

Abstract
Symptoms of papillary fibroelastomas are often related to thromboembolic events but are rarely caused by a mechanical impairment of blood supply by the tumor itself. We describe a case of a papillary fibroelastoma in a 91-year-old female patient leading to a cardiac arrest through intermittent occlusion of the left coronary artery.
Keywords: tumor, histology, cardiac, aortic valve & root, heart disease
Introduction
Papillary fibroelastoma is a rare benign primary cardiac tumor. In most cases, it does not cause any symptoms. 1 If symptoms occur, they are consequences of embolization of either tumor fragments or adherent thrombus. 2 3 They result in stroke or myocardial infarction with potentially life-threatening consequences. Direct occlusion of a coronary artery by the tumor itself is rare and possibly diagnosed by an autopsy after a sudden cardiac death. 2 We describe a patient who presented with recurrent syncope and in-hospital cardiopulmonary resuscitation due to a mass adhering to the aortic valve.
Case Report
A 91-year-old female patient without any history of cardiovascular disease was admitted to the emergency department after syncope. Shortly after admission, the patient had a cardiac arrest with the need for cardiopulmonary resuscitation for 1 minute. Thereafter, blood pressure, heart rate, and left ventricular ejection fraction were within normal ranges. Computer tomography for excluding a pulmonary embolism showed a tumor attached to the aortic valve ( Fig. 1 ). In transesophageal echocardiography the circular, well-defined mass, 1.3 cm × 1 cm in size, was suspected a papillary fibroelastoma. After interdisciplinary discussion, the decision was made to surgically remove the mass. Intraoperatively, the neoplasm was confirmed to be in direct proximity to the orifice of the left main coronary artery ( Fig. 2 ). The tumor was removed in total. Because of the advanced age local cryotherapy, which may be applied in order to prevent recurrence, was not performed. 4 The aortic valve could be preserved. At the end of the surgery, transesophageal echocardiography showed normal heart function with a competent aortic valve. The patient was transferred to the intensive care unit. Further recovery was uneventful. The patient was transferred to a geriatric ward on the third postoperative day and discharged from hospital 17 day after surgery. The histopathological result confirmed the diagnosis of papillary fibroelastoma.
Fig. 1.
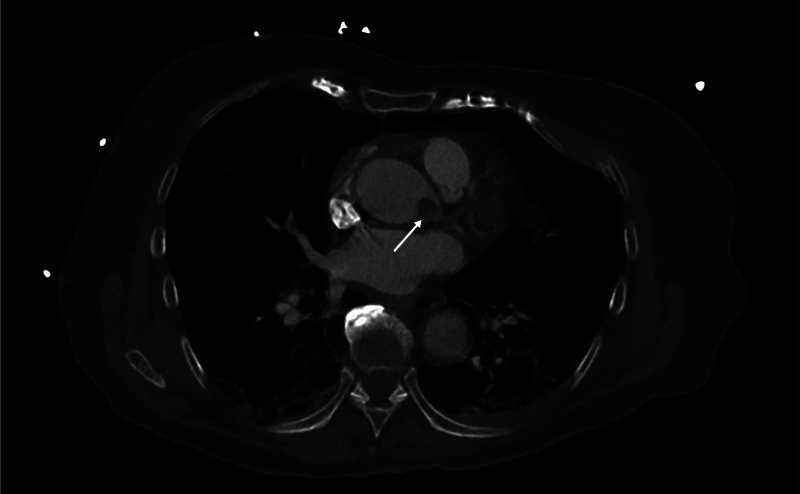
Computer tomographic scan showing a tumor in direct neighborhood to the orifice of the left coronary artery.
Fig. 2.
