

Abstract
Introduction and importance:
Bladder diverticula are commonly due to obstruction of the bladder outlet and are typically treated conservatively. However, the rarity and complexity of multiple giant diverticula require a tailor-made surgical approach.
Case presentation:
We report on a 72-year-old male who presented with severe urinary symptoms and lumbar pain, diagnosed with multiple giant bladder diverticula, including one compressing the ureter. The complex presentation of the patient, including his age and comorbidities, added layers of complexity to the clinical decision-making process.
Interventions and outcomes:
The patient underwent a two-stage surgery consisting of transurethral prostate resection followed by resection of three diverticula. Postoperatively, the patient showed a remarkable improvement in urinary symptoms, resolution of hydronephrosis, and, more importantly, no complications, demonstrating the efficacy and safety of the surgical strategy chosen.
Relevance and impact:
This case underscores the challenges in managing complex bladder diverticula, highlighting the importance of personalized treatment strategies and further research in atypical urological conditions. Furthermore, this case highlights the need to increase awareness and research on rare urological conditions. By sharing detailed insights from this case, we aim to enrich the clinical knowledge base, ultimately improving patient outcomes in similar challenging scenarios.
Keywords: bladder diverticula, case report, diagnostic imaging, surgical management, urology
Introduction
Highlights
An unusual case of multiple giant bladder diverticula required specialized surgery.
The patient, 72, had severe symptoms due to a diverticulum compressing the ureter.
Treatment included catheterization, antibiotics, and prostate and diverticula resection.
Post-surgery, the patient had improved urinary function without complications.
The case highlights the need for personalized care and research in complex urological issues.
Bladder diverticula are common urological conditions, characterized by the protrusion of the urothelium through the muscle fibers of the bladder wall, resulting in pouch-shaped structures. These typically form due to increased intravesical pressure and concurrent weakness in the bladder wall1. Although bladder diverticula are a frequent clinical encounter, the manifestation of multiple giant bladder diverticula is extraordinarily rare, presenting significant diagnostic and therapeutic dilemmas.
The literature reports that patients with bladder diverticula frequently have a range of urinary symptoms, including difficulty voiding and recurrent urinary tract infections (UTIs)2. Advanced diagnostic tools, particularly computed tomography (CT) scans, play a crucial role in identifying these anomalies by providing detailed information on the size, number, and potential complications associated with the diverticula.
In terms of management, surgical intervention often becomes necessary, especially when the diverticula is large, symptomatic, or associated with complications. The existing body of research suggests that, although conservative treatments may suffice for smaller asymptomatic diverticula, complex cases, such as those involving multiple giant diverticula, require a more aggressive surgical approach3.
This report details a rare case of multiple giant bladder diverticula, elaborating on its clinical presentation, diagnostic evaluation, and surgical management. In this case, our objective is to highlight the critical need for tailored surgical strategies in the management of such unusual and challenging presentations. Furthermore, we discuss the importance of a comprehensive approach in the field of urology in recognizing and effectively treating atypical bladder diverticula, thus enriching current understanding and treatment paradigms.
Case presentation
Patient information and clinical presentation
A 72-year-old male patient with a significant medical history of benign prostatic hyperplasia and recurrent urinary tract infections presented with a recent exacerbation of lumbar pain and severe urinary retention. The patient described the pain as persistent and worsening, significantly impacting his daily activities. A clinical examination revealed a palpable, firm mass in the hypogastrium. Rectal examination confirmed an enlarged prostate, estimated at 40 g, consistent with his known history of prostatic hypertrophy.
Diagnostic assessment
Laboratory tests indicated elevated renal function (creatinine: 240 μmol/l) and normal white and red blood cell counts. Urinalysis returned positive for Escherichia coli, which was sensitive to cefotaxime. Pelvic and retroperitoneal ultrasound examinations revealed multiple bladder diverticula, the largest being a posterior diverticulum measuring 12 cm×6 cm×8 cm. Additional findings included significant postvoid residual volume and unilateral right hydronephrosis with increased parenchymal echogenicity. CT imaging confirmed the presence of multiple giant bladder diverticula, with one compressing the right ureter and causing dilation of the renal cavity (Fig. 1).
