anxiety Disorder assessment. SD = standard deviation. NB: Where the values do not add up to the total n followed up, it is because some patients did not answer all questions and therefore there are missing values for some items.
Primary outcome
At 12 weeks follow-up, the mean BDI-II score was 18.5 (SD 10.2) in the intervention arm and 16.9 (10.3) in the control (Table 3 and Figure 2). The adjusted mean score was slightly lower in the intervention arm, but not statistically significant (adjusted mean difference −0.46; 95% confidence interval (CI) = −2.16 to 1.26; P = 0.60).
Table 3.
Primary and secondary outcomes at baseline, 12 weeks, and 26 weeks follow-up
| Baseline | 12 weeks | 26 weeks | ||||||
|---|---|---|---|---|---|---|---|---|
|
| ||||||||
| n | Mean score (SD) | n | Mean score (SD) | Mean adjusted differencea (95% CI); P-value | n | Mean score (SD) | Mean adjusted differencea (95% CI); P-value | |
| Depression (BDI-II score) | ||||||||
| Intervention | 302 | 24.1 (8.96) | 252 | 18.5 (10.17) | −0.46 (−2.16 to 1.26); P = 0.602 | 226 | 15.1 (10.84) | −1.63 (−3.48 to 0.21); P = 0.082 |
| Control | 227 | 22.4 (9.52) | 195 | 16.9 (10.30) | REF | 184 | 14.7 (10.65) | REF |
|
| ||||||||
| Social functioning (WSAS score) | ||||||||
| Intervention | 302 | 17.3 (9.94) | 237 | 14.7 (9.54) | 0.48 (−1.03 to 2.00); P = 0.531 | 212 | 11.6 (9.59) | 1.34 (−3.20 to 0.53); P = 0.160 |
| Control | 227 | 16.6 (10.06) | 195 | 13.2 (9.90) | REF | 183 | 12.0 (9.99) | REF |
|
| ||||||||
| Quality of Life (EQ-5D-5L score) | ||||||||
| Intervention | 302 | 0.659 (0.232) | 256 | 0.694 (0.236) | −0.002 (−0.0412 to 0.0372) P = 0.94 | 221 | 0.718 (0.249) | 0.053 (0.013 to 0.093); P = 0.01 |
| Control | 226 | 0.667 (0.226) | 197 | 0.708 (0.213) | REF | 183 | 0.696 (0.225) | REF |
|
| ||||||||
| Satisfaction with care (MISS total score) | ||||||||
| Intervention | 302 | N/A | N/A | 217 | 121.8 (27.37) | 5.39 (−1.39 to 12.16); P = 0.119 | ||
| Control | 227 | N/A | N/A | 176 | 116.0 (26.75) | REF | ||
Adjusted for baseline value, baseline anxiety (GAD-7 score), sociodemographics, past history of depression, and practice as a random effect. BDI-II = Beck Depression Inventory, Second Edition. GAD-7 = Generalised Anxiety Disorder questionnaire. MISS = Medical Interview Satisfaction Scale. REF = reference value. WSAS = Work and Social Adjustment Scale.
One patient withdrew immediately after enrolment and did not complete an EQ-5D-5L at baseline.
Figure 2.

Mean BDI-II depression scores at baseline, 12 weeks, and 26 weeks follow-up.
At 26 weeks both groups improved further on the BDI-II (Table 3 and Figure 2). The score was slightly lower in the intervention arm, but not significantly (adjusted mean difference −1.63; 95% CI = −3.48 to 0.21; P = 0.08). The 95% CI included a difference favouring the intervention by more than 3.0 points on the BDI-II so a clinically important difference in depression at 26 weeks could not be excluded.
As a sensitivity analysis, the primary outcome was re-analysed using a multiple imputation model, including the baseline value, clustering by practice, and all covariates included in the model. The inferences at 12 and 26 weeks were unchanged (adjusted mean difference at 12 weeks −0.18; 95% CI = −1.82 to 1.45; P = 0.83, and at 26 weeks −0.93; 95% CI = −2.69 to 0.83; P = 0.30).
Secondary outcomes
A similar pattern was seen for social functioning at 12 and 26 weeks, with scores improving between baseline and 12 weeks, and further by 26 weeks, but no significant difference between arms (Table 3).
Quality of life improved in both arms between baseline and 12 weeks, then improved further in the intervention arm, but went down slightly in the control (Table 3 and Figure 3). The difference between arms was not statistically significant at 12 weeks but was significant at 26 weeks, favouring the intervention (adjusted mean difference 0.053; 95% CI = 0.013 to 0.093; P = 0.01).
