

ABSTRACT
BACKGROUND:
The COVID-19 pandemic led to approximately half of the working population in the United Kingdom being unable to work temporarily. This study aims to understand the employment needs and experiences of people with multiple sclerosis (MS) in the UK during this period.
METHODS:
Multiple methods were used, including an online survey and follow-up interviews with people with MS who were employed prior to the start of the pandemic restrictions in March 2020.
RESULTS:
The online survey was completed by 101 eligible participants and we interviewed 15 of them for qualitative data in the follow-up. Survey data indicated that the work experience of people with MS improved during the pandemic because they were allowed to work from home. However, participants experienced increased feelings of anxiety and loneliness. From the interviews, we extracted 5 themes: (1) the benefits of working from home; (2) the challenges of working during the COVID-19 pandemic; (3) the relevance of managers; (4) returning to “normal”; and (5) the need for vocational support.
CONCLUSIONS:
The pandemic showed that MS symptom management was improved by work flexibility (eg, working from home, breaks, flexible working hours); for people with MS, these accommodations improved both their ability to work and their self-perceived productivity. Future research should explore the support needs of people with MS who work remotely and determine whether pandemic-influenced work accommodations are sustainable over time.
Keywords: Covid-19, employment, vocational rehabilitation, survey, United Kingdom
Throughout the world in March 2020, in the initial stages of the COVID-19 pandemic, social distancing rules were established to reduce the spread of the virus. Lockdowns prevented people from leaving their homes unless strictly necessary (eg, to buy food). In the United Kingdom, these changes resulted in approximately half the working population being unable to work.1 Only certain categories of workers, such as health care workers (known as key workers), were permitted to travel to work. To avoid enormous job loss, the UK government created a job retention scheme (known as furlough).2 Throughout the pandemic, this plan supported 11.6 million people on temporary leave (furlough) and almost 1.3 million businesses.3 From March 2020, a group of approximately 1.8 million people who were considered at high risk for complications from the virus were advised by chief medical officers across the UK to shield themselves for 12 weeks.4 This group included people with a weak immune system, such as people with multiple sclerosis (MS), who were on high-efficacy or immunosuppressive disease-modifying treatment.
With offices forced to close, the pandemic had a substantial impact on the labor market. People with disabilities were 1.5 times more likely to be unemployed when compared with people without disabilities.5 Additionally, 71% of workers with disabilities reported losing income, being furloughed, or being made redundant.5
Simultaneously, the social and environmental changes that arose because of the pandemic, such as working from home, may have led to unintended benefits, such as improved flexibility for workers with disabilities.6 To date, there is no evidence of the impact of the COVID-19 pandemic on the employment of people with MS in the UK. Understanding their experiences can provide insight into the future vocational rehabilitation (VR) needs of this group of workers. The British Society for Rehabilitation Medicine (BSRM) defines VR as “a process whereby those disadvantaged by illness or disability can be enabled to access, maintain or return to employment or other useful occupation.”7
This study aims to explore the employment needs and experiences of people with MS in the UK during the COVID-19 pandemic.
METHODS
Participants
A survey aimed at people with MS was distributed through social media, blog posts written by the authors, local networks, and newsletters for people with MS. The survey was also advertised in the neurology clinics of 4 major hospitals in the UK (Nottingham, Leeds, London, and Cardiff). People with MS with appointments at these hospitals were informed about the study either during their appointment (conducted remotely because of the COVID- 19 pandemic) or were contacted by a member of their health care team about the study.
People were included in the study if they were between 18 and 65 years of age, diagnosed with MS, in paid employment before March 2020, able to consent and communicate in English, and living in the UK.
Study Design
This was a multiple-methods study with an online survey followed by individual interviews. The online package consisted of a participant information sheet, a consent form, and the data collection instrument.
The survey had 1 open question to explore the unintended benefits of working during the COVID-19 pandemic and 28 closed questions regarding participants’ clinical characteristics (eg, type of MS), demographics (eg, age, gender), employment situation (eg, organization size), impact of COVID-19 (eg, shielding, financial impact), employment support received before and after the pandemic (eg, working from home, flexible working schedule), main challenges with working during COVID-19, confidence and ability to work during the pandemic, and future VR needs (eg, legal knowledge, fatigue management).
Instead of using several standardized questionnaires with multiple items, a questionnaire was developed to reduce participants’ burden and to capture a wide range of experiences arising from the frequent changes in the legislation and working patterns that happened during the pandemic.
Upon completion of the survey, participants were asked to provide their contact details if they wished to complete a follow-up interview. To select interviewees from those interested, we used purposive sampling based on known predictors of unemployment for people with MS (eg, physical disability, age, education).8–11 Selected candidates were contacted via email to participate in an interview via Microsoft Teams. Participants completed an interview-specific consent form before the interview.
The development of the survey and interview topic guide was underpinned by the International Classification of Functioning Disability and Health (ICF)12 and the Behavior Change Wheel (BCW).13 These were selected because they have proven to be effective in research mapping the employment needs of people with MS.14 Research documents were reviewed by a patient and public involvement adviser with MS. Examples of questions from the survey and interview topic guide are presented in TABLE S1.
Data Analysis
Questions regarding demographic, clinical, and employment characteristics and future VR needs were summarized using descriptive statistics. Questions exploring support received before and during the pandemic were analyzed using the McNemar test, suitable for analysis of paired dichotomous data.
Data concerning the main challenges of working during the pandemic were analyzed by performing a series of univariate logistic regression analyses to explore relationships between respondents’ clinical, demographic, and employment characteristics based on the likelihood that respondents would report challenges working during COVID-19. Likert scale data were analyzed using descriptive statistics and we computed the associated CIs around the proportions; we selected each answer using binomial exact. Data were handled using IBM SPSS Statistics and Stata (StataCorp). An open-ended question exploring the unintended benefits of working during COVID-19 was analyzed using content analysis.15 Interviews, conducted by a research assistant (CP) with a background in health psychology, were audio-recorded and transcribed verbatim. Data were handled using NVivo version 12.16 Data were analyzed by 2 researchers (CP, BDP) using Framework Analysis17,18 and informed by the ICF and BCW. The main findings and themes from the interviews were discussed with the wider research team. We used Yardley’s framework to maintain the quality of the data collected and analyzed.19
Ethics Approval
Ethics approval was obtained from the Bradford Leeds Research Ethics Committee (20/YH/0312).
