

Pulmonary embolism and deep vein thrombosis are treated using similar drugs and physical methods. The efficacy of intravenous infusion of unfractionated heparin was first proved in a randomised trial in 1960. Subsequently, trials concentrated on the dose, duration of infusion, mode of administration, and combination with warfarin treatment. Later trials have reported the efficacy and cost effectiveness of low molecular weight heparin compared with unfractionated heparin.
Unfractionated heparin
Unfractionated heparin, administered by continuous infusion or subcutaneous injections adjusted to achieve activated partial thromboplastin time (APTT) greater than 1.5, is effective as initial treatment of venous thromboembolism. Initial heparinisation should be followed by long term anticoagulation with oral anticoagulants. APTT is a global coagulation test and not specific for heparin, and it is also influenced by various plasma proteins and clotting factors. Measuring plasma heparin levels is more accurate but it is impractical and expensive. A sensible approach is to standardise the APTT with plasma heparin within each laboratory.
Antithrombotic treatment is often inadequate in the first few days, predisposing to recurrences. Anticoagulation with warfarin after discharge should continue for at least three months, possibly six months. Low molecular weight heparin is as efficacious as unfractionated heparin in prophylaxis and treatment
The most common mistake when starting heparin treatment is failure to achieve adequate anticoagulation. APTT ratios of less than 1.5 during the first few days of heparin therapy increase the long term risk of venous thromboembolism recurrence. Hence, the initial bolus dose should be adequate and APTT monitored every six hours during the first 24 hours of heparin infusion.
Initial antithrombotic therapy for deep vein thrombosis with unfractionated heparin
Check baseline APTT, prothrombin time, full blood count
Confirm there are no contraindications to heparin therapy
Intravenous bolus 5000 IU
- Choose between:
-
Continuous unfractionated heparin infusion—Start infusion at 18 IU/kg/hour (∼30 000/24 hours in a 70 kg man)Check APTT every six hours for first 24 hours, then daily thereafterAim for APTT 1.5-2.5×normalRecheck APTT at six hours after each adjustmentContinue infusion for five to seven days
- Subcutaneous—Start at 17 500 IU every 12 hours (or 250 IU/kg every 12 hours)
-
Check platelet count daily for thrombocytopenia
Warfarin therapy can be started on the first day of heparin therapy according to local protocol
Continue heparin for at least four to five days after starting warfarin
Stop heparin when INR greater than 2 for more than 48 hours
Continue warfarin therapy for at least three months keeping INR between 2 and 3 (target 2.5)
Oral anticoagulants may be started at the same time and should be continued for at least three to six months, depending on the individual. The optimal duration of intravenous heparin treatment is five to seven days because this is the time needed to obtain an adequate and persistent reduction in the vitamin K dependent clotting factors with oral anticoagulants such as warfarin. Heparin can then be stopped when concomitant use with warfarin has achieved an international normalised ratio (INR) of 2-3 for at least 48 hours. In patients with large ileofemoral vein thromboses or major pulmonary embolism, heparin infusion can be continued for up to 10 days.
Heparin use for more than five to six days is associated with a rare risk of thrombocytopenia. In a recent trial, only one of 308 patients (0.32%) who received unfractionated heparin for acute pulmonary embolism developed a thrombocytopenia, whereas none of 304 patients receiving low molecular weight heparin had this problem. The thrombocytopenia is normally mild, but precipitous falls in platelet count to less than 100 000×109/l can occur. When this happens, antibody mediated injury to platelets should be suspected. As this condition may be associated with arterial or venous thromboembolism, heparin should be stopped and warfarin use delayed. Alternative anticoagulation cover should be given by danaparoid, a heparinoid, or hirudin, a thrombin inhibitor, until the platelet count rises above 100 000 and it is safe to start warfarin. Unfractionated heparin has also been reported to increase platelet activation in vivo: low molecular weight heparin had no such effect.
Low molecular weight heparin
Low molecular weight heparin has a more predictable relation between dose and response than unfractionated heparin and does not need monitoring or adjustments if the dose is based on patient body weight. Low molecular weight heparin is also associated with lower risk of thrombocytopenia. Its use in deep vein thrombosis and pulmonary embolism is now firmly established: many trials and meta-analysis have confirmed its superior efficacy, safer profile, and greater cost effectiveness over unfractionated heparins. However, all low molecular weight heparins are different, and trials for one product cannot be extrapolated to another. The introduction of low molecular weight heparin has advanced antithrombotic therapy by providing effective anticoagulation without the need for monitoring or adjustments. It also allows patients with uncomplicated deep vein thrombosis to be treated in the community, saving an average of four to five days' admission per patient.
