

 This work is licensed under a
This work is licensed under a Abstract
Background
Current guidelines recommend different postpartum approaches for patients started on levothyroxine (LT4) during pregnancy.
Objective
We studied the postpartum management of these patients and determined factors associated with long-term hypothyroidism.
Methods
A retrospective study was conducted at a tertiary center between 2014 and 2020, with LT4 initiation according to 2014 ETA recommendations. We performed multivariate logistic regression (MVR) and a receiver operating characteristic curve analysis to determine variables associated with long-term hypothyroidism and their optimal cutoffs.
Results
LT4 was initiated in 177 pregnant women, and 106/177 (60%) were followed at long-term (at least 6 months post partum) (28.5 (9.0–81.9) months). LT4 could have been stopped in 45% of patients who continued it immediately after delivery. Thirty-six out of 106 (34%) patients were long-term hypothyroid. In them, LT4 was initiated earlier during pregnancy than in euthyroid women (11.7 ± 4.7 vs 13.7 ± 6.5 weeks, P = 0.077), at a higher thyroid-stimulating hormone (TSH) level (4.1 (2.2–10.1) vs 3.5 (0.9–6.9) mU/L, P = 0.005), and reached a higher dose during pregnancy (62.8 ± 22.2 vs 50.7 ± 13.9 µg/day, P = 0.005). In the MVR, only the maximal LT4 dose during pregnancy was associated with long-term hypothyroidism (odds ratio (OR) = 1.03, 95% CI: 1.00–1.05, P = 0.003). The optimal cutoffs for predicting long-term hypothyroidism were an LT4 dose of 68.75 µg/day (87% specificity, 42% sensitivity; P = 0.013) and a TSH level ≥ 3.8 mU/L (68.5% specificity, 77% sensitivity; P = 0.019).
Conclusion
One-third of the patients who started on LT4 during pregnancy had long-term hypothyroidism. The TSH level at treatment initiation and the LT4 dose during pregnancy could guide the decision for continuing long-term LT4.
Keywords: levothyroxine, pregnancy, hypothyroidism, follow-up
Introduction
Hypothyroidism diagnosed during pregnancy, whether subclinial or overt, is associated with adverse pregnancy and neonatal outcomes (1). Existing guidelines unanimously recommend the treatment of overt hypothyroidism (OH) in this setting, but some controversy remains about the management of subclinical hypothyroidism (SCH). The European Thyroid Association (ETA) recommends treating SCH with levothyroxine (LT4) to normalize maternal serum thyroid-stimulating hormone (TSH) values within the trimester-specific pregnancy reference range or, when not available, to the following reference range upper limits: first trimester, 2.5 mU/L; second trimester, 3.0 mU/L; third trimester, 3.5 mU/L (2). The more recent American Thyroid Association (ATA) guidelines recommend LT4 treatment in patients with TSH levels above the pregnancy trimester-specific reference range and to be considered in women with thyroid autoimmunity (TAI) with a serum TSH ≥2.5 mIU/L (3), given the association between thyroid autoantibodies, miscarriage, and preterm birth (4). Where pregnancy trimester-specific reference ranges are not available, the ATA suggests an upper limit of about 4 IU/mL for the first trimester, based on newer data on factors influencing the upper reference range of normal TSH. The same cutoff was recently advocated by the ETA guideline for the management of thyroid disorders in women undergoing assisted reproduction (5). In contrast to the ETA, ATA does not recommend the treatment of first-trimester isolated hypothyroxinemia (2, 3).
There are also differences in the postpartum management of patients started on LT4 during pregnancy. According to the ETA, LT4 treatment could be discontinued at delivery in women with TSH less than 5 mU/L and negative thyroperoxidase antibodies (TPOAb) at diagnosis. In contrast, the ATA considers treatment discontinuation in women requiring an LT4 dose of ≤ 50 µg/day during pregnancy, after a discussion between the patient and the caregiver (2, 3). Few studies have investigated the evolution of postpartum thyroid function in women for whom LT4 was initiated during pregnancy, but the incidence of persistent hypothyroidism after delivery could be as high as one-third of the patients (6, 7, 8), calling for a more accurate management of LT4 treatment started during pregnancy.
The aim of our study was to determine the postpartum management and long-term evolution of thyroid function in women started on LT4 during pregnancy, as well as the predictive factors of persistent hypothyroidism.
Materials and methods
We retrospectively analyzed the medical records of 985 pregnant women treated with LT4 during pregnancy and followed at a single tertiary center between January 2014 and December 2020 in Brussels, Belgium. From these women, 500 were excluded because of LT4 initiation before pregnancy, 94 patients for known thyroid disease or taking drugs interfering with thyroid function, and 214 patients because of missing data. Specifically, 149/214 (69%) because of no information on LT4 dose (these were patients seen in our hospital during the last trimester of pregnancy, with treatment initiated in another hospital), 10/214 (5%) because of no information on thyroid function at LT4 initiation, 42/214 (20%) due to no information about the timing of LT4 initiation (before or during the pregnancy), and 13/214 (6%) because of follow-up during pregnancy in another hospital.
Patients treated with LT4 during or outside a previous pregnancy in whom the treatment was withdrawn were included. The final analysis included 177 patients in whom LT4 was initiated during pregnancy. In total, 106 of these patients were followed for 6 months or more after delivery and analyzed for ‘long-term’ persistent hypothyroidism. Figure 1 illustrates the study selection process in detail.
