

Abstract
This cross-sectional study evaluates growth of transport policies and policy components that directed emergency medical services (EMS) to bypass local emergency departments for the closest certified stroke centers as a proven treatment for stroke.
Introduction
Stroke is a leading cause of mortality and long-term morbidity in the US.1 Rapid prehospital transport to certified stroke centers is critical to restore the blood supply to the brain with clot-lysing drugs (thrombolytics) or clot-retrieval procedures (thrombectomy).2 Stroke systems of care (SSOC) coordinate, integrate, and streamline transport of patients by emergency medical services (EMS) to certified stroke centers, which have higher treatment utilization and lower mortality than noncertified centers.3,4 Using policy data sources, we evaluated growth of SSOC EMS transport policies and policy components that directed EMS to bypass local emergency departments for the closest certified stroke centers as a proven treatment for stroke.
Methods
Centers for Disease Control and Prevention (CDC) legal analysts retrospectively analyzed SSOC laws that went into effect from January 1, 2005, through January 1, 2020, across 50 states and Washington, DC, using the Westlaw Next search engine. Laws were independently and redundantly coded by policy effective date and level of authority (required, required with exceptions, authorized, prohibited, or not applicable/silent) by 2 legal analysts. Discrepancies were addressed via discussion until a consensus was met. If the language of the law fell short of authorized, it was coded as “other.” If a law did not address a policy intervention, it was coded as not applicable/silent. The search was supplemented with published data from state websites and previous publications.5 This study was approved by the institutional review board at Stanford University.
We listed the stroke policy components and included definitions from the Westlaw Next database (Table). The stroke policies included center-based and EMS-based components, tiered stroke centers, stroke task force or statewide or regional continuous quality improvement, EMS triage and transport protocols, stroke alerts, and stroke assessments. We also tracked each stroke policy component over time for states with and without a stroke policy implementation.
Table. Statewide Stroke Policy Components and Definitions, 2005-2020.
| Stroke policy component | Definition |
|---|---|
| Tiered stroke centers | Law expressly requires or authorizes hospitals or other health care facilities to hold themselves out as providing stroke care at a specified level |
| Standardized emergency medical technician stroke assessment | Law authorizes emergency medical technician education and/or training in stroke assessment, triage and transport using stroke protocols, scales, or other assessment tools |
| Stroke task force or continuous quality improvement, statewide or regional | Law requires or authorizes establishment of a task force, advisory body, council, commission, committee, subcommittee, workgroup, or similar entity whose role is to oversee or advise on the development and/or implementation of a SSOC or the coordination of stroke care across EMS, hospital, and posthospital care within an existing trauma system of care; law expressly establishes or authorizes a statewide (defined as a state-level or centralized approach to providing care across the state) stroke CQI plan; planning process; process, program, or stroke system evaluation; system performance monitoring (or measurement); and stroke system quality assurance |
| EMS stroke alerts | Law expressly authorizes prenotification (direct communication) between EMS and receiving facility that an emergency medical technician is transporting a patient with a suspected stroke to the facility by ground or air |
| EMS triage and transport protocols | Law expressly authorizes or requires statewide and/or regional EMS protocols for stroke assessment and triage and statewide and/or regional EMS transport protocols to a stroke facility using ground transport |
Abbreviations: CQI, continuous quality improvement; EMS, emergency medical services; SSOC, stroke system of care.
States with SSOC EMS policies were recorded for each study year. Data were summarized with statewide SSOC EMS policies each year from January 1, 2005, to January 1, 2020. Data were analyzed using Stata/MP, version 16.1 (StataCorp).
Results
The Figure displays the stroke policy components by statewide EMS bypass policy status over time. Sixteen states had stroke policy components in place before a statewide EMS policy was in effect. Policies were not found to be clustered regionally. Many stroke policy components were enacted simultaneously, and for 17 states, these components were in place soon after the statewide EMS bypass policy went into effect.
Figure. Growth of Emergency Medical Services (EMS) Bypass Policies and Components for Patients With Acute Stroke, 2005-2020.
