

Abstract
Focal fibrocartilaginous dysplasia (FFCD) is a rare disease that can cause angular deformities of long bones. The common pathologic finding is a thick fibrotic band extending from epiphysis to metaphysis on one side of the bone. The tethering effect of the fibrotic band around the growth plate is thought to be the main etiology for the development and progression of the deformity. FFCD mostly affects the proximal tibia and the distal femur. The literature contains different treatment options. Here, we present the case of a 20-month-old girl with FFCD on the medial side of the distal femur causing varus deformity. Our treatment protocol included excision of the fibrotic band from the medial side and application of a two-hole plate for guided growth on the lateral side of the distal femur. Deformity correction was achieved rapidly with no complications. A literature review is also presented along with pathologic and magnetic resonance imaging findings.
Keywords: Fibrocartilaginous Dysplasia, Guided Growth, Femoral Deformity, Fibrous
Introduction
Focal fibrocartilaginous dysplasia (FFCD) is a rare kind of fibrous dysplasia with different amounts of hyaline cartilage (1). It is a genetic disease caused by a missense mutation. Differential diagnosis includes enchondroma, chondromyxoid fibroma, eosinophilic granuloma, and chondrosarcoma owing to hyaline cartilage. Angular deformity caused by FFCD may complicate differential diagnosis, and the deformity can be confused with infantile Blount’s disease in the tibia. The patient should be evaluated clinically in a comprehensive manner, and the definitive diagnosis can be made with biopsy showing benign fibrous tissue and hyaline cartilage with the lack of atypia (2). FFCD with angular deformity was described for the first time by Bell et al. in an infant with unilateral tibia vara (3). The mechanism of the deformity in FFCD is considered to be a fibrous band acting like a tether between the metaphysis and the growth plate. The tethering effect of the fibrous band causes a hemiepiphysiodesis effect and results in angular deformities as well as limb-length discrepancies of long bones (4, 5). Patients are mostly diagnosed with varus or valgus malalignment of the lower extremities at the age of 12–24 months (6).
A total of 23 cases of fibrocartilaginous dysplasia of the distal femur have been reported, but the literature lacks a standard treatment algorithm for long-bone deformities in FFCD. Spontaneous resolution was observed in 2 cases, whereas in the others, excision of the fibrous band, curettage, osteotomy, or a combination of different surgical methods was applied (4, 5, 7, 8).
Guided growth with tension band plating has become popular for angular deformities of the long bones in the past few decades. The guided growth technique aims to control the physeal activity on one side of the physis while allowing it on the other side. The temporary inhibition of growth and low risk of physeal injury are the main advantages of the technique. Being able to achieve temporary hemiepiphysiodesis with a low risk of physeal injury allows surgeons to use the technique in patients of very young age. Stevens et al. have treated 65 angular deformities with tension band plating and achieved satisfactory correction in 97% of the deformities (9). Yılmaz et al. have shown that tension band plating was also effective in different kinds of skeletal dysplasia with low growth potential (10).
FFCD is a unique and rare pathology with a fibrous band causing a tethering effect on one side of the physis. We think that the fibrous lesion needs to be removed to prevent the tethering effect, and tension band plating is an effective alternative treatment for coronal plane deformity. This case presentation aimed to report the result of a combined approach for varus deformity of the distal femur caused by medial FFCD.
Case Presentation
A 20-month-old girl with varus deformity of the left lower extremity was evaluated in an outpatient clinic. Her radiological evaluation revealed varus deformity of the distal femur with a sclerotic lesion in the metaphysis. An effort was made to take an X-ray with a lift to create a level pelvis, but the patient was not compliant. No apparent sagittal plane deformity was observed during the clinical examination; therefore, a lateral erect full-length X-ray was not obtained. The mechanical lateral distal femoral angle (mLDFA) was 132° (Figure 1), the medial proximal tibial angle was 91°, and the affected femur was 1.5 cm shorter than the normal side. Magnetic resonance imaging (MRI) of the left femur was also conducted. The MRI revealed a low-signal area in the medial part of the distal femur on both T1- and T2-weighted sequences (Figure 2). This thick, low-signal lesion was interpreted as a fibrotic band, and it extended from the epiphyseal area into the metaphyseal groove blended with the periosteum proximally. The patient had no history of metabolic disease, trauma, or infection.
Figure 1. a–d.
