

Abstract
Background
The safety and technical success of endoscopic ultrasound-guided antegrade treatment (EUS-AG) compared to balloon enteroscopy-assisted endoscopic cholangiopancreatography (BE-ERCP) for choledocholithiasis in Roux-en-Y gastrectomy has not been well documented. We performed a systematic review and meta-analysis to assess the safety and efficacy of the 2 procedures.
Methods
A systematic search of multiple databases was undertaken through January 25, 2024, to identify relevant studies comparing the 2 procedures. Standard meta-analysis methods were employed using a random-effects model. For each outcome, risk-ratio (RR), 95% confidence interval (CI), and P-values were generated. P<0.05 was considered significant. Heterogeneity was assessed using the I2 statistic.
Results
Three studies with 795 patients (95 in the EUS-AG group and 700 in the BE-ERCP group) were included. The technical success rate was similar between EUS-AG and BE-ERCP (RR 1.08, 95%CI 0.84-1.38; P=0.57; I2=56%). The overall rate of adverse effects was higher in the BE-ERCP group than in the EUS-AG group (RR 1.95, 95%CI 1.21-3.15; P=0.006; I2=0 %). Rates of clinical success, pancreatitis, perforation, and bile peritonitis were similar between the 2 procedure techniques.
Conclusions
Our analysis showed no distinct advantage in using one technique over the other for patients with Roux-en-Y anatomy in achieving technical and clinical success. However, the incidence of adverse effects was greater in the BE-ERCP group than in the EUS-AG group.
Keywords: Roux-en-Y gastric bypass, endoscopic ultrasound, balloon enteroscopy
Introduction
Endoscopic retrograde cholangiopancreatography (ERCP) has evolved greatly over recent years, from a diagnostic and therapeutic procedure for hepatobiliary diseases such as choledocholithiasis to management of pancreatic duct stones, benign and malignant structures, and bile and pancreatic leaks [1]. Although considered safe, ERCP poses a significant risk of post-ERCP pancreatitis (PEP) which occurs in 3-15% of ERCP cases, increasing up to 25% in high-risk cases, even in experienced hands [2]. Additional complications and difficulties can arise in patients with surgically altered anatomy depending on the postoperative anatomy. Some of the difficulties include traversing the anastomosis to reach the pancreaticobiliary tract and cannulation of the papilla [3].
Patients with Roux-en-Y gastric bypass (RYGB) require an alternative approach to ERCP, as traditional ERCP endoscopes are not long enough to reach the papilla in these patients [4]. Different approaches for ERCP can be employed in patients with Roux-en-Y anatomy, including laparoscopic-assisted ERCP (LA-ERCP), endoscopic ultrasound (EUS)-directed transgastric ERCP (EDGE), balloon enteroscopy-assisted ERCP (BE-ERCP), and EUS-guided antegrade (EUS-AG) treatment for biliary disease [5]. BE-ERCP is performed using a single or double balloon enteroscope transorally, through the Roux limb and the jejunostomy up to the pancreaticobiliary limb to identify the papilla [6]. EUS-AG treatment involves left intrahepatic bile duct puncture under EUS guidance, guidewire advancement into the bile duct, guidewire manipulation through the papilla or the anastomosis, tract dilation, and then performing EUS-guided transhepatic AG stone removal and/or AG balloon dilation for anastomotic strictures [7].
Studies have reported similar technical success rates and adverse effects when EDGE is compared to LA-ERCP for RYGB [8].
Recent studies have evaluated the efficacy and safety of EUS-AG vs. BE-ERCP in treating biliary diseases in patients with RYGB. Given the limited sample sizes in individual studies, we conducted a systematic review and meta-analysis of the existing literature to provide a conclusive assessment of this topic.
Materials and methods
This study adhered to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines and no language restriction was applied [9].
Search strategy
A detailed and comprehensive search of the following databases was conducted from inception through January 25, 2024: MEDLINE (PubMed, National Center for Biotechnology Information), Embase(Embase.com, Elsevier), Web of Science Core Collection, Korean Journal Index, and SciELO Citation Index (Web of Science Platform, Clarivate), Cochrane Central Register of Controlled Trials (Cochrane Library, Wiley), and Global Index Medicus (World Health Organization). An additional manual hand search was also performed. The keywords and subject terms for the concepts of “Roux-en-Y gastric bypass”, “balloon enteroscopy”, “endoscopic retrograde cholangiopancreatography”, “endoscopic ultrasonography” and “interventional ultrasonography” were developed for Embase and translated to the vocabulary of other databases.