Figure 3.

Mean EQ-5D-5L quality-of-life scores at baseline, 12 weeks, and 26 weeks follow-up.
Patient ratings in the two arms were similar at baseline on the EQ-5D-5L subscales for mobility, self-care, and pain or discomfort, and remained so (Supplementary Table S1). Slightly more patients in the intervention declared severe or extreme problems for anxiety and depression at baseline (23.5% versus 19.5%). At 26 weeks follow-up, the proportions declaring no problem with anxiety and depression were 22.6% in the intervention arm versus 13.5% in the control. Improvement in the anxiety and depression dimension therefore explained the overall greater improvement in scores in the intervention arm.
Total scores for satisfaction with care looking back over 26 weeks were very similar between arms (Table 3). The mean score for the intervention arm was 121.8 and 116.0 for the control arm. The same was found for all four satisfaction subscales (Distress–relief, Communication–comfort, Rapport, and Compliance–intent).
Post-hoc analysis of 50% improvement, and remission, at 26 weeks
A post-hoc analysis was conducted of categorical improvements in BDI-II scores at 26 weeks, to further investigate differences in depression, given the wide CIs around the mean difference, and because of the difference that was found in proportions of patients reporting no anxiety and depression on the EQ-5D-5L at 26 weeks (Supplementary Table S1). The proportions in each arm who improved by ≥50% on the BDI-II, were compared with the proportions who scored >13 at baseline (the threshold for ‘caseness’) and subsequently remitted to ≤13 by 26 weeks.
The proportions of patients improving by ≥50% were not significantly different (102/226 intervention [45.1%] versus 69/185 [37.3%] controls; OR 1.53; 95% CI = 0.92 to 2.56; P = 0.10), but the proportion of patients remitting in the intervention arm was significantly greater (100/201 [49.8%] versus 59/148 [39.9%]; OR 2.18; 95% CI = 1.12 to 4.24; P = 0.02).
Post-hoc per-protocol analysis of depression outcome
In the intervention arm 190 out of 259 patients (73.4%) had PHQ-9s recorded in the medical record, and in the control arm 35 out of 201 patients (17.4%). However, around half of those recorded were the baseline PHQ-9s carried out by the researchers. Only 124 patients had recorded PHQ-9s carried out by their GPs during follow-up: 106 in the intervention arm (40.9%) and 18 in the control arm (8.9%).
Post-hoc, GP compliance was defined with the protocol in the intervention arm as carrying out and recording a follow-up PHQ-9, and in the control arm with not carrying out and recording one. On that basis, a post-hoc per-protocol analysis of depression outcome was carried out for the 106 intervention participants with a recorded follow-up PHQ-9, compared with that for the 209 control participants without a recorded follow-up PHQ-9. At 12 weeks the fully adjusted difference in BDI-II score was −1.57 points (95% CI = −3.47 to 0.35; P = 0.108) and at 26 weeks −1.08 (95% CI = −3.40 to 1.24; P = 0.361), so there were no significant differences in depression symptom counts at either point.
Use of antidepressants
Medical records data were obtained for 259 intervention arm patients (85.8%) and 201 controls (88.5%). Of these 174 (67.2%) and 112 (55.7%), respectively, had antidepressant prescriptions recorded over 26 weeks, but the difference between arms was not significant (odds ratio (OR) 1.83; 95% CI = 0.96 to 3.48; P = 0.07, adjusted for baseline depression, baseline anxiety, baseline antidepressant use, sociodemographics, and practice).
A post-hoc per-protocol analysis found that of the 106 patients in the intervention with a recorded follow-up PHQ-9, 71 (67.0%) received a prescription for antidepressants, compared with 102/183 (55.7%) of the 209 controls with no recorded follow-up PHQ-9. The adjusted OR was 2.80 (95% CI = 1.14 to 6.88; P = 0.025), showing significantly more antidepressant prescribing in those with a recorded follow-up PHQ-9 administered by the GP.
Contact with mental health and social services
In their records, 90 out of 259 patients in the intervention arm (34.7%) and 68 out of 201 controls (33.8%) had contacts over 26 weeks with mental health and social services (mental health nurse, counsellor, psychologist, psychiatrist, and social workers), which were not significantly different between arms (adjusted OR 1.37; 95% CI = 0.71 to 2.63; P = 0.342).