Advantages of low molecular weight heparin over unfractionated heparin
More reliable relation between dose and response
Does not need monitoring
Does not need dose adjustments
Lower incidence of thrombocytopenia
No excess bleeding
Can be administered by patient at home
Saves about five to six days' admission per patient
Coumarins
Warfarin is the most widely used oral anticoagulant for treating venous thromboembolism. It is well absorbed from the gut, metabolised in the liver, and excreted in urine. The lag time for warfarin to take effect may be related to the natural clearance of normal clotting factors from plasma. Of the vitamin K dependent clotting factors, factor II takes the longest to clear. Warfarin monitoring is performed using an INR rather than prothrombin time, which may vary between laboratories. Warfarin interacts with many other drugs and alcohol. It is also teratogenic and may induce spontaneous abortion.
Duration of anticoagulation therapy for venous thromboembolism*
Three to six months
First event with reversible† or time limited risk factor (patient may have underlying factor V Leiden or prothrombin 20210 mutation)
More than six months
Idiopathic venous thromboembolism, first event
A year to life time
First event‡ with cancer (until resolved), anticardiolipin antibody, antithrombin deficiency
Recurrent event, idiopathic or with thrombophilia
*All recommendations are subject to modification by individual characteristics including patient preference, age, comorbidity, and likelihood of recurrence†Reversible or time limited risk factors such as surgery, trauma, immobilisation, and oestrogen use‡Proper duration of therapy is unclear in first event with homozygous factor V Leiden, homocystinaemia, deficiency of protein C or S, or multiple thrombophilias; and in recurrent events with reversible risk factors
A target INR range of 2-3 is standard for treatment of venous thromboembolism. Higher levels tend to increase incidence of bleeding without reducing recurrent thromboembolism and so are unnecessary. The exception to this is for patients with the antiphospholipid antibody syndrome, where the risk of recurrent venous thromboembolism is high. Here, an INR of 3-4.5 is recommended. Warfarin should be started in conjunction with heparin or low molecular weight heparin when the diagnosis of venous thromboembolism is confirmed, although local protocols may vary in their starting doses and titration schedule. As indicated, heparin should be continued concomitantly for five days and until INR is >2.
Warfarin therapy should then be maintained for at least three months in all patients. However, it has recently been established that longer treatments (such as six months) may be necessary. Patients without a readily identifiable risk factor (idiopathic venous thromboembolism) have higher rates of recurrences. These recurrences can be reduced by prolonged anticoagulation. However, there is a corresponding rise in bleeding complications with prolonged anticoagulation. Current recommendations advocate anticoagulation for at least six months for the first presentation of idiopathic venous thromboembolism. Patients with recurrent venous thromboembolism and hypercoagulable states (acquired or inherited) or with cancer (especially while receiving chemotherapy) should take anticoagulation therapy for at least a year, and perhaps indefinitely.
Thrombolytic regimens for pulmonary embolism
1 Check suitability of patient for thrombolysis
2 Choose between: Streptokinase—250 000 IU loading dose then 100 000 IU/hour for 24 hours Urokinase—4400 IU/kg loading dose then 2700 IU/kg/hour for 12 hours Alteplase—100 mg intravenously over an hour
3 Check APTT two to four hours after starting infusion: >10 seconds prolongation indicates active fibrinolysis
4 Start heparin at 30 000 IU/hour when APTT < 2
5 Adjust according to local protocol to keep APTT 1.5-2.5
Thrombolytic therapy
Unlike heparin and warfarin, which prevent extension and recurrences of thrombosis, thrombolytic agents (including streptokinase, urokinase, and tissue plasminogen activator) lyse the thrombi. It is therefore unsurprising that patients with pulmonary embolism treated with streptokinase and urokinase are three times more likely to show clot resolution than patients taking heparin alone. Even so, thrombolytic therapy of pulmonary embolism does not dissolve the clot completely as it does with acute coronary thrombosis, and increases the risk of bleeding. Occasionally, thrombolytic therapy is administered via a catheter placed in the pulmonary artery. The catheter can be used to “disrupt” the thrombus before starting the drug.