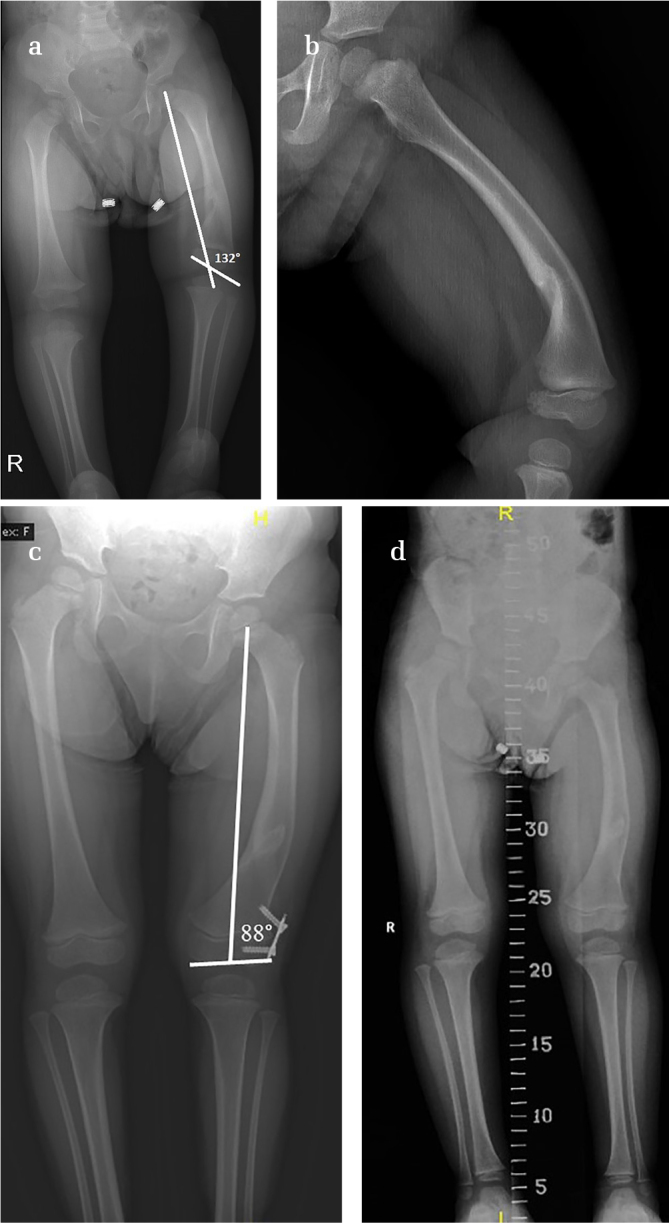
Preoperative standing X-ray shows varus and procurvatum deformity of the distal femur. The mechanical lateral distal femoral angle mLDFA was 132° (a, b). The mLDFA was 88°, and acceptable alignment was achieved in the 12-month follow-up after surgery (c). The 2-year follow-up X-ray shows good coronal plane alignment and 1.5 cm limb-length discrepancy (d)
Figure 2. a, b.
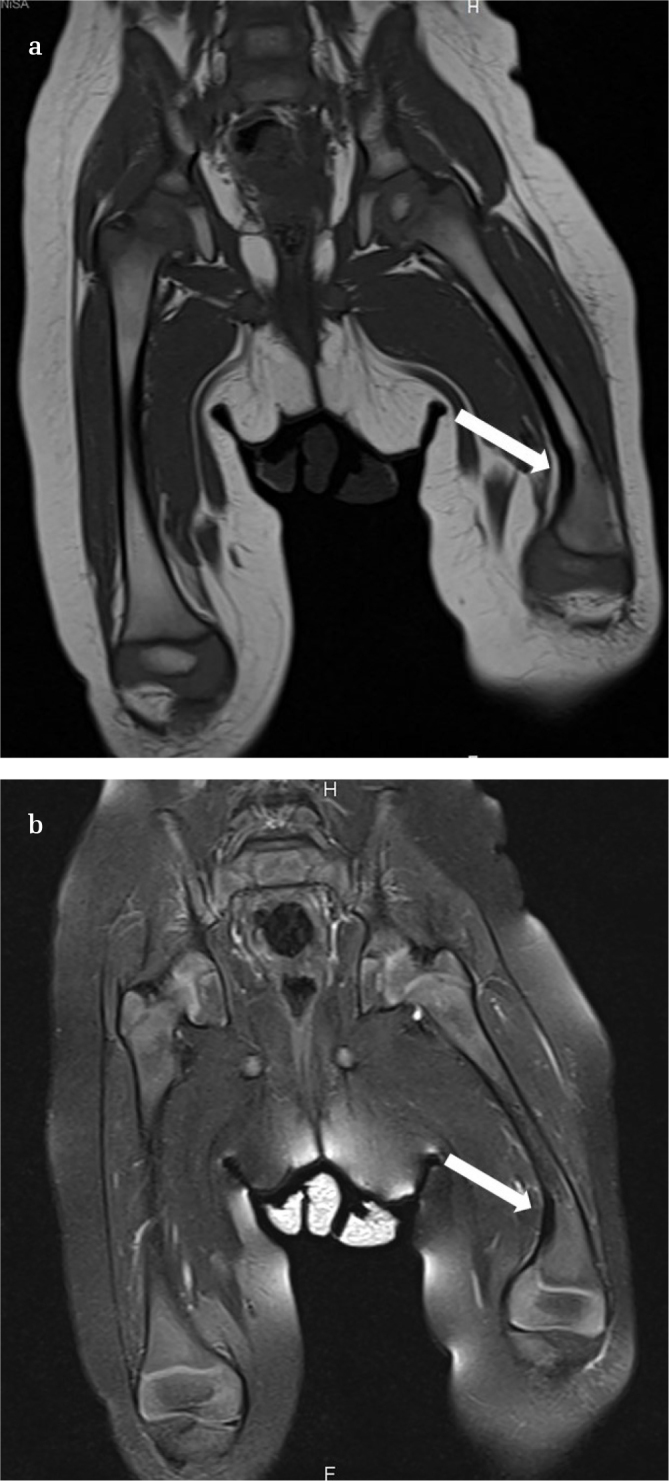
T1- (a) and T2- (b) weighted sequences revealed a hypointense fibrotic band extending from the epiphysis to the metaphyseal area (white arrows) on the medial side of the distal femur. The thick low-signal lesion blends with the periosteum proximally
The femoral deformity in the patient was thought to have been caused by the FFCD, and she was taken to the operating room for the removal of the femoral lesion on the medial side (Figure 3a) and the application of a two-hole plate on the lateral side of the growth plate. We thought that removal of the lesion alone would give unpredictable results in terms of deformity correction; therefore, the procedure was combined with tension band plating of the lateral distal femur (Figure 3b).
Figure 3. a–d.
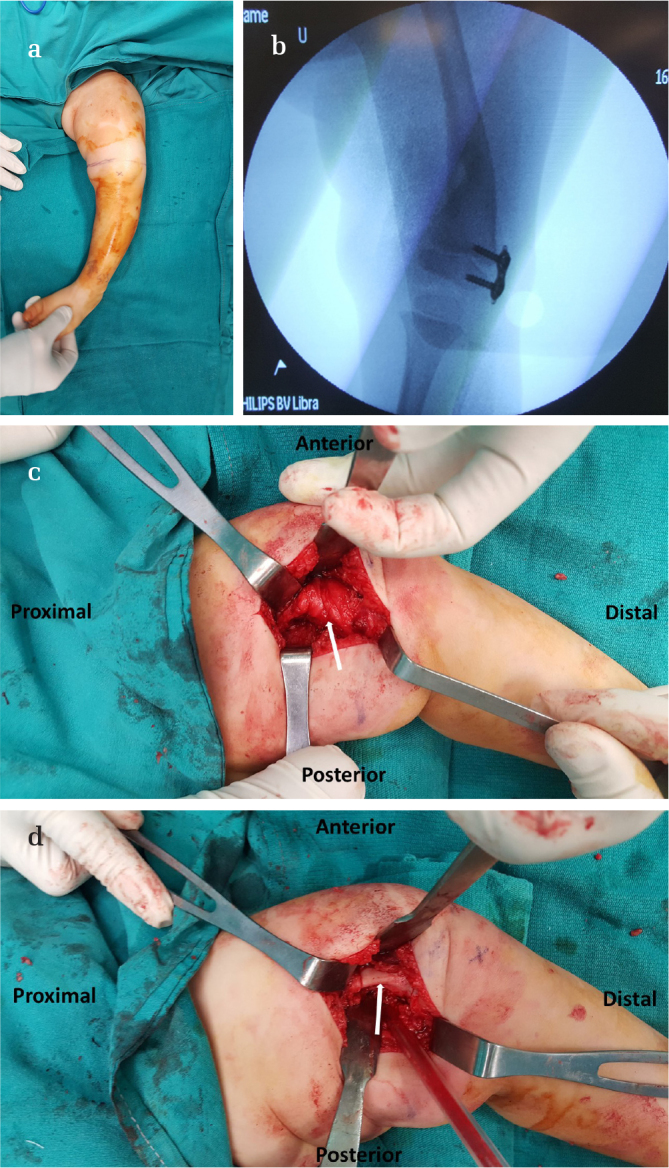
Femoral varus deformity of the patient caused by focal fibrocartilaginous dysplasia (a). Intraoperative fluoroscopy image showing tension band plating in place after excision the fibrous band (b). Appearance of the fibrous tissue (white arrow) after retraction of the vastus medialis (c). Bony area (white arrow) after excision of the fibrous lesion starting from the level of the physis to the metaphyseal groove (d)
Surgical technique