Figure 1.

Computed tomography scan showing three giant bladder diverticula with compression of the right ureter (B, bladder, D, diverticulum).
Initial management
The patient’s acute presentation was managed with immediate bladder catheterization, which drained 4000 ml of cloudy urine and temporarily relieved the obstructive symptoms. Concurrent antibiotic therapy was initiated, which led to improvement in renal function and resolution of the infection, stabilizing the patient’s condition and preparing him for definitive surgical intervention.
Surgical intervention
Given the complexity of the bladder diverticula and the patient’s comorbidities, a comprehensive two-stage surgical approach was executed within a single operative session to minimize the risks associated with multiple surgeries. The initial stage involved a transurethral resection of the prostate (TURP) aimed at addressing the underlying benign prostatic hyperplasia, which contributed to the patient’s bladder outlet obstruction and was a predisposing factor for the diverticula formation.
Immediately following the TURP, the surgical team proceeded with the second stage. A subumbilical laparotomy was performed to provide optimal exposure to the bladder. A vesical incision was made, allowing precise localization and stenting of the ureteral orifices. The most significant intervention involved the meticulous resection of three large diverticula, including the notably large posterior diverticulum that was compressing the right ureter and contributing to hydronephrosis. The necks of the excised diverticula were closed using a double-layer suturing technique to ensure a robust and watertight closure, thus preventing potential complications such as leakage or recurrence (Figs 2, 3).
Figure 2.

Intraoperative image showing dissection of the diverticulum mucosa.
Figure 3.
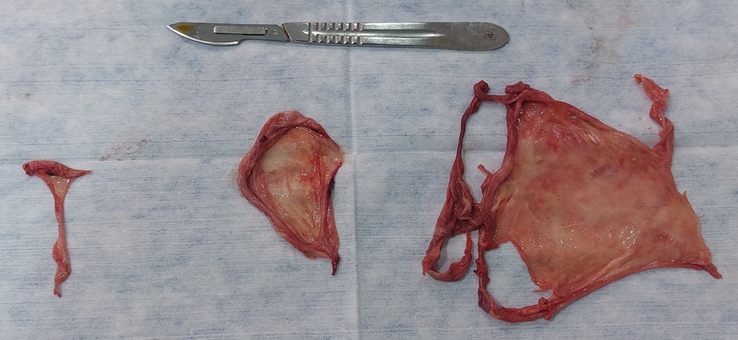
An image showing the resected wall of the diverticula.
To monitor and manage postoperative fluid accumulation and ensure proper healing, a surgical drain was placed at the end of the procedure. The drain was carefully monitored and maintained until it was deemed safe for removal, which occurred on the fifth postoperative day when clear signs of recovery were evident and the risk of complications like seroma or infection was minimized.
Postoperative course
The patient’s postoperative course was uneventful. Follow-up consultations showed the patient to be satisfied, with improved urinary function and stable renal function.
Follow-up
At 6 months of follow-up, there were no complications or recurrence of the condition and no residual urine was observed after the void.
Discussion
Mechanism of formation of the bladder diverticulum
Bladder diverticula are characterized by the protrusion of the urothelium through the muscular wall of the bladder, forming an extraneous sac1. Typically, this sac lacks muscular coverage, which impairs its effectiveness in urine removal. Although often clinically insignificant, certain cases can lead to persistent lower urinary tract symptoms (LUTS), recurrent urinary tract infections (UTIs), bladder stones4, and even a potential for malignant transformation5. These complications arise primarily from disrupted urinary function, particularly problems with detrusor muscle coordination and contraction. Studies suggest that the risk of cancerous changes in bladder diverticula ranges from 1 to 10%, necessitating surgical intervention in cases that could otherwise be considered dormant5.
Bladder diverticula are often associated with bladder outlet obstruction (BOO), and many patients experience improvement after treatments aimed at this obstruction6. This association is due to the fact that BOO leads to a chronic elevation of bladder pressures, which in turn promotes diverticula formation by exacerbating the inherent weaknesses in the bladder wall7. Comprehensive evaluations, including endoscopy, imaging, and urodynamic studies, are crucial to guide patients before considering surgical intervention. Furthermore, the development of a diverticulum often results from increased internal pressures due to low bladder compliance, and the presence of a diverticulum can further exacerbate this condition, creating a feedback loop that worsens LUTS5. This feedback mechanism highlights the importance of timely diagnosis and management to prevent progression and complications.