Indications for inferior vena cava filter placement
Patients at high risk of proximal deep vein thrombosis extension where anticoagulation is contraindicated
Recurrent venous thromboembolism despite adequate anticoagulation
Chronic recurrent venous thromboembolism with pulmonary hypertension
Simultaneous surgical pulmonary embolectomy or endarterectomy
Until there is more evidence that thrombolytic therapy reduces mortality in pulmonary embolism, this treatment should be reserved for patients with massive pulmonary embolism, cardiorespiratory compromise, and low risk of bleeding. Evidence is emerging that streptokinase can decrease swelling and pain in deep vein thrombosis. Again, further trials are needed before this can be recommended routinely.
Mechanical and surgical treatment of pulmonary embolism
Inferior vena cava filter placementIndications—See box above
Pulmonary embolectomyIndication—Massive pulmonary embolism compromising cardiac output where thrombolysis has failed or is contraindicatedExperienced cardiac surgical cover essentialWhere available, catheter transvenous extraction of emboli may be an alternative to pulmonary embolectomy
Pulmonary endarterectomyIndication—Chronic recurrent pulmonary embolism with secondary pulmonary hypertension
Physical methods
Non-drug treatments include physically preventing embolisation of the thrombi and extraction of thromboemboli (usually from the pulmonary vasculature).
Inferior vena cava filters may be used when anticoagulation is contraindicated in patients at high risk of proximal deep vein thrombosis extension or embolisation. The filter is normally inserted via the internal jugular or femoral vein. It is then advanced under fluoroscopic guidance to the inferior vena cava. Filters are now available that are easy to insert, and complications are low in skilled hands. For now, this technique should be considered in patients with recurrent symptomatic pulmonary embolism and as primary prophylaxis of thromboembolism in patients at high risk of bleeding (such as patients with extensive trauma or visceral cancer), although the evidence is based on uncontrolled case series. The only randomised trial showed a reduction in pulmonary embolism but no improvement in short or long term survival, because of greater risk of recurrent deep vein thrombosis in patients who received a filter.
Other mechanical and surgical treatments are usually reserved for massive pulmonary embolism where drug treatments have failed or are contraindicated. None of these methods has shown a long term reduction in mortality, but better techniques have led to acceptable complication rates and warrant further evaluation.
Treatment during pregnancy
Unfractionated heparin and low molecular weight heparin do not cross the placenta and are probably safe for the fetus during pregnancy. Oral anticoagulants cross the placenta and can cause fetal bleeding and malformations. Pregnant women with venous thromboembolism can be treated with therapeutic doses of subcutaneous heparin or low molecular weight heparin until after delivery, when warfarin can be used safely.
Further reading
Decousus H, Leizorovicz A, Parent F, Page Y, Tardy B, Girard P, et al. A clinical trial of vena caval filters in the prevention of pulmonary embolism in patients with proximal deep vein thrombosis.
Geerts WH, Heit JA, Clagett GP, Pineo GF, Colwell CW, Anderson FA Jr, et al. Prevention of venous thromboembolism. Chest 2000;119:132-75S
Heit JA, O'Fallon WM, Petterson T, Lohse CM, Silverstein MD, Mohr DN, et al. Relative impact of risk factors for deep vein thrombosis and pulmonary embolism. Arch Intern Med 2002;162:1245-8
Levine M, Gent M, Hirsch J, Leclerc J, Anderson D, Weitz J, et al. A comparison of low-molecular-weight heparin administered primarily at home with unfractionated heparin administered in the hospital for proximal deep-vein thrombosis. N Engl J Med 1996;334:677-81
Walker ID, Greaves M, Preston FE. Guideline: investigation and management of heritable thrombophilia. Br J Haematol 2001;114:512-28
Figure.