The search strategy was created by an experienced librarian (WL-S) and reviewed by another investigator (AI). The detailed search strategy for Embase is provided in Supplementary Table 1 (122KB, pdf) . All results were exported to EndNote 20 citation management software (Clarivate, Philadelphia, Penn., USA) and duplicates were removed by successive iterations of EndNote’s duplicate detection algorithms and manual inspection. Screening of the articles was performed by 2 independent reviewers (AI and ZA) and any discrepancy was resolved through mutual discussion. Bibliographies of the articles included were also checked to see if any additional articles fulfilled our study criteria.
Inclusion and exclusion criteria
We included studies based on the following criteria: 1) randomized controlled trials (RCTs), prospective or retrospective cohort studies, and cross-sectional studies comparing EUS-AG and BE-ERCP directly; and 2) studies that documented outcomes relevant to our research and included all studies with comparative arms. We excluded case reports, review articles and conference abstracts.
Data collection and outcomes
Two independent reviewers performed the data collection (AI and ZA), and any discrepancy was discussed and resolved. The primary outcomes of our analysis were the rates of technical success and overall adverse effects of EUS-AG and BE-ERCP. Secondary outcomes included clinical success rates, and rates of pancreatitis, perforation and bile peritonitis. Data were collected and tabulated in Microsoft Excel (Microsoft, Redmond, Wash, USA) by 2 independent reviewers (AI and ZA). Any discrepancy in data collection was resolved through mutual discussion.
Study definitions
Technical success of the procedure was defined as achieving successful biliary access and intervention, including the successful placement of biliary drainage and/or performance of stone removal procedures. Clinical success of the procedure was defined as clearance of all stones, confirmed by cholangiogram, intraductal US, or direct visualization by cholangioscopy, either on its own or with adjunctive techniques, such as repeating the procedure, percutaneous transhepatic biliary drainage or surgery.
Statistical analysis
We performed a meta-analysis of the included studies using Review Manager 5.3 (Cochrane Collaboration, Copenhagen, The Nordic Cochrane Centre). The random-effects model was used to calculate the weighted pooled risk ratio (RR) and mean difference (MD), with the corresponding 95% confidence intervals (CI) of our desired outcome. A P-value <0.05 was considered statistically significant. The heterogeneity of the effect size estimates across the studies was quantified using the Q statistic and I2 (P<0.10 was considered significant). A value of I2<50% was chosen to indicate low heterogeneity, and ≥50% for substantial heterogeneity [10].
Bias assessment
The bias assessment for included studies was evaluated using Newcastle–-Ottawa scale for observational studies and the Cochrane Risk of Bias Tool for RCTs [11]. Publication bias was assessed visually, using funnel plots, as well as quantitatively, using Egger’s regression analysis. A P-value <0.05 was indicative of substantial publication bias.
Results
Systematic review
Using the search strategy above, 33 studies were screened, duplicates were removed, and 3 were included (Fig. 1) [12-14]. All included studies were observational. A total of 795 patients were included, which also corresponded to the total number of procedures performed, including EUS-AG and BE-ERCP.
Figure 1.