The first part of the procedure was applied through a medial longitudinal incision just proximal to the level of the distal femur growth plate. The lesion, which was formed by thick fibrous tissue blended with the periosteum, was exposed after the vastus medialis was retracted anteriorly. The fibrous lesion was exposed from the epiphysis to the metaphyseal groove. The excision was started from the epiphyseal area. Attention was given not to excise normal cartilage from the epiphysis and damage the growth plate. Once the lesion was detached from the epiphyseal area, the excision continued proximally including the periosteum over the metaphysis. The excision of the fibrous lesion was completed at the level of metaphyseal groove. Excision of the fibrous band was followed by the application of tension band plating, as described in the literature (Figure 3. c, d).
Histopathologically, the lesion was composed of hyalinized fibrous and mature adipocytic tissue lined with synovium on one side. The fibrous tissue was reminiscent of a tendon or thickened fascia. Papillary architecture made up of the synovial cells revealed the presence of synovial tissue lying on the fibrous tissue (Figure 4).
Figure 4. a, b.

(a) Low-power field view demonstrates mature adipocytes at the bottom and hyalinized fibrous tissue resembling a tendon and papillary synovial tissue on top (40×, hematoxylin and eosin). (b) High-power magnification reveals synovial lining on the hyalinized hypocellular fibrous tissue (200×, hematoxylin and eosin)
The patient was followed up at 4-month intervals. Correction of the deformity was achieved in 12 months after the surgery, and the tension band plating was removed at the age of 34 months. A 1-year follow-up X-ray after the removal of the plate revealed good alignment of the lower extremity with no recurrence, and 1.5 cm of limb-length discrepancy remained constant.