RESULTS
One hundred and four participants completed the survey. Three participants were excluded because they did not meet the inclusion criteria (eg, unemployed before the pandemic). Therefore, we analyzed data from 101 participants, and 15 completed the follow-up interview. Interviews lasted 30 to 60 minutes.
Sample Description
TABLE 1 presents the participants’ demographic characteristics. Survey participants were, on average, 45.2 (SD 10.3) years of age and had been living with MS for, on average, 8.7 (SD 7.8) years. Interview participants were, on average, 47.1 (SD 9.3) years of age and had been living with MS for an average of 10.9 (SD 10.4) years.
Table 1.
Participant Characteristics
| Survey (N =101) | Interviews (n =15) | |
|---|---|---|
| Sex | ||
| Female | 79 (78.2%) | 9 (60.0%) |
| Male | 22 (21.4%) | 6 (40.0%) |
| Ethnicity | n = 100 | |
| White British | 97 (97.0%) | 14 (93.3%) |
| Black/African/Caribbean/Black British | 1 (1.0%) | 0 |
| Asian/Asian British | 2 (2.0%) | 1 (6.6%) |
| Living arrangements | ||
| Living alone | 15 (14.9%) | 3 (20.0%) |
| Living with partner | 46 (45.5%) | 4 (26.6%) |
| Living with family | 39 (38.6%) | 8 (53.3%) |
| Living with friends | 1 (1.0%) | 0 |
| Education | ||
| GCSE | 5 (4.9%) | 1 (6.6%) |
| Collegea | 13 (12.9%) | 4 (26.6%) |
| Degree | 34 (33.7%) | 4 (26.6%) |
| Postgraduate | 45 (44.5%) | 6 (40.0%) |
| Other | 4 (3.9%) | 0 |
| MS characteristics | n = 100 | |
| Relapsing-remitting MS | 86 (86.0%) | 10 (66.6%) |
| Secondary progressive MS | 8 (8.0%) | 4 (26.6%) |
| Primary progressive MS | 5 (5.0%) | 1 (6.6%) |
| Not known | 1 (1.0%) | 0 |
| EDSS | n = 44 | n = 10 |
| 0-3 | 21 (47.9%) | 3 (30.0%) |
| 3.5-6.0 | 16 (36.9%) | 2 (20.0%) |
| 6.5-9.0 | 7 (15.2%) | 5 (50.0%) |
| Employment characteristics (multiple choice) | ||
| Employed full time | 58 (57.4%) | 7 (46.6%) |
| Employed part time | 33 (32.6%) | 5 (33.3%) |
| Self-employed full time | 4 (3.9%) | 1 (6.6%) |
| Self-employed part time | 4 (3.9%) | 1 (6.6%) |
| Student | 3 (2.9%) | 1 (6.6%) |
| Working and job hunting | 2 (1.9%) | 0 |
| Medically retired | 1 (0.9%) | 0 |
| Doing volunteer work | 1 (0.9%) | 0 |
| Size of employer b | ||
| Large (>250 employees) | 62 (61.4%) | 6 (40.0%) |
| Medium (50-249) | 20 (19.8%) | 6 (40.0%) |
| Small (10-49) | 11 (10.9%) | 1 (6.6%) |
| Micro (>9) | 8 (7.9%) | 2 (13.3%) |
| Main job typec | n = 97 | n = 15 |
| Survey (N = 101) | Interviews (n = 15) | |
| Main job typec | n = 97 | n = 15 |
| Level 4 (professional and managerial) |
48 (49.5%) | 7 (46.6%) |
| Level 3 (associated professional and technical/skilled trade) |
27 (27.8%) | 5 (33.3%) |
| Level 2 (administrative, caring, leisure, sales, customer service, process, plant, and machinery operatives) |
19 (19.6%) | 1 (6.6%) |
| Level 1 (elementary occupation) |
3 (3.1%) | 2 (13.3%) |
| Disclosed MS diagnosis to employer | ||
| Yes | 89 (88.1%) | 14 (93.3%) |
| No | 7 (6.9%) | 0 |
| Not applicable | 5 (5.0%) | 1 (6.7%) |
EDSS, Expanded Disability Status Scale; GCSE, General Certificate of Secondary Education; MS, multiple sclerosis.
College refers to a 2-year program to prepare students for university entrance exams. Thus, degree refers to a bachelor’s degree.
Organization size obtained from UK government guidelines.
Office for National Statistics. SOC 2020. Updated January 19, 2023. https://www.ons.gov.uk/methodology/classificationsandstandards/standardoccupationalclassificationsoc/soc2020
Only 31.7% of participants received a recommendation from the UK government or a health care professional to shield during the first national lockdown; however, 43.6% of participants chose to shield themselves for most of the pandemic.
Most participants (70.0%) did not receive state benefit payments. For those who received benefits, the most common was the personal independence payment (28.0%), a welfare benefit to help working adults. Regarding the economic impact of the pandemic, roughly half of the participants reported no impact or a positive impact, 17.8% of participants reported a short-term negative impact, and 7.9% reported a long-lasting negative impact.
Respondents reported a diverse range of employment arrangements during the pandemic. The most common was working from home (67.3%), followed by going to the usual place of work (15.8%). Up to 37.6% reported being identified as key workers.
Participants who were unable to work were furloughed because they were shielding (3.0%), were furloughed for other reasons (ie, the company stopped trading; 5.0%), were made redundant (4.0%), or were self-employed but unable to work (2.0%).
Survey Results
TABLE S2A shows the support and work accommodations participants received before and during the pandemic. Only the proportion of people allowed to work from home differs significantly between the 2 time periods. More people were permitted to work from home during the pandemic than before (P <.001). Some items were excluded from the analysis because they did not reach a minimum of 10 discordant pairs (TABLE S2B).