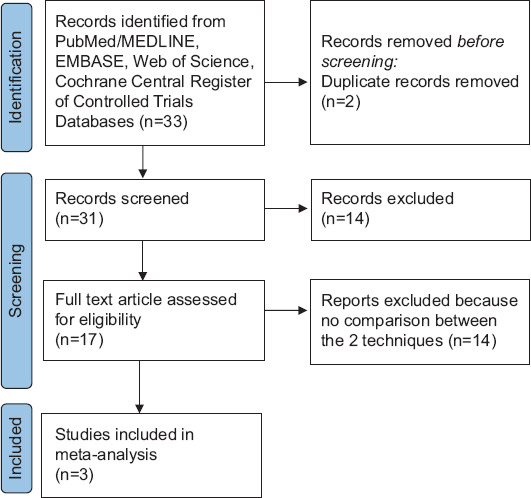
PRISMA flow diagram for selection of studies [9]
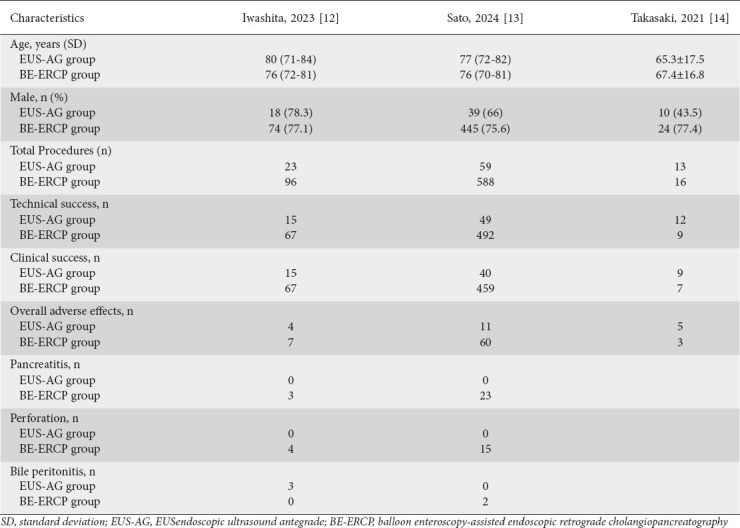
The mean age of participants included in the study was 65±15 years, with 610 (74%) males. Table 1 shows the demographic details and outcomes for each study. A total of 95 EUS-AG and 700 BE-ERCP procedures were performed in patients with RYGB.
Table 1.
Baseline study demographics and outcomes for each study
Primary outcomes
The technical success rates of EUS-AG and BE-ERCP were similar (RR 1.08, 95%CI 0.84-1.38; P=0.57; I2=56%; Fig. 2A). The overall rate of adverse effects was higher in the BE-ERCP group than in the EUS-AG group (RR 1.95, 95%CI 1.21-3.15; P=0.006; I2=0%; Fig. 2B).
Figure 2.
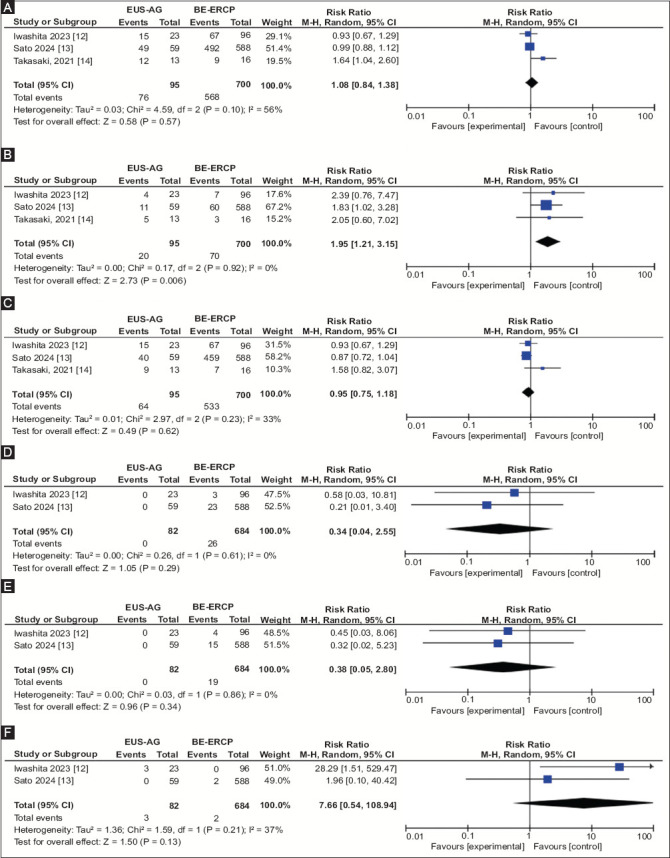
EUS guided antegrade treatment vs Balloon enteroscopy ERCP for biliary disease in patients with Roux en Y gastrectomy. (A) Forest plot comparing technical success of EUS-AG vs BE-ERCP for biliary disease in Roux en Y gastrectomy. (B) Forest plot comparing overall adverse effects of EUS-AG vs BE-ERCP for biliary disease in Roux en Y gastrectomy. (C) Forest plot comparing clinical success of EUS-AG vs BE-ERCP for biliary disease in Roux en Y gastrectomy. (D) Forest plot comparing rate of pancreatitis of EUS-AG vs BE-ERCP for biliary disease in Roux en Y gastrectomy. (E) Forest plot comparing rate of perforation of EUS-AG vs BE-ERCP for biliary disease in Roux en Y gastrectomy. (F) Forest plot comparing rate of bile peritonitis of EUS-AG vs BE-ERCP for biliary disease in Roux en Y gastrectomy
EUS-AG, endoscopic ultrasound-guided antegrade; BE-ERCP, balloon enteroscopy-assisted endoscopic retrograde cholangiopancreatography; CI, confidence interval
Secondary outcomes
The clinical success rate of EUS-AG was similar to that of BE-ERCP (RR 0.95, 95%CI 0.75-1.18; P=0.62; I²=33%; Fig. 2C).
