

Abstract
Background
Immunotherapy functions by leveraging immunoregulation drugs to bolster the immune system’s capacity to identify and eliminate cancerous cells. In contrast to radiotherapy and chemotherapy, immunotherapy exhibits diminished side effects, heightened efficacy, and prolonged survival rates. Nevertheless, meticulous exploration into the determinants governing the advantageous effects of immunotherapy among patients who have previously undergone multiple prior therapies has yet to be conducted. Albumin (ALB) as a nutritional indicator has not been thoroughly studied for its prognostic effect on efficacy or survival. This study aims to identify factors that influence treatment outcomes among patients undergoing third-line or later immunological therapies.
Methods
A cohort of 250 lung cancer patients undergoing toripalimab or tislelizumab immunotherapy was the focal point of data collection. The determination of the median value facilitated the establishment of a cut-off point, enabling the categorization of continuous variables. After data collection, a series of statistical analyses of various clinical factors at baseline were performed, including nonparametric tests, logistic regression, and Cox proportional risk modeling. The last follow-up was in May 2022. The primary study endpoint was overall survival (OS).
Results
A total of 250 patients were enrolled in the study, of which 129 patients received first- or second-line immunotherapy and 121 patients received third-line or subsequent immunotherapy. According to Cox multifactor regression analysis, in patients receiving either first- or second-line therapy, the ALB level exhibited negligible prognostic relevance (P>0.05). However, in patients subjected to immunotherapy beyond the second line, the ALB level manifested significant prognostic importance (P=0.039). Notably, patients demonstrating elevated ALB levels achieved a higher disease control rate (DCR) (70.0% vs. 52.5%, P=0.05) and displayed a tendency towards a heightened objective response rate (ORR) (20.0% vs. 16.4%, P=0.61) in comparison to those with lower ALB levels.
Conclusions
Among patients undergoing immunotherapy in the third line or subsequent treatment phases, elevated ALB levels in baseline correlated with DCR and OS. Thus, the pre-immunotherapy ALB level emerges as an autonomous predictor of OS in patients subjected to third- or later line immunotherapy interventions.
Keywords: Third- or later line, immunotherapy, lung cancer, albumin (ALB)
Highlight box.
Key findings
• In patients treated with third- or later line immunotherapy, elevated albumin (ALB) levels were associated with better disease control rates and longer overall survival.
What is known and what is new?
• ALB is a nutritional indicator, and malnutrition is associated with poorer clinical outcomes.
• ALB is associated with better clinical outcomes in lung cancer patients who receive immunotherapy as a third- or later line treatment.
What is the implication, and what should change now?
• ALB may be a prognostic factor in lung cancer patients who receive immunotherapy above the third line. This may provide monitoring indicators for future patient treatment and assist in determining patient prognosis.
Introduction
Lung cancer persists as the leading cause of cancer-related deaths globally (1), and is the most prevalent cancer and the primary cause of tumor-related fatalities in China (2). Immunotherapy has emerged as a highly potent novel treatment modality for lung cancer.
Presently, the most developed immunotherapeutic approach involves the use of programmed cell death protein 1 (PD-1) or programmed cell death ligand 1 (PD-L1) therapy, such as tislelizumab and pembrolizumab. This marks the inaugural approval of a PD-1 monoclonal antibody for urothelial carcinoma in China and stands as the sole PD-1 antibody globally to have demonstrated benefits in both first-line combined chemotherapy and second-line monotherapy for advanced non-small cell lung cancer (NSCLC) across the entire population (3,4). Another notable agent, toripalimab, represents the premier monoclonal antibody targeting PD-1 produced within China that has gained marketing approval in China. Multiple phase 1/2 clinical trials have showcased its promising anti-tumor efficacy in NSCLC treatment, along with gastric cancer, esophageal cancer, and various other malignancies (5,6).
Research indicates that the heightened expression of PD-L1 in tumor tissue is the leading marker for projecting anti-tumor responses, although its utility is influenced by the tumor microenvironment (TME) (7,8). Moreover, molecular analysis has revealed a high response rate across most cancer types to tumor mutation burden (TMB) and microsatellite instability (MSI) status, but its practicality in clinical settings remains unverified (6,9). Research has shown the C-reactive protein to albumin ratio (CAR) to be a pivotal prognostic determinant, where a low CAR correlated with extended overall survival (OS) (10). Notably, malnutrition has been exposed as an autonomous risk factor contributing to heightened cancer mortality among the elderly (11,12). Adequately nourished elderly cancer patients have displayed enhanced tolerance to treatment side effects, whereas malnourishment has been correlated with inferior clinical outcomes (13,14). Indices such as the prognostic nutritional index (PNI) and nutritional risk index (NRI) interlink with albumin (ALB), lower ALB levels correlate with poorer patient nutritional status and worse clinical prognoses (15). And ALB data are readily available and complete.