Table S2:
Support Received Before and During COVID-19
| A. Included in analysis | ||||||
|---|---|---|---|---|---|---|
| Before the COVID-19 pandemic, did your employer implement any modifications in your work schedule, duties, or environment to accommodateyour multiple sclerosis? | ||||||
| n | “Yes” before pandemic, n (%) | “Yes” during pandemic, n (%) | Discordant pairs* | P | ||
| From no to yes | From yes to no | |||||
| I was allowed to work from home. | 64 | 20 (31.25%) | 44 (68.75%) | 30 | 8 | .001 |
| I was provided with equipment such as a work laptop, walking aid, special chair, etc. | 28 | 16 (57.14%) | 12 (42.86%) | 6 | 10 | .45 |
| I was allowed to work flexible hours or allowed to take more breaks. | 39 | 21 (53.84%) | 18 (46.16%) | 7 | 10 | .62 |
| I reduced my working hours or responsibilities | 18 | 12 (66.67%) | 6 (33.33%) | 4 | 10 | .18 |
| I did not need support at work. | 40 | 23 (57.5%) | 17 (42.5%) | 15 | 9 | 30 |
| I did not receive reasonable adjustments (eg, changes in my work arrangements or duties to manage my multiple sclerosis). | 78 | 43 (55.12%) | 35 (44.87%) | 18 | 10 | .18 |
Discordant pairs refer to participants who (1) were not receiving this support before the pandemic but started receiving the support during the pandemic (from no to yes), or (2) were receiving support before the pandemic but stopped receiving that support during the pandemic (from yes to no).
| B. Excluded from analysis | |||||
|---|---|---|---|---|---|
| Area of support | n | Before, n (%) | During, n (%) | From no to yes | From yes to no |
| I have requested additional support, but it was declined. | 9 | 7 (77.78%) | 2 (22.22%) | 5 | 0 |
| I was provided with assistive technology (eg, text-to-speech software, digital recorders) | 3 | 2 (66.67%) | 1 (33.33%) | 1 | 2 |
| I was provided with more supervision or support. | 6 | 4 (66.67%) | 2 (33.33%) | 1 | 2 |
| I moved to a different role within the organization. | 8 | 6 (75%) | 2 (25%) | 2 | 6 |
| I received physical adaptations in my work environment or equipment to enable me to work from home. | 3 | 1 (33.33%) | 2 (66.67%) | 2 | 1 |
| I applied for outside help (eg, government programs) and was successful | 3 | 1 (33.33%) | 2 (66.67%) | 2 | 1 |
| I applied for outside help (eg, government programs) and was not successful | 0 | 0 | 0 | - | - |
From no to yes: participants who were not receiving this support before the pandemic but started receiving the support during the pandemic.
From yes to no: participants who were receiving support before the pandemic but stopped receiving that support during the pandemic.
Note: The items presented in Table S2 represent those that could not be included in the McNemar test because there were fewer than 10 discordant pairs.
Confidence and Ability to Work During COVID-19
Participants reported feeling less confident about meeting clients/colleagues in person, and more confident about using technology at work (eg, having meetings remotely). Although some participants reported a reduced ability to concentrate at work (40.4%) and to manage fatigue (39.6%), for most, self-reported ability to work did not change (TABLE S3).
Table S3:
Self-Reported Confidence Levels and Ability to Work During COVID-19
| Less confident than beforen(%, 95% CI) | No change n(%, 95% CI) | More confident than beforen(%, 95% CI) | Total | |
|---|---|---|---|---|
| Going to work (if working outside of home) | 40(47.6%, 0.36-0.58) | 39(46.4%, 0.35-0.57) | 5(5.9%, 0.02-0.13) | 84 |
| Attend your usual workplace after the lockdown | 43(47.5%, 0.36-0.57) | 40(44.0%, 0.33-0.54) | 8(8.8%, 0.03-0.16) | 91 |
| Meeting in person with clients or customers | 55(61.1%, 0.50-0.71) | 29(32.2%, 0.22-0.42) | 6(6.66%, 0.02-0.13) | 90 |
| Having meetings via telephone or online platforms | 8(8.1%, 0.03-0.15) | 28(28.3%, 0.19-0.38) | 63(63.6%, 0.53-0.73) | 99 |
| Requesting support from your employer | 14(14.9%, 0.08-0.23) | 59(62.8%, 0.52-0.72) | 21(22.3%, 0.14-0.32) | 94 |
| Following social-distancing rules at work | 28(30.1%, 0.21-0.40) | 39(41.9%, 0.31-0.52) | 26(27.9%, 0.19-0.38) | 93 |
| Finding a new job | 43(48.3%, 0.35-0.56) | 41(46.1%, 0.35-0.56) | 5(5.61%, 0.01-0.12) | 89 |
| Worse than beforen(%, 95% CI) | No change n(%, 95% CI) | Better than before n(%, 95% CI) | Total | |
|---|---|---|---|---|
| Ability to concentrate when working | 40(40.4%, 0.30-0.50) | 46(46.5%, 0.36-0.56) | 13(13.1%, 0.07-0.21) | 99 |
| Ability to work outside the usual place of work (eg, home) | 22(22.4%, 0.14-0.31) | 44(44.9%, 0.34-0.55) | 32(32.6%, 0.23-0.42) | 98 |
| Ability to work in the usual place of work (eg, outside home) | 29(32.6%, 0.23-0.43) | 50(56.2%, 0.45-0.66) | 10(11.2%, 0.05-0.19) | 89 |
| Ability to take transport to and from work | 17(20.0%, 0.12-0.30) | 65(76.5%, 0.66-0.84) | 3(3.5%,0.007-0.09) | 85 |
| Having access to the internet | 11(11.5%, 0.05-0.19) | 80(83.3%, 0.74-0.90) | 5(5.2%, 0.01-0.11) | 96 |
| Ability to managing work and home responsibilities | 26(26.8%, 0.18-0.36) | 58(59.8%, 0.43-0.69) | 13(13.4%, 0.07-0.21) | 97 |
| Support received from the employer | 17(18.3%, 0.11-0.27) | 55(59.1%, 0.48-0.69) | 21(22.6%, 0.14-0.32) | 93 |
| Ability to manage fatigue | 38(39.6%, 0.29-0.50) | 43(44.8%, 0.34-0.55) | 15(15.6%, 0.09-0.24) | 96 |
| Ability to manage difficulties walking or moving around | 20(21.0%, 0.13-0.30) | 69(72.7%, 0.62-0.81) | 6(6.3%, 0.02-0.13) | 95 |
| Presence of health problems other than multiple sclerosis | 21(21.6%, 0.13-0.31) | 74(76.3%, 0.66-0.84) | 2(2.1%, 0.002-0.07) | 97 |
Unintended Benefits
The unintended benefits of working during the pandemic were low in this cohort (TABLE S4). Participants cited reduced travel (19.8%), including traveling without much traffic, as the most important unintended benefit, followed by being allowed to work from home (12.8%).