Figure 1.

Flowchart of patients started on LT4 during pregnancy and their postpartum long-term thyroid status. LT4: levothyroxine; long-term follow-up: at least 6 months postpartum follow-up.
Thyroid function tests and criteria for LT4 initiation during pregnancy
In our hospital, thyroid function (TSH and freeT4) and the presence of TPOAb are routinely tested at the first obstetrical visit during the first trimester of pregnancy. Locally derived trimester-specific reference ranges for free T4 (FT4) exist in our hospital since June 2014, but for TSH, only the non-pregnant reference range is available. Before June 2014, TSH, FT4, and thyroid antibodies were measured with a chemiluminescent immunoassay (DXL, Beckman Coulter), and after June 2014 using an electrochemiluminescent immunoassay on a Cobas e602 analyzer (Roche Diagnostics). The reference ranges were as follows: TSH 0.2–3.5 mU/L before June 2014 and 0.27–4.2 mU/L after June 2014; FT4: 12–22 pmol/L non-pregnant, 12.6–19.7 pmol/L first trimester, 9.7–17.5 pmol/L second trimester, 8.1–15.3 pmol/L third trimester; TPOAb positive >5.1 U/mL before June 2014 and >115 U/m–L after June 2014.
LT4 treatment was prescribed according to the 2014 ETA guidelines recommendations (2). The thyroid status at LT4 initiation was defined as follows: euthyroidism (normal range TSH and normal trimester-specific range FT4); SCH (TSH above upper normal range and normal trimester-specific FT4); OH (TSH above upper normal range and FT4 below normal trimester-specific range); and isolated hypothyroxinemia (normal TSH and FT4 below normal trimester-specific range).
Thyroid status at long-term postpartum follow-up
Euthyroidism was defined as normal TSH without LT4 treatment, hypothyroidism as normal TSH under LT4 treatment or TSH above the upper normal range with or without LT4 treatment, and hyperthyroidism as TSH below the lower normal range in the absence of LT4 treatment.
Statistical analysis
Statistical analyses were performed using the IPSS Statistics software from IBM (version 25.0). A P-value of less than 0.05 was considered significant. Continuous variables were described either as mean ± s.d. or median with the percentiles 5 and 95. Discrete variables were described using their frequency. Subgroup analyses were performed using Pearson’s χ2 test for categorical unpaired variables. Student’s t-test was used for comparing means of continuous unpaired variables. We performed univariate and multivariate logistic regression analysis (MVR) to determine variables associated with long-term hypothyroidism. We included in the MVR only those variables that were significantly associated (P < 0.1) with long-term hypothyroidism in univariate logistic regression. Finally, we used receiver operating characteristic (ROC) curve analysis to describe optimal cutoffs and area under the curve (AUC) for factors significantly associated with long-term hypothyroidism in MVR. For MVR, all input variables were entered simultaneously.
Results
Characteristics of patients started on LT4 during pregnancy
The general characteristics of the 177 patients initiated on LT4 during pregnancy were in majority similar to those of the pregnant population in Brussels area for the reference year 2021. The mean age at diagnosis was 30.9 ± 4.9 years, the pre-conception BMI was 24.5 ± 4.8 kg/m², and 94/177 (53%) of women were multiparous. Twenty-three of 147 (15.5%) patients had a history of LT4 treatment during a previous pregnancy. There were more women with infertility history in our population (32/177 (18%)) than in the reference Belgian population (5.4%). The pregnancy and neonatal outcomes were similar in terms of gestational diabetes, birth weight, prematurity, and pre-eclampsia. Additionally, there were fewer cases of macrosomia and neonatal unit admissions in our population (11/172 (6.5%) vs 13% and 12/172 (7%) vs 10.1%, respectively).
At LT4 treatment initiation, 24/177 (13.5%) of patients were euthyroid, 105/177 (59.5%) had SCH, 31/177 (17.5%) had OH, and 17/177 (9.5%) had isolated hypothyroxinemia. LT4 treatment was initiated at a mean gestational age of 13.1 (9–16.8) weeks, at a median TSH of 3.6 (1.2–7.1) mU/L, and a mean FT4 of 12.6 ± 2.5 pmol/L. TPOAb was measured at the time of LT4 treatment initiation and was positive in 75/168 (45%) of patients (Table 1). Of the 24 women initiated on LT4 while being euthyroid, 14/24 (58%) were TPOAb positive, and in most of them, the treatment was initiated for that reason. The reason for LT4 initiation in euthyroid TPOAb-negative patients was not always specified, but 3/10 patients had an IVF procedure, and 2/10 patients were TgAb positive. The LT4 treatment was initiated by the endocrinologist in only 37/177 (21%) of patients, but the majority of patients (139/177 (78.5%)) were further followed by the endocrinologist during pregnancy. The maximal mean LT4 dose reached during pregnancy was 54.2 ± 16.2 µg/day.
Table 1.
Characteristics of patients started on LT4 during pregnancy. Results are shown as mean ± s.d. or median (percentile 5–95).
| Characteristics | n | Values |
|---|---|---|
| Gestational age (weeks) | 177 | 13.1 ± 6.7 |
| TSH (mU/L) | 177 | 3.6 (1.2–7.1) |
| FT4 (pmol/L) | 176 | 12.6 ± 2.5 |
| TPOAb ULN | 168 | 0.5 (0.14–14.71) |
| TPOAb + | 168 | 75/168 (45%) |
| Maximal LT4 dose during pregnancy (µg/day) | 177 | 54.2 ± 16.2 |
| LT4 prescription by endocrinologist | 177 | 37/177 (21%) |
| Follow-up by endocrinologist | 177 | 139/177 (78.5%) |
FT4, free T4; LT4, levothyroxine; TPOAb, thyroperoxidase antibodies; TPOAb ULN, a ratio of the absolute TPOAb value to the ULN; ULN, upper normal limit.