A study has unveiled a correlation between the number of treatment lines and the efficacy of immunotherapy, establishing that earlier treatment lines yield superior treatment efficacy (16). Both the anti-PD-1 monoclonal antibody nivolumab and anti-PD-L1 atezolizumab have exhibited superior clinical outcomes compared to docetaxel, significantly prolonging patients’ OS in advanced NSCLC as second-line and subsequent chemotherapies (17,18). In the KEYNOTE-010 trial, pembrolizumab extended survival and treatment-related adverse events were less common compared to docetaxel (19). However, in real-world scenarios, a substantial proportion of lung cancer patients receive immunotherapy as third-line treatment or beyond (20). The identification of advantageous groups for immunotherapy within this patient cohort holds significant relevance. Detailed exploration into the characteristics associated with clinical benefits of immunotherapy in these patient populations remains lacking.
This study scrutinizes diverse fundamental characteristics and pathological factors among lung cancer patients undergoing immunotherapy, particularly focusing on those receiving third-line or beyond immunotherapy. Our investigation aims to delineate the factors influencing benefits among patients undergoing third-line or later immunological treatments. We present this article in accordance with the STROBE reporting checklist (available at https://tlcr.amegroups.com/article/view/10.21037/tlcr-24-378/rc).
Methods
Clinical data collection
This study comprised a multi-center retrospective analysis. Lung cancer patients receiving immunotherapy at the First Affiliated Hospital of Shandong First Medical University, Weifang People’s Hospital, and Linyi Cancer Hospital between March 2019 and August 2021 were included in the study, who were mainly treated with tislelizumab or toripalimab. We gathered patients’ medical records, tracked their progress, and subsequently analyzed the collected data. The primary objective was to investigate the factors influencing clinical outcomes among lung cancer patients undergoing different lines of immunotherapy in real-world settings.
Ethical approval
Ethical approval for this study was granted by the ethics committees of the First Affiliated Hospital of Shandong First Medical University (No. 2022 S005). Weifang People’s Hospital and Linyi Cancer Hospital were informed and agreed with this study. The study was conducted in accordance with the Declaration of Helsinki (as revised in 2013). Given the retrospective nature of the study, informed consent requirements were waived by the ethics committees of the First Affiliated Hospital of Shandong First Medical University.
Efficacy evaluation
The Response Evaluation Criteria in Solid Tumors (RECIST) 1.1 standards were employed to assess tumor efficacy. Complete response (CR) signified the disappearance of all targeted lesions and the reduction of pathological lymph nodes’ short axis to <10 mm. Partial response (PR) denoted a ≥30% reduction from the baseline sum of lengths and diameters of all target lesions. Disease progression (PD) was characterized by an at least 20% increase in the sum of lesion diameters, with an additional criterion requiring an absolute increase of at least 5 mm in the sum of lengths and diameters during the study period. Disease stability (SD) indicated lesions that did not meet the criteria for PR or PD but fell between these measures, where the minimum sum of diameters served as a reference.
The objective response rate (ORR) signified the proportion of patients whose tumor volume shrunk to a predefined value within a specified duration, typically encompassing both CR and PR. Disease control rate (DCR) was calculated as the ratio of cases exhibiting remission (PR + CR) and SD post-treatment against the total assessable cases. Given that SD also reflected effective treatment, DCR held greater scientific value than ORR as an efficacy indicator. The study’s primary endpoint, OS, served as a representation of the long-term prognosis for patients undergoing immunotherapy.
Follow-up
Routine telephone follow-up was conducted every 2–3 months based on outpatient information. The main follow-up was based on the results of recent hematology and imaging tests, and the patient’s efficacy and survival were evaluated. The initiation time commenced from the onset of the initial treatment, and the follow-up concluded in May 2022, the date of the patients’ first disease progression or death recorded.
Statistical analysis
The non-parametric test was used to analyze the correlation between various factors and treatment outcomes. Survival curves were generated using the Kaplan-Meier method. To identify independent prognostic factors, univariate and multivariate Cox proportional hazards model underwent forward logistic regression (LR) multivariate analysis.
All data were statistically analyzed using the software SPSS 25.0 (IBM Corp., Armonk, NY, USA). All analyses were 2-sided, and significance was set at P<0.05. No alterations were introduced to the statistical tests.
Results
Patients’ baseline characteristics
A cohort of 250 patients participated in the study, comprising 129 individuals undergoing first- or second-line immunotherapy and 121 individuals receiving third- or subsequent line immunotherapy. Among them, 201 patients (80.4%) were male and 49 patients (19.6%) were female. The median age for the entire cohort was 65 years (ranging between 61 and 72 years).
The majority of patients presented with stage IV lung cancer at the initial diagnosis (60.8%). Tumor distribution encompassed 40 cases of small cell lung cancer (SCLC; 16.0%), 78 cases of adenocarcinoma (31.2%), 115 cases of squamous cell carcinoma (46.0%), and 17 cases of mixed carcinoma (6.8%). In terms of treatment, 72 patients (28.8%) received monotherapy using immunotherapy, whereas 178 patients (71.2%) underwent combination therapy with immunotherapy. Summary statistics for all patients and tumor characteristics are provided in Table 1.