Adverse events
The 2 groups were similar in terms of pancreatitis (RR 0.34, 95%CI 0.04-2.55; P=0.29; I²=0%; Fig. 2D), perforation (RR 0.38, 95%CI 0.05-2.80; P=0.34; I²=0%; Fig. 2E), and bile peritonitis (RR 7.66, 95%CI 0.54-108.94; P=0.13; I²=37%; Fig. 2F).
Bias assessment
The bias assessment of the included observational studies using the Newcastle–-Ottawa scale showed a score of 5-8 for all studies (Supplementary Table 2 (122KB, pdf) ). The publication bias was difficult to assess both qualitatively and quantitatively, as the number of studies was insufficient.
Discussion
To the best of our knowledge, this study represents the first systematic review and meta-analysis to compare EUS-AG and BE-ERCP specifically in the context of RYGB patients. Based on this meta-analysis, the technical and clinical success rates were comparable between EUS-AG and BE-ERCP, as were the incidences of pancreatitis, perforation and bile leak, suggesting a similar safety profile. However, it is noteworthy that the overall rate of adverse effects was found to be higher in the BE-ERCP group compared to the EUS-AG group. This observation may influence the choice of technique, favoring EUS-AG over BE-ERCP for its potentially lower risk of adverse effects.
ERCP in patients with surgically altered anatomy is difficult, and requires an experienced endoscopist, a good understanding of the length of afferent limb, the type of endoscope used with choice of approach, and compatible ERCP accessories with various endoscopic types [15].
Device-assisted enteroscopy (DAE) procedures are currently considered the first-line approach for patients with Roux-en-Y anatomy, because of their lower costs and risks compared to surgery [16]. DAE can be performed with BE-ERCP or spiral enteroscopy. Recently, alternative access techniques, including LA-ERCP and EDGE, have been gaining importance through improving efficacy and success rates. Studies report that LA-ERCP and EDGE show greater technical, cannulation and therapeutic success compared to enteroscopy-assisted ERCP, though they are also associated with more adverse events [17].
The core of our findings indicates that there is no significant difference in the technical and clinical success rates between EUS-AG and BE-ERCP. This outcome suggests that both techniques are equally viable options for endoscopic intervention in RYGB, allowing for flexibility in clinical decision-making based on the practitioner’s expertise and the specific circumstances of each case [12-14]. Itoi et al, in a recent case series of patients with surgically altered anatomy and choledocholithiasis, report a technical success rate of 60% with the EUS-AG technique [18]. Iwashita et al also reported the results of a prospective study of AG stenting in 20 patients with surgically altered anatomy. In their study, the technical and clinical success rates of EUS-AG treatment were both 95% [19].
Our meta-analysis showed a higher overall adverse event rate in the BE-ERCP group as compared to EUS-AG, and our results are on a par with what has been reported in the literature. A recent retrospective analysis by Gerson et al demonstrated that double BE is associated with a higher complication rate compared with standard endoscopic procedures. The perforation rate was significantly elevated in patients with altered surgical anatomy undergoing diagnostic retrograde double BE procedures [20]. Inamdar et al also reported an overall 32 adverse events, mainly involving pancreatitis, bleeding, perforation and death from embolic stroke [21]. Sato et al reported aspiration pneumonia in 4 patients, respiratory failure in 2 patients, pulmonary embolism in 1 and bradycardia in 1 patient in BE-ERCP patients, compared to none of these adverse effects in patients undergoing EUS-AG [13]. Differences in the pooled safety of these procedures are a key finding of this study.