The patient’s family was informed that the data concerning the case would be submitted for publication, and they provided consent.
Discussion
FFCD is a benign lesion that causes long-bone deformities in early childhood. Although the pathologic mechanism by which FFCD causes bone deformities has not been elucidated, it is thought to be the tethering effect of the thick fibrous tissue extending from the epiphysis to the metaphysis, causing a hemiepiphysiodesis effect. Jouve et al. have suggested calling this lesion as “fibrous periosteal inclusion” (4). They have stated that spontaneous resolution or deterioration in deformity may occur depending on the strength and length of this fibrous structure. FFCD is mostly seen in the proximal tibia and distal femur. It can cause varus or valgus deformities, depending on the location of the lesion (11). Although spontaneous resolution of the deformity was reported in half of the tibia cases, it is less likely to occur in the femur (5, 7).
To date, there have been 23 cases of distal femoral angular deformity caused by FFCD with various treatment methods and outcomes in the literature (12–18) (Table 1). Thabet et al. have reported spontaneous resolution of distal femoral angular deformity in an 18-month-old girl over 7 years of follow-up (5). Lateral distal femoral angle improved from 120° to 86° with 1 cm of residual limb-length discrepancy. Johari et al. followed up a 2-year-old patient, and mLDFA improved from 127° to 87° without any surgical intervention (7). Limb-length discrepancy increased from 1.5 to 3.0 cm. Although those deformities resolved spontaneously, this treatment approach leaves the patient with a deformed extremity for a long time, and there is no certain time period in which the correction is anticipated.
Table 1.