Table 1. Patient demographics and tumor characteristics.
| Features | Values |
|---|---|
| Age at start of immunotherapy (years), median [interquartile range] | 65 [61–72] |
| Sex, n (%) | |
| Male | 201 (80.4) |
| Female | 49 (19.6) |
| Pathological type, n (%) | |
| Adenocarcinoma | 78 (31.2) |
| Squamous carcinoma | 115 (46.0) |
| Small cell carcinoma | 40 (16.0) |
| Mixed carcinoma | 17 (6.8) |
| Tobacco, n (%) | |
| Active smoker | 169 (67.6) |
| Never smoker | 81 (32.4) |
| Alcohol, n (%) | |
| Active | 71 (28.4) |
| Never | 179 (71.6) |
| Neoplasm staging, n (%) | |
| ≤ III* | 98 (39.2) |
| > III | 152 (60.8) |
| Therapy lines, n (%) | |
| ≤2 | 129 (51.6) |
| >2 | 121 (48.4) |
*, the TNM staging was based on the AJCC 8th edition (when the initial diagnosis). AJCC, American Joint Committee on Cancer.
Differences in the distribution of clinicopathological features
We examined the clinicopathological characteristics of patients undergoing different lines of immunotherapy (first- or second-line vs. third- or later line immunotherapy), encompassing factors such as sex, age, tumor stage, pathological type, and pre-immunotherapy peripheral blood indices.
The proportion of patients aged over 65 years who underwent first- or second-line treatment exceeded those receiving third- or subsequent line treatment (58.5% vs. 41.5%, P=0.03). Notably, individuals at later cancer stages (IV) were significantly more prevalent among those undergoing third- or later line immunotherapy compared to those on first- or second-line treatment (57.9% vs. 42.1%, P<0.001). Patients without a history of alcohol consumption were more inclined towards early treatment as opposed to later treatment (60.9% vs. 39.1%, P<0.001). However, no substantial differences emerged in age, pathological type, or smoking history concerning the distribution across treatment lines. Detailed information is presented in Table 2.
Table 2. Distribution of clinicopathological features.
| Features | First- or second-line immunotherapy, n (%) | Third- or later line immunotherapy, n (%) | P value |
|---|---|---|---|
| Age (years) | 0.03 | ||
| ≤65 | 57 (44.2) | 70 (57.9) | |
| >65 | 72 (55.8) | 51 (42.1) | |
| Sex | 0.47 | ||
| Female | 23 (17.8) | 26 (21.5) | |
| Male | 106 (82.2) | 95 (78.5) | |
| Neoplasm staging | <0.001 | ||
| ≤ III* | 65 (50.4) | 33 (27.3) | |
| > III | 64 (49.6) | 88 (72.7) | |
| Pathological type | 0.64 | ||
| SCLC | 22 (17.1) | 18 (14.9) | |
| NSCLC | 107 (82.9) | 103 (85.1) | |
| Smoking history | 0.31 | ||
| Yes | 91 (70.5) | 78 (64.5) | |
| No | 38 (29.5) | 43 (35.5) | |
| Alcohol history | <0.001 | ||
| Yes | 20 (15.5) | 51 (42.1) | |
| No | 109 (84.5) | 70 (57.9) |
*, the TNM staging was based on the AJCC 8th edition (when the initial diagnosis). SCLC, small cell lung cancer; NSCLC, non-small cell lung cancer; AJCC, American Joint Committee on Cancer.
Peripheral hematological indices displayed no significant differences in distribution across distinct treatment lines. Key indicators are displayed in Figure 1.
Figure 1.
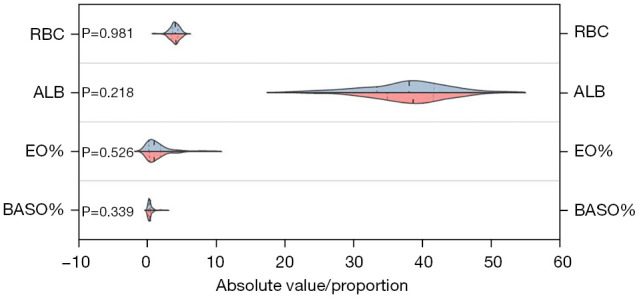
Distribution differences in various treatment lines concerning red blood cells, ALB, EO%, and BASO% between the 2 groups. Blue represents patients undergoing first- or second-line immunotherapy; red signifies patients on third- or subsequent line immunotherapy. These hematologic indicators did not display significant distribution differences across various treatment lines. RBC, red blood cells; ALB, albumin; EO%, percentage of acidophilic cell; BASO%, percentage of basophil cell.
Survival analyses in patients based on treatment lines
We conducted an analysis across all patients to determine factors influencing the prognosis of those receiving immunotherapy. The univariate proportional hazards model revealed that patients in the first- or second-line treatment group exhibited longer OS compared to those in the third- or subsequent line treatment group [hazard ratio (HR) =1.509, 95% confidence interval (CI): 1.021–2.229, P=0.04]. Additionally, patients younger than 65 years had a longer OS in contrast to those aged over 65 years (HR =1.672, 95% CI: 1.138–2.455, P=0.009), whereas male patients demonstrated longer OS than their female counterparts (HR =0.598, 95% CI: 0.385–0.928, P=0.02). Although patients at earlier cancer stages displayed a trend towards better prognosis compared to those at later stages (HR =1.253, 95% CI: 0.827–1.899, P=0.29), the pathological tumor classification, smoking, and alcohol history did not exhibit significance. Notably, certain peripheral blood indicators, such as red blood cell (RBC) count (HR =0.726, 95% CI: 0.550–0.958, P=0.02) and ALB (HR =0.964, 95% CI: 0.935–0.995, P=0.02), displayed substantial significance when analyzed as continuous variables. However, other hematologic indicators did not demonstrate statistical significance.