Table S4:
Unintended Benefits of Working During COVID-19
| n (%) | |
|---|---|
| Reduced travel | 20 (19.8%) |
| Working from home | 13 (12.8%) |
| Better work-life balance | 8 (7.9%) |
| Reduced fatigue | 8 (7.9%) |
| Employer/colleagues understand benefits of working from home | 8 (7.9%) |
| Increased productivity/concentration | 6 (5.9%) |
| Flexible working | 6 (5.9%) |
| Reduced anxiety | 4 (3.9%) |
| Learning new skills | 3 (2.9%) |
| More time with family | 2 (1.9%) |
| Reevaluate life values | 2 (1.9%) |
| Save money | 1 (0.9%) |
Note: Multiple answers were allowed; percentage is of respondents who selected each answer option (eg, 100% would represent that all respondents to the question chose that option).
Future VR Needs
Although 45% of the participants reported no VR needs (FIGURE S1), a sizable proportion identified the need for help with managing anxiety and/or depression (30%), managing MS symptoms (25%), and managing employers’ expectations (19%).
FIGURE S1.
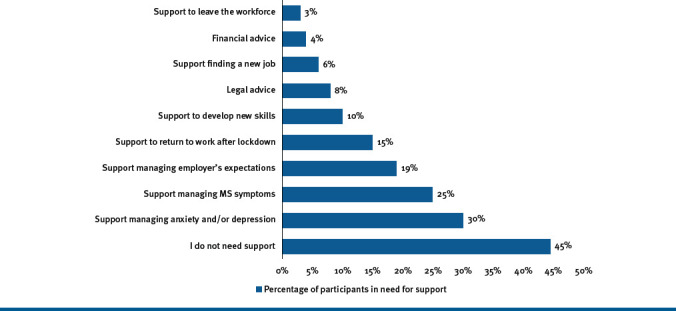
Future Vocational Needs for Individuals With Multiple Sclerosis (MS)
Challenges Working During COVID-19
Being female (OR, 4.27; 95% CI, 1.44-12.73) and working in the public sector (OR, 10; 95% CI, 1.08-92.5) were associated with an increased likelihood of reported anxiety or stress during the pandemic. More self-reported MS symptoms (OR, 1.31; 95% CI, 1.05-1.64) were associated with an increased likelihood of a reported lack of support from managers or colleagues. A higher level of education was associated with an increased likelihood of reporting changes to workload (OR, 1.78; 95% CI, 1.05-3.03), as well as a trend suggesting a decrease in being rendered unable to work due to shielding (OR, 0.33; 95% CI, 0.12-0.99) (TABLE S5).
Table S5:
Challenge Predictors
| A. Predictors of respondents reporting anxiety or stress | |||||
|---|---|---|---|---|---|
| 95% CI | |||||
| Variable | B (SE) | P value | OR | Lower | Upper |
| Demographic | |||||
| Sex: female | 1.45 (0.56) | .01* | 4.27 | 1.44 | 12.73 |
| Age | -0.04 (0.02) | .1 | 0.97 | 0.93 | 1.01 |
| Education | 0.09 (0.23) | .69 | 1.1 | 0.7 | 1.72 |
| Clinical | |||||
| Type of MS | 1.3 (0.69) | .06 | 3.66 | 0.94 | 14.22 |
| Years with MS | -0.01 (0.26) | .69 | 0.99 | 0.94 | 1.04 |
| Number of symptoms | 0.03 (0.07) | .72 | 1.03 | 0.89 | 1.18 |
| Employment-related | |||||
| Size of employer | 0.18 (0.21) | .41 | 1.19 | 0.79 | 1.8 |
| Organizational | |||||
| Self-employment | -1.61 (1.12) | .15 | 0.2 | 0.02 | 1.78 |
| Private | 0.96 (1.15) | .41 | 2.6 | 0.27 | 24.65 |
| Public | 2.3 (1.14) | .04* | 10 | 1.08 | 92.5 |
| Disclosure to employer (yes) | 0.53 (0.76) | .48 | 1.71 | 0.38 | 7.57 |
| B. Predictors of respondents reporting lack of adequate workspace | |||||
|---|---|---|---|---|---|
| 95% CI | |||||
| Variable | B (SE) | P value | OR | Lower | Upper |
| Demographic | |||||
| Sex: female | 0.48 (0.68) | .49 | 1.61 | 0.42 | 6.12 |
| Age | 0.02 (0.03) | .4 | 1.02 | 0.97 | 1.08 |
| Education | 0.53 (0.35) | .12 | 1.71 | 0.87 | 3.35 |
| Clinical | |||||
| Type of MS | 0.23 (0.82) | .78 | 1.26 | 0.25 | 6.24 |
| Years with MS | -0.01 (0.03) | .71 | 0.99 | 0.92 | 1.06 |
| Number of symptoms | 0.15 (0.1) | .12 | 1.16 | 0.96 | 1.4 |
| Employment-related | |||||
| Size of employer | 0.47 (0.34) | .16 | 1.61 | 0.83 | 3.12 |
| Organizational | |||||
| Self-employment | -0.17 (1.13) | .66 | 0.84 | 0.09 | 7.68 |
| Private | -0.28 (1.2) | .82 | 0.76 | 0.07 | 7.9 |
| Public | 0.43 (1.14) | .71 | 1.54 | 0.16 | 14.49 |
| Voluntary | 0.51 (1.59) | .75 | 1.67 | 0.07 | 37.73 |
| Disclosure to employer (yes) | -19.83 (14210.36) | >.99 | 0 | 0 | - |
| C. Predictors of respondents reporting fear of going to their normal workplace | |||||
|---|---|---|---|---|---|
| 95% CI | |||||
| Variable | B (SE) | P value | OR | Lower | Upper |
| Demographic | |||||
| Sex: female | 0.85 (0.6) | .16 | 2.34 | 0.72 | 7.6 |
| Age | 0.01 (0.02) | .73 | 1.01 | 0.97 | 1.05 |
| Education | -0.23 (0.24) | .35 | 0.8 | 0.5 | 1.28 |
| Clinical | |||||
| Type of MS | 0.42 (0.7) | .55 | 1.53 | 0.39 | 5.99 |
| Years with MS | -0.003 (0.03) | .93 | 1 | 0.94 | 1.05 |
| Number of symptoms | 0.03 (0.08) | .72 | 1.03 | 0.88 | 1.2 |
| Employment-related | |||||
| Size of employer | 0.34 (0.26) | .17 | 1.42 | 0.86 | 2.35 |
| Organizational | |||||
| Self-employment | -0.8 (1.12) | .88 | 0.45 | 0.05 | 4.01 |
| Private | 0.84 (1.15) | .47 | 2.31 | 0.24 | 21.97 |
| Public | 0.92 (1.14) | .42 | 2.5 | 0.27 | 23.12 |
| Disclosure to employer (yes) | 0.32 (0.85) | .71 | 1.38 | 0.26 | 7.25 |
| D. Predictors of respondents reporting loneliness | |||||
|---|---|---|---|---|---|
| 95% CI | |||||
| Variable | B (SE) | P value | OR | Lower | Upper |
| Demographic | |||||
| Sex: female | 0.33 (0.53) | .54 | 1.39 | 0.49 | 3.95 |
| Age | -0.01 (0.02) | .59 | 0.99 | 0.95 | 1.03 |
| Education | 0.3 (0.26) | .25 | 1.34 | 0.81 | 2.22 |
| Clinical | |||||
| Type of MS | 1.13 (0.8) | .16 | 3.1 | 0.65 | 14.9 |
| Years with MS | -0.03 (0.03) | .34 | 0.97 | 0.92 | 1.03 |
| Number of symptoms | 0.03 (0.08) | .72 | 1.03 | 0.88 | 1.2 |
| Employment-related | |||||