Characteristics of patients started on LT4 during pregnancy and followed at long-term after delivery
One hundred and six of the patients (106/177; 60%) initiated on LT4 during pregnancy had long-term postpartum follow-up (Fig. 1). Forty-nine out of the 177 (28%) patients had no postpartum follow-up. There were no differences in terms of general characteristics, thyroid function tests, or LT4 treatment between patients with or without follow-up, except that followed patients were more frequently managed by endocrinologists during pregnancy (85/106 (80%) vs 32/49 (65%), P = 0.045).
The median postpartum follow-up time was 28.5 (9.0–81.8) months. Of the 106 women treated with LT4 during pregnancy and followed long-term after delivery, 13 (12.5%) were euthyroid at LT4 initiation, 11 (10.5%) had isolated hypothyroxinemia, 66 (62%) had SCH, and 16 (15%) had OH. At the last visit, 68 (64%) of patients were euthyroid, 36 (34%) were hypothyroid, and 2 (2%) were thyrotoxic. Of the women on long-term follow-up, 36/86 (42%) of those with TSH > 2.5 mU/L and 20/44 (45%) of those with TSH > 4 mU/L at diagnosis were long-term hypothyroid. Further, 34/106 (32%) patients continued or restarted LT4, at a mean dose of 57.9 ± 24.5 µg/day.
LT4 treatment discontinuation after delivery
Of the 106 long-term followed patients, 22 (21%) continued LT4 after delivery and only 49 patients discontinued the treatment. There was no information on how the remaining 35 patients were managed immediately after delivery, but most of them (24 patients; 68.5%) were euthyroid with no LT4 treatment at long-term follow-up (Fig. 1). Of the 22 patients who continued the treatment, 12 (55%) received an LT4 dose ≥ 50 µg/day during pregnancy, in contrast to only 8/49 (17%) of women who discontinued it (P = 0.001). The median TSH at LT4 initiation was higher in patients who continued the treatment compared to those who discontinued it (5.1 (2.6–8.8) mU/L vs 3.5 (1.4–9.9) mU/L, P = 0.010) (Table 2). At long-term follow-up, there were more hypothyroid patients among those who continued the treatment than among those who discontinued it (14/22 (64%) vs 13/49 (26.5%), P = 0.003) (Fig. 1).
Table 2.
Characteristics of patients who continued (n = 22) or discontinued (n = 49) LT4 treatment immediately after delivery. Results shown as mean ± s.d. or median (percentile 5–95). Values in bold indicate statistical significance.
| LT4 discontinuation | LT4 continuation | P | |
|---|---|---|---|
| General characteristics | |||
| Age (years) | 30 (21.2–38.6) | 29 (23.2–36) | 0.876 |
| Pre-conception BMI (kg/m2) | 24 (19.6–36.2) | 22 (18.6–25.4) | 0.044 |
| LT4 treatment | 0.993 | ||
| Previous treatment | 9/43 (21%) | 4/19 (21%) | |
| Previous treatment during pregnancy | 7/43 (16%) | 3/19 (15.5%) | |
| Multiparous | 27/49 (55%) | 10/22 (45.5%) | 0.383 |
| Infertility treatment | 4/49 (8%) | 3/22 (13.5%) | 0.469 |
| At LT4 initiation during pregnancy | |||
| Gestational age (weeks) | 11 (5.2–25.1) | 9.5 (3.6–21.8) | 0.239 |
| TSH (mU/L) | 3.5 (1.4–9.9) | 5.1 (2.6–8.8) | 0.010 |
| FT4 (pmol/L) | 13.8 (8.5–16.3) | 12.5 (8.9–17.5) | 0.247 |
| TPOAb ULN | 2.7 (0.21–18.12) | 0.25 (0.05–27.72) | 0.011 |
| TPOAb+ | 34/47 (72.5%) | 8/22 (36.5%) | 0.004 |
| Maximal LT4 dose during pregnancy (µg/day) | 50 (25–75) | 50 (50–100) | 0.001 |
| LT4 prescription by endocrinologist | 10/49 (20.5%) | 8/22 (36.5%) | 0.153 |
| Follow-up by endocrinologist | 45/49 (92%) | 19/22 (86.5%) | 0.669 |
FT4, free T4; LT4, levothyroxine; TPOAb, thyroperoxidase antibodies; TPOAb ULN, a ratio of the absolute TPOAb value to the ULN; ULN, upper normal limit.
Comparisons of long-term hypothyroid and euthyroid patients
The general characteristics of long-term euthyroid and hypothyroid patients at LT4 treatment initiation during pregnancy are presented in Table 3. There were no differences in terms of gestational age, BMI, parity, previous LT4 treatment, infertility, pregnancy, and neonatal outcomes between the two groups.
Table 3.