Literature review for distal femoral FFCD
| Author | Sex; Age | Location | Age at Surgery | Deformity | Treatment |
|---|---|---|---|---|---|
| Albinana et al. (15) | F; 16 m. | Medial | NR | Varus 45° | Periosteal release |
| Macnicol et al. (11) | M; 24 m. | Medial | NR | Varus 35° | Osteotomy |
| M; 10 m. | Medial | NR | Varus | Osteotomy | |
| Choi et al. (16) | M; 17 m. | Posteromedial | 33 m. | Varus 42° | Osteotomy+ Lengthening |
| F; 15 m. | Posterolateral | 25 m. | Valgus 22° | Osteotomy+ Lengthening | |
| Beaty and Barrett (17) | M; 30 m. | Lateral | 54 m. | Valgus 20° | Osteotomy |
| M; 42 m. | Medial | 66 m. | Varus 15° | Osteotomy +Band excision | |
| F; 15 m. | Posteromedial | NR | Varus 30° | Osteotomy +Band excision | |
| M; 9 m. | Lateral | NR | Valgus | Osteotomy +Band excision | |
| VallcaneraCalatayudet al. (18) | M; 13 m. | Medial | 24 m. | Varus 60° | Osteotomy + Band excision |
| Amillo et al. (19) | M; 27 m. | Medial | 44 m. | Valgus 40° | Osteotomy + Fibrous band excision |
| Poul and Straka (13) | M; 11 m. | Posteromedial | NR | Varus 27° | Band excision + Periosteal release |
| Ruchelsman et al. (8) | F; 13 m. | Posterolateral | 27 m. | Valgus 30° | Band excision + Curettage |
| Berson et al. (20) | F; 16 m. | Anteromedial | 29 m. | Varus 36° | Osteotomy + Band excision |
| M; 15 m. | Medial | 24 m. | Varus 22° | Osteotomy + Band excision | |
| Ando et al. (6) | M: 12 m. | Medial | 24 m. | Varus 40° | Band excision + Correction with Ilizarov |
| Jouve et al. (4) | F; 40 m. | Lateral | 40 m. | Valgus 15° | Curettage |
| Thabet et al. (5) | F; 18 m. | Medial | No surgery | LDFA 120°, MPTA 103° | Observation |
| Welborn et al. (14) | M; 16 m. | Medial | 29 m. | Varus 31° | Guided growth |
| M; 13 m. | NR | 21 m. | Varus 28° | Guided growth | |
| M; 16 m. | NR | 22 m. | Varus 34° | Guided growth | |
| Johari and Anjum (7) | 24 m. | Posteromedial | No surgery | Varus 39° | Observation |
| Thanacharoenpanich et al. (21) | 25 m. | Posterolateral | 32 m. | Valgus 20° | Fibrous band excision + Curettage+ Varus osteotomy |
NR: Not reported; mLDFA: mechanical lateral distal femoral angle; m: month; M: male; F: female
Rodríguez et al. have treated 2 individuals aged 15 months and 19 months, who had distal femoral angular deformity with excising fibrous tether and osteotomy of the femur (12). They have reported good femoral alignment and acceptable limb-length discrepancy. However, we should keep in mind that femoral correction osteotomy is more invasive and prone to complications, such as nonunion, under/overcorrection, or implant-related complications. Moreover, 4–6 weeks of immobilization in a single-leg hip spica casting is required after surgery. We think that a less invasive approach without osteotomy should be used in those young patients.
Ruchelsman et al. have treated a 34-month-old girl with valgus deformity of the distal femur (8). Excision and curettage of the lateral fibrous band was performed, and the deformity was resolved with only 1 cm of limb-length discrepancy in the 2-year follow-up. In another case report, correction of the deformity after excision of the fibrous tissue required 108 months (13). Although we can anticipate that the deformity will resolve after fibrous tissue excision alone, the time period for correction is unpredictable, and long time period might be required before satisfactory correction is obtained. We think that a more proactive approach is needed for deformity correction.
Welborn et al. have reported 3 patients with distal femoral varus deformity, aged 13–16 months (14). All of their patients were treated with guided growth through a two-hole plate. One patient had 1 cm of limb-length discrepancy, whereas another had increased femoral anteversion, which was treated with femoral derotation osteotomy. Their approach did not include fibrous band excision. The tethering effect of the fibrous band is one of the main pathologic mechanisms causing the deformity. Although it has not been reported, one of the potential complications of not removing the fibrous band might be insufficient correction and increased risk of recurrence.