| Size of employer | 0.3 (0.24) | .22 | 1.34 | 0.84 | 2.16 |
| Organizational | |||||
| Self-employment | -0.17 (1.13) | .66 | 0.84 | 0.09 | 7.68 |
| Private | -0.28 (1.2) | .82 | 0.76 | 0.07 | 7.9 |
| Public | 0.43 (1.14) | .71 | 1.54 | 0.16 | 14.49 |
| Disclosure to employer (yes) | -19.83 (14210.36) | >.99 | 0 | 0 | - |
| E. Predictors of respondents reporting changes in their workload | |||||
|---|---|---|---|---|---|
| 95% CI | |||||
| Variable | B (SE) | P value | OR | Lower | Upper |
| Demographic | |||||
| Sex: female | -0.04 (0.5) | .94 | 0.96 | 0.36 | 2.57 |
| Age | -0.02 (0.02) | .48 | 0.99 | 0.95 | 1.03 |
| Education | 0.58 (0.27) | .03* | 1.78 | 1.05 | 3.03 |
| Clinical | |||||
| Type of MS | 0.19 (0.64) | .77 | 1.21 | 0.34 | 4.24 |
| Years with MS | -0.004 (0.03) | .88 | 1 | 0.94 | 1.05 |
| Number of symptoms | -0.07 (0.08) | .36 | 0.93 | 0.8 | 1.08 |
| Employment-related | |||||
| Size of employer | 0.33 (0.24) | .16 | 1.4 | 0.87 | 2.23 |
| Organizational | |||||
| Self-employment | -1.09 (1.12) | .62 | 0.34 | 0.04 | 3 |
| Private | 0.84 (1.15) | .47 | 2.31 | 0.24 | 21.97 |
| Public | 1.17 (1.13) | .35 | 3.23 | 0.35 | 29.68 |
| Voluntary | 1.61 (1.48) | .28 | 5 | 0.27 | 91.52 |
| Disclosure to employer (yes) | 1.47 (1.09) | .18 | 4.33 | 0.51 | 36.72 |
| F. Predictors of respondents reporting not being able to work due to shielding | |||||
|---|---|---|---|---|---|
| 95% CI | |||||
| Variable | B (SE) | P value | OR | Lower | Upper |
| Demographic | |||||
| Sex: female | -0.19 (1.18) | .87 | 0.83 | 0.08 | 8.39 |
| Age | 0.04 (2.58) | .4 | 1.05 | 0.94 | 1.16 |
| Education | -1.07 (0.54) | .05* | 0.33 | 0.12 | 0.99 |
| Clinical | |||||
| Type of MS | -0.84 (1.2) | .49 | 0.43 | 0.04 | 4.52 |
| Years with MS | -0.02 (0.07) | .8 | 0.98 | 0.85 | 1.13 |
| Number of symptoms | 0.22 (0.2) | .28 | 1.24 | 0.84 | 1.84 |
| Employment-related | |||||
| Size of employer | -0.33 (0.46) | .47 | 0.72 | 0.29 | 1.76 |
MS, multiple sclerosis.
Indicates statistical significance.
Interview Findings
We identified 5 themes in the interviews that could be subdivided into 9 themes. TABLE 2 summarizes and quantifies the data explained below and presents illustrative quotes from the interviewees.
Table 2.
Themes From Interviews and Illustrative Quotes
| Benefits of working from home | Fewer distractions (n =12) | “I’m more productive working on my own becausethere’s no distraction….There are some really noisy people who sit near me in the office, and I find it really distracting like when I’m on a call [and] I can’t hear my client.” |
| Not having to travel to work (n =10) | “The lockdown made it easier for me because I didn’t have to spend time going to work. My productivity increased dramatically as a result of lockdown because I didn’t need to go and get from my wheelchair into my car and go into the university.” | |
| Challenges working during COVID-19 | Lack of support (n =8) | “I first went back in June last year; I was very anxious, because of not being allowed to wear a face covering and getting close to these children. I was extremely anxious.” |
| Barriers to receiving reasonable adjustments (n =6) | “One of the things that I feel we battle with is…there are a lot of people with MS who know perfectly well the specific things that they would need to make them more productive. But there are some hardliners out there who are not willing to consider that. They just do not believe in it.” | |
| Relevance of manager | Supportive manager (n = 6) | “My manager and the administration manager…were quite happy to let me work from home. Even this year I was waiting until I was fully vaccinated before they wanted to integrate me back into the school.” |
| Disengagement of manager (n =3) | “I’d been off for 5 months. They didn’t keep me up to speed with what was happening….My manager was lacking contact [with] me, so it was only through some of my colleagues that I found out what was going on.” | |
| Returning to normal | Continuation of working from home (n =6) | “I’ve just changed my contract to work permanentlyfrom home. I hadn’t considered it, or I hadn’t thought about it before.” |
| Concerns about returning to the office (n =5) | “I have some anxiety about the vulnerability to infection because it is an enclosed space, it is recirculating air, and I am conscious that the medication I’m on for my MS will reduce the effectiveness of the vaccines.” | |
| Vocational needs | (n =7) | “I phoned up [human resources] and asked for advice and they said, ‘Well, go and do some exercise,’ and I said, ‘I can’t. I need you to actually take my circumstances into account.’” |
MS, multiple sclerosis.
Note: The number below the subthemes reflects the number of interviewees contributing to each.
Theme 1: Benefits of working from home
At some point during the pandemic, 12 interviewees worked from home. In contrast to the survey results, interviewees reported fewer distractions while working from home. Prior to COVID-19, many participants had worked in loud, open-plan offices that hampered their ability to concentrate. The reduced noise levels at home improved their concentration and increased their productivity.