Further analyses were conducted within the first- or second-line and third- or subsequent line populations to ascertain predictors linked to treatment line numbers. This exploration aimed to identify the predominant population that reaped benefits from immunotherapy during third- or subsequent line treatment.
In patients receiving first- or second-line immunotherapy, the univariate proportional hazards model indicated that male patients exhibited longer OS compared to female patients (HR =0.410, 95% CI: 0.212–0.792, P=0.008). There was a tendency for individuals under 65 years of age to display longer OS compared to those aged over 65 years (HR =1.823, 95% CI: 0.973–3.419, P=0.06). Additionally, patients diagnosed with stages I, II, or III cancer trended towards better prognoses compared to stage IV patients (HR =1.739, 95% CI: 0.927–3.261, P=0.09). However, the pathological tumor classification, tobacco, and alcohol use history did not show significance. Notably, the RBC count (HR =0.593, 95% CI: 0.361–0.976, P=0.04) exhibited significant importance when analyzed as a continuous variable, whereas other hematologic indicators did not demonstrate statistical significance. Subsequent multivariate proportional hazards analysis identified male sex (P=0.008) as an independent prognostic factor among patients receiving first- or second-line immunotherapy.
Among patients undergoing third- or later line immunotherapy, the univariate proportional hazards model revealed that individuals younger than 65 years old exhibited improved OS compared to those older than 65 years (HR =1.992, 95% CI: 1.204–3.297, P=0.007). However, sex, tumor pathology, smoking history, and alcohol use history did not show statistical significance. Notably, ALB (HR =0.950, 95% CI: 0.912–0.990, P=0.01) emerged as statistically significant when analyzed as a continuous variable, whereas other hematological indices lacked statistical significance. The subsequent multivariate proportional hazards analysis identified age below 65 years (HR =1.821, 95% CI: 1.096–3.023, P=0.02) and ALB (HR =0.957, 95% CI: 0.918–0.998, P=0.04) as independent prognostic factors. Detailed information is presented in Tables 3-5. Based on the above findings, ALB showed independent prognostic significance for long-term prognosis in patients with third- or later line immunotherapy, but not in patients with first- or second-line immunotherapy. Next, we focused on the role of ALB in patients receiving third- or later line treatment.
Table 3. Univariable analyses of overall survival in all patients (n=250).
| Features | HR (95% CI) | P value |
|---|---|---|
| Age (>65 vs. ≤65 years) | 1.672 (1.138–2.455) | 0.009 |
| Sex (male vs. female) | 0.598 (0.385–0.928) | 0.02 |
| Treatment lines (3 or above vs. 1 or 2) | 1.509 (1.021–2.229) | 0.04 |
| Pathological staging (IV vs. I or II or III) | 1.253 (0.827–1.899) | 0.29 |
| Pathological type (SCLC vs. NSCLC) | 1.018 (0.612–1.694) | 0.95 |
| Tobacco use history (yes vs. no) | 0.931 (0.623–1.391) | 0.73 |
| Alcohol use history (yes vs. no) | 0.932 (0.618–1.407) | 0.74 |
| RBC | 0.726 (0.550–0.958) | 0.02 |
| ALB | 0.964 (0.935–0.995) | 0.02 |
| BASO% | 0.466 (0.201–1.082) | 0.08 |
| EO% | 0.948 (0.834–1.077) | 0.41 |
HR, hazard ratio; CI, confidence interval; SCLC, small cell lung cancer; NSCLC, non-small cell lung cancer; RBC, red blood cell; ALB, albumin; BASO%, percentage of basophil cell; EO%, percentage of acidophilic cell.
Table 4. Univariable and multivariable analyses of overall survival in patients with first- or second-line immunotherapy (n=129).
| Features | Univariable model | Multivariable model | |||
|---|---|---|---|---|---|
| HR (95% CI) | P value | HR (95% CI) | P value | ||
| Age (>65 vs. ≤65 years) | 1.823 (0.973–3.419) | 0.06 | |||
| Sex (male vs. female) | 0.410 (0.212–0.792) | 0.008 | 0.410 (0.212–0.792) | 0.008 | |
| Pathological staging (IV vs. I or II or III) | 1.739 (0.927–3.261) | 0.09 | |||
| Pathological type (SCLC vs. NSCLC) | 0.944 (0.435–2.049) | 0.88 | |||
| Tobacco use history (yes vs. no) | 0.900 (0.484–1.675) | 0.74 | |||
| Alcohol use history (yes vs. no) | 0.548 (0.238–1.262) | 0.16 | |||
| RBC | 0.539 (0.361–0.976) | 0.04 | |||
| ALB | 0.978 (0.928–1.030) | 0.40 | |||
| BASO% | 0.870 (0.472–1.604) | 0.66 | |||
| EO% | 0.900 (0.744–1.089) | 0.28 | |||
HR, hazard ratio; CI, confidence interval; SCLC, small cell lung cancer; NSCLC, non-small cell lung cancer; RBC, red blood cell; ALB, albumin; BASO%, percentage of basophil cell; EO%, percentage of acidophilic cell.