Diagnostic techniques
Diverticula are detectable using imaging techniques such as ultrasound, CT, and magnetic resonance imaging (MRI)1. Each of these modalities offers unique advantages; ultrasound provides a quick, non-invasive first look, CT scans offer detailed anatomical views, and MRI provides excellent soft tissue contrast without radiation exposure. A voiding cystourethrogram is particularly effective in diagnosing the diverticula of the bladder, allowing clear visualization of the relationship between the ureteral orifice and the diverticulum’s opening, as well as its size8. This technique is crucial for evaluating bladder functionality and the impact of diverticula on urine flow. These diagnostic tools are indispensable for the accurate identification and assessment of bladder diverticula, especially in complex cases such as the one presented in this report. Furthermore, endoscopic examination not only complements these imaging studies by providing a direct view of the interior of the bladder but also allows therapeutic interventions if needed1.
Surgical techniques for the management of bladder diverticulum
Various surgical approaches are available to treat bladder diverticula, including transabdominal methods, either extraperitoneal or intraperitoneal. These procedures can be performed using open surgery, laparoscopy, or robotic-assisted methods, each offering different advantages in terms of invasiveness, recovery time, and precision6,9. For patients who are not suitable candidates for extensive surgery, an endoscopic approach involving fulguration or resection can be considered10. Endoscopic techniques are less invasive and can be particularly beneficial for patients with high surgical risk or those with smaller and less complicated diverticula.
The primary surgical strategy involves dissecting near the diverticulum wall, with meticulous repair of any defects in the bladder muscle. Often, reflux or involvement of the ureteral meatus is associated with the diverticulum, requiring homolateral ureteral reimplantation. In cases of bilateral reflux, bilateral ureteral reimplantation may be indicated10. Such interventions are crucial in preventing future complications, such as recurrent infections or worsening renal function. In our case, the patient with a giant bladder diverticulum experienced significant lower urinary tract symptoms (LUTS). We opted for an intravesical surgical approach, which resulted in an uncomplicated postoperative recovery and excellent long-term results.
This case report of multiple giant bladder diverticula illuminates the intricate and diverse nature of urological anomalies that physicians may encounter. It underscores the crucial role of thorough diagnostic evaluations in identifying such complex conditions. Effective surgical management requires a customized approach that considers both the anatomical challenges and the general health status of the patient. The effectiveness of customized surgical strategies, as demonstrated in this case, is crucial in the treatment of these rare and elaborate urological presentations. Our experience with this particular case not only sheds light on the challenges posed by atypical bladder diverticula but also emphasizes the importance of personalized patient care.
Furthermore, this case serves as a testament to the necessity for continuous research and scholarly discourse in urology. It highlights the need to refine and advance diagnostic techniques and treatment modalities, especially for unusual presentations of bladder diverticula. Such advances are essential to improve patient outcomes and expand our understanding of urological pathologies.
SCARE Guidelines: The work has been reported in line with the SCARE (Surgical CAse REport) criteria11.
Conclusion
The successful treatment of this case of multiple giant bladder diverticula not only reaffirms the importance of personalized medical approaches but also underscores the ongoing need for innovation and exploration in the field of urological care. This case illustrates the complexity of bladder diverticula management and the critical role of surgical strategies adapted to the unique anatomical and clinical characteristics of each patient. By overcoming the challenges presented by this rare and complex condition, we highlight the potential for improved outcomes through meticulous planning and execution of surgical interventions.
Furthermore, this experience emphasizes the need for continuous advancement in diagnostic and surgical techniques. The topic prompts the call for further research on the pathophysiology of bladder diverticula and the development of new methodologies that can improve diagnostic precision and treatment efficacy. Ultimately, our case contributes to the broader discourse on how urological care can evolve, with the goal of providing more effective, less invasive, and highly personalized treatment options for patients with complex urological conditions.
Ethical approval
Not applicable.