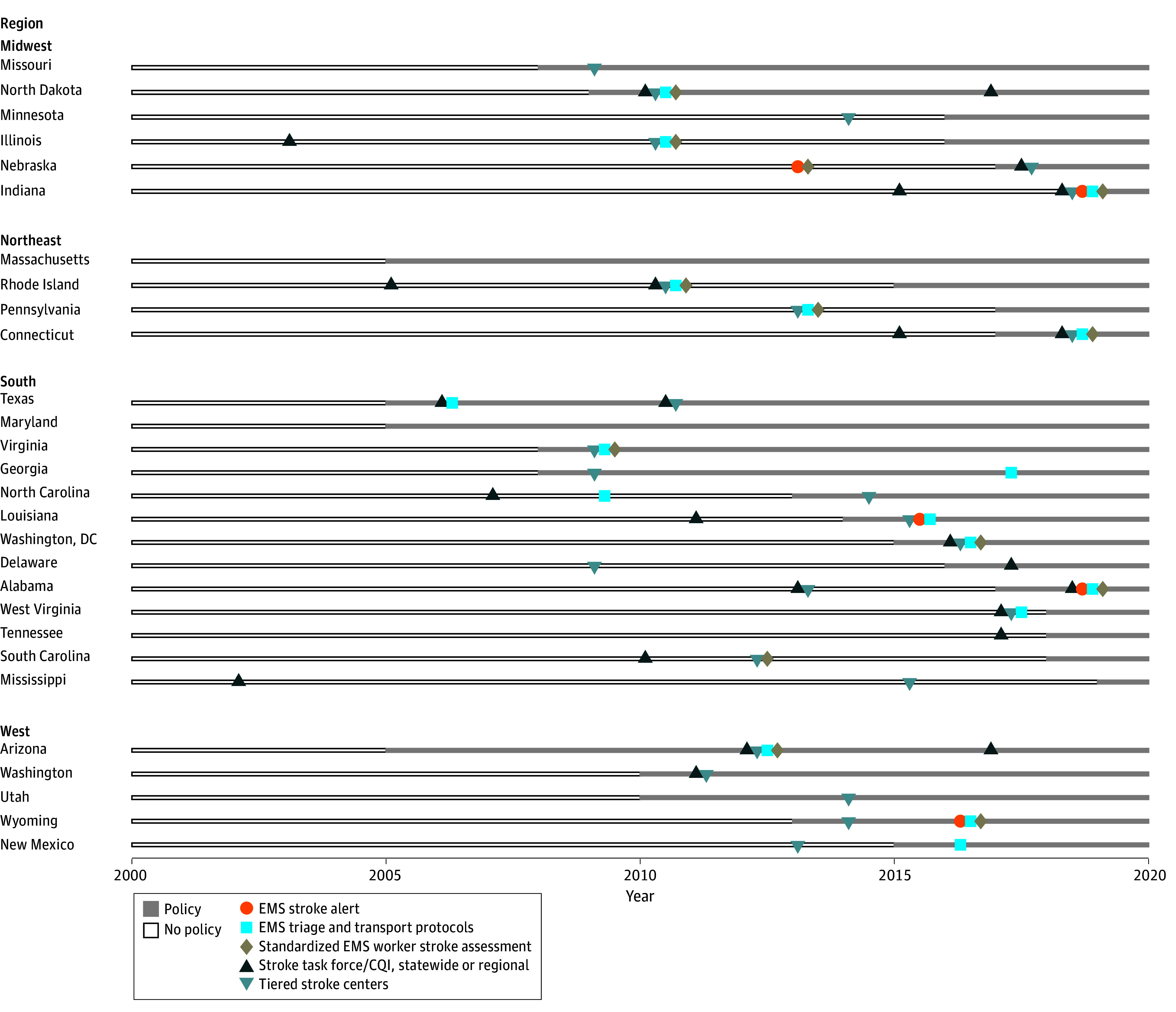
CQI indicates continuous quality improvement.
Discussion
SSOC EMS policies increased from 2005 to 2020, consistent with prior literature and efforts to enhance acute stroke care.5,6 An early evaluation of EMS bypass policies and stroke center designation demonstrated improved quality of care, including timely assessment and higher treatment.6 However, it is unknown whether these initiatives have directly led to more patients being transported to stroke centers and greater use of thrombolytics in varied populations. While this analysis represents a first step in understanding the effect of these policies on stroke outcomes, additional research is needed to understand the impact over time.
Although EMS bypass policies were enacted early in the 21st century, expansion began during 2010 and accelerated after 2015. Novel treatments (ie, thrombectomy) implemented for patients with acute ischemic stroke coupled with the need for ambulance transport of these patients to specialized centers for treatment may have led to the expansion of these policies. Stroke task forces were created in many states along with the enactment of stroke care policies. Presently, many states with an SSOC policy have tiered stroke centers that include basic and advanced treatment facilities to cater to patients.
A primary limitation of this study is the lack of data available for states with no policies. However, this analysis sets the stage for the future evaluation of SSOC policies. If SSOC policies and policy components generate the expected benefits of greater utilization of stroke centers, future guidelines could standardize best practices in acute stroke care, thereby minimizing outcome differences across regions.
Data Sharing Statement
References
- 1.Stroke facts. Centers for Disease Control and Prevention . May 15, 2024. Accessed May 28, 2024. https://www.cdc.gov/stroke/data-research/facts-stats/?CDC_AAref_Val=https://www.cdc.gov/stroke/facts.htm
- 2.Gauberti M, Martinez de Lizarrondo S, Vivien D. Thrombolytic strategies for ischemic stroke in the thrombectomy era. J Thromb Haemost. 2021;19(7):1618-1628. doi: 10.1111/jth.15336 [DOI] [PubMed] [Google Scholar]
- 3.Rajamani K, Millis S, Watson S, et al. Thrombolysis for acute ischemic stroke in Joint Commission–certified and –noncertified hospitals in Michigan. J Stroke Cerebrovasc Dis. 2013;22(1):49-54. doi: 10.1016/j.jstrokecerebrovasdis.2011.06.003 [DOI] [PubMed] [Google Scholar]
- 4.Man S, Schold JD, Uchino K. Impact of stroke center certification on mortality after ischemic stroke: the Medicare cohort from 2009 to 2013. Stroke. 2017;48(9):2527-2533. doi: 10.1161/STROKEAHA.116.016473 [DOI] [PubMed] [Google Scholar]
- 5.Song S, Saver J. Growth of regional acute stroke systems of care in the United States in the first decade of the 21st century. Stroke. 2012;43(7):1975-1978. doi: 10.1161/STROKEAHA.112.657809 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Gropen TI, Gagliano PJ, Blake CA, et al. ; NYSDOH Stroke Center Designation Project Workgroup . Quality improvement in acute stroke: the New York state stroke center designation project. Neurology. 2006;67(1):88-93. doi: 10.1212/01.wnl.0000223622.13641.6d [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
Data Sharing Statement