Table 5. Univariable and multivariable analyses of overall survival in patients with third- or later line immunotherapy (n=121).
| Features | Univariable models | Multivariable model | |||
|---|---|---|---|---|---|
| HR (95% CI) | P value | HR (95% CI) | P value | ||
| Age (>65 vs. ≤65 years) | 1.992 (1.204–3.297) | 0.007 | 1.821 (1.096–3.023) | 0.02 | |
| Sex (male vs. female) | 0.807 (0.444–1.466) | 0.48 | |||
| Pathological staging (IV vs. I or II or III) | 0.788 (0.451–1.376) | 0.40 | |||
| Pathological type (SCLC vs. NSCLC) | 1.118 (0.565–2.210) | 0.75 | |||
| Tobacco use history (yes vs. no) | 1.008 (0.592–1.716) | 0.98 | |||
| Alcohol use history (yes vs. no) | 0.911 (0.551–1.506) | 0.72 | |||
| RBC | 0.800 (0.571–1.119) | 0.20 | |||
| ALB | 0.950 (0.912–0.990) | 0.01 | 0.957 (0.918–0.998) | 0.04 | |
| BASO% | 1.414 (0.628–3.185) | 0.40 | |||
| EO% | 1.062 (0.918–1.229) | 0.42 | |||
SCLC, small cell lung cancer; NSCLC, non-small cell lung cancer; RBC, red blood cell; ALB, albumin; BASO%, percentage of basophil cell; EO%, eosinophils percentage; HR, hazard ratio; CI, confidence interval.
To further evaluate the prognostic significance of ALB, we categorized patients into 2 groups based on the ALB cutoff value, determined as 38.5 g/L through X-tile analysis. Additionally, other hematological indicators were assessed as continuous variables. Our analysis revealed substantial differences in OS between the 2 ALB groups, as depicted in Figure 2. Patients in the high-ALB group exhibited extended OS (11.0 vs. 9.0 months, HR =0.485, 95% CI: 0.291–0.807, P=0.005) and a tendency towards prolonged progression-free survival (PFS) (5.0 vs. 4.0 months, HR =0.866, 95% CI: 0.561–1.338, P=0.52) post-immunotherapy compared to those in the low-ALB group. The multivariate proportional hazards model identified elevated ALB levels (HR =0.543, 95% CI: 0.325–0.908, P=0.02) and older age (>65 vs. ≤65 years) (HR =1.776, 95% CI: 1.067–2.957, P=0.03) as independent prognostic factors among patients undergoing third- or subsequent line immunotherapy. This indicates that patients with higher ALB levels constitute the primary beneficiary population in terms of survival from third- or later line immunotherapy. Notably, patients’ sex and some other blood indicators did not exhibit significant associations with clinical prognosis. Detailed information is presented in Figure 3.
Figure 2.
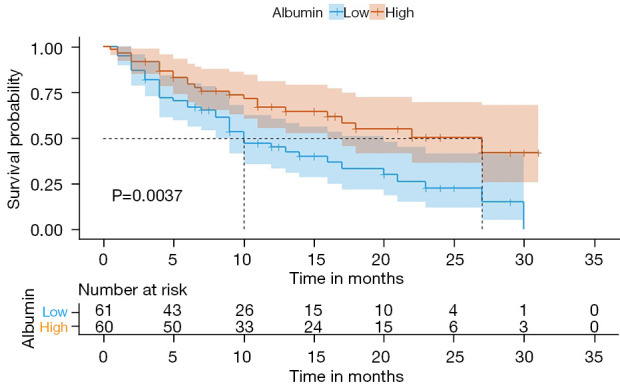
Survival curves for overall survival in both groups. As depicted, patients with elevated ALB levels exhibited better survival, contrasting with patients with lower ALB levels who demonstrated poorer survival. ALB, albumin.
Figure 3.

Among patients undergoing third- or subsequent line immunotherapy, subgroup multivariate Cox regression analysis indicated that ALB and age stood as independent prognostic factors. SCLC, small cell lung cancer; NSCLC, non-small cell lung cancer; RBC, red blood cell; ALB, albumin; BASO%, percentage of basophil cell; EO%, percentage of acidophilic cell; HR, hazard ratio; CI, confidence interval; OS, overall survival.
Pathological features
In examining the factors influencing ALB levels among patients receiving third- or subsequent line immunotherapy, we analyzed parameters such as patient’s sex, age, tumor staging, pathological type, and previous treatments received.
Individuals with an active alcohol use history (62.5% vs. 41.1%, P=0.02) and those lacking a history of radiation treatment (54.8% vs. 32.1%, P=0.04) exhibited higher ALB levels. Furthermore, patients at stage IV (54.5% vs. 36.4%, P=0.08) and those without a history of antiangiogenic drug application (56.9% vs. 38.8%, P=0.05) tended to demonstrate elevated ALB levels. However, there were no significant differences in ALB levels concerning age (P=0.31), sex (P=0.40), pathological type (P=0.15), and smoking history (P=0.38).
Efficacy evaluation
In our efficacy evaluation, data was gathered from 121 patients who underwent immunotherapy beyond the second line, revealing an ORR of 18.2% and a DCR of 61.2%.