Characteristics of long-term euthyroid (n = 68) and hypothyroid (n = 36) patients at LT4 initiation during pregnancy. Results are shown as mean ± s.d . or median (percentile 5–95). Values in bold indicate statistical significance.
| Long-term euthyroid | Long-term hypothyroid | P | |
|---|---|---|---|
| Age (years) | 30.9 ± 5.2 | 30.4 ± 3.9 | 0.620 |
| Pre-conception BMI (kg/m²) | 25.1 ± 5.3 | 23.4 ± 3.4 | 0.059 |
| LT4 treament | 0.675 | ||
| Previous treatment | 10/55 (18%) | 7/32 (22%) | |
| Previous treatment during pregnancy | 9/55 (16.5%) | 5/32 (15.5%) | |
| Multiparous | 31/68 (45.5%) | 24/36 (66.5%) | 0.285 |
| Infertility treatment | 13/68 (19%) | 3/36 (8.5%) | 0.147 |
| Gestational age (weeks) | 13.7 ± 6.5 | 11.7 ± 4.7 | 0.077 |
| TSH (mU/L) | 3.5 (0.9–6.9) | 4.1 (2.2–10.1) | 0.005 |
| FT4 (pmol/L) | 12.7 ± 2.6 | 12.7 ± 2.4 | 0.901 |
| TPOAb ULN | 0.53 (0.14–17.64) | 2.37 (0.09–20.4) | 0.323 |
| TPOAb+ | 28/64 (44%) | 21/35 (60%) | 0.122 |
| TPOAb tertiles | 0.432 | ||
| 1st tertile: 0.05–0.31 × ULN | 21/64 (33%) | 12/35 (34.5%) | |
| 2nd tertile: 0.31–3.26 × ULN | 24/64 (37.5%) | 9/35 (25.5%) | |
| 3rd tertile: 3.26–42.84 × ULN | 19/64 (29.5%) | 14/35 (40%) | |
| Maximal LT4 dose during pregnancy (µg/day) | 50.7 ± 13.9 | 62.8 ± 22.2 | 0.005 |
| LT4 prescription by endocrinologist | 16/68 (23.5%) | 9/36 (25%) | 0.867 |
| Follow-up by endocrinologist | 55/68 (81%) | 30/36 (83.5%) | 0.758 |
FT4, free T4; LT4, levothyroxine; TPOAb, thyroperoxidase antibodies; TPOAb ULN, a ratio of the absolute TPOAb value to the ULN; ULN, upper normal limit.
In long-term hypothyroid patients, LT4 was initiated earlier during pregnancy than in euthyroid patients (11.7 ± 4.7 vs 13.7 ± 6.5 weeks, P = 0.077), at a higher TSH level (4.1 (2.2–10.1) vs 3.5 (0.9–6.9) mU/L, P = 0.005), and reached a higher dose during pregnancy (62.8 ± 22.2 vs 50.7 ± 13.9 µg/day, P = 0.005). LT4 dose distribution for each group was significantly different (P = 0.038). There were fewer euthyroid patients at LT4 initiation in the long-term hypothyroid patients (3% vs 17.5%, P = 0.029). There were no differences in terms of TPOAb positivity, level, or tertile between the long-term hypothyroid and the euthyroid patients.
Predictive factors of persistent hypothyroidism
In the univariate logistic regression, TSH level at LT4 initiation and the maximal LT4 dose during pregnancy were predictive for the risk of long-term hypothyroidism (OR = 1.37, 95% CI: 1.08–1.73, P = 0.009 and OR = 1.04, 95% CI: 1.01–1.06, P = 0.003, respectively), while gestational age, pre-conception BMI, or TPOAb level or positivity at LT4 initiation were not (Table 4). However, only the maximal LT4 dose during pregnancy (OR = 1.03, 95% CI: 1.00–1.05, P = 0.003) was associated with long-term hypothyroidism in multivariate logistic regression. ROC analysis showed that a maximal LT4 dose of 68.75 µg/day during pregnancy (87% specificity, 42% sensitivity; AUC = 0.649, 95% CI: 0.53–0.76; P = 0.013) and a TSH level ≥ 3.8 mU/L at treatment initiation (68.5% specificity, 77% sensitivity; AUC = 0.723, 95% CI: 0.53–0.91; P = 0.019) were the optimal cutoffs for predicting long-term hypothyroidism. (Fig. 2A and B)
Table 4.
Uni- and multivariate logistic regression analysis of factors influencing the risk of long-term hypothyroidism. Values are odds ratio with 95% CI. Values in bold indicate statistical significance.
| Univariate | Multivariate | |||
|---|---|---|---|---|
| OR (95% CI) | P | OR (95% CI) | P | |
| Gestational age | 0.944 (0.877–1.017) | 0.132 | – | |
| Pre-conception BMI | 0.924 (0.841–1.016) | 0.102 | – | |
| TSH (mU/L) | 1.371 (1.083–1.736) | 0.009 | 1.229 (0.952–1.585) | 0.113 |
| TPOAb ULN (continuous) | 1.036 (0.969–1.107) | 0.301 | – | |
| TPOAb positivity (categorical) | 1.875 (0.810–4.340) | 0.142 | – | |
| Maximal LT4 dose during pregnancy | 1.040 (1.014–1.068) | 0.003 | 1.031 (1.003–1.059) | 0.030 |
LT4, levothyroxine; TPOAb ULN, a ratio of the absolute TPOAb value to the ULN; TPOAb, thyroperoxidase antibodies; ULN, upper normal limit.
Figure 2.