Consent
Written informed consent was obtained from the patient for the publication of this case report and any accompanying images. A copy of the written consent form is available for review by the Editor-in-Chief of this journal upon request.
Patient perspective
Successful surgical intervention in this case of multiple giant bladder diverticula significantly improved the patient’s quality of life, effectively alleviating his pain and resolving his urinary problems. After surgery, the patient reported a marked reduction in discomfort and an improved ability to perform daily activities, which had been markedly hampered by his symptoms prior to treatment. This improvement underscores the impact of tailored surgical strategies not only on clinical outcomes but also on patient satisfaction and quality of life. The patient expressed gratitude for the restored function and relief from chronic symptoms, illustrating the profound personal benefits of successful medical intervention in complex urological conditions.
Sources of funding
Not applicable.
Author contribution
All authors have contributed equally to the work reported in this manuscript, including the conception, design, execution, data acquisition, analysis and interpretation, and the drafting and revising of the manuscript for important intellectual content.
Conflicts of interest disclosure
The authors declare that they have no conflicts of interest concerning this article.
Research registration unique identifying number (UIN)
Not applicable.
Guarantor
Wael Gazzah.
Data availability statement
The datasets are available from the corresponding author on reasonable request.
Provenance and peer review
Not commissioned, externally peer-reviewed.
Footnotes
Sponsorships or competing interests that may be relevant to content are disclosed at the end of this article.
Published online 15 May 2024
Contributor Information
Wael Gazzah, Email: waelgazzah@gmail.com.
Souheil Ben Taher, Email: souheilbentaher@yahoo.com.
Sedki Masmoudi, Email: sedki.masmoudi@yahoo.fr.
Mahmoud Hamza, Email: mahmoud.hza@gmail.com.
Sahbi Naouar, Email: urologistsurgeon2016@gmail.com.
Braiek Salem, Email: salembraiek@hotmail.fr.
References
- 1.Abou Zahr R, Chalhoub K, Ollaik F, et al. Congenital bladder diverticulum in adults: a case report and review of the literature. Case Rep Urol 2018;2018:9748926. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Han Z, Sun X, Ma X, et al. Bladder diverticulum accompanied by abdominal pain: a case description. Quant Imaging Med Surg 2024;14:1215–1218. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Wu D, Dai R, Zheng S. Management of a large urinary bladder diverticulum with an open extravesical diverticulectomy. Asian J Surg 2023;46:2164–2165. [DOI] [PubMed] [Google Scholar]
- 4.Gazzah W, Mansi Z, Zaidi B. Contraceptive complication: emergence of a bladder stone - a case report. Int J Surg Case Rep 2024;118:109622. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Tan S, Sakaria S. Bladder diverticulum - a case report. J Educ Teach Emerg Med 2020;5:V15–V18. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Janardanan S, Nigam A, Moschonas D, et al. Urinary bladder diverticulum: a single-center experience in the management of refractory lower urinary symptoms using a robotic platform. Cureus 2023;15:e42354. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Celebi S, Kuzdan Ö, Özaydin S, et al. The effect of bladder diverticula on bladder function: an experimental study in rabbits. J Pediatr Surg 2016;51:1538–1542. [DOI] [PubMed] [Google Scholar]
- 8.Jiang S, Ren Q, Wang X, et al. A huge bladder diverticulum in an elderly: a case report. SAGE Open Med Case Rep 2020;8:2050313X2094347. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Giannarini G, Rossanese M, Macchione L, et al. Robot-assisted bladder diverticulectomy using a transperitoneal extravesical approach. Eur Urol Open Sci 2022;44:162–168. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Zhengqiang W, Yinglei W, Cheng L, et al. One-stage laparoscopy combined with resectoscope in the treatment of huge bladder diverticulum, multiple stones in diverticulum, multiple stones in bladder and benign prostatic hyperplasia: a case report. Front Med 2022;9:1036222. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Sohrabi C Mathew G Maria N et al. Collaborators . The SCARE 2023 guideline: updating consensus Surgical CAse REport (SCARE) guidelines. Int J Surg Lond Engl 2023;109:1136–1140. [DOI] [PMC free article] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Data Availability Statement
The datasets are available from the corresponding author on reasonable request.