Nearly all participants reported that not having to travel to work was the main positive aspect of working from home. Reduced commuting meant fewer accessibility problems, especially for wheelchair users. This led to increased energy levels, which were sometimes channeled into leisure activities.
Theme 2: Challenges faced when working during COVID-19
Participants experienced challenges when returning to their workplaces, mostly associated with a lack of support, as social distancing rules were not followed there, potentially increasing their chances of contracting COVID-19. Conversely, loneliness was reported as a downside of working from home. Those who were self-employed felt particularly overlooked, because for some such as those working in the film industry, their jobs did not allow the possibility to work from home, and they could not afford to go on furlough.
A series of barriers to receiving reasonable adjustments were discussed. Not all participants received the necessary tools to work from home. For example, 1 participant who could not afford to pay for the internet was unable to work for months because the employer did not provide her with further support. Others reported an increase in their workloads.
Theme 3: Relevance of manager
Most participants reported having supportive managers who were understanding of participants’ MS and accommodated their requests for reasonable adjustments. These positive relationships remained even during the pandemic and became stronger because these managers considered the needs of their employees with MS when planning the return to the office.
Some participants had difficult relationships with their managers even before the pandemic. This was either because the managers did not understand MS or because they were not willing to provide their employees with reasonable adjustments. Those with a poor relationship with their manager felt isolated. This was mainly attributed to the disengagement of managers whose communication with their employees was infrequent.
A challenge faced by 2 interviewees was having a new manager whom they had never met in person. This made it difficult for them to develop a positive relationship and disclose their MS.
Theme 4: Returning to normal
As society began to reopen, nearly all of the participants intended to continue to work from home in some capacity. Before the pandemic, only 5 of the 15 interviewees had a hybrid working pattern, working from home at least 1 day a week.
Participants expressed a preference for continuing to work from home due to the benefits previously discussed. While some were pushed to return to the office, 3 managed to change their contracts to permanently work from home.
Interviewees had mixed feelings regarding how safe it was to return to the office. The opinions seemed to vary according to their beliefs in the efficacy of the vaccines.
Understandably, many participants were anxious about how their MS treatment reduced their immune function and vaccine efficacy. This was paired with concerns about the infection risk in office spaces.
Theme 5: Vocational needs
Even after the pandemic, interviewees felt they needed additional help to continue working. Most had received some mental health support from their employers, usually virtual well-being sessions. However, some participants saw this as a “box-ticking exercise” for employers. Furthermore, these sessions contained no information about the needs of people with disabilities. Interviewees also wanted more help requesting reasonable adjustments and understanding their legal rights at work.
DISCUSSION
There were conflicting findings between the survey and interviews regarding the challenges and benefits of working with MS during the COVID-19 pandemic. Of survey respondents, 40% said they faced more difficulties concentrating while working during the pandemic than they did before the pandemic. In contrast, interviewees reported improved work performance because working from home meant that they had fewer distractions.
These conflicting results may be explained by the diverse demographic and employment characteristics of the interviewees. For example, the survey included a slightly larger proportion of women than the interviews. Previous studies have found associations between women and unemployment, with women being more likely to be unemployed than men.10 Therefore, sex-related differences in responsibilities and workload may be responsible for the discrepancy in our findings.
A similar study (N = 69) conducted in the United States found high rates of job loss.20 This was not the case for our sample, potentially because our participants had relatively high levels of education and many had office-based jobs, both of which have been shown to protect against job loss.21,22 Differences in the support schemes offered in the UK vs in the US may also be a reason for this discrepancy.
Most research has focused on understanding the barriers to job retention, but little attention has been given to the support that could remove these barriers.23,24 Our study has reported the types of support that people with MS find beneficial to improving their work experience. Having a flexible work schedule (eg, being allowed to take breaks, flexible working hours) or working from home are the adjustments most commonly requested by people with MS.14,25,26 Before the pandemic, most employers rejected requests for this kind of support. Our findings and others27 suggest that employers may be reconsidering their views about remote working. In an online survey of managers before the pandemic, 57% believed employees had to be present in the workplace to advance in their roles; this decreased to 48% during the pandemic,27 which suggests a cultural shift in work practices as companies realize they can operate remotely. Whether this shift and the unintended benefit for people with MS can be sustained long term, as things return to normal, remains to be seen.
Our survey participants identified some unintended benefits to working during the COVID-19 pandemic (eg, reduced travel, working from home). This aligns with a UK-based study, which reported higher levels of satisfaction with work arrangements during the pandemic for people who were allowed to work from home vs those who were not permitted to do so.28
In previous studies, a large proportion of people with MS reported fatigue as a reason for leaving the workforce.29 Although having a flexible working schedule can help manage fatigue within the context of work, some survey participants did report more difficulty in managing fatigue than before the pandemic. This variability may have been caused by increased caring responsibilities during the pandemic (ie, homeschooling), feelings of anxiety, social isolation, and changes in eating behaviors.30
Research has shown that working from home can lead to higher job satisfaction and lower levels of absenteeism in employees with disabilities.31 Thus, employers should consider providing flexibility to their employees with MS by allowing them to work from home where possible. Unfortunately, there are also disadvantages to working from home, some of which were discussed in the interviews, such as reduced communication with the team, not having access to equipment (including the internet), or not having a suitable working environment in the home.32 Although not all jobs can be conducted from home, in-office workers could still benefit from having the flexibility to take breaks and rest if they feel fatigued during the day. Regardless of the type of employment (manual labor vs office-based work), employers need to be open to reasonable adjustments to match employee needs such as being allowed to have a flexible working pattern that allows the employee with MS to manage disease-related and environmental factors (eg, office accessibility, working patterns).33
The findings from the regression analyses suggest that being a woman with MS and working in the public sector were associated with experiencing more feelings of anxiety or stress when working during the pandemic. People in these categories may be at a higher risk of job loss because increased feelings of anxiety or stress can worsen MS symptoms,34 and aggravated symptoms may lead to withdrawal from the workforce.
It is well known that people with higher levels of disability experience more problems remaining employed.8–10 Unfortunately, participants who reported a larger number of MS symptoms when working during the pandemic were less likely to receive support from their managers. The lack of support could also put them at a higher risk of job loss.
Interviewees reported that most of their employers offered generic mental health support, but failed to consider other avenues of support that might better meet the needs of people with disabilities. A recent report suggests that organizations tend to have policies in place to help people with disabilities at work, but employers often lack the knowledge and skills to implement them.35 The challenges of supporting people with disabilities in the workplace may have been amplified during the pandemic. Thus, VR services should include support for employers that implement reasonable adjustments.