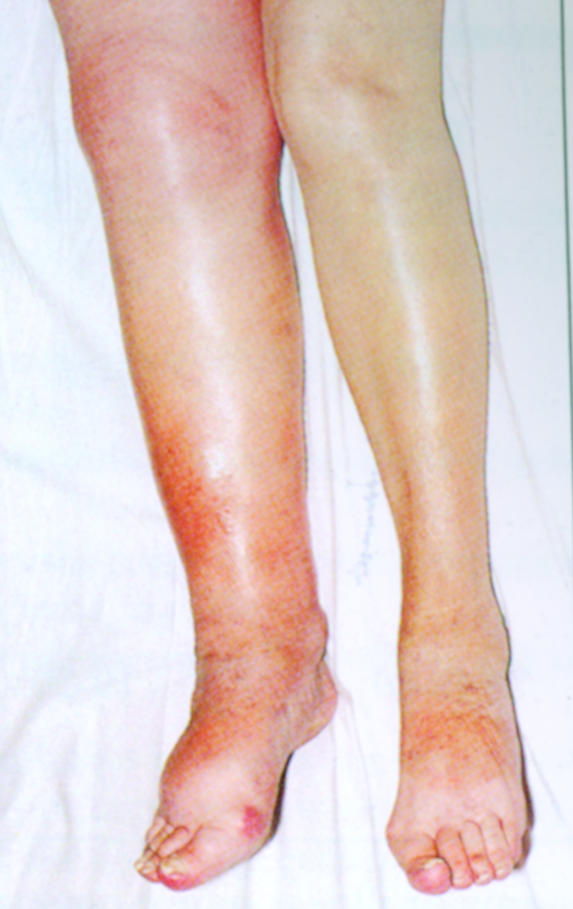
Right ileofemoral deep vein thrombosis
Figure.
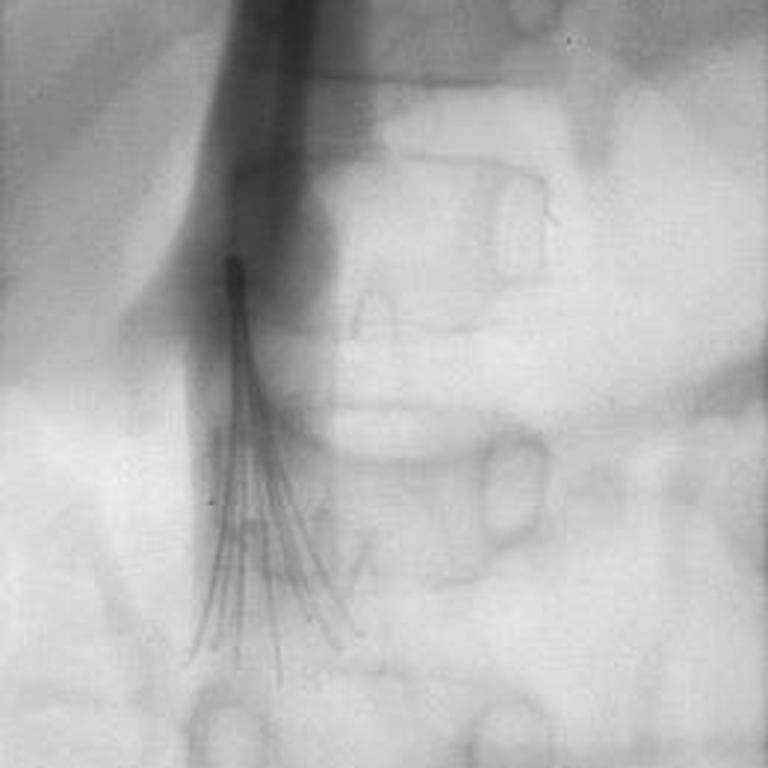
Vena cavagram showing umbrella delivery device for filter inserted into the inferior vena cava through the jugular vein
Acknowledgments
The data on duration of anticoagulation therapy for venous thromboembolism is adapted from the 6th ACCP guidelines Hyers TM, et al. Antithrombotic therapy for venous thromboembolic disease. Chest 2001;119:176-93S
Footnotes
Alexander G G Turpie is professor of medicine, McMaster University, Hamilton, Canada; Bernard S P Chin is research fellow and Gregory Y H Lip is professor of cardiovascular medicine at the haemostasis thrombosis and vascular biology unit, university department of medicine, City Hospital, Birmingham.
The ABC of antithrombotic therapy is edited by Gregory Y H Lip and Andrew D Blann, senior lecturer in medicine, haemostasis thrombosis and vascular biology unit, university department of medicine, City Hospital, Birmingham. The series will be published as a book in spring 2003.