

Central venous catheterization establishes temporary, efficient, and rapid use of deep venous access in patients, which provides high flow rate fluid perfusion, enables measurement of central venous pressure, and acts as an important reference for clinical decision-making. However, various complications such as pneumothorax, hemothorax, hematoma, and puncture failure can easily occur during the puncture and catheterization process, which can impede its efficacy. Among these complications, accidental insertion of the puncture needle into the artery occasionally occurs, especially when inserting a thick sheath. Improper handling can lead to local hematoma, hemorrhagic shock, and immediate life-threatening risks. Relevant imaging examinations should be performed as soon as possible to determine the location of arterial injury and decide the correct therapeutic pathway. In this article, the author summarizes three recent cases wherein central venous catheterization inadvertently entered an artery. Finally, we proposed an algorithm to delineate the optimal treatment strategy to guarantee optimal management of these patients.
Here are three cases of supra-aortic arterial lesions treated with different techniques described.
Case 1 An 84-year-old male patient was diagnosed as acute heart failure. In order to provide essential support, a 7F left subclavian vein central venous catheter was inserted with the guidance of ultrasound imaging. The measurement of blood gases assessing a high degree of oxygenation confirmed the diagnosis of an arterial lesion. The patient was immediately transferred to the catheterization room, and the catheter was confirmed through the central venous catheter multi-position angiography (Figure 1A). Considering the relatively external puncture point, the relatively straight subclavian artery, and the large rib space suggested by palpation, the decision was made to remove the catheter and close the puncture site with a percutaneous vascular closure device. The 0.035J guide wire in the vascular occluder kit was inserted via the misplaced catheter, with the tip of the wire in the ascending thoracic aorta. The misplaced venous catheter was removed, and the Angio-Seal 8F vascular occluder was placed. Concurrently, 5F JR 3.5 angiogram catheter was pushed to the proximal part of the puncture site through the left radial artery. The angiogram confirmed that there was no extravasation of contrast, and his subclavian and vertebral arteries had normal patency (Figure 1B).
Figure 1.
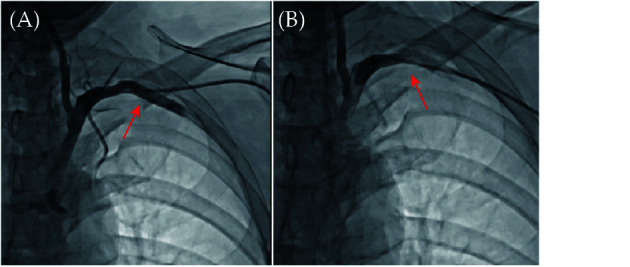
Left subclavian artery angiography.
Central venous catheter into the left subclavian artery (red arrow, A). The insertion point (red arrow) was no extravasation of contrast and the blood vessels was patent (B).
Case 2 An 82-year-old female patient underwent left internal jugular vein catheterization for dialysis access. After catheterization, the dialysis tube was suspected to enter the artery by mistake. Through the right femoral artery approach, confirmed that the 12F dialysis tube wrongly penetrated the left subclavian artery, about 10 mm away from the left vertebral artery (Figure 2A). The above examination results provide conditions for the use of covered stents to block the puncture point of the left subclavian artery, and it will not affect the blood supply of the branch vessels. Before the stent was released, the dialysis tube was partially withdrawn, leaving about 10 mm, and the preset dialysis sheath guide wire was retained. Under the positioning of the MP contrast catheter, the FLUENCY plus Vascular Stent Graft 10 mm × 40 mm covered stent (produced by Boston Company, USA) was released with the front end of the left vertebral artery as the positioning point. Then, the dialysis tube was withdrawn while the guide wire was still kept, and the contrast agent was rechecked to ensure it showed no obvious leakage. Finally, the guide wire was completely withdrawn, and the stent was found to be released satisfactorily and positioned accurately by reexamination angiography (Figure 2B).
Figure 2.
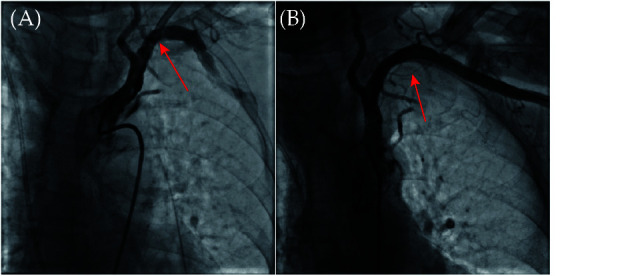
Peripheral arterial angiography.