Upon assessing patients who had undergone multiple cycles of third- or subsequent line immunotherapy, those in the high ALB group exhibited superior DCR (70.0% vs. 52.5%, P=0.05) and displayed a trend towards higher ORR (20.0% vs. 16.4%, P=0.61) compared to individuals in the low ALB group. Patients with elevated ALB levels demonstrated higher DCR and a tendency towards increased ORR, although the latter was not statistically significant. Therefore, higher ALB levels appeared to correlate with enhanced treatment response among patients undergoing third- or subsequent line immunotherapy. Detailed data is provided in Table 6.
Table 6. Cross-table analysis of efficacy in patients with third- or later line immunotherapy (n=121).
| Parameters | Low ALB, n (%) | High ALB, n (%) | OR (95% CI) | P value |
|---|---|---|---|---|
| ORR | 0.61 | |||
| PD + SD | 51 (83.6) | 48 (80.0) | 1.045 (0.883–1.237) | |
| PR + CR | 10 (16.4) | 12 (20.0) | 0.820 (0.383–1.752) | |
| DCR | 0.05 | |||
| PD | 29 (47.5) | 18 (30.0) | 1.585 (0.993–2.530) | |
| SD + PR + CR | 32 (52.5) | 42 (70.0) | 0.749 (0.560–1.002) |
ALB, albumin; OR, odds ratio; CI, confidence interval; ORR, objective response rate; PD, progressive disease; SD, stable disease; PR, partial response; CR, complete response; DCR, disease control rate.
Discussion
We conducted an analysis of the fundamental characteristics and clinical factors among lung cancer patients undergoing immunotherapy. The findings, derived from real-world multicenter data involving the application of China-made immune drugs, highlighted a significant association between higher baseline ALB levels and extended OS during immunological treatment. Notably, ALB emerged as an independent predictor for prognosis in patients undergoing third- or subsequent line immunotherapy.
Immunotherapy offers several notable advantages. Firstly, it allows treatment irrespective of cancer type or stage. Secondly, it exhibits promising dual effects in reducing cancer and prolonging long-term survival. Thirdly, it can be combined with surgical, chemotherapy, and radiotherapy approaches. An international real-world retrospective analysis documented an OS of 4.7 months and a response rate of 18% when assessing patients with SCLC using third-line chemotherapy (21). Furthermore, an observed ORR of 11.9% (95% CI: 6.5–19.5%) was confirmed in recurrent SCLC patients treated with third- or later line immunotherapy (22).
Various peripheral blood indicators have been extensively utilized to assess treatment efficacy and clinical prognosis. TMB stands out as an autonomous biomarker for gauging immune checkpoint inhibitor response across multiple cancer types, encompassing bladder cancer, melanoma, SCLC, and NSCLC (23). A specific study demonstrated that the ORR was 21.3% for patients exhibiting high TMB (≥248 mutations via total exome sequencing), compared to 4.8% for those with low TMB (<143 mutations via total exome sequencing) (24). Additionally, other metrics derived from routine blood tests, such as the platelet to lymphocyte ratio (PLR) and lymphocyte to monocyte ratio (LMR), have demonstrated prognostic implications in various cancers (25,26).
Global research indicates that systemic inflammation and nutritional status serve as pivotal prognostic factors for cancer patients (27). In certain studies, the CAR, indicating both inflammatory and nutritional status, has shown potential prognostic value in lung cancer (10,28). A study has developed an immune checkpoint inhibitor (ICI) specific nutrient index (NI) for metastatic gastrooesophageal junction (mGOJ)/gastric cancer (GC) patients receiving second-line ICI (29). Furthermore, a variety of ALB-related clinical indicators have been shown to be significantly related to tumor prognosis. For example, a low pretreatment albumin to globulin ratio (AGR) has been significantly associated with diminished OS (27). ALB concentration combined with neutrophil-to-lymphocyte ratio (NLR) (COA-NLR) can be used as an effective biomarker for prognosis of patients with NSCLC who have undergone excision therapy (30). The albumin-to-alkaline phosphatase ratio (AAPR) is an innovative prognostic indicator for patients with various cancers, the level of AAPR in patients with gastric cancer is significantly decreased, which affects the prognosis of patients (31). Nonetheless, the detailed prognostic significance of ALB in immunotherapy remains inadequately explored.
ALB stands as the primary protein in human plasma, pivotal for maintaining bodily nutrition and osmotic pressure. Irrespective of the presence of malnutrition, serum ALB levels were notably reduced in patients with locally advanced or metastatic malignant tumors. Notably, nutritional status significantly impacts the tolerance to treatment side effects, particularly in older patients (13). Diminished serum ALB levels correspond to poorer nutritional status, directly impacting the efficacy of anti-tumor therapy. In our study, a heightened pre-treatment ALB level emerged as a straightforward and substantial prognostic indicator for lung cancer patients undergoing second-line or subsequent immunotherapy, correlating with extended survival. These insights help to guide nutritional support therapy for patients, thereby enhancing their nutritional status before commencing immunotherapy.
This study does, however, possess limitations. Primarily, the sample size constraints might introduce statistical biases, potentially losing representative samples and somewhat restricting the statistical robustness of this study. Secondly, being a multicenter study involving patients across various clinical stages receiving immunotherapy during the specified period, disparities in treatment approaches might have influenced patient outcomes. Thirdly, owing to the retrospective nature of our study, incomplete peripheral blood indicator data for all patients may have resulted in the absence of certain prognostic markers. Lastly, divergent studies adopted distinct ALB cut-off values, indicating a potential factor influencing the outcomes.