We performed excision of the fibrous band on the medial side and guided growth with a two-hole plate on the lateral distal femur. In this way, we removed the basic pathologic structure causing the deformity and applied a surgical technique (temporary guided growth utilizing a two-hole plate) that has been shown to be effective and safe for deformity correction at a young age. With this technique, the hemiepiphysiodesis effect is temporary and the risk of permanent physeal arrest is very low. Rapid correction of the coronal plane angular deformity was obtained. Procurvatum deformity of the patient was neglected considering the better remodeling capacity of the femur in the sagittal plane. Osteotomy could be planned if the patient had significant sagittal plane deformity during follow-up, but there was no need for osteotomy.
Conclusion
Excision of the fibrous band combined with guided growth is an effective option for management of angular deformities caused by FFCD.
HIGHLIGHTS.
Focal Fibrocartilaginous Dysplasia (FFCD) is a rare cause of lower extremity deformity in children.
The pathologic mechanism behind the development of deformity in FFCD is thought to be the tethering effect of the fibrous lesion in epi-metaphyseal region.
Although it is unpredictable, spontaneous correction was reported in the literature. So, follow-up of the patients until one year of age before surgery can be applied.
Different treatment modalities have been proposed for the correction of the deformities including fibrous band excision alone, osteotomies and guided growth.
We believe that a more proactive approach including excision of fibrocartilaginous lesion and application of two-hole tension-band plate for guided growth is more reliable and effective.
Footnotes
Informed Consent: Informed consent was obtained from the parents’ of the patients.
Author Contributions: Concept - G.Y.; Design - G.Y., S.B.; Supervision - G.Y.; Resources - G.Y., S.B., E.T.Y., K.K.; Materials - G.Y., S.B., E.T.Y., K.K.; Data Collection and/or Processing - S.B, E.T.Y., K.K.; Analysis and/or Interpretation - G.Y., S.B.; Literature Review - G.Y., S.B., E.T.Y.; Writing - S.B., E.T.Y., K.K.; Critical Review - G.Y.
Conflict of Interest: The authors have no conflicts of interest to declare.
Financial Disclosure: The authors declared that this study has received no financial support.
References
- 1. Kyriakos M, McDonald DJ, Sundaram M. Fibrous dysplasia with cartilaginous differentiation (“fibrocartilaginous dysplasia”): a review, with an illustrative case followed for 18 years. Skeletal Radiol. 2004;33:51–62. doi: 10.1007/s00256-003-0718-x. [DOI] [PubMed] [Google Scholar]
- 2. Müezzinoğlu B, Öztop F. Fibrocartilaginous dysplasia: a variant of fibrous dysplasia. Malays J Pathol. 2001;23:35–40. [PubMed] [Google Scholar]
- 3. Bell S, Campbell P, Cole W, Menelaus M. Tibia vara caused by focal fibrocartilaginous dysplasia. Three case reports. J Bone Joint Surg Br. 1985;67:780–4. doi: 10.1302/0301-620X.67B5.4055881. [DOI] [PubMed] [Google Scholar]
- 4. Jouve J-L, Kohler R, Mubarak SJ, Nelson SC, Dohin B, Bollini G. Focal fibrocartilaginous dysplasia (“ fibrous periosteal inclusion”): an additional series of eleven cases and literature review. J Pediatr Orthop. 2007;27:75–84. doi: 10.1097/BPO.0b013e31802b7139. [DOI] [PubMed] [Google Scholar]
- 5. Thabet AM, Belthur MV, Herzenberg JE. Spontaneous resolution of angular deformity of the distal femur in focal fibrocartilaginous dysplasia: a case report. J Pediatr Orthop B. 2010;19:161–3. doi: 10.1097/BPB.0b013e3283361b11. [DOI] [PubMed] [Google Scholar]