The dialysis tube was entered the left subclavian artery mistakenly (red arrow, A). The insertion point (red arrow) was no bleeding and branch compression after stent implantation (B).
Case 3 A 60-year-old female patient underwent right subclavian vein puncture and catheterization at another medical facility. A 7F central venous catheter was considered to have mistakenly entered the artery. After a week, the patient was transferred to our hospital’s catheter room for an angiography examination. The results revealed that the puncture point of the indwelling catheter was located near the cardiac end of the right common carotid artery, about 2 cm away from the opening of the ascending aorta, and a pseudoaneurysm had formed; in addition, there were multiple plaques in the internal carotid artery (Figure 3A). A 260 cm hard hydrophilic-coated guidewire was threaded through the femoral artery angiography catheter into the right common carotid artery. The 10F SteerEase catheter was delivered to the descending aorta and then the FLUENCY plus Vascular Stent Graft 10 mm × 40 mm self-expanding covered stent (produced by Boston Company, USA) was pushed to the right common carotid artery. Ensure that both ends of the stent are covered with the insertion point of the sheath, and the proximal end of the stent is about 3 mm above the mouth of the right common carotid artery (Figure 3B). After accurate positioning, the stent was slowly released and the misplaced sheath was withdrawn. The angiography showed that there was no extravasation at the insertion point, and the pseudoaneurysm disappeared (Figure 3C).
Figure 3.

The right common carotid artery angiography.
Central venous catheter into the right common carotid artery and a pseudoaneurysm had formed (red arrow, A). Precise positioning of stent (red arrow, B). The culprit vessel (red arrow) was no extravasation and the pseudoaneurysm disappeared (C).
After a careful review of literature and our case series, we would propose an algorithm to delineate the optimal treatment strategy to guarantee optimal management of these patients (Figure 4).
Figure 4.

Proposed algorithm.
The management of inadvertent arterial lesions during central venous access procedures.
Initially the anatomical relationship of the catheter and vessel should be confirmed by Doppler ultrasonography examination or computed tomography angiography. If the location of the puncture point is within 2 mm of significant collateral vessels, we can choose open surgical treatment. Otherwise, we suggest endovascular treatment.
In cases that the arterial injury is small (made by needle smaller than 16 Gauge or catheter less than 4F), the needle or the catheter can be removed performing a direct manual compression of the external site with low risk of major complications.[1] Simply remove the catheter and apply pressure, is not applied so easily to the carotid or subclavian arteries, because it is difficult or impossible to effectively compress these vessels especially in patient with anticoagulant treatment. So the Doppler ultrasonography examination or computed tomography angiography have to be carried out to check the integrity of the injured artery looking for bleeding, hematoma, thrombosis, pseudoaneurysm, and arteriovenous fistula. If the arterial lesion still present, we suggest endovascular treatment.
In cases that the arterial injury sizing is between 4F–8F,then the arterial angiography or computed tomography angiography have to be carried out to check the situation of the injured artery for there is local lumen stenosis or not.
If the damaged artery has no lumen stenosis, the most chosen option is vascular closure device. Suggest having an experienced interventional doctor use a Suture-Mediated Closure System or Angio-Seal occluder for treatment in the catheter room, afterwards, it is necessary to confirm that there was no extravasation of contrast, and the injured artery had normal patency. If there is lumen stenosis or plaque at the puncture site, stent graft placement should be considered.
In cases that the arterial injury sizing is larger than 8F, since there are no pre-embedded two staplers (Suture-Mediated Closure System), it is recommended to perform endovascular stent graft placement. Using a single vascular occlusion device for > 8F arterial injury may cause adverse consequences (e.g., hematomas or pseudoaneurysm).
In clinical practice, establishing an infusion channel through deep vein puncture is a widely employed method, especially in the care of critically ill patients.[2] We focus on the management of the puncture needle accidentally enter the artery. According to recent research on the treatment methods for accidental insertion of central venous catheters into arteries, insertion methods can be roughly divided into four categories.
In the beginning, the sequential descending methods cause a slow rebound of blood vessels, including gradual degradation and replacement of dilated catheters,[3] or alternative replacement of guide wires.[4] However, this method still carries the potential risk of major bleeding.