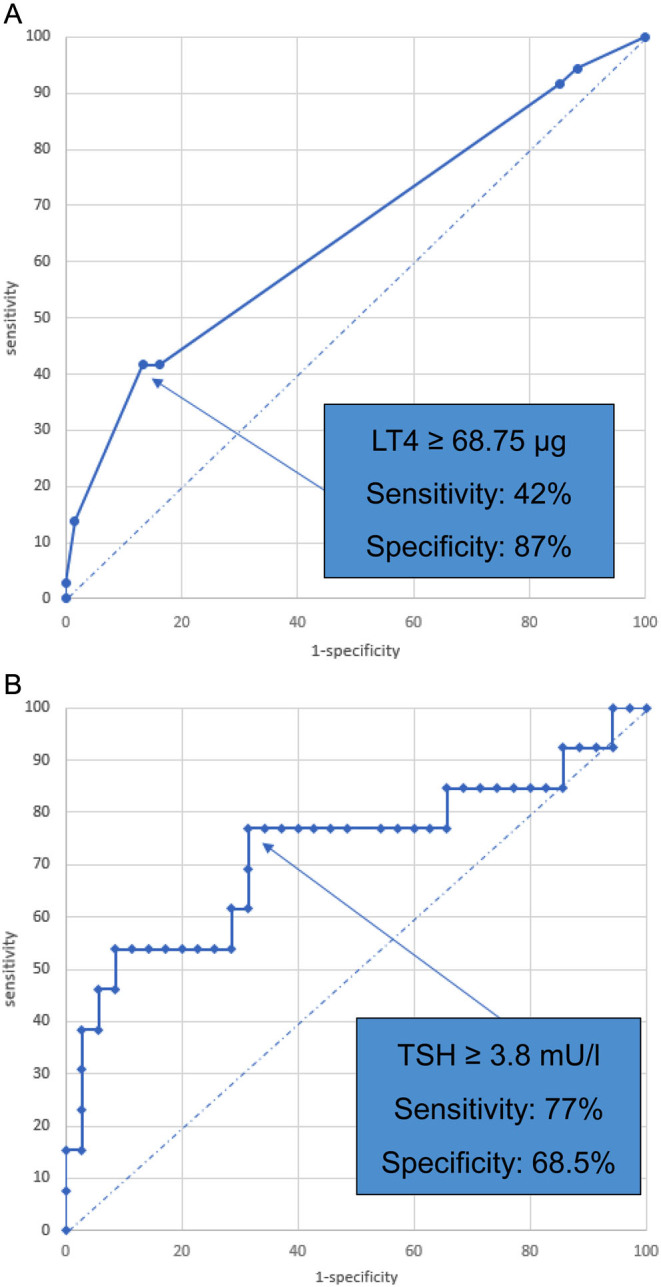
Receiver operating characteristic (ROC) curve for maximal LT4 dose (µg/day) during pregnancy (a) and TSH level (mU/L) at LT4 initiation (b) predictive for long-term hypothyroidism. LT4, levothyroxine.
Discussion
In our study of a population of pregnant women representative for our area (9), we found that one-third of patients initiated on LT4 during pregnancy had long-term persistent hypothyroidism. However, this proportion could vary according to the severity of hypothyroidism at LT4 initiation and different TSH cutoffs used to define it (6, 7, 8, 10). Shields et al. found that 16.5% of patients with SCH and isolated hypothyroxinemia had persistent high TSH levels > 4.5 mU/L over 5 years postpartum follow-up, but the proportion increased to 24.5% when only women with pregnancy SCH were considered (6). The prevalence of long-term hypothyroidism increases with the increasing cut-off of diagnostic TSH, from 18% in a large Indian study of 467 women with SCH (7) when trimester-specific TSH reference range was used, up to 39% in a recent prospective Chinese study that defined SCH as TSH > 4 mU/L (8). Although we used a lower diagnostic TSH cut-off, the rather high proportion of persistent hypothyroidism found in our study could be explained by the inclusion of a significant proportion of patients with OH. At a much higher TSH level at diagnosis during pregnancy (mean TSH 13.2 mU/L), 64% of patients developed OH over >10 years follow-up in the seminal study by Haddow et al. (11).
Another confounding factor for the prevalence of persistent hypothyroidism is the continuation of LT4 treatment after delivery. In our study, there were significantly more patients who continued the treatment after delivery in the long-term hypothyroid group than in the euthyroid group. The reason for treatment continuation was not always known, and we cannot rule out therapeutic inertia, as almost half of those who continued the treatment had a TSH < 4.0 mU/L at LT4 initiation and received during pregnancy a maximal LT4 dose of 50 µg/day or less, which should have been stopped according to current recommendations (3, 12). These patients account for almost one-third of long-term hypothyroid patients and could lead to an overestimation of the persistence of hypothyroidism. In the study by Linardi et al., the prevalence of persistent hypothyroidism goes down from 75.5% to 28% when only the patients who discontinued the treatment are analyzed (10).
If discontinuation of LT4 treatment after delivery is not considered, this could lead to long-term overtreatment, especially when the indication for LT4 initiation during pregnancy is not justified. In our study, LT4 was started in 13.5% of patients although they were euthyroid according to 2014 ETA criteria. If the 2017 ATA criteria had been applied, 50/177 (28%) patients would have been treated. Recent evidence does not support LT4 treatment in euthyroid women, whether TPOAb was positive or not, including those with a miscarriage history (13, 14). Moreover, LT4 treatment was initiated in 9.5% of patients in our study for isolated hypothyroxinemia, according to 2014 ETA guidelines. Although isolated hypothyroxinemia in pregnancy has been associated with adverse maternal metabolic profile and obstetrical outcomes (15, 16) and intellectual disability in offspring (17), current evidence does not support LT4 treatment for this indication (16).