Interestingly, almost half of the people surveyed indicated that they did not need any additional support or accommodations for their MS from their employers. However, the overall findings suggest that participants could benefit from support that helps them manage symptoms and relationships at work. These findings align with previous research that suggests that people with MS may not identify themselves as having problems at work.36 This may cause people to access employment services too late, when they have already reached the point where they are at an increased risk of job loss. Thus, it is recommended that health care professionals ask their patients with MS about their jobs and help them reflect on their employment situation to identify those in need of support.36
Limitations
Our study was underpinned by theoretical frameworks that allowed for the identification of biological (ie, MS symptoms) and environmental (ie, job characteristics) factors that were easy or challenging to manage at work during the pandemic. However, it still had some limitations. The survey was conducted online, which might lead to bias toward people who have internet access and a better command of technology. However, to facilitate participation, it was possible to complete the survey on a smartphone. Due to the recruitment approach (eg, social media, posters in clinical areas), we could not estimate the response rate for the survey. Only 3 participants recruited for the survey were from a minority ethnic group. Therefore, we did not capture in detail the experiences of these populations. Finally, this study was conducted after the first national lockdown in the UK. There were 2 more lock-downs, and the support offered to organizations varied considerably throughout the pandemic. Nevertheless, this study provided valuable information about the issues that people with MS experienced while working in the UK during the COVID-19 pandemic.
CONCLUSIONS
The flexibility of working from home enabled people with MS to better manage their condition, in part by removing the impact of traveling to work. However, people with MS also faced difficulties managing their ability to concentrate when working and managing fatigue levels.
Future research should explore the impact that flexible working arrangements (eg, working from home, breaks at work, modifying working hours) can have on the long-term productivity, frequency of absence due to sickness, and employment rates of people with MS and the associated costs to and benefits for employers. It should also explore how the organizational learning around supporting employees with MS persists to determine whether these pandemic-influenced work facilitators are or can be sustained.
PRACTICE POINTS
As proven by COVID-19 pandemic data, flexibility at work, including being allowed to take breaks or working from home, can help people self-manage their multiple sclerosis (MS) symptoms and feel better supported by their employers.
Clinicians should offer advice and resources to their patients on how to manage MS symptoms in the workplace, how to disclose their MS diagnosis to their employers, and how to determine their legal rights at work.
ACKNOWLEDGMENTS:
We would like to thank the participants for their time and involvement in the research. We would like to thank collaborators at the 4 sites (Nottingham University Hospitals, Leeds Teaching Hospital, Cardiff and Vale University Local Health Board, and Queen Mary University London) for their support throughout the study.
Footnotes
PREVIOUS PRESENTATION: This study was presented as a poster and 1-minute express presentation at the annual Rehabilitation in Multiple Sclerosis conference; May 2023; Genoa, Italy.
FINANCIAL DISCLOSURES: Roshan das Nair, PhD, has received funding (speakers’ bureau) from Biogen, Merck, and Novartis. In the past 5 years, Emma Tallantyre, PhD, FRCP, has received an honorarium for consulting work from Biogen, Janssen, Merck, Novartis, and Roche. She also received travel grants to attend or speak at educational meetings from Biogen, Merck, Novartis, Roche, and Takeda.
REFERENCES
- 1.COVID-19 [Accessed May 18, 2020];Government of the United Kingdom. https://www.gov.uk/coronavirus [Google Scholar]
- 2.Check if you can claim for your employees’ wages through the Coronavirus Job Retention Scheme. HM Revenue and Customs. [Accessed May 18, 2020]. Oct 29, 2021. https://www.gov.uk/guidance/claim-for-wage-costs-through-the-coronavirus-job-retention-scheme
- 3.An overview of workers who were furloughed in the UK: October 2021 Office of National Statistics; Oct 1, 2021. https://www.ons.gov.uk/employmentandlabourmarket/peopleinwork/employmentandemployeetypes/articles/anoverviewofworkerswhowerefurloughedintheuk/october2021 [Google Scholar]
- 4.Guidance on shielding and protecting people who are clinically extremely vulnerable from COVID-19 Public Health England; [Accessed May 18, 2020]. https://www.gov.uk/government/publications/guidance-on-shielding-and-protecting-extremely-vulnerable-persons-from-covid-19 [Google Scholar]
- 5.Francis-Devine B, Powell A. Coronavirus: Impact on the Labour Market. House of Commons Library; Aug 9, 2022. [Accessed January 8, 2023]. https://researchbriefings.files.parliament.uk/documents/CBP-8898/CBP-8898.pdf [Google Scholar]
- 6.Holland P. Will disabled workers be winners or losers in the post-COVID-19 labour market? Disabilities. 2021;1(3):161–173. doi: 10.3390/disabilities1030013. doi: [DOI] [Google Scholar]
- 7.British Society of Rehabilitation Medicine Vocational Rehabilitation-The Way Forward. 2nd ed. British Society of Rehabilitation Medicine; 2003. p. 5. [Google Scholar]
- 8.Povolo CA, Blair M, Mehta S, Rosehart H, Morrow SA. Predictors of vocational status among persons with multiple sclerosis. Mult Scler Relat Disord. 2019;36:101411. doi: 10.1016/j.msard.2019.101411. doi: [DOI] [PubMed] [Google Scholar]
- 9.Busche KD, Fisk JD, Murray TJ, Metz LM. Short term predictors of unemployment in multiple sclerosis patients. Can J Neurol Sci. 2003;30(2):137–142. doi: 10.1017/s0317167100053403. doi: [DOI] [PubMed] [Google Scholar]