In a post-hoc per-protocol analysis, 48 (45.3%) of the 106 patients in the intervention arm with a recorded follow-up PHQ-9 had a mental health service contact, compared with 57/183 (31.1%) of the controls with no follow-up PHQ-9. The adjusted OR was 3.96 (95% CI = 1.38 to 11.34; P = 0.010) showing significantly more mental health contacts for those with a recorded follow-up PHQ-9 administered by the GP.
Adverse events
There were two serious adverse events. One patient in the control arm reported suicidal ideas; they were assessed by the trial principal investigator and found to be at higher risk, and the GP was informed immediately. The patient was referred to a community mental health team (CMHT) for immediate assessment and withdrawn from the study. One patient in the intervention arm was hospitalised with COVID-19 and ketoacidosis: a severe event, but not related to the trial.
The suicidal ideation SOP was triggered 318 times, 180 times for patients in the intervention arm patients, and 138 times for controls, in proportion to patient numbers in each arm. Altogether, 267 (146 intervention, 121 control) were rated ‘minimal risk’, 38 (25 intervention, 13 control) ‘lower risk’, and 13 (nine intervention, four control) ‘higher risk’. In four cases (two intervention and two control) participants were withdrawn from the study.
Discussion
Summary
No significant difference was found between the intervention and control arms in the primary outcome, which was depression on the BDI-II at 12 weeks. However, it was not possible to rule out a clinically significant benefit at 26 weeks, given the upper limit of the 95% CI included the MCID of 3.0 points.13 Evidence was found of benefit in a categorical analysis of remission of depression to a BDI-II <13 at 26 weeks, but this was a post-hoc analysis, and there was no significant difference in a similar analysis of the proportions of patients with a 50% improvement in depression.
There were no significant differences found in social functioning and satisfaction with care, although the differences found tended to favour the intervention. Quality-of-life scores were, however, significantly higher in the intervention arm at 26 weeks. The better quality-of-life score was owing to a greater proportion of patients in the intervention arm reporting no anxiety and depression. Anxiety symptoms were not measured specifically at follow-up, but it may be that some patients were reassured to see their depression was improving, and therefore felt less anxious.
Overall, more patients in the intervention arm than controls had recorded antidepressant prescriptions over 26 weeks (67.4% versus 55.7%), but this difference was not statistically significant. There was no overall difference in mental health and social service contacts either, with one-third of patients in both arms having at least one. However, in post-hoc per-protocol analyses, including only those patients in the intervention arm who had follow-up PHQ-9s administered and recorded by their GPs, there was significantly greater antidepressant prescribing and contact with mental health services than among controls with no follow-up monitoring.
Strengths and limitations
A strength of the study is that its design was informed by a feasibility trial,12 which led to choosing the cluster design, avoiding contamination between arms in applying the intervention, and optimising adherence to study procedures in practices. However, a cluster randomised design increases the risk of selection bias among practitioners deciding whether to approach patients opportunistically in consultations. More than twice as many patients in the intervention arm than control arm were recruited opportunistically, and overall the ratio of patients randomised was 1.3 to 1, which may have reflected lower motivation to take part on the part of patients in the control arm, who were offered only usual care. Selection bias may explain higher baseline depression and anxiety scores, and lower quality of life, in the intervention arm, although the two arms were relatively well-balanced in terms of patient demographics, and analyses were adjusted for baseline differences.
Participating practitioners were trained in both the use of the PHQ-9 and treatment choices related to severity scores, while considering contextual factors. The amount of training was limited to 2 hours but was considered an amount feasible to offer at scale.
Recruitment to the trial was challenging, particularly during the COVID-19 pandemic, when practices had significant extra pressures. The revised target of 554 patients was not quite achieved, by 25, but the follow-up rate of 85.6% was better than predicted and primary outcome data were gathered on sufficient participants to answer the main research question with precision, so the result for the primary outcome may be regarded as robustly negative. It is possible, however, that there was a difference in depression at 26 weeks, which was missed owing to lacking power at that point.
It was not possible to blind participants and researchers given the pragmatic cluster design, but self-report outcome measures avoided possible observer bias, and the statistical analyses were all carried out blind to allocation.
Delivering the intervention was challenging, and not as it would be in routine practice. Practitioners could not administer the PHQ-9 when patients first presented with depression, because patients had to be given information about the study and at least 24 hours to consider taking part before consenting. This was a requirement of the NHS Research Ethics Committee. To avoid asking the GP to bring the patient back to administer the first PHQ-9, the researcher administered it at baseline assessment instead. Treatment could therefore have started at the initial consultation before the baseline score could be taken into account.