- 6. Ando A, Hatori M, Hosaka M, et al. A patient with focal fibrocartilaginous dysplasia in the distal femur and review of the literature. Tohoku J Exp Med. 2008;215:307–12. doi: 10.1620/tjem.215.307. [DOI] [PubMed] [Google Scholar]
- 7. Johari A, Anjum R. Spontaneous resolution of focal fibrocartilaginous dysplasia of femur on long-term follow-up: case report and review of literature. J Pediatr Orthop B. 2019;28:127–31. doi: 10.1097/BPB.0000000000000570. [DOI] [PubMed] [Google Scholar]
- 8. Ruchelsman DE, Madan SS, Feldman DS. Genu valgum secondary to focal fibrocartilaginous dysplasia of the distal femur. J Pediatr Orthop. 2004;24:408–13. doi: 10.1097/01241398-200407000-00012. [DOI] [PubMed] [Google Scholar]
- 9. Stevens PM. Guided growth for angular correction: a preliminary series using a tension band plate. J Pediatr Orthop. 2007;27:253–9. doi: 10.1097/BPO.0b013e31803433a1. [DOI] [PubMed] [Google Scholar]
- 10. Yılmaz G, Oto M, Thabet AM, et al. Correction of lower extremity angular deformities in skeletal dysplasia with hemiepiphysiodesis: a preliminary report. J Pediatr Orthop. 2014;34:336–45. doi: 10.1097/BPO.0000000000000089. [DOI] [PubMed] [Google Scholar]
- 11. Macnicol MF. Focal fibrocartilaginous dysplasia of the femur. J Pediatr Orthop B. 1999;8:61–3. doi: 10.1097/01202412-199901000-00016. [DOI] [PubMed] [Google Scholar]
- 12. Albinana J, Cuervo M, Certucha J, Gonzalez-Mediero I, Abril J. Five additional cases of local fibrocartilaginous dysplasia. J Pediatr Orthop B. 1997;6:52–5. doi: 10.1097/01202412-199701000-00011. [DOI] [PubMed] [Google Scholar]
- 13. Beaty JH, Barrett IR. Unilateral angular deformity of the distal end of the femur secondary to a focal fibrous tether. A report of four cases. J Bone Joint Surg. 1989;71:440–5. doi: 10.2106/00004623-198971030-00023. [DOI] [PubMed] [Google Scholar]
- 14. Choi IH, Kim CJ, Cho T-J, et al. Focal fibrocartilaginous dysplasia of long bones: report of eight additional cases and literature review. J Pediatr Orthop. 2000;20:421–7. doi: 10.1097/01241398-200007000-00002. [DOI] [PubMed] [Google Scholar]
- 15. Vallcanera Calatayud A, Nebot CS, Fernandez MM, Orts HC. Varus deformity of the distal end of the femur secondary to a focal fibrous lesion. Pediatr Radiol. 1994;24:74–5. doi: 10.1007/BF02017672. [DOI] [PubMed] [Google Scholar]
- 16. Amillo S, Mora G, Leniz P. Progressive genu valgum secondary to a fibrous tether at the distal aspect of the femur. A case report. J Bone Joint Surg. 1998;80:424–7. doi: 10.2106/00004623-199803000-00016. [DOI] [PubMed] [Google Scholar]
- 17. Berson L, Dormans JP, Drummond DS, Davidson RS, Guerra JJ, Collins M. Fibrous lesion of the distal femur associated with angular deformity. J Pediatr Orthop. 1999;19(4):527–30. doi: 10.1097/01241398-199907000-00021. [DOI] [PubMed] [Google Scholar]
- 18. Thanacharoenpanich S, Kulkrittaya S, Pakpianpairoj C, Liupolvanich P, Chiarapattanakom P. Fibrous tether of the distal femur produced unilateral genu valgus with subsequent patellar dislocation: case report and review of the literature. J Pediatr Orthop B. 2016;25:573–81. doi: 10.1097/BPB.0000000000000304. [DOI] [PubMed] [Google Scholar]
- 19. Rodríguez P, Parra M, Miralles M, De Orbe G, Curto A. Unilateral femoral deformity due to a focal fibrous tether. Eur Radiol. 1998;8:603–5. doi: 10.1007/s003300050443. [DOI] [PubMed] [Google Scholar]
- 20. Poul J, Straka M. Periosteal tethering of growth plates in long bones (focal fibrocartilaginous dysplasia) Acta Chir Orthop Traumatol Cech. 2003;70:182–6. [PubMed] [Google Scholar]
- 21. Welborn MC, Stevens P. Correction of angular deformities due to focal fibrocartilaginous dysplasia using guided growth: a preliminary report. J Pediatr Orthop. 2017;37:e183–e7. doi: 10.1097/BPO.0000000000000785. [DOI] [PubMed] [Google Scholar]