Nevertheless, these findings should be approached cautiously in clinical practice, considering the aforementioned limitations. Hence, for further validation of our conclusions, future research should be conducted prospectively, and involve larger sample sizes and more comprehensive clinical data.
Conclusions
ALB has been demonstrated as an independent predictor of OS in patients undergoing third-line and subsequent immunotherapy. Elevated baseline ALB levels correlate with improved treatment response among patients.
Supplementary
The article’s supplementary files as
Acknowledgments
Funding: None.
Ethical Statement: The authors are accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved. The study was conducted in accordance with the Declaration of Helsinki (as revised in 2013). The study was approved by the ethics committees of the First Affiliated Hospital of Shandong First Medical University (No. 2022 S005) and informed consent requirements were waived. Weifang People’s Hospital and Linyi Cancer Hospital were informed and agreed with this study.
Footnotes
Reporting Checklist: The authors have completed the STROBE reporting checklist. Available at https://tlcr.amegroups.com/article/view/10.21037/tlcr-24-378/rc
Data Sharing Statement: Available at https://tlcr.amegroups.com/article/view/10.21037/tlcr-24-378/dss
Peer Review File: Available at https://tlcr.amegroups.com/article/view/10.21037/tlcr-24-378/prf
Conflicts of Interest: All authors have completed the ICMJE uniform disclosure form (available at https://tlcr.amegroups.com/article/view/10.21037/tlcr-24-378/coif). A.R. serves as an unpaid editorial board member of Translational Lung Cancer Research from November 2022 to October 2024. He also reports stock options offered by IQVIA Holdings Inc. The other authors have no conflicts of interest to declare.
References
- 1.Steven A, Fisher SA, Robinson BW. Immunotherapy for lung cancer. Respirology 2016;21:821-33. 10.1111/resp.12789 [DOI] [PubMed] [Google Scholar]
- 2.Chen W, Zheng R, Baade PD, et al. Cancer statistics in China, 2015. CA Cancer J Clin 2016;66:115-32. 10.3322/caac.21338 [DOI] [PubMed] [Google Scholar]
- 3.Lee A, Keam SJ. Tislelizumab: First Approval. Drugs 2020;80:617-24. 10.1007/s40265-020-01286-z [DOI] [PubMed] [Google Scholar]
- 4.Liu SY, Wu YL. Tislelizumab: an investigational anti-PD-1 antibody for the treatment of advanced non-small cell lung cancer (NSCLC). Expert Opin Investig Drugs 2020;29:1355-64. 10.1080/13543784.2020.1833857 [DOI] [PubMed] [Google Scholar]
- 5.Tang B, Yan X, Sheng X, et al. Safety and clinical activity with an anti-PD-1 antibody JS001 in advanced melanoma or urologic cancer patients. J Hematol Oncol 2019;12:7. 10.1186/s13045-018-0693-2 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Wang F, Wei XL, Wang FH, et al. Safety, efficacy and tumor mutational burden as a biomarker of overall survival benefit in chemo-refractory gastric cancer treated with toripalimab, a PD-1 antibody in phase Ib/II clinical trial NCT02915432. Ann Oncol 2019;30:1479-86. 10.1093/annonc/mdz197 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Herbst RS, Soria JC, Kowanetz M, et al. Predictive correlates of response to the anti-PD-L1 antibody MPDL3280A in cancer patients. Nature 2014;515:563-7. 10.1038/nature14011 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Taube JM, Klein A, Brahmer JR, et al. Association of PD-1, PD-1 ligands, and other features of the tumor immune microenvironment with response to anti-PD-1 therapy. Clin Cancer Res 2014;20:5064-74. 10.1158/1078-0432.CCR-13-3271 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Perrier A, Didelot A, Laurent-Puig P, et al. Epigenetic Mechanisms of Resistance to Immune Checkpoint Inhibitors. Biomolecules 2020;10:1061. 10.3390/biom10071061 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Miyazaki T, Yamasaki N, Tsuchiya T, et al. Ratio of C-reactive protein to albumin is a prognostic factor for operable non-small-cell lung cancer in elderly patients. Surg Today 2017;47:836-43. 10.1007/s00595-016-1448-8 [DOI] [PubMed] [Google Scholar]
- 11.Shakersain B, Santoni G, Faxén-Irving G, et al. Nutritional status and survival among old adults: an 11-year population-based longitudinal study. Eur J Clin Nutr 2016;70:320-5. 10.1038/ejcn.2015.109 [DOI] [PubMed] [Google Scholar]
- 12.Zhang X, Pang L, Sharma SV, et al. Malnutrition and overall survival in older patients with cancer. Clin Nutr 2021;40:966-77. 10.1016/j.clnu.2020.06.026 [DOI] [PubMed] [Google Scholar]
- 13.Zhang X, Edwards BJ. Malnutrition in Older Adults with Cancer. Curr Oncol Rep 2019;21:80. 10.1007/s11912-019-0829-8 [DOI] [PubMed] [Google Scholar]