In our study, we found that the TSH level at treatment initiation and the maximal LT4 dose during pregnancy are predictive of persistent hypothyroidism. Previous studies have found associations between long-term hypothyroidism and TSH > 5 mU/L at diagnosis (6, 7, 10), LT4 dose at the end of pregnancy (7), TPOAb (6, 7, 8), or TgAb (8) positivity at diagnosis and at 6 weeks postpartum follow-up (8), gestational age at treatment initiation (8), multiparity (10), or maternal age (7). TSH was significantly higher at LT4 initiation in patients who were long-term hypothyroid in our study, and a TSH level > 3.8 mU/L was predictive of this evolution. This value is also close to the 4.0 mU/L cutoff beyond which epidemiological studies have shown an association between thyroid function and adverse maternal and neonatal outcomes (18, 19, 20), and beyond which the 2017 ATA guidelines suggest initiating LT4 treatment during pregnancy where pregnancy trimester-specific reference range is not available. In addition, a maximal LT4 dose of 68.57 µg/day was found predictive of long-term hypothyroidism in our study. This dose, larger more than the 50 µg cutoff suggested by ATA guidelines (3), might be explained by the inclusion of OH patients with higher peri-conception TSH levels and greater substitution need during pregnancy. In our long-term hypothyroid patients, as in the study by Li et al. (10), LT4 treatment was initiated at an earlier gestational age, demonstrating the lack of adaptation of these patients to the metabolic stress of the pregnancy.
We were not able to reproduce previous findings about the predictive value of TPOAb regarding long-term hypothyroidism (6, 7, 8). TAI impairs the thyroidal response to hCG (21) as a function of TPOAb and/or TgAb levels (22, 23), with a higher risk of hypothyroidism during and after pregnancy at higher antibody levels (23). Although TPOAb positivity was present in almost half of patients started on LT4 in our study, and this proportion was numerically higher in long-term hypothyroid patients, TPOAb was not associated with persistent hypothyroidism. This could be explained by the fact that most of our patients had TPOAb in the lowest tertiles. In two previous studies that showed an association between TPOAb and persistent hypothyroidism (6, 8), antibodies were measured at a more advanced gestational age than in our study (28 and 22 weeks vs 13 weeks), and the persistence of a significant TPOAb level at a late stage of pregnancy could indicate a more aggressive autoimmune phenotype with a higher impact on subsequent thyroid function.
This study also draws attention to the real-life management after LT4 initiation during pregnancy. Although the control of thyroid function is recommended 6 weeks after delivery (2, 3), almost one-third of our patients had no follow-up, compared to 16.5% in the study by Neelaveni et al. (7) and 45% in the study by Li et al. (8), and slightly more than half had long-term follow-up. In our study, being followed up by an endocrinologist seems to be of added value for the long-term management of these patients. As there were no differences in characteristics at LT4 initiation and during treatment between patients with or without follow-up, one might expect the same long-term evolution in the latter and misdiagnosis of persistent hypothyroidism in women susceptible to being pregnant again. However, a postpartum follow-up might not be necessary in some patients, for instance, in those with isolated hypothyroxinemia, given the low prevalence of persistent hypothyroidism in this group (8, 12). A normal thyroid function at 6 weeks post partum does not exclude the risk of long-term hypothyroidism, which can develop in 28% of patients followed for a median of 11 (7, 8, 9, 10, 11, 12, 13, 14, 15, 16, 17, 18, 19) months (8), especially when thyroid antibodies are positive. Consequently, as suggested by the 2014 ETA guidelines, the follow-up should be continued at least for 1 year after delivery.
Our study has several limitations related to its retrospective nature, which could increase the risk of selection and information bias. One-fifth of our pregnant patients on LT4 was excluded because there was not enough information about the reasons, timing, and importance of LT4 treatment. These patients might have had different clinical characteristics from those included. The group of patients included was small, and information on LT4 treatment management after delivery was not always available. We did not study the impact of TgAb on the occurrence of long-term hypothyroidism, as they were measured in only 55% of patients at LT4 instauration, nor the impact of iodine supplementation or ferritin levels as possible confounding factors for thyroid dysfunction during pregnancy. Also, there was not enough information about the occurrence of postpartum thyroiditis (PPT) in our population. Hypothyroidism can persist in up to 40% of women with PPT, especially those TPOAb positive (24), and we cannot rule out that PPT was the cause of LT4 restoration in some of our patients.
Based on our findings, LT4 treatment initiated during pregnancy could be reasonably discontinued in patients with TSH < 4.0 mU/L at diagnosis who received less than 68.75 µg/day LT4. We suggest continuing LT4 treatment in patients diagnosed with OH during pregnancy and in patients with SCH defined as a TSH > 4.0 mU/L during the first trimester of pregnancy, given the high prevalence of persistent hypothyroidism (8). The dose to be continued could be reduced by one-third to one-half of the maximal dose required during pregnancy, depending on the initial TSH elevation, and based on the increased requirement for thyroid hormones during pregnancy (25, 26). If the treatment was prescribed for isolated hypothyroxinemia, it should be discontinued after delivery. Thyroid function should be checked at 6 weeks post partum and until at least 1 year after delivery.