As only 73.4% of patients in the intervention arm had PHQ-9s recorded in their records, the GPs obviously did not record their scores routinely, since it is known 100% had PHQ-9s administered by the researchers at baseline, and these were all communicated to the practices. Only 40.9% of patients in the intervention arm had follow-up, GP-administered PHQ-9s recorded, although the actual numbers of follow-up PHQ-9s carried out may well have been higher. The GPs in the intervention arm were asked to administer follow-up PHQ-9s with all their participating patients but did not insist that they recorded the follow-up PHQ-9s, which is a limitation of the study. Effectively, instituting a policy of monitoring using the PHQ-9 was tested, which was known would not necessarily be carried out per protocol, which would likely be the case to a greater extent in routine practice.
The resources were not available to collect detailed information in real-time of individual GPs’ patient treatment plans and whether they were changed following PHQ-9 assessment at follow-up. However, the post-hoc per-protocol analyses, indicating that significantly increased antidepressant prescribing, and mental health service contacts were associated with carrying out and recording follow-up PHQ-9s, suggested that the GPs may have increased antidepressant treatment and referrals to specialist services on finding less than desired improvements in scores at follow-up.
A smaller proportion (17.4%) of patients in the control arm also had at least one PHQ-9 recorded, despite the fact practitioners in the control arm were asked not to use them. These may have been administered outside practices in psychology services, or by temporary practitioners within practices. However, this was a relatively low level of use, so there was good differentiation between the arms, and the pre-specified analyses were conducted on an intention-to-treat basis.
There were relatively few exclusion criteria, tending to increase the heterogeneity of the sample and generalisability of the findings. The computer codes used to identify patients through the records searches included symptom codes (for example, ‘low mood’) in addition to specific diagnoses (for example, ‘depressive disorder’), to avoid missing patients not given a specific diagnosis.
However, there was a relatively large drop-off from the 11 468 patients approached to take part down to the 529 who eventually consented and were enrolled in the study, only 5.5% of those approached in the intervention arm, and 3.8% in the control.
Comparison with previous literature
The findings are consistent with previous trials that have mostly shown no benefit for depression outcome. Only one trial found a reduction in depression,17 but no changes in management to explain the benefit.18 Two others found changes in management but not outcomes.19,20 The most recent found no difference in depression, but reduced anxiety at 8 weeks, and improved functioning at 24 weeks follow-up.21
Evidence of benefit from PROMs has been found in psychological therapy settings including improved outcome,22 and making therapy more efficient.23 However, in psychological services PROMs are given multiple times during therapy, and facilitate adjustment of treatment. With only 1–2 PHQ-9s given in the present study, the information available to GPs was more restricted. PROMs used in monitoring progress in psychological services are also more extensive than the PHQ-9 alone, and the implications of results for therapy are discussed with supervisors between sessions.22, 23 Finally, psychological services offer a range of evidence-based treatments, whereas GP treatment is largely antidepressants alone, and may be less effective in changing depression outcome.1
Implications for research and practice
The absence of evidence for improvement in the outcome of depression from studies of follow-up monitoring with PROMs in primary care suggests that guidelines that recommend their use1–4 should continue to make them discretionary rather than mandatory, at least outside psychological therapy settings, where there is good evidence of benefit. Monitoring patients who like to see improvement in their scores is justifiable, as it may improve their quality of life. The post-hoc analyses also suggest that conducting and recording follow-up PHQ-9s may lead to greater antidepressant prescribing and referrals to mental health services. However, their use is not without cost, in terms of the time taken, even though they are relatively cheap. The cost-effectiveness of using the PHQ-9 in this study will be reported separately.
In addition, continuing to recommend outcome monitoring with PROMs may be justified based on providing greater transparency to health service funders and the public about the management of depression and patients’ responses to particular treatments.
Future research on depression monitoring in primary care should improve the delivery of monitoring and test PROMs, which cover anxiety and social functioning as well as depression. PROMS should be completed remotely between consultations; facilitated by automated analysis and feedback of the results to practitioners and patients; and specific recommendations for treatment should be delivered. Practitioners interpreting PROM results will still need to consider the circumstances surrounding individuals’ histories of depression, and responses to treatments.