We acknowledge the limitations associated with our study. First, the sample size is small, with only 795 patients. No RCTs were available comparing EUS-AG and BE-ERCP, and our results were based on observational studies, with their inherent bias. Hence, we advocate for the need for high-quality RCTs comparing both techniques in terms of their efficacy, risks and complications. Third, given the low number of full studies reporting all possible adverse effects, we cannot fully evaluate the adverse effects profile for each procedure. Fourth, the experience of endoscopists cannot be disregarded. Lastly, the procedures were performed in high volume tertiary centers, limiting generalizability. However, despite these limitations we performed a robust systematic review with stringent inclusion and exclusion criteria. Moreover, as it is the only meta-analysis focusing on this topic, the findings of this study add valuable information to the current literature.
In conclusion, we noted no statistical difference in the rates of technical success, clinical success, pancreatitis, perforation or bile peritonitis between the 2 endoscopic techniques. The overall rate of adverse effects was higher in the BE-ERCP group than in the EUS-AG group. Future well-conducted studies are needed to validate our findings.
Summary Box
What is already known:
Endoscopic ultrasound (EUS)-directed transgastric (EDGE) and laparoscopic-assisted (LA) endoscopic retrograde cholangiopancreatography (ERCP) are increasingly used for the management of choledocholithiasis in patients with Roux-en-Y gastric bypass (RYGB)
Balloon enteroscopy-assisted ERCP (BE-ERCP) is associated with more adverse effects and less technical success compared to LA-ERCP and EDGE
What the new findings are:
EUS-antegrade treatment is a newer technique for the management of choledocholithiasis in RYGB
EUS-antegrade treatment is associated with fewer overall adverse effects compared to BE-ERCP
Biography
University of Toledo, Ohio, USA; Bon secours Mercy Health, Toledo, Ohio, USA; University of New South Wales, Sydney, Australia; University of Iowa Hospitals and Clinics, Iowa City, USA; Henry Ford Hospital, Detroit, Michigan, USA; University of Toledo Libraries, Toledo, Ohio, USA; Geisinger Wyoming valley medical center, Wilkes-Barre, Pennsylvania, USA; West Virginia University, Morgantown, USA; Orlando Gastroenterology, Florida, USA; United Health Services, Binghamton, New York, USA
Footnotes
Conflict of Interest: None
References
- 1.Sanders DJ, Bomman S, Krishnamoorthi R, Kozarek RA. Endoscopic retrograde cholangiopancreatography:current practice and future research. World J Gastrointest Endosc. 2021;13:260–274. doi: 10.4253/wjge.v13.i8.260. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Elmunzer BJ. Reducing the risk of post-endoscopic retrograde cholangiopancreatography pancreatitis. Dig Endosc. 2017;29:749–757. doi: 10.1111/den.12908. [DOI] [PubMed] [Google Scholar]
- 3.Moreels TG. ERCP in the patient with surgically altered anatomy. Curr Gastroenterol Rep. 2013;15:343. doi: 10.1007/s11894-013-0343-3. [DOI] [PubMed] [Google Scholar]
- 4.Baron TH. Approaches to ERCP in patients with Roux-en-Y gastric bypass anatomy. Gastroenterol Hepatol (N Y) 2019;15:622–624. [PMC free article] [PubMed] [Google Scholar]
- 5.Khara HS, Parvataneni S, Park S, Choi J, Kothari TH, Kothari ST. Review of ERCP techniques in Roux-en-Y gastric bypass patients:highlight on the novel EUS-directed transgastric ERCP (EGDE) technique. Curr Gastroenterol Rep. 2021;23:10. doi: 10.1007/s11894-021-00808-3. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Ayoub F, Brar TS, Banerjee D, et al. Laparoscopy-assisted versus enteroscopy-assisted endoscopic retrograde cholangiopancreatography (ERCP) in Roux-en-Y gastric bypass:a meta-analysis. Endosc Int Open. 2020;8:E423–E436. doi: 10.1055/a-1070-9132. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Mukai S, Itoi T, Sofuni A, et al. EUS-guided antegrade intervention for benign biliary diseases in patients with surgically altered anatomy (with videos) Gastrointest Endosc. 2019;89:399–407. doi: 10.1016/j.gie.2018.07.030. [DOI] [PubMed] [Google Scholar]