Conclusion
One-third of patients started on LT4 during pregnancy have long-term hypothyroidism, but this proportion could be overestimated by the unjustified continuation of treatment in some patients immediately after delivery. We observe deviations from current recommendations concerning the indications of LT4 initiation during pregnancy, the management of LT4 treatment after delivery, and the follow-up strategy. The TSH level at treatment initiation and the LT4 dose during pregnancy could guide the decision for continuing long-term LT4 treatment.
Declaration of interest
KGP received lecture fees from the IBSA Institut Biochimique SA, Berlin-Chemie AG and the Merck company between 2016 and 2022. From September 2023 on, he is the secretary of the European Thyroid Association (ETA). KGP is on the editorial board of European Thyroid Journal. KGP was not involved in the review or editorial process for this paper, on which he is listed as an author.
Funding
This work did not receive any specific grant from any funding agency in the public, commercial, or not-for-profit sector.
Statement of ethics
This study protocol was reviewed and approved by the local Ethics Committee (Comité d’Ethique Hospitalo-Facultaire des Cliniques Universitaires St-Luc, Université Catholique de Louvain, Brussels, Belgium). Written informed consent was not required due to the retrospective nature of the study.
Data availability statement
The data that support the findings of this study are not publicly available due to their containing information that could compromise the privacy of research participants but are available from MCB upon reasonable request.
Author contribution statement
MCB wrote the first draft. SD collected the clinical data and DM and SMC performed all statistical analyses. CD, RF, OA, DM, and FD cared for patients and KGP provided revisions for the manuscript. MCB and FD led the clinical study. All authors reviewed and approved the final manuscript.
References
- 1.Taylor PN & Lazarus JH. Hypothyroidism in pregnancy. Endocrinology and Metabolism Clinics of North America 201948547–556. ( 10.1016/j.ecl.2019.05.010) [DOI] [PubMed] [Google Scholar]
- 2.Lazarus J Brown RS Daumerie C Hubalewska-Dydelczyk A Negro R & Vaidya B. 2014 European thyroid association guidelines for the management of subclinical hypothyroidism in pregnancy and in children. European Thyroid Journal 2014376–94. ( 10.1159/000362597) [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Alexander EK, Pearce EN, Brent GA, Brown RS, Chen H, Dosiou C, Grobman WA, Laurberg P, Lazarus JH, Mandel SJ, et al.2017 Guidelines of the American Thyroid Association for the diagnosis and management of thyroid disease during pregnancy and postpartum. Thyroid 201727315–389. ( 10.1089/thy.2016.0457) [DOI] [PubMed] [Google Scholar]
- 4.Thangaratinam S Tan A Knox E Kilby MD Franklyn J & Coomarasamy A. Association between thyroid autoantibodies and miscarriage and preterm birth: meta-analysis of evidence. BMJ 2011342d2616. ( 10.1136/bmj.d2616) [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Poppe K Bisschop P Fugazzola L Minziori G Unuane D & Weghofer A. 2021 European Thyroid Association guideline on thyroid disorders prior to and during assisted reproduction. European Thyroid Journal 20219281–295. ( 10.1159/000512790) [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Shields BM Knight BA Hill AV Hattersley AT & Vaidya B. Five-year follow-up for women with subclinical hypothyroidism in pregnancy. Journal of Clinical Endocrinology and Metabolism 201398E1941–E1945. ( 10.1210/jc.2013-2768) [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Neelaveni K Kumar KVSH Sahay R & Ramesh J. Postpartum follow-up in women diagnosed with subclinical hypothyroidism during pregnancy. Indian Journal of Endocrinology and Metabolism 201721699–702. ( 10.4103/ijem.IJEM_452_16) [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Li N Yang J Chen X Huang J Lai M Fang F Gu L Wang YF & Peng YD. Postpartum follow-up of patients with subclinical hypothyroidism during pregnancy. Thyroid 2020301566–1573. ( 10.1089/thy.2019.0714) [DOI] [PubMed] [Google Scholar]
- 9.Van Leeuw V & Leroy Ch. Santé périnatale en Région bruxelloise – Année 2021. Centre d’Epidémiologie Périnatale. 2022. Disponible sur: rapport_CEPIP_Bxl_2022-fr.pdf. Accessed on January 27, 2024. [Google Scholar]
- 10.Linardi A Kakoulidis I Ilias I Michou A Pappa A Venaki E & Koukkou E. Postpartum follow-up of women who developed subclinical hypothyroidism during pregnancy. Medical Sciences 2020829. ( 10.3390/medsci8030029) [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Haddow JE, Palomaki GE, Allan WC, Williams JR, Knight GJ, Gagnon J, O’Heir CE, Mitchell ML, Hermos RJ, Waisbren SE, et al.Maternal thyroid deficiency during pregnancy and subsequent neuropsychological development of the child. New England Journal of Medicine 1999341549–555. ( 10.1056/NEJM199908193410801) [DOI] [PubMed] [Google Scholar]