Acknowledgments
To see the author contributions, please see Supplementary Information S6. Thanks to the following: Professor Bernd Löwe of the University of Hamburg, an international adviser; Sophie Johnson, Ben Hammond, and Charlotte Hookham in Southampton, Daniel Lawrence and Taylor Hooper in Liverpool, and Paula Beharry and Thomas Gant at University College London, who provided administrative support; Tammy Thomas and Louisa Little, who provided oversight from the Southampton Clinical Trials Unit; Claire Winch, Debbie Kelly, Nicola Blakey, Heather Kenyon and Nnenna Omeje, of Thames Valley and South Midlands Clinical Research Network, who provided assistance with data collection. Thanks to the Trial Steering committee (TSC) members who were: Michael Barkham (academic psychologist and chair); Susan Collinson (PPI representative); Laura Gray (statistician); Stavros Petrou (health economist); and Linda Gask (academic psychiatrist). Thanks also to the trial Independent Data Monitoring Committee (IDMC) members who were Richard Byng (academic GP and chair), Jill Mollison (statistician), and Jaime Delgadillo (academic psychologist). Most of all, many thanks to the participating patients and practitioners at the practices, which are detailed in Supplementary Information S6.
Funding
This project was funded by the National Institute for Health and Social Care Research (NIHR) Health Technology Assessment programme (grant reference no. HTA 17/42/02). The views expressed in this publication are those of the authors and not necessarily those of the NIHR or the Department of Health and Social Care.
Ethical approval
The study was approved by the West of Scotland NHS Research Ethics Committee 5, on 21 September 2018 (ref: 18/WS/0144).
Data
Our research ethics permission is for use of the data by the research team only. Applications to use the data need to be in the form of a peer-reviewed protocol, and will be considered by the three lead investigators, Tony Kendrick, Glyn Lewis and Mark Gabbay, in the first instance, before a decision on data sharing will be taken by the rest of the co-authors. Qualitative data will not be shared, due to the relatively high risk of breaches of confidentiality arising from the nature of qualitative interviews, which are difficult to make completely anonymous.
Provenance
Freely submitted; externally peer reviewed.
Competing interests
All authors completed a disclosure form at: http://www.icmje.org/coi_disclosure.pdf. For further details, see Supplementary Information S5.
Patient and public involvement
The authors are grateful for the patient and public involvement. See Supplementary Information S6 for details.
Trial registration number
International Standard Randomised Controlled Trial Number (ISRCTN) no: 17299295.
Discuss this article:
References
- 1.National Institute for Health and Care Excellence (NICE) Depression in adults: treatment and management. NICE guideline [NG222] 2022. https://www.nice.org.uk/guidance/ng222/chapter/Recommendations#recognition-and-assessment (accessed 20 March 2024). [PubMed]
- 2.Health Resources and Services Administration Uniform Data System Clinical Quality Measures. 2020 https://bphc.hrsa.gov/sites/default/files/bphc/data-reporting/2020-clinical-measures-handout.pdf (accessed 20 March 2024). [Google Scholar]
- 3.Kaiser Permanente Mental health monitoring tool. https://wa-provider.kaiserpermanente.org/static/pdf/provider/patient-ed/screenings/bhi-monitoring-tool.pdf (accessed 20 March 2024). [Google Scholar]
- 4.Nederlands Huisartsen Genootschap (Dutch Society of General Practitioners) NHG guideline on depression. 2019 https://richtlijnen.nhg.org/standaarden/depressie#volledige-tekst-3-beoordelen-van-de-ernst-van-de-depressieve-stoornis (accessed 20 March 2024). [Google Scholar]
- 5.Kendrick T, El-Gohary M, Stuart B, et al. Routine use of patient reported outcome measures (PROMs) for improving treatment of common mental health disorders in adults. Cochrane Database Syst Rev. 2016 doi: 10.1002/14651858.CD011119.pub2. DOI: . [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Kendrick T, Maund E. Do PROMS improve outcomes in patients with depression in primary care? BMJ. 2020 doi: 10.1136/bmj.m3313. DOI: . [DOI] [PubMed] [Google Scholar]