- 8.Kedia P, Tarnasky PR, Nieto J, et al. EUS-directed transgastric ERCP (EDGE) versus laparoscopy-assisted ERCP (LA-ERCP) for Roux-en-Y gastric bypass (RYGB) anatomy:a multicenter early comparative experience of clinical outcomes. J Clin Gastroenterol. 2019;53:304–308. doi: 10.1097/MCG.0000000000001037. [DOI] [PubMed] [Google Scholar]
- 9.Page MJ, David M, Patrick MB, et al. PRISMA 2020 explanation and elaboration:updated guidance and exemplars for reporting systematic reviews. BMJ. 2021;372:n160. doi: 10.1136/bmj.n160. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Higgins JP, Thompson SG, Deeks JJ, Altman DG. Measuring inconsistency in meta-analyses. BMJ. 2003;327:557–560. doi: 10.1136/bmj.327.7414.557. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Ardolino E, Wang SS, Patwardhan VR. Evidence of significant ceftriaxone and quinolone resistance in cirrhotics with spontaneous bacterial peritonitis. Dig Dis Sci. 2019;64:2359–2367. doi: 10.1007/s10620-019-05519-4. [DOI] [PubMed] [Google Scholar]
- 12.Iwashita T, Iwasa Y, Senju A, et al. Comparing endoscopic ultrasound-guided antegrade treatment and balloon endoscopy-assisted endoscopic retrograde cholangiopancreatography in the management of bile duct stones in patients with surgically altered anatomy:a retrospective cohort study. J Hepatobiliary Pancreat Sci. 2023;30:1078–1087. doi: 10.1002/jhbp.1321. [DOI] [PubMed] [Google Scholar]
- 13.Sato T, Nakai Y, Kogure H, et al. ERCP using balloon-assisted endoscopes versus EUS-guided treatment for common bile duct stones in Roux-en-Y gastrectomy. Gastrointest Endosc. 2024;99:193–203. doi: 10.1016/j.gie.2023.09.001. [DOI] [PubMed] [Google Scholar]
- 14.Takasaki Y, Ishii S, Shibuya T, et al. Endoscopic ultrasound-guided antegrade procedures for managing bile duct stones in patients with surgically altered anatomy:comparison with double-balloon enteroscopy-assisted endoscopic retrograde cholangiography (with video) Dig Endosc. 2021;33:1179–1187. doi: 10.1111/den.13927. [DOI] [PubMed] [Google Scholar]
- 15.Krutsri C, Kida M, Yamauchi H, Iwai T, Imaizumi H, Koizumi W. Current status of endoscopic retrograde cholangiopancreatography in patients with surgically altered anatomy. World J Gastroenterol. 2019;25:3313–3333. doi: 10.3748/wjg.v25.i26.3313. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Wang TJ, Ryou M. Evolving techniques for endoscopic retrograde cholangiopancreatography in gastric bypass patients. Curr Opin Gastroenterol. 2018;34:444–450. doi: 10.1097/MOG.0000000000000474. [DOI] [PubMed] [Google Scholar]
- 17.Gkolfakis P, Papaefthymiou A, Facciorusso A, et al. Comparison between enteroscopy-, laparoscopy- and endoscopic ultrasound-assisted endoscopic retrograde cholangio-pancreatography in patients with surgically altered anatomy:a systematic review and meta-analysis. Life (Basel) 2022;12:1646. doi: 10.3390/life12101646. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Itoi T, Sofuni A, Tsuchiya T, Ijima M, Iwashita T. Endoscopic ultrasonography-guided transhepatic antegrade stone removal in patients with surgically altered anatomy:case series and technical review (with videos) J Hepatobiliary Pancreat Sci. 2014;21:E86–E93. doi: 10.1002/jhbp.165. [DOI] [PubMed] [Google Scholar]
- 19.Iwashita T, Nakai Y, Hara K, Isayama H, Itoi T, Park DH. Endoscopic ultrasound-guided antegrade treatment of bile duct stone in patients with surgically altered anatomy:a multicenter retrospective cohort study. J Hepatobiliary Pancreat Sci. 2016;23:227–233. doi: 10.1002/jhbp.329. [DOI] [PubMed] [Google Scholar]
- 20.Gerson LB, Tokar J, Chiorean M, et al. Complications associated with double balloon enteroscopy at nine US centers. Clin Gastroenterol Hepatol. 2009;7:1177–1182. doi: 10.1016/j.cgh.2009.07.005. 1182.e1-3. [DOI] [PubMed] [Google Scholar]
- 21.Inamdar S, Slattery E, Sejpal DV, et al. Systematic review and meta-analysis of single-balloon enteroscopy-assisted ERCP in patients with surgically altered GI anatomy. Gastrointest Endosc. 2015;82:9–19. doi: 10.1016/j.gie.2015.02.013. [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.