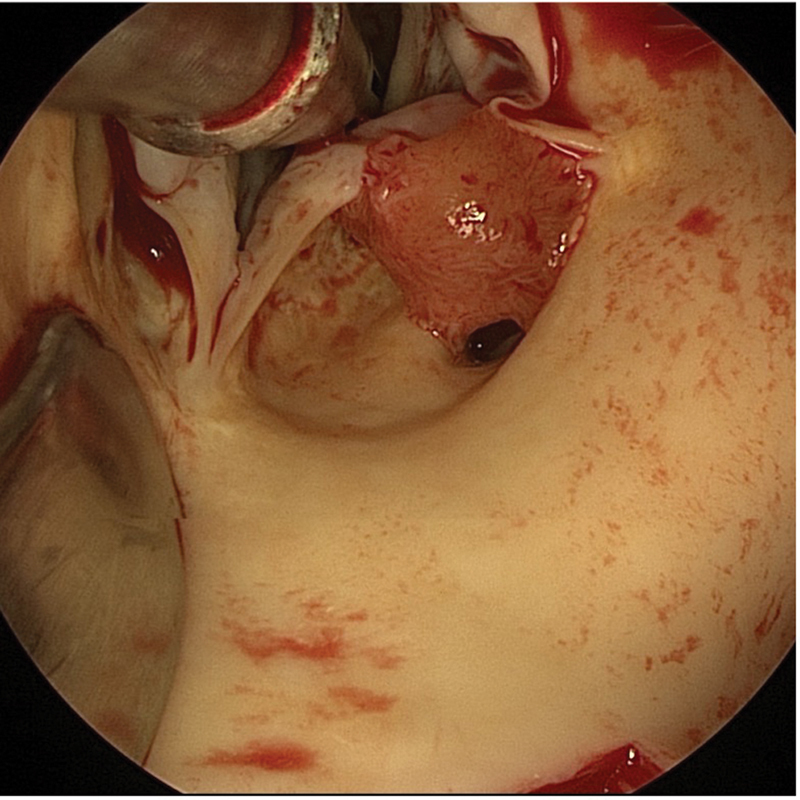
Intraoperative view of the aortic valve from above with the tumor attached to the left coronary cusp of the aortic valve partially obstructing the orifice of the left coronary artery.
Discussion
Primary cardiac tumors have an incidence of 0.02% and are mostly benign. 3 One of them is the papillary fibroelastoma, the third-most common primary cardiac neoplasm after myxoma and lipoma. 1 Even though it can arise from any endocardial tissue, it mostly affects the valves, predominantly any aortic cusp or mitral leaflet. 3 5 It is usually a small, mobile tumor with a diameter of about 1 cm with a frond-like, papillary appearance. 1 It is often found incidentally on transesophageal echocardiography performed for other reasons or detected on a CT scan after an embolic event. 1 3 Definitive diagnosis is made by a histopathologic examination. 1 Indications for surgery are large and mobile tumors. Curative treatment is complete resection of the tumor with the aim of preservation of the native valve. Hereafter, the recurrence rate is low. 5 6
Symptoms mostly occur after an embolic event. In rare cases, the tumor causes mechanical obstruction itself. In the present case, we found a fibroelastoma intermittently obstructing the left coronary artery orifice, responsible for resuscitation of the patient, as described above. Therefore, if a suspect mass arises near a coronary ostium the presence of a papillary fibroelastoma must be taken into consideration.
Footnotes
Conflict of Interest None declared.
References
- 1.Erdoes G, Stalder M, Basciani R, Gugger M, Carrel T, Eberle B. An uncommon cause of coronary artery ostial obstruction: papillary fibroelastoma. Echocardiography. 2010;27(03):337–340. doi: 10.1111/j.1540-8175.2009.01087.x. [DOI] [PubMed] [Google Scholar]
- 2.Chiba N, Matsuzaki M, Furuya S et al. Complete occlusion of the left main trunk coronary artery by a cardiac papillary fibroelastoma in a hemodynamically unstable patient. J Cardiol Cases. 2015;13(04):97–100. doi: 10.1016/j.jccase.2015.11.002. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Maleszewski J J, Bois M C, Bois J P, Young P M, Stulak J M, Klarich K W. Neoplasia and the heart: pathological review of effects with clinical and radiological correlation. J Am Coll Cardiol. 2018;72(02):202–227. doi: 10.1016/j.jacc.2018.05.026. [DOI] [PubMed] [Google Scholar]
- 4.Mandryk Y, Czesla M, Flora C, Massoudy P. Concomitant tumourous lesions in the left atrium and aortic valve suspected to be myxoma. Eur J Cardiothorac Surg. 2020;57(05):1011–1012. doi: 10.1093/ejcts/ezz314. [DOI] [PubMed] [Google Scholar]
- 5.Kouchoukos N T, Blackstone E H, Hanley F L, Kirklin J K. 4th ed. Chap. 18. Amsterdam, Netherlands: Elsevier Saunders; 2013. Cardiac tumor; pp. 750–759. [Google Scholar]
- 6.Sorour A A, Kurmann R D, El-Am E A et al. Recurrence of pathologically proven papillary fibroelastoma. Ann Thorac Surg. 2022;113(04):1208–1214. doi: 10.1016/j.athoracsur.2021.03.114. [DOI] [PubMed] [Google Scholar]