- 14.Bullock AF, Greenley SL, McKenzie GAG, et al. Relationship between markers of malnutrition and clinical outcomes in older adults with cancer: systematic review, narrative synthesis and meta-analysis. Eur J Clin Nutr 2020;74:1519-35. 10.1038/s41430-020-0629-0 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Farag CM, Antar R, Akosman S, et al. What is hemoglobin, albumin, lymphocyte, platelet (HALP) score? A comprehensive literature review of HALP's prognostic ability in different cancer types. Oncotarget 2023;14:153-72. 10.18632/oncotarget.28367 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Zhou J, Chao Y, Yao D, et al. Impact of chronic obstructive pulmonary disease on immune checkpoint inhibitor efficacy in advanced lung cancer and the potential prognostic factors. Transl Lung Cancer Res 2021;10:2148-62. 10.21037/tlcr-21-214 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Fehrenbacher L, von Pawel J, Park K, et al. Updated Efficacy Analysis Including Secondary Population Results for OAK: A Randomized Phase III Study of Atezolizumab versus Docetaxel in Patients with Previously Treated Advanced Non-Small Cell Lung Cancer. J Thorac Oncol 2018;13:1156-70. 10.1016/j.jtho.2018.04.039 [DOI] [PubMed] [Google Scholar]
- 18.Horn L, Spigel DR, Vokes EE, et al. Nivolumab Versus Docetaxel in Previously Treated Patients With Advanced Non-Small-Cell Lung Cancer: Two-Year Outcomes From Two Randomized, Open-Label, Phase III Trials (CheckMate 017 and CheckMate 057). J Clin Oncol 2017;35:3924-33. 10.1200/JCO.2017.74.3062 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Herbst RS, Baas P, Kim DW, et al. Pembrolizumab versus docetaxel for previously treated, PD-L1-positive, advanced non-small-cell lung cancer (KEYNOTE-010): a randomised controlled trial. Lancet 2016;387:1540-50. 10.1016/S0140-6736(15)01281-7 [DOI] [PubMed] [Google Scholar]
- 20.Lahiri A, Maji A, Potdar PD, et al. Lung cancer immunotherapy: progress, pitfalls, and promises. Mol Cancer 2023;22:40. 10.1186/s12943-023-01740-y [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Simos D, Sajjady G, Sergi M, et al. Third-line chemotherapy in small-cell lung cancer: an international analysis. Clin Lung Cancer 2014;15:110-8. 10.1016/j.cllc.2013.11.003 [DOI] [PubMed] [Google Scholar]
- 22.Ready N, Farago AF, de Braud F, et al. Third-Line Nivolumab Monotherapy in Recurrent SCLC: CheckMate 032. J Thorac Oncol 2019;14:237-44. 10.1016/j.jtho.2018.10.003 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.Goodman AM, Kato S, Bazhenova L, et al. Tumor Mutational Burden as an Independent Predictor of Response to Immunotherapy in Diverse Cancers. Mol Cancer Ther 2017;16:2598-608. 10.1158/1535-7163.MCT-17-0386 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.Hellmann MD, Callahan MK, Awad MM, et al. Tumor Mutational Burden and Efficacy of Nivolumab Monotherapy and in Combination with Ipilimumab in Small-Cell Lung Cancer. Cancer Cell 2018;33:853-861.e4. 10.1016/j.ccell.2018.04.001 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.Zhang H, Xia H, Zhang L, et al. Clinical significance of preoperative neutrophil-lymphocyte vs platelet-lymphocyte ratio in primary operable patients with non-small cell lung cancer. Am J Surg 2015;210:526-35. 10.1016/j.amjsurg.2015.03.022 [DOI] [PubMed] [Google Scholar]
- 26.Li W, Ma G, Wu Q, et al. Prognostic value of lymphocyte-to-monocyte ratio among Asian lung cancer patients: a systematic review and meta-analysis. Oncotarget 2017;8:110606-13. 10.18632/oncotarget.20574 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27.Li J, Wang Y, Wu Y, et al. Prognostic Value of Pretreatment Albumin to Globulin Ratio in Lung Cancer: A Meta-Analysis. Nutr Cancer 2021;73:75-82. 10.1080/01635581.2020.1737155 [DOI] [PubMed] [Google Scholar]
- 28.Zhou T, Zhan J, Hong S, et al. Ratio of C-Reactive Protein/Albumin is An Inflammatory Prognostic Score for Predicting Overall Survival of Patients with Small-cell Lung Cancer. Sci Rep 2015;5:10481. 10.1038/srep10481 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29.Morelli C, Formica V, Patrikidou A, et al. Nutritional index for immune-checkpoint inhibitor in patients with metastatic gastro-esophageal junction/gastric cancer. J Gastrointest Oncol 2022;13:2072-81. 10.21037/jgo-22-217 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 30.Weng J, Huang J, Yu W, et al. Combination of albumin concentration and neutrophil-to-lymphocyte ratio for predicting overall survival of patients with non-small cell lung cancer. J Thorac Dis 2021;13:5508-16. 10.21037/jtd-21-1320 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 31.Wang Y, Xiong F, Yang J, et al. Decreased albumin-to-alkaline phosphatase ratio predicted poor survival of resectable gastric cancer patients. J Gastrointest Oncol 2021;12:1338-50. 10.21037/jgo-21-430 [DOI] [PMC free article] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
The article’s supplementary files as