- 12.Stagnaro-Green A. Postpartum management of women begun on levothyroxine during pregnancy. Frontiers in Endocrinology 20156183. ( 10.3389/fendo.2015.00183) [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Sun X Hou N Wang H Ma L Sun J & Liu Y. A meta-analysis of pregnancy outcomes with levothyroxine treatment in euthyroid women with thyroid autoimmunity. Journal of Clinical Endocrinology and Metabolism 2020105dgz217. ( 10.1210/clinem/dgz217) [DOI] [PubMed] [Google Scholar]
- 14.van Dijk MM, Vissenberg R, Fliers E, van der Post JAM, van der Hoorn MP, de Weerd S, Kuchenbecker WK, Hoek A, Sikkema JM, Verhoeve HR, et al.Levothyroxine in euthyroid thyroid peroxidase antibody positive women with recurrent pregnancy loss (T4LIFE trial): a multicentre, randomised, double-blind, placebo-controlled, phase 3 trial. Lancet. Diabetes and Endocrinology 202210322–329. ( 10.1016/S2213-8587(2200045-6) [DOI] [PubMed] [Google Scholar]
- 15.Furnica RM Gruson D Lazarus JH Maiter D Bernard P & Daumerie C. First trimester isolated maternal hypothyroxinaemia: adverse maternal metabolic profile and impact on the obstetrical outcome. Clinical Endocrinology 201786576–583. ( 10.1111/cen.13301) [DOI] [PubMed] [Google Scholar]
- 16.Han Y Gao X Wang X Zhang C Gong B Peng B Li J Liu A & Shan Z. A systematic review and meta-analysis examining the risk of adverse pregnancy and neonatal outcomes in women with isolated hypothyroxinemia in pregnancy. Thyroid 202333603–614. ( 10.1089/thy.2022.0600) [DOI] [PubMed] [Google Scholar]
- 17.Thompson W Russell G Baragwanath G Matthews J Vaidya B & Thompson-Coon J. Maternal thyroid hormone insufficiency during pregnancy and risk of neurodevelopmental disorders in offspring: a systematic review and meta-analysis. Clinical Endocrinology 201888575–584. ( 10.1111/cen.13550) [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Maraka S Ospina NM O’Keeffe DT Espinosa De Ycaza AE Gionfriddo MR Erwin PJ Coddington CC 3rd Stan MN Murad MH & Montori VM. Subclinical hypothyroidism in pregnancy a systematic review and meta-analysis. Thyroid 201626580–590. ( 10.1089/thy.2015.0418) [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Consortium on Thyroid and Pregnancy—Study Group on Preterm Birth—Study Group on Preterm Birth, Korevaar TIM, Derakhshan A, Taylor PN, Meima M, Chen L, Bliddal S, Carty DM, Meems M, Vaidya B, et al.Association of Thyroid Function Test Abnormalities and Thyroid Autoimmunity with Preterm Birth: a systematic review and meta-analysis. JAMA 2019322632–641. ( 10.1001/jama.2019.10931) [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Toloza FJK, Derakhshan A, Männistö T, Bliddal S, Popova PV, Carty DM, Chen L, Taylor P, Mosso L, Oken E, et al.Association between maternal thyroid function and risk of gestational hypertension and pre-eclampsia: a systematic review and individual-participant data meta-analysis. Lancet. Diabetes and Endocrinology 202210243–252. ( 10.1016/S2213-8587(2200007-9) [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Korevaar TI, Steegers EA, Pop VJ, Broeren MA, Chaker L, de Rijke YB, Jaddoe VW, Medici M, Visser TJ, Tiemeier H, et al.Thyroid autoimmunity impairs the thyroidal response to human chorionic gonadotropin: two population-based prospective cohort studies. Journal of Clinical Endocrinology and Metabolism 201710269–77. ( 10.1210/jc.2016-2942) [DOI] [PubMed] [Google Scholar]
- 22.Hou Y, Liu A, Li J, Wang H, Yang Y, Li Y, Fan C, Zhang H, Wang H, Ding S, et al.Different thyroidal responses to human chorionic gonadotropin under different thyroid peroxidase antibody and/or thyroglobulin antibody positivity conditions during the first half of pregnancy. Thyroid 201929577–585. ( 10.1089/thy.2018.0097) [DOI] [PubMed] [Google Scholar]
- 23.Andersen SL, Bruun NH, Christensen PA, Lykkeboe S, Handberg A, Hansen AB, Lundgaard MH, Knøsgaard L, Uldall Torp NM, Carlé A, et al.Cut-offs for thyroid peroxidase and thyroglobulin antibodies in early pregnancy. European Thyroid Journal 202211e220142. ( 10.1530/ETJ-22-0142) [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.Stuckey BG Kent GN Ward LC Brown SJ & Walsh JP. Postpartum thyroid dysfunction and the long-term risk of hypothyroidism: results from a 12-year follow-up study of women with and without postpartum thyroid dysfunction. Clinical Endocrinology 201073389–395. ( 10.1111/j.1365-2265.2010.03797.x) [DOI] [PubMed] [Google Scholar]
- 25.Yassa L Marqusee E Fawcett R & Alexander EK. Thyroid hormone early adjustment in pregnancy (the THERAPY) trial. Journal of Clinical Endocrinology and Metabolism 2010953234–3241. ( 10.1210/jc.2010-0013) [DOI] [PubMed] [Google Scholar]
- 26.Mandel SJ Larsen PR Seely EW & Brent GA. Increased need for thyroxine during pregnancy in women with primary hypothyroidism. New England Journal of Medicine 199032391–96. ( 10.1056/NEJM199007123230204) [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Data Availability Statement
The data that support the findings of this study are not publicly available due to their containing information that could compromise the privacy of research participants but are available from MCB upon reasonable request.