Vascular closure devices can be used for treatment. This method is simple and minimally invasive. For catheters that have mistakenly entered arteries, using the Angio-Seal can safely and effectively close blood vessels, but these are all case reports. The Angio-Seal sealing device is easy to operate and is mainly used for suturing sheath puncture openings below 8F.[5] Using an Angio-Seal occluder will mean only one opportunity, as the guide wire cannot be retained after the occluder is used. Therefore, to ensure successful outcomes, the operation needs to be performed by a clinician who is experienced in using vascular occluders. A vascular suture device system (such as Perclose Proglide[6]) can suture the vascular break at the interventional puncture point through endovascular technology.[7]
The next option involves treatment with covered stents. When the catheter enters the artery at a deeper position, or the artery injury is larger than 8F, especially the local lumen has stenosis, intravascular implantation of a covered stent could be the best method to treat the damaged artery.[8] However, the location and mode of the puncture point need to be considered to preserve the important branches. Cases 2 & 3 in this report were both large-diameter dialysis tubes mistakenly inserted into the artery, and the entry site was deeper or has stenosis. In these situations, vascular occluders and sutures were unsuitable.[9]
Another option would be surgical repair. Although the trauma is significant, and it is necessary to dissect the large blood vessels surrounding the free injury area, the hemostatic effect is determined. Furthermore, most of the patients who need deep vein catheterization are elderly patients with multiple organ dysfunction syndrome, stopping antithrombotic drugs during the perioperative period will increase the risk of cardiovascular and cerebrovascular embolism.[10] Therefore, surgical treatment should be avoided as much as possible.
In summary, once a puncture accidentally enters the artery, we suggest the above mentioned algorithm to delineate the optimal treatment strategy.
ACKNOWLEDGMENTS
All authors had no conflicts of interest to disclose.
References
- 1.Dornbos DL 3rd, Nimjee SM, Smith TP Inadvertent arterial placement of central venous catheters: systematic review and guidelines for treatment. J Vasc Interv Radiol. 2019;30:1785–1794. doi: 10.1016/j.jvir.2019.05.017. [DOI] [PubMed] [Google Scholar]
- 2.Bowdle A Vascular complications of central venous catheter placement: evidence-based method for prevention and treatment. J Cardiothorac Vasc Anesth. 2014;28:358–368. doi: 10.1053/j.jvca.2013.02.027. [DOI] [PubMed] [Google Scholar]
- 3.McGee DC, Gould MK Preventing complications of central venous catheterization. N Engl J Med. 2003;348:1123–1133. doi: 10.1056/NEJMra011883. [DOI] [PubMed] [Google Scholar]
- 4.Gabriele P, Emanuele G, Ilenia DS, et al Management of inadvertent supra-aortic arterial lesions during central venous access procedures: report of six cases and proposed algorithm. Ann Vasc Surg. 2021;75:308–314. doi: 10.1016/j.avsg.2021.02.012. [DOI] [PubMed] [Google Scholar]
- 5.Ananthakrishnan G, White RD, Bhat R, et al Inadvertent subclavian artery cannulation: endovascular repair using a collagen closure device-report of two cases and review of the literature. Case Rep Vasc Med. 2012;2012:150343. doi: 10.1155/2012/150343. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Safety Committee of Japanese Society of Anesthesiologists Practical guide for safe central venous catheterizatio and management 2017. J Anesth. 2020;34:167–186. doi: 10.1007/s00540-019-02702-9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Bechara CF, Annambhotla S, Lin PH Access site management with vascular closure devices for percutaneous transarterial procedures. J Vasc Surg. 2010;52:1682–1696. doi: 10.1016/j.jvs.2010.04.079. [DOI] [PubMed] [Google Scholar]
- 8.Faraj J, Choudhary A, Ritter JC Covered stenting as bail-out technique for central venou catheter malposition within the brachiocephalic trunk. Vasc Endovascular Surg. 2020;54:65–68. doi: 10.1177/1538574419873175. [DOI] [PubMed] [Google Scholar]
- 9.Teichgräber UK, Benter T, Gebel M, et al A sonographically guided technique for central venous access. AJR Am J Roentgenol. 1997;169:731–733. doi: 10.2214/ajr.169.3.9275887. [DOI] [PubMed] [Google Scholar]
- 10.Dixon OG, Smith GE, Carradice D, et al A systematic review of management of inadvertent arterial injury during central venous catheterisation. J Vasc Access. 2017;18:97–102. doi: 10.5301/jva.5000611. [DOI] [PubMed] [Google Scholar]