- 7.Spitzer RL, Kroenke K, Williams JB. Validation and utility of a self-report version of PRIME-MD: the PHQ primary care study. Primary Care Evaluation of Mental Disorders. Patient Health Questionnaire. JAMA. 1999;282(18):1737–1744. doi: 10.1001/jama.282.18.1737. [DOI] [PubMed] [Google Scholar]
- 8.Beck AT, Steer RA, Brown GK. Manual for the Beck Depression Inventory-II. San Antonio, TX: Psychological Corporation; 1996. [Google Scholar]
- 9.Mundt JC, Marks IM, Shear MK, Greist JH. The Work and Social Adjustment Scale: a simple measure of impairment in functioning. Br J Psychiatry. 2002;180:461–464. doi: 10.1192/bjp.180.5.461. [DOI] [PubMed] [Google Scholar]
- 10.EuroQol Research Foundation EQ-5D-5L. 2024. https://euroqol.org/information-and-support/euroqol-instruments/eq-5d-5l/
- 11.Meakin R, Weinman J. The ‘Medical Interview Satisfaction Scale’ (MISS-21) adapted for British general practice. Fam Pract. 2002;19(3):257–263. doi: 10.1093/fampra/19.3.257. [DOI] [PubMed] [Google Scholar]
- 12.Kendrick T, Stuart B, Leydon GM, et al. Patient-reported outcome measures for monitoring primary care patients with depression: PROMDEP feasibility randomised trial. BMJ Open. 2017 doi: 10.1136/bmjopen-2016-015266. DOI: . [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Button KS, Kounali D, Thomas L, et al. Minimal clinically important difference on the Beck Depression Inventory—II according to the patient’s perspective. Psychol Med. 2015 doi: 10.1017/S0033291715001270. DOI: . [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Spitzer RL, Kroenke K, Williams JB, Löwe B. A brief measure for assessing generalized anxiety disorder: the GAD-7. Arch Intern Med. 2006;166(10):1092–1097. doi: 10.1001/archinte.166.10.1092. [DOI] [PubMed] [Google Scholar]
- 15.Dube P, Kurt K, Bair MJ, et al. The P4 screener: evaluation of a brief measure for assessing potential suicide risk in 2 randomized effectiveness trials of primary care and oncology patients. Prim Care Companion J Clin Psychiatry. 2010;12(6):PCC.10m00978. doi: 10.4088/PCC.10m00978blu. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Kendrick T, Moore M, Leydon G, et al. Patient-reported outcome measures for monitoring primary care patients with depression (PROMDEP): study protocol for a randomised controlled trial. Trials. 2020 doi: 10.1186/s13063-020-04344-9. DOI: . [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Yeung AS, Jing Y, Brenneman SK, et al. Clinical Outcomes in Measurement-based Treatment (COMET): a trial of depression monitoring and feedback to primary care physicians. Depress Anxiety. 2012 doi: 10.1002/da.21983. DOI: . [DOI] [PubMed] [Google Scholar]
- 18.Chang TE, Jing Y, Yeung AS, et al. Effect of communicating depression severity on physician prescribing patterns: findings from the Clinical Outcomes in Measurement-based Treatment (COMET) trial. Gen Hosp Psychiatry. 2012;34(2):105–112. doi: 10.1016/j.genhosppsych.2011.12.003. [DOI] [PubMed] [Google Scholar]
- 19.Mathias SD, Fifer SK, Mazonson PD, et al. Necessary but not sufficient: the effect of screening and feedback on outcomes of primary care patients with untreated anxiety. J Gen Intern Med. 1994 doi: 10.1007/BF02600303. DOI: . [DOI] [PubMed] [Google Scholar]
- 20.Wikberg C, Westman J, Petersson EL, et al. Use of a self-rating scale to monitor depression severity in recurrent GP consultations in primary care — does it really make a difference? A randomised controlled study. BMC Fam Pract. 2017 doi: 10.1186/s12875-016-0578-9. DOI: . [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Browning M, Bilderbeck AC, Dias R, et al. The clinical effectiveness of using a predictive algorithm to guide antidepressant treatment in primary care (PReDicT): an open-label, randomised controlled trial. Neuropsychopharmacology. 2021 doi: 10.1038/s41386-021-00981-z. DOI: . [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Delgadillo J, de Jong K, Lucock M, et al. Feedback-informed treatment versus usual psychological treatment for depression and anxiety: a multisite, open-label, cluster randomised controlled trial. Lancet Psychiatry. 2018 doi: 10.1016/S2215-0366(18)30162-7. DOI: . [DOI] [PubMed] [Google Scholar]
- 23.Delgadillo J, Overend K, Lucock M, et al. Improving the efficiency of psychological treatment using outcome feedback technology. Behav Res Ther. 2017 doi: 10.1016/j.brat.2017.09.011. DOI: . [DOI] [PubMed] [Google Scholar]