- 10.Honarmand K, Akbar N, Kou N, Feinstein A. Predicting employment status in multiple sclerosis patients: the utility of the MS functional composite. J Neurol. 2011;258(2):244–249. doi: 10.1007/s00415-010-5736-8. doi: [DOI] [PubMed] [Google Scholar]
- 11.Roessler RT, Rumrill PD, Fitzgerald SM. Predictors of employment status for people with multiple sclerosis. Rehabil Couns Bull. 2004;47(2):96–103. doi: 10.1177/00343552030470020401. doi: [DOI] [Google Scholar]
- 12.World Health Organization World Health Organization; [Accessed May 18, 2020]. International Classification of Functioning, Disability and Health (ICF)https://www.who.int/standards/classifications/international-classification-of-functioning-disability-and-health [Google Scholar]
- 13.Michie S, van Stralen MM, West R. The behaviour change wheel: a new method for characterising and designing behaviour change interventions. Implement Sci. 2011;6:42. doi: 10.1186/1748-5908-6-42. doi: [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.De Dios Pérez B, Radford K, das Nair R. Experiences of people with multiple sclerosis at work: towards the understanding of the needs for a job retention vocational rehabilitation intervention. Work. 2022;72(1):303–313. doi: 10.3233/WOR-210012. doi: [DOI] [PubMed] [Google Scholar]
- 15.Cole FL. Content analysis: process and application. Clin Nurse Spec. 1988;2(1):53–57. doi: 10.1097/00002800-198800210-00025. doi: [DOI] [PubMed] [Google Scholar]
- 16.Nvivo 12 Version 12. QSR International; 2018. [Accessed May 18, 2020]. https://community.lumivero.com/s/nvivo-knowledge-base?language=en_US [Google Scholar]
- 17.Parkinson S, Eatough V, Holmes J, Stapley E, Midgley N. Framework analysis: a worked example of a study exploring young people’s experiences of depression. Qual Res Psychol. 2016;13:109–129. doi: 10.1080/14780887.2015.1119228. doi: [DOI] [Google Scholar]
- 18.Pope C, Ziebland S, Mays N. Qualitative research in health care: analysing qualitative data. BMJ. 2000;320(7227):114–116. doi: 10.1136/bmj.320.7227.114. doi: [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Yardley L. Dilemmas in qualitative health research. Psychol Health. 2000;15:215–228. doi: 10.1080/08870440008400302. doi: [DOI] [Google Scholar]
- 20.Bishop M, Rumrill SP. The employment impact of the COVID-19 pandemic on Americans with MS: preliminary analysis. J Vocat Rehabil. 2021;54(1):81–87. doi: 10.3233/JVR-201120. doi: [DOI] [Google Scholar]
- 21.Krause I, Kern S, Horntrich A, Ziemssen T. Employment status in multiple sclerosis: impact of disease-specific and non-disease-specific factors. Mult Scler. 2013;19(13):1792–1799. doi: 10.1177/1352458513485655. doi: [DOI] [PubMed] [Google Scholar]
- 22.Simmons RD, Tribe KL, McDonald EA. Living with multiple sclerosis: longitudinal changes in employment and the importance of symptom management. J Neurol. 2010;257(6):926–936. doi: 10.1007/s00415-009-5441-7. doi: [DOI] [PubMed] [Google Scholar]
- 23.Doogan C, Playford ED. Supporting work for people with multiple sclerosis. Mult Scler. 2014;20(6):646–650. doi: 10.1177/1352458514523499. doi: [DOI] [PubMed] [Google Scholar]
- 24.Sweetland J, Howse E, Playford ED. A systematic review of research undertaken in vocational rehabilitation for people with multiple sclerosis. Disabil Rehabil. 2012;34(24):2031–2038. doi: 10.3109/09638288.2012.669019. doi: [DOI] [PubMed] [Google Scholar]
- 25.New research for MS Week shows 1/3 people with MS kept it secret MS Society UK; Apr 19, 2021. [Accessed January 8, 2023]. https://www.mssociety.org.uk/what-we-do/news/new-research-ms-week-shows-13-people-ms-kept-it-secret [Google Scholar]
- 26.Sweetland J. Vocational Rehabilitation for People With Multiple Sclerosis. Dissertation. University College London; 2010. [Accessed January 8, 2023]. https://discovery.ucl.ac.uk/1352628/1/1352628.pdf [Google Scholar]
- 27.Birkett H, Forbes S, Evans L, Chung H. Managing Employees During COVID-19: Flexible Working and the Future of Work (Phase Two) University of Birmingham; 2021. [Accessed January 8, 2023]. https://www.birmingham.ac.uk/documents/college-social-sciences/business/research/responsible-business/managing-employees-during-covid19.pdf [Google Scholar]
- 28.Beesley R, Cauchi M, Davies L, et al. Multiple sclerosis and COVID-19: assessing risk perception, patient behaviors and access to disease-modifying therapies. Mult Scler Relat Disord. 2022;68:104121. doi: 10.1016/j.msard.2022.104121. doi: [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29.Strober LB, Christodoulou C, Benedict RH, et al. Unemployment in multiple sclerosis: the contribution of personality and disease. Mult Scler. 2012;18(5):647–653. doi: 10.1177/1352458511426735. doi: [DOI] [PubMed] [Google Scholar]
- 30.Dicken SJ, Mitchell JJ, Newberry Le Vay J, et al. Impact of COVID-19 pandemic on weight and BMI among UK adults: a longitudinal analysis of data from the HEBECO study. Nutrients. 2021;13(9):2911. doi: 10.3390/nu13092911. doi: [DOI] [PMC free article] [PubMed] [Google Scholar]
- 31.Giovanis E, Ozdamar O. Accommodating employees with disabilities: the role of flexible employment schemes in Europe. SSRN. 2019 doi: 10.2139/ssrn.3441925.. doi: [DOI] [Google Scholar]
- 32.Bolisani E, Scarso E, Ipsen C, Kirchner K, Hansen JP. Working from home during COVID-19 pandemic: lessons learned and issues. Manag Mark. 2020;15(S1):458–476. doi: 10.2478/mmcks-2020-0027. doi: [DOI] [Google Scholar]
- 33.Vitturi BK, Rahmani A, Dini G, et al. Work barriers and job adjustments of people with multiple sclerosis: a systematic review. J Occup Rehabil. 2023;33(3):450–462. doi: 10.1007/s10926-022-10084-1. doi: [DOI] [PubMed] [Google Scholar]
- 34.Mohr DC, Hart SL, Julian L, Cox D, Pelletier D. Association between stressful life events and exacerbation in multiple sclerosis: a meta-analysis. BMJ. 2004;328(7442):731. doi: 10.1136/bmj.38041.724421.55. doi: [DOI] [PMC free article] [PubMed] [Google Scholar]
- 35.Kumar S, Provost C. Ableism and the Labour Market. University College of London; 2022. [Accessed May 18, 2020]. https://discovery.ucl.ac.uk/id/eprint/10154323/ [Google Scholar]
- 36.Sweetland J, Playford D, Radford KA. What is ‘early intervention’ for work related difficulties for people with multiple sclerosis? A case study report. J Neurol Neurophysiol. 2014;5(6):1–7. doi: 10.4172/2155-9562.1000252. doi: [DOI